
Preterm Prelabour Rupture of Membranes before Viability in Twin Pregnancies: What Can We Expect?

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Outcomes
2.3. Data Collection
2.4. PPROM Assessment and Management
2.5. Statistical Analysis
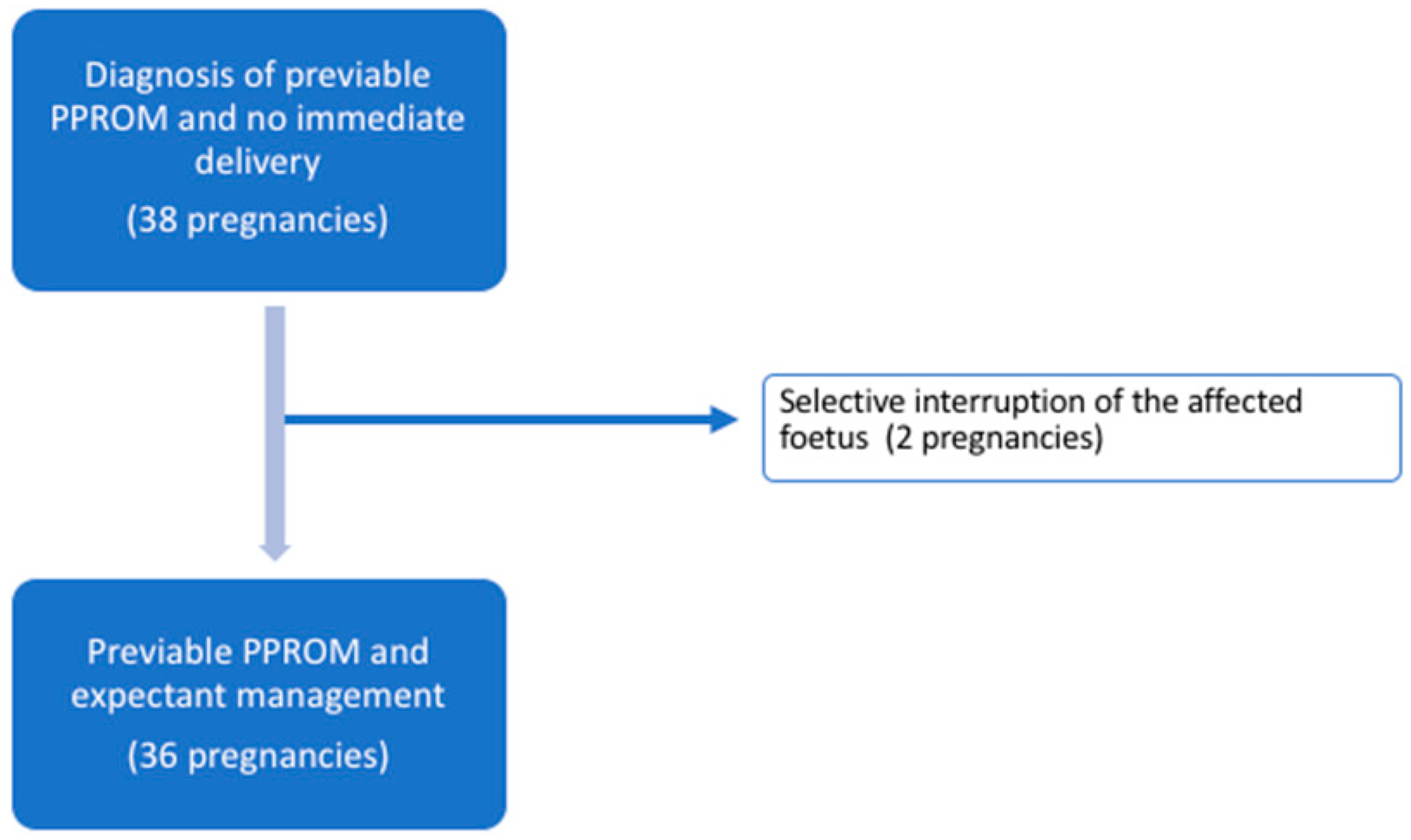
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variables | No Foetoscopy (N = 22) | Foetoscopy (N = 16) | p-Value |
| Gestational age at PPROM (weeks) | 17.9 (15.0–21.6) | 18.8 (16.8–22.6) | 0.147 |
| Previous invasive procedure | 6/22 (27.3) | 1/16 (6.3) | 0.203 |
| MVP-AF (mm) at PPROM MVP-AF (mm) 1 week after PPROM | 0 (0–13.5) 6 (0–15) | 19.5 (13–26) 15.5 (0–25) | 0.007 0.218 |
| Cervical length (mm) | 30.5 (21.5–37) | 37.5 (32–44.5) | 0.054 |
| Selective termination | 0 (0) | 2/16 (12.5) | 0.171 |
| Gestational age at delivery (weeks) | 26.5 (23–28.7) | 23.9 (21–28.6) | 0.417 |
| Latency to delivery (weeks) | 6.5 (3.6–12) | 3.1 (2–8.6) | 0.127 |
| PPROM related complications * | 8/22 (36.4) | 3/14 (21.4) | 0.467 |
| Intrauterine foetal demise Miscarriage (<23 + 0 weeks) | 3/44 (6.8) 9/44 (20.5) | 2/28 (7.1) 10/28 (35.7) | >0.99 0.152 |
| Overall perinatal survival Neonatal survival if delivery ≥23 + 0 weeks † | 24/44 (54.6) 24/30 (80) | 11/28 (39.3) 11/14 (78.6) | 0.207 >0.99 |
| Composite neonatal morbidity ǂ Pulmonary hypoplasia | 15/30 (50) 4/30 (13.3) | 7/14 (50) 0 (0) | >0.99 0.290 |
References
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Sela, H.Y.; Simpson, L.L. Preterm premature rupture of membranes complicating twin pregnancy: Management considerations. Clin. Obstet. Gynecol. 2011, 54, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Wagner, P.; Sonek, J.; Mayr, S.; Abele, H.; Goelz, R.; Hoopmann, M.; Kagan, K.O. Outcome of dichorionic diamniotic twin pregnancies with spontaneous PPROM before 24 weeks’ gestation. J. Matern. Fetal. Neonatal. Med. 2017, 30, 1750–1754. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.F.; Holmgren, C.M.; Silver, R.M.; Varner, M.W.; Manuck, T.A. Outcomes of expectantly managed pregnancies with multiple gestations and preterm premature rupture of membranes prior to 26 weeks. Am. J. Obstet. Gynecol. 2015, 212, 2151–2159. [Google Scholar] [CrossRef]
- Waters, T.P.; Mercer, B.M. The management of preterm premature rupture of the membranes near the limit of fetal viability. Am. J. Obstet. Gynecol. 