
Smoking Increases the Risk of Hepatocellular Carcinoma and Cardiovascular Disease in Patients with Metabolic-Associated Fatty Liver Disease
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Data Collection
2.3. Definition of MAFLD and Control Group
0.053 × (Waist circumference) − 15.745
2.4. Study Outcome
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics of the Study Population
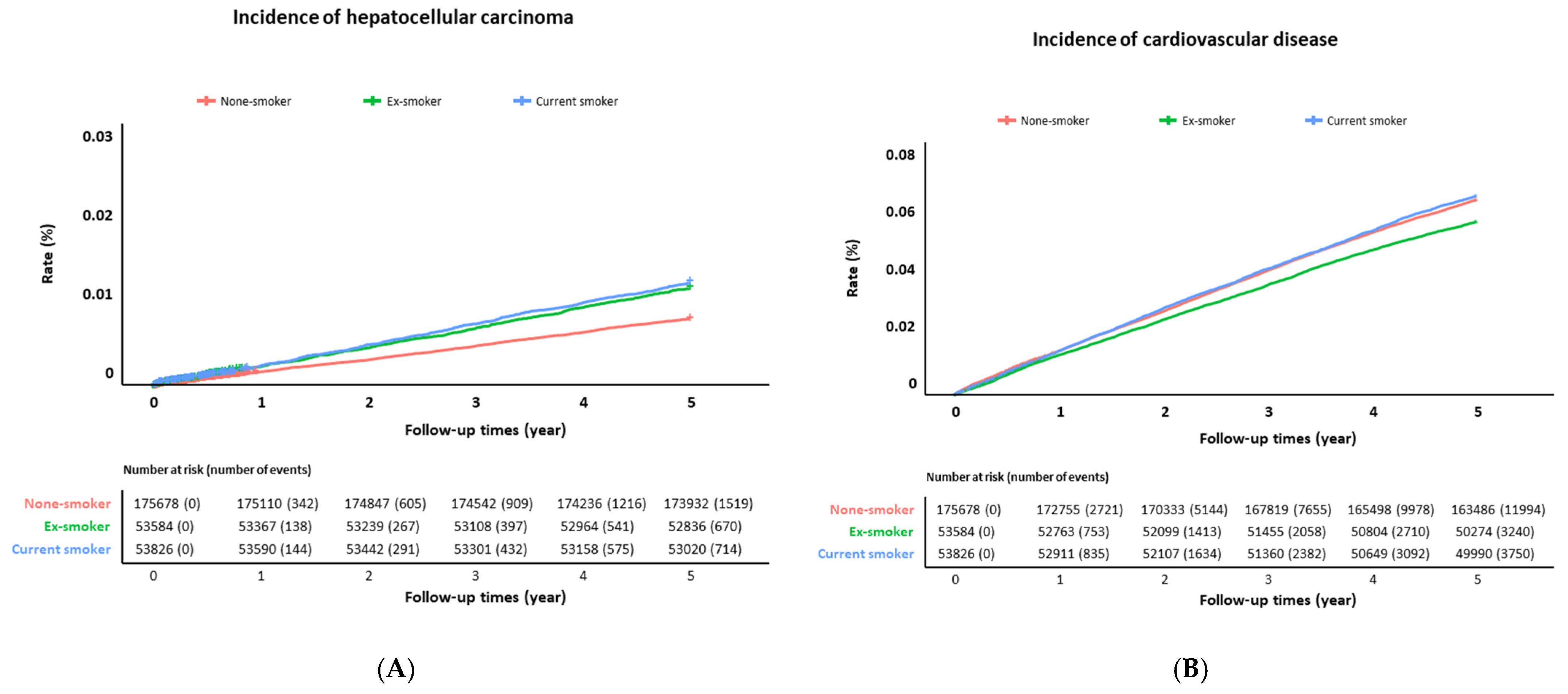
3.2. Incidence of HCC and CVD
3.3. Association between Smoking and Incident HCC
3.4. Smoking on the Development of CVD
3.5. Effect of Smoking in Stratification by Sex
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Fouad, Y.; Waked, I.; Bollipo, S.; Gomaa, A.; Ajlouni, Y.; Attia, D. What’s in a name? Renaming ‘NAFLD’ to ‘MAFLD’. Liver Int. 2020, 40, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Tsutsumi, T.; Nakano, D.; Eslam, M.; George, J.; Torimura, T. MAFLD enhances clinical practice for liver disease in the Asia-Pacific region. Clin. Mol. Hepatol. 2022, 28, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Quek, J.; Ng, C.H.; Tang, A.S.P.; Chew, N.; Chan, M.; Khoo, C.M.; Wei, C.P.; Chin, Y.H.; Tay, P.; Lim, G.; et al. Metabolic Associated Fatty Liver Disease Increases the Risk of Systemic Complications and Mortality. A Meta-Analysis and Systematic Review of 12 620 736 Individuals. Endocr. Pract. 2022, 28, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.J.; Singal, A.K. Trends in Liver Disease Etiology Among Adults Awaiting Liver Transplantation in the United States, 2014–2019. JAMA Netw. Open. 2020, 3, e1920294. [Google Scholar] [CrossRef] [PubMed]
- Korean Liver Cancer Association (KLCA) and National Cancer Center (NCC) Korea. 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma. J. Liver Cancer 2023, 23, 1–120. [Google Scholar] [CrossRef]
- Daher, D.; Dahan, K.S.E.; Singal, A.G. Non-alcoholic fatty liver disease-related hepatocellular carcinoma. J. Liver Cancer 2023, 23, 127–142. [Google Scholar] [CrossRef]
- Rutledge, S.M.; Asgharpour, A. Smoking and Liver Disease. Gastroenterol. Hepatol. (N. Y.) 2020, 16, 617–625. [Google Scholar]
- Addolorato, G.; Bataller, R.; Burra, P.; DiMartini, A.; Graziadei, I.; Lucey, M.R.; Mathurin, P.; O’Grady, J.; Pageaux, G.; Berenguer, M. Liver Transplantation for Alcoholic Liver Disease. Transplantation 2016, 100, 981–987. [Google Scholar] [CrossRef]
- Adams, L.A.; Anstee, Q.M.; Tilg, H.; Targher, G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017, 66, 1138–1153. [Google Scholar] [CrossRef]
- Marti-Aguado, D.; Clemente-Sanchez, A.; Bataller, R. Cigarette smoking and liver diseases. J. Hepatol. 2022, 77, 191–205. [Google Scholar] [CrossRef]
- Shohdy, K.S.; Abdel-Rahman, O. Is smoking causally-associated with hepatitis B virus-related hepatocellular carcinoma? Ann. Transl. Med. 2019, 7, S44. [Google Scholar] [CrossRef]
