


Combined Prognostic Value of Preprocedural Protein–Energy Wasting and Inflammation Status for Amputation and/or Mortality after Lower-Extremity Revascularization in Hemodialysis Patients with Peripheral Arterial Disease
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. GNRI and CRP Measurements
2.3. Follow-Up
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Predictive Value of the GNRI and CRP
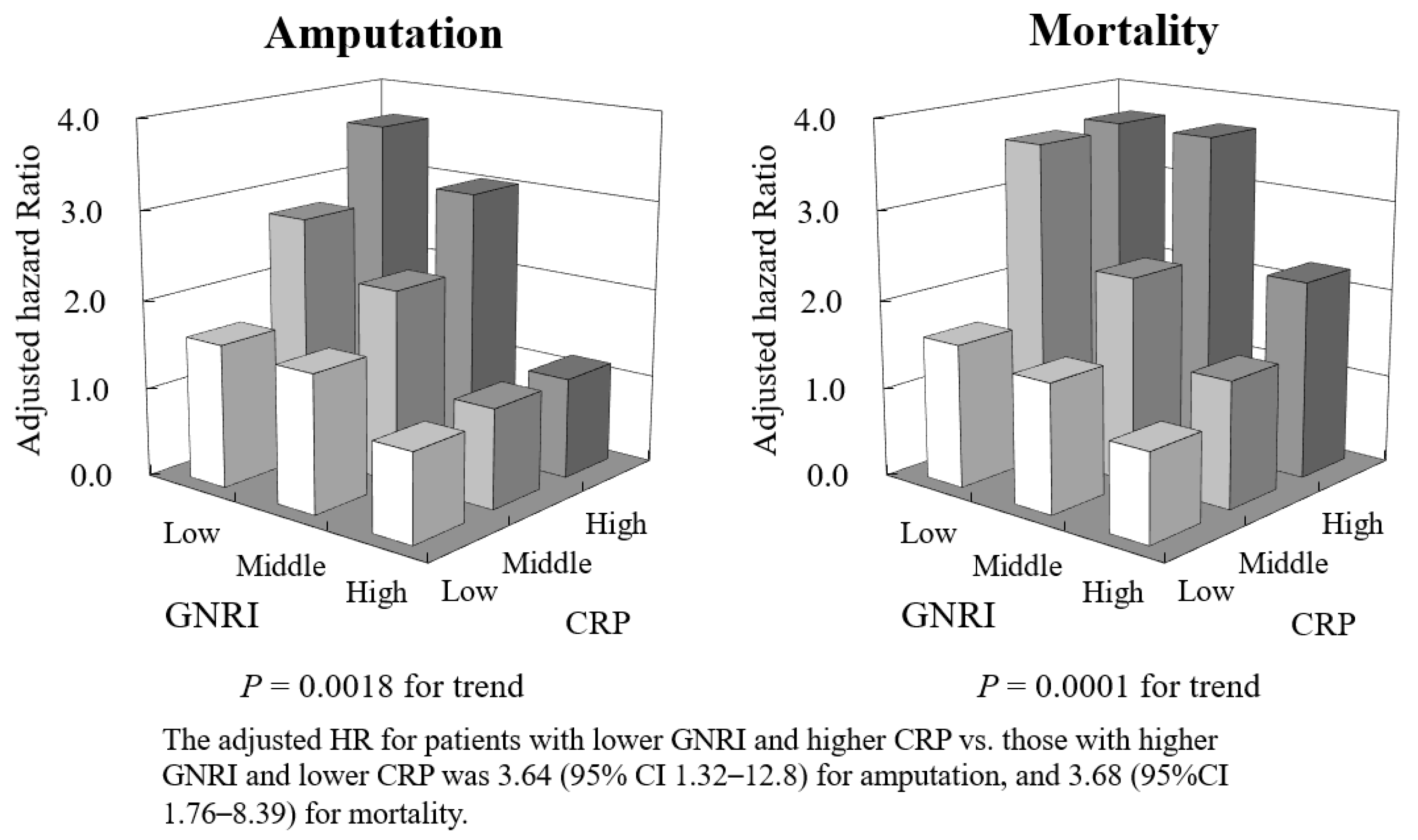
3.3. Combined Predictive Value of the GNRI and CRP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [PubMed]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016—40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef]
- Mok, Y.; Ballew, S.H.; Matsushita, K. Prognostic Value of Chronic Kidney Disease Measures in Patients with Cardiac Disease. Circ. J. 2017, 81, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, K.; Sang, Y.; Chen, J.; Ballew, S.H.; Shlipak, M.; Coresh, J.; Peralta, C.A.; Woodward, M. Novel “Predictor Patch” Method for Adding Predictors Using Estimates from Outside Datasets—A Proof-of-Concept Study Adding Kidney Measures to Cardiovascular Mortality Prediction. Circ. J. 2019, 83, 1876–1882. [Google Scholar] [CrossRef] [