2009, 201, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Cobo, T.; Munrós, J.; Ríos, J.; Ferreri, J.; Migliorelli, F.; Baños, N.; Gratacós, E.; Palacio, M. Contribution of Amniotic Fluid along Gestation to the Prediction of Perinatal Mortality in Women with Early Preterm Premature Rupture of Membranes. Fetal. Diagn. Ther. 2018, 43, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Sim, W.H.; Araujo-Júnior, E.; Da Silva-Costa, F.; Sheehan, P.M. Maternal and neonatal outcomes following expectant management of preterm premature rupture of membranes before viability. J. Perinat. Med. 2017, 45, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Kiver, V.; Boos, V.; Thomas, A.; Henrich, W.; Weichert, A. Perinatal outcomes after previable preterm premature rupture of membranes before 24 weeks of gestation. J. Perinat. Med. 2018, 46, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Palacio, M.; Cobo, T.; Figueras, F.; Gómez, O.; Coll, O.; Cararach, V.; Gratacós, E. Previable rupture of membranes: Effect of amniotic fluid on pregnancy outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 138, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Brumbaugh, J.E.; Colaizy, T.T.; Nuangchamnong, N.; O’Brien, E.A.; Fleener, D.K.; Rijhsinghani, A.; Klein, J.M. Neonatal survival after prolonged preterm premature rupture of membranes before 24 weeks of gestation. Obstet. Gynecol. 2014, 124, 992–998. [Google Scholar] [CrossRef]
- Keselman, L.; Perlitz, Y.; Younis, J.; Ben-Ami, M. Nonconventional Approach to Twin Pregnancies Complicated by Extremely Preterm Premature Rupture of Membranes of One Twin. Am. J. Perinatol. 2008, 25, 161–162. [Google Scholar] [CrossRef] [PubMed]
- Lim, B.; Butler, B.; Gagnon, A.; Lim, K.; Marquette, G.; Dahlgren, L. Outcomes of Selective Reduction of DCDA Twins Complicated by PV-PROM Compared with Expectant Management: A Case Series and Review of the Literature. J. Obstet. Gynaecol. Can. 2018, 40, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, R.S.; Blanco, J.D.; St Clair, P.J.; Castaneda, Y.S. Quantitative bacteriology of amniotic fluid from women with clinical intraamniotic infection at term. J. Infect. Dis. 1982, 145, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Van der Heyden, J.L.; Van der Ham, D.P.; Van Kuijk, S.; Notten, K.J.B.; Janssen, T.; Nijhuis, J.G.; Willekes, C.; Porath, M.; Van der Post, J.A.; Halbertsma, F.; et al. Outcome of pregnancies with preterm premature rupture of membranes before 27 weeks’ gestation: A retrospective cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Ekin, A.; Gezer, C.; Taner, C.E.; Ozeren, M.; Uyar, I.; Gulhan, I. Risk factors and perinatal outcomes associated with latency in preterm premature rupture of membranes between 24 and 34 weeks of gestation. Arch. Gynecol. Obstet. 2014, 290, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Kibel, M.; Barrett, J.; Tward, C.; Pittini, A.; Kahn, M.; Melamed, N. The natural history of preterm premature rupture of membranes in twin pregnancies. J. Matern. Fetal. Neonatal. Med. 2017, 30, 1829–1835. [Google Scholar] [CrossRef] [PubMed]