- Taye, B.W. Hepatitis C virus infection and tobacco smoking—Joint health effects and implications for treatment of both: A systematic review. medRxiv 2021. [Google Scholar] [CrossRef]
- Zhang, X.F.; Wei, T.; Liu, X.M.; Liu, C.; Lv, Y. Impact of cigarette smoking on outcome of hepatocellular carcinoma after surgery in patients with hepatitis B. PLoS ONE 2014, 9, e85077. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Diabetologia 2016, 59, 1121–1140. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef]
- Lee, H.; Lee, H.W.; Kim, S.U.; Chang Kim, H. Metabolic Dysfunction-Associated Fatty Liver Disease Increases Colon Cancer Risk: A Nationwide Cohort Study. Clin. Transl. Gastroenterol. 2022, 13, e00435. [Google Scholar] [CrossRef]
- Lee, H.; Lee, Y.H.; Kim, S.U.; Kim, H.C. Metabolic Dysfunction-Associated Fatty Liver Disease and Incident Cardiovascular Disease Risk: A Nationwide Cohort Study. Clin. Gastroenterol. Hepatol. 2021, 19, 2138–2147. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Huang, D.Q.; El-Serag, H.B.; Loomba, R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 223–238. [Google Scholar] [CrossRef]
- Patel, R.R.; Ryu, J.H.; Vassallo, R. Cigarette smoking and diffuse lung disease. Drugs 2008, 68, 1511–1527. [Google Scholar] [CrossRef]
- Sasco, A.J.; Secretan, M.B.; Straif, K. Tobacco smoking and cancer: A brief review of recent epidemiological evidence. Lung Cancer 2004, 45 (Suppl. S2), S3–S9. [Google Scholar] [CrossRef]
- Wilson, P.W. Smoking, smoking cessation, and risk of cardiovascular disease. Curr. Treat. Options Cardiovasc. Med. 2006, 8, 276–281. [Google Scholar] [CrossRef]
- Abdullah, A.S.; Husten, C.G. Promotion of smoking cessation in developing countries: A framework for urgent public health interventions. Thorax 2004, 59, 623–630. [Google Scholar] [CrossRef]
- El-Zayadi, A.R. Heavy smoking and liver. World J. Gastroenterol. 2006, 12, 6098–6101. [Google Scholar] [CrossRef]
- Husain, K.; Scott, B.R.; Reddy, S.K.; Somani, S.M. Chronic ethanol and nicotine interaction on rat tissue antioxidant defense system. Alcohol 2001, 25, 89–97. [Google Scholar] [CrossRef]
- Watanabe, K.; Eto, K.; Furuno, K.; Mori, T.; Kawasaki, H.; Gomita, Y. Effect of cigarette smoke on lipid peroxidation and liver function tests in rats. Acta Med. Okayama 1995, 49, 271–274. [Google Scholar] [CrossRef]
- Yu, M.W.; Yang, S.Y.; Chiu, Y.H.; Chiang, Y.C.; Liaw, Y.F.; Chen, C.J. A p53 genetic polymorphism as a modulator of hepatocellular carcinoma risk in relation to chronic liver disease, familial tendency, and cigarette smoking in hepatitis B carriers. Hepatology 1999, 29, 697–702. [Google Scholar] [CrossRef]
- Suzuki, N.; Wakisaka, S.; Takeba, Y.; Mihara, S.; Sakane, T. Effects of cigarette smoking on Fas/Fas ligand expression of human lymphocytes. Cell. Immunol. 1999, 192, 48–53. [Google Scholar] [CrossRef]
- Meliska, C.J.; Stunkard, M.E.; Gilbert, D.G.; Jensen, R.A.; Martinko, J.M. Immune function in cigarette smokers who quit smoking for 31 days. J. Allergy Clin. Immunol. 1995, 95, 901–910. [Google Scholar] [CrossRef]
- Wang, L.Y.; Chen, C.J.; Zhang, Y.J.; Tsai, W.Y.; Lee, P.H.; Feitelson, M.A.; Lee, C.S.; Santella, R.M. 4-Aminobiphenyl DNA damage in liver tissue of hepatocellular carcinoma patients and controls. Am. J. Epidemiol. 1998, 147, 315–323. [Google Scholar] [CrossRef]
- Sherman, M. Vinyl chloride and the liver. J. Hepatol. 2009, 51, 1074–1081. [Google Scholar] [CrossRef]
- Wang, B.; Zhang, Y.; Xu, D.Z.; Wang, A.H.; Zhang, L.; Sun, C.S.; Li, L.S. [Meta-analysis on the relationship between tobacco smoking, alcohol drinking and p53 alteration in cases with esophageal carcinoma]. Zhonghua Liu Xing Bing Xue Za Zhi 2004, 25, 775–778. [Google Scholar]
- Lee, Y.C.; Cohet, C.; Yang, Y.C.; Stayner, L.; Hashibe, M.; Straif, K. Meta-analysis of epidemiologic studies on cigarette smoking and liver cancer. Int. J. Epidemiol. 2009, 38, 1497–1511. [Google Scholar] [CrossRef]
- Abdel-Rahman, O.; Helbling, D.; Schob, O.; Eltobgy, M.; Mohamed, H.; Schmidt, J.; Giryes, A.; Mehrabi, A.; Iype, S.; John, H.; et al. Cigarette smoking as a risk factor for the development of and mortality from hepatocellular carcinoma: An updated systematic review of 81 epidemiological studies. J. Evid. Based Med. 2017, 10, 245–254. [Google Scholar] [CrossRef]
- Jung, H.S.; Chang, Y.; Kwon, M.J.; Sung, E.; Yun, K.E.; Cho, Y.K.; Shin, H.; Ryu, S. Smoking and the Risk of Non-Alcoholic Fatty Liver Disease: A Cohort Study. Am. J. Gastroenterol. 2019, 114, 453–463. [Google Scholar] [CrossRef]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver Fibrosis, but No Other Histologic Features, Is Associated With Long-term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2015, 149, 389–397. [Google Scholar] [CrossRef]
- Hassan, M.M.; Abdel-Wahab, R.; Kaseb, A.; Shalaby, A.; Phan, A.T.; El-Serag, H.B.; Hawk, E.; Morris, J.; Singh Raghav, K.P.; Lee, J.S.; et al. Obesity Early in Adulthood Increases Risk but Does Not Affect Outcomes of Hepatocellular Carcinoma. Gastroenterology 2015, 149, 119–129. [Google Scholar] [CrossRef]
- Ioannou, G.N. Epidemiology and risk-stratification of NAFLD-associated HCC. J. Hepatol. 2021, 75, 1476–1484. [Google Scholar] [CrossRef]
- Yuan, J.M.; Govindarajan, S.; Arakawa, K.; Yu, M.C. Synergism of alcohol, diabetes, and viral hepatitis on the risk of hepatocellular carcinoma in blacks and whites in the U.S. Cancer 2004, 101, 1009–1017. [Google Scholar] [CrossRef]
- Marrero, J.A.; Fontana, R.J.; Fu, S.; Conjeevaram, H.S.; Su, G.L.; Lok, A.S. Alcohol, tobacco and obesity are synergistic risk factors for hepatocellular carcinoma. J. Hepatol. 2005, 42, 218–224. [Google Scholar] [CrossRef]