- Bartin, R.; Colmant, C.; Bourgon, N.; Ville, Y.; Stirnemann, J. Effect of gestational age at laser therapy on perinatal outcome in monochorionic diamniotic pregnancies affected by twin-to-twin transfusion syndrome. BJOG 2022, 129, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.J.; Hong, J.S.; Romero, R.; Yoon, B.H. The frequency and clinical significance of intra-amniotic inflammation in twin pregnancies with preterm labor and intact membranes. J. Matern. Fetal. Neonatal. Med. 2019, 32, 527–541. [Google Scholar] [CrossRef] [PubMed]


| Variables | Twin Pregnancies (N = 38) | Dichorionic (N = 17) | Monochorionic (N = 21) | p-Value |
|---|---|---|---|---|
| Maternal age (years) | 32.4 (30.1- 37.2) | 34.4 (30.7–37.9) | 31.1 (29.2–36.9) | 0.138 |
| Ethnicity | ||||
| - Caucasian - Maghreb - Hispanic - Asian | 32/38 (84.2) 3/38 (7.9) 2/38 (5.3) 1/38 (2.6) | 14/17 (82.3) 1/17 (5.9) 1/17 (5.9) 1/17 (5.9) | 18/21 (85.7) 2/21 (9.5) 1/21 (4.8) 0/21 (0) | 0.882 |
| Body mass index | 24.7 (20.3–29.7) | 27.9 (22.5–35.7) | 22.6 (18.4–25.5) | 0.083 |
| ART | 13/38 (34.2) | 11/17 (64.7) | 2/21 (9.5) | 0.001 |
| Nulliparity | 25/38 (65.8) | 13/17 (76.5) | 12/21 (57.1) | 0.307 |
| SPTB * risk factors | 4/38 (10.5) | 1/17 (5.9) | 3/21 (14.3) | 0.613 |
| Previous invasive procedure † GA at procedure | 7/38 (18.4) 13.6 (12.0–20.0) | 5/17 (29.4) 13.6 (12–16) | 2/21 (9.5) 16.6 (13.3–20) | 0.207 0.699 |
| Previous foetoscopy GA at foetoscopy | 16/21 (76.2) 16.8 (16.2–17.7) | NA NA | ||
| GA at PPROM | 18.6 (16.0–22.0) | 16.6 (15–20.9) | 19.3 (16.7–22.3) | 0.146 |
| MVP-AF (mm) at PPROM | 10 (0–20.5) | 0 (0–15) | 17 (10–26) | 0.012 |
| MVP-AF (mm) 1 week after PPROM | 10 (0–19) | 0 (0–10) | 16.5 (10–25) | 0.014 |
| Cervical length (mm) | 33.5 (25–40) | 31 (25–40) | 37 (23–41) | 0.520 |
| Variables | Twin Pregnancies (N = 36) |
|---|---|
| Gestational age at delivery | 25.4 (22.1–28.6) |
| Latency to delivery (weeks) | 5.4 (2.6–9.6) |
| Chorioamnionitis Placental abruption Cord prolapse | 8/36 (22.2%) 1/36 (2.8%) 2/36 (5.6%) |
| Maternal morbidity * | 6/36 (16.7%) |
| Foetuses (N = 72) | |
| Intrauterine foetal demise Miscarriage (<23 + 0 weeks) | 5/72 (6.9%) 19/72 (26.4%) |
| Overall perinatal survival Neonatal survival if delivery ≥23 + 0 weeks † | 35/72 (48.6%) 35/44 (79.5%) |
| Birthweight (grams) † Neonatal death † Composite neonatal morbidity ǂ | 988.5 (800–1260) 9/44 (20.5%) 22/44 (50%) |
| Pulmonary hypoplasia | 4/44 (9.1%) |