- Petrick, J.L.; Campbell, P.T.; Koshiol, J.; Thistle, J.E.; Andreotti, G.; Beane-Freeman, L.E.; Buring, J.E.; Chan, A.T.; Chong, D.Q.; Doody, M.M.; et al. Tobacco, alcohol use and risk of hepatocellular carcinoma and intrahepatic cholangiocarcinoma: The Liver Cancer Pooling Project. Br. J. Cancer 2018, 118, 1005–1012. [Google Scholar] [CrossRef]
- Hajat, A.; Lucas, J.B.; Kington, R. Health Outcomes among Hispanic Subgroups: Data from the National Health Interview Survey, 1992–1995. In Advance Data; U.S. Department of Health and Human Services: Washington, DC, USA; Centers for Disease Control and Prevention: Atlanta, GA, USA; National Center for Health Statistics: Hyattsville, MD, USA, 2000; pp. 1–14. [Google Scholar]
- Pomerleau, C.S.; Pomerleau, O.F.; Snedecor, S.M.; Mehringer, A.M. Defining a never-smoker: Results from the nonsmokers survey. Addict. Behav. 2004, 29, 1149–1154. [Google Scholar] [CrossRef]
- Wu, E.M.; Wong, L.L.; Hernandez, B.Y.; Ji, J.F.; Jia, W.; Kwee, S.A.; Kalathil, S. Gender differences in hepatocellular cancer: Disparities in nonalcoholic fatty liver disease/steatohepatitis and liver transplantation. Hepatoma Res. 2018, 4, 66. [Google Scholar] [CrossRef]
- Huxley, R.R.; Woodward, M. Cigarette smoking as a risk factor for coronary heart disease in women compared with men: A systematic review and meta-analysis of prospective cohort studies. Lancet 2011, 378, 1297–1305. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total | MAFLD | Control | p-Value * |
|---|---|---|---|---|
| (n = 283,088) | (n = 110,863) | (n = 172,225) | ||
| Age, years | 58.6 ± 8.6 | 58.2 ± 8.2 | 58.8 ± 8.9 | <0.001 |
| Male | 159,139 (56.2%) | 83,636 (75.4%) | 75,503 (43.8%) | <0.001 |
| Body mass index, kg/m2 | 23.7 ± 2.9 | 25.8 ± 2.6 | 22.3 ± 2.2 | <0.001 |
| Waist circumference, cm | 81.4 ± 8.4 | 88.1 ± 6.3 | 77.1 ± 6.5 | <0.001 |
| Systolic blood pressure, mmHg | 125.1 ± 15.5 | 129.3 ± 15.0 | 122.4 ± 15.1 | <0.001 |
| Diastolic blood pressure, mmHg | 77.6 ± 10.1 | 80.4 ± 9.9 | 75.8 ± 9.8 | <0.001 |
| Diabetes | 25,109 (8.9%) | 13,927 (12.6%) | 11,182 (6.5%) | <0.001 |
| Hypertension | 66,676 (23.6%) | 35,311 (31.9%) | 31,365 (18.2%) | <0.001 |
| Dyslipidemia | 16,341 (5.8%) | 8005 (7.2%) | 8336 (4.8%) | <0.001 |
| Smoking | <0.001 | |||
| Non-smoker | 175,678 (62.1%) | 52,159 (47.0%) | 123,519 (71.7%) | |
| Ex-smoker | 53,584 (18.9%) | 29,050 (26.2%) | 24,534 (14.2%) | |
| Current smoker | 53,826 (19.0%) | 29,654 (26.7%) | 24,172 (14.0%) | |
| Alcohol consumption | <0.001 | |||
| None | 155,868 (55.1%) | 43,996 (39.7%) | 111,872 (65.0%) | |
| Mild | 70,870 (25.0%) | 29,792 (26.9%) | 41,078 (23.9%) | |
| Moderate | 23,205 (8.2%) | 13,995 (12.6%) | 9210 (5.3%) | |
| Heavy drinker | 33,145 (11.7%) | 23,080 (20.8%) | 10,065 (5.8%) | |
| Regular exercise | 151,854 (53.6%) | 61,999 (55.9%) | 89,855 (52.2%) | <0.001 |
| Total cholesterol, mg/dL | 200.7 ± 37.0 | 205.4 ± 38.9 | 197.6 ± 35.4 | <0.001 |
| HDL cholesterol, mg/dL | 55.0 ± 24.7 | 51.3 ± 26.3 | 57.4 ± 23.3 | <0.001 |
| LDL cholesterol, mg/dL | 118.9 ± 36.7 | 116.9 ± 39.8 | 120.2 ± 34.5 | <0.001 |
| Triglyceride, mg/dL | 139.4 ± 91.1 | 195.8 ± 111.1 | 103.2 ± 48.2 | <0.001 |
| Fatty liver index | 28.8 ± 23.0 | 53.0 ± 17.2 | 13.2 ± 7.8 | <0.001 |
| Hepatic steatosis index | 31.9 ± 4.3 | 34.9 ± 4.3 | 30.1 ± 3.2 | <0.001 |
| Follow-up period (days) | 1104.1 ± 672.5 | 1111.6 ± 666.9 | 1093.2 ± 680.5 | 0.428 |
| Total | MAFLD | Control | p-Value * | |
|---|---|---|---|---|
| (n = 283,088) | (n = 110,863) | (n = 172,225) | ||
| Outcome: hepatocellular carcinoma | ||||
| Total follow-up (day) | 1813.1 ± 124.9 | 1808.8 ± 143.3 | 1815.9 ± 111.4 | <0.001 |
| Event (n) | 2903 (1.0%) | 1723 (1.6%) | 1180 (0.7%) | <0.001 |
| Time to event (day) | 1104.1 ± 672.5 | 1111.6 ± 666.9 | 1093.2 ± 680.5 | 0.43 |
| Outcome: cardiovascular disease | ||||
| Total follow-up (day) | 1758.3 ± 282.1 | 1747.4 ± 303.2 | 1765.4 ± 267.5 | <0.001 |
| Event (n) | 18,984 (6.7%) | 8688 (7.8%) | 10,296 (6.0%) | <0.001 |
| Time to event (day) | 1063.1 ± 670.4 | 1053.2 ± 668.7 | 1071.3 ± 671.7 | 0.04 |
| Group | Non-Smoker | Ex-Smoker | Current Smoker | |
|---|---|---|---|---|
| Total | Total, no. | 175,678 | 53,584 | 53,826 |
| Events, no. | 1519 | 670 | 714 | |
| Person-years | 873,465 | 265,865 | 266,901 | |
| Adjusted * HR | 1 (ref) | 1.11 (1.00–1.24) | 1.21 (1.09–1.35) | |
| MAFLD | Total, no. | 52,159 | 29,050 | 29,654 |
| Events, no. | 745 | 451 | 527 | |
| Person-years | 258,616 | 144,007 | 146,767 | |
| Adjusted * HR | 1 (ref) | 1.04 (0.91–1.19) | 1.24 (1.08–1.41) | |
| Control | Total, no. | 123,519 | 24,534 | 24,172 |
| Events, no. | 774 | 219 | 187 | |
| Person-years | 614,849 | 121,858 | 120,134 | |
| Adjusted * HR | 1 (ref) | 1.18 (0.99–1.42) | 1.07 (0.89–1.30) | |
| Subgroup: liver cirrhosis | Total, no. | 166 | 126 | 156 |
| Events, no. | 17 | 11 | 17 | |
| Person-years | 792 | 597 | 720 | |
| Adjusted * HR | 1 (ref) | 0.89 (0.40–1.99) | 1.25 (0.59–2.64) |
| Group | Non-Smoker | Ex-Smoker | Current Smoker | |
|---|---|---|---|---|
| Total | Total, no. | 175,678 | 53,584 | 53,826 |
| Events, no. | 11,994 | 3240 | 3750 | |
| Person-years | 845,810 | 259,027 | 258,893 | |
| Adjusted * HR | 1 (ref) | 0.95 (0.91–1.00) | 1.24 (1.19–1.30) | |
| MAFLD | Total, no. | 52,159 | 29,050 | 29,654 |
| Events, no. | 4583 | 1860 | 2245 | |
| Person-years | 248,422 | 140,148 | 142,167 | |
| Adjusted * HR | 1 (ref) | 0.92 (0.86–0.97) | 1.22 (1.15–1.30) | |
| Control | Total, no. | 123,519 | 24,534 | 24,172 |
| Events, no. | 7411 | 1380 | 1505 | |