| Variables | OR (95% Confidence Interval) | p-Value |
|---|---|---|
| Monochorionicity | 1.65 (0.41–6.68) | 0.481 |
| Assisted reproductive technology | 1.30 (0.32–5.33) | 0.719 |
| Previous invasive procedure * Foetoscopy | 2.33 (0.36–15.05) 1.71 (0.40–7.27) | 0.373 0.467 |
| Gestational age at PPROM | 1.04 (0.83–1.30) | 0.716 |
| MVP-AF < 1 cm at PPROM diagnosis MVP-AF < 1 cm after 1-week of PPROM | 1.33 (0.28–6.28) 1.25 (0.21–7.62) | 0.716 0.809 |
| Cervical length < 25 mm at PPROM | 0.54 (0.09–3.14) | 0.498 |
| Intrauterine foetal demise of one twin | 1.00 (0.12–8.13) | >0.99 |
| C-reactive protein levels at PPROM Leucocytosis † at PPROM | 1.63 (0.74–3.59) 1.50 (0.26–8.82) | 0.222 0.654 |
| Gestational age at delivery | 0.22 (0.06–0.75) | 0.016 |
| Variables | OR (95% Confidence Interval) | p-Value |
| Monochorionicity | 0.30 (0.06–1.38) | 0.121 |
| ART | 3.54 (0.63–19.82) | 0.151 |
| Previous invasive procedure * Foetoscopy | 0.51 (0.09–2.79) 0.39 (0.09–1.68) | 0.436 0.207 |
| GA at PPROM | 1.23 (0.97–1.56) | 0.094 |
| MVP-AF < 1 cm at PPROM diagnosis MVP-AF < 1 cm after 1-week of PPROM | 1.67 (0.35–8.04) 3.21 (0.47–21.80) | 0.525 0.232 |
| Cervical length < 25 mm at PPROM | 0.39 (0.07–2.04) | 0.265 |
| Intrauterine foetal demise of one twin | 0.23 (0.03–1.65) | 0.144 |
| C-reactive protein levels at PPROM Leucocytosis † at PPROM | 1.11 (0.58–2.14) 1.67 (0.29–9.44) | 0.748 0.564 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ponce, J.; Cobo, T.; Murillo, C.; Gonce, A.; Domínguez, N.; Crovetto, F.; Guirado, L.; Palacio, M.; Bennasar, M. Preterm Prelabour Rupture of Membranes before Viability in Twin Pregnancies: What Can We Expect? J. Clin. Med. 2023, 12, 2949. https://doi.org/10.3390/jcm12082949
Ponce J, Cobo T, Murillo C, Gonce A, Domínguez N, Crovetto F, Guirado L, Palacio M, Bennasar M. Preterm Prelabour Rupture of Membranes before Viability in Twin Pregnancies: What Can We Expect? Journal of Clinical Medicine. 2023; 12(8):2949. https://doi.org/10.3390/jcm12082949
Chicago/Turabian StylePonce, Júlia, Teresa Cobo, Clara Murillo, Anna Gonce, Nadia Domínguez, Francesca Crovetto, Laura Guirado, Montse Palacio, and Mar Bennasar. 2023. "Preterm Prelabour Rupture of Membranes before Viability in Twin Pregnancies: What Can We Expect?" Journal of Clinical Medicine 12, no. 8: 2949. https://doi.org/10.3390/jcm12082949
APA StylePonce, J., Cobo, T., Murillo, C., Gonce, A., Domínguez, N., Crovetto, F., Guirado, L., Palacio, M., & Bennasar, M. (2023). Preterm Prelabour Rupture of Membranes before Viability in Twin Pregnancies: What Can We Expect? Journal of Clinical Medicine, 12(8), 2949. https://doi.org/10.3390/jcm12082949