| Person-years | 597,388 | 118,880 | 116,726 | |
| Adjusted * HR | 1 (ref) | 0.96 (0.90–1.03) | 1.21 (1.13–1.29) | |
| Subgroup: liver cirrhosis | Total, no. | 166 | 126 | 156 |
| Events, no. | 15 | 8 | 19 | |
| Person-years | 782 | 595 | 724 | |
| Adjusted * HR | 1 (ref) | 0.84 (0.34–2.11) | 1.79 (0.83–3.88) |
| Total | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| Outcome | Model | Smoking | Adjusted HR | p | Adjusted HR | p | Adjusted HR | p |
| HCC | Model 1 * | Smoking (−) | 1 (ref) | 1 (ref) | 1 (ref) | |||
| Smoking (+) | 1.17 (1.06–1.28) | 0.001 | 1.05 (0.93–1.18) | 0.43 | 1.09 (0.64–1.86) | 0.75 | ||
| Model 2 † | Smoking (−) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Smoking (+) | 1.12 (1.00–1.25) | 0.056 | 1.14 (1.01–1.28) | 0.03 | 1.10 (0.64–1.87) | 0.74 | ||
| Model 3 § | Smoking (−) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Smoking (+) | 1.14 (1.02–1.28) | 0.02 | 1.14 (1.02–1.29) | 0.03 | 1.23 (0.72–2.12) | 0.45 | ||
| CVD | Model 1 * | Smoking (−) | 1 (ref) | 1 (ref) | 1 (ref) | |||
| Smoking (+) | 0.79 (0.76–0.82) | <0.001 | 0.86 (0.82–0.91) | <0.001 | 1.28 (1.07–1.54) | 0.008 | ||
| Model 2 † | Smoking (−) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Smoking (+) | 1.06 (1.01–1.12) | 0.03 | 1.05 (0.99–1.11) | 0.08 | 1.32 (1.10–1.58) | 0.003 | ||
| Model 3 § | Smoking (−) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Smoking (+) | 1.08 (1.03–1.14) | 0.003 | 1.08 (1.02–1.14) | 0.009 | 1.34 (1.11–1.61) | 0.002 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, J.-J.; Park, M.Y.; Cho, E.J.; Yu, S.J.; Kim, S.G.; Kim, Y.J.; Kim, Y.S.; Yoon, J.-H. Smoking Increases the Risk of Hepatocellular Carcinoma and Cardiovascular Disease in Patients with Metabolic-Associated Fatty Liver Disease. J. Clin. Med. 2023, 12, 3336. https://doi.org/10.3390/jcm12093336
Yoo J-J, Park MY, Cho EJ, Yu SJ, Kim SG, Kim YJ, Kim YS, Yoon J-H. Smoking Increases the Risk of Hepatocellular Carcinoma and Cardiovascular Disease in Patients with Metabolic-Associated Fatty Liver Disease. Journal of Clinical Medicine. 2023; 12(9):3336. https://doi.org/10.3390/jcm12093336
Chicago/Turabian StyleYoo, Jeong-Ju, Man Young Park, Eun Ju Cho, Su Jong Yu, Sang Gyune Kim, Yoon Jun Kim, Young Seok Kim, and Jung-Hwan Yoon. 2023. "Smoking Increases the Risk of Hepatocellular Carcinoma and Cardiovascular Disease in Patients with Metabolic-Associated Fatty Liver Disease" Journal of Clinical Medicine 12, no. 9: 3336. https://doi.org/10.3390/jcm12093336
APA StyleYoo, J. -J., Park, M. Y., Cho, E. J., Yu, S. J., Kim, S. G., Kim, Y. J., Kim, Y. S., & Yoon, J. -H. (2023). Smoking Increases the Risk of Hepatocellular Carcinoma and Cardiovascular Disease in Patients with Metabolic-Associated Fatty Liver Disease. Journal of Clinical Medicine, 12(9), 3336. https://doi.org/10.3390/jcm12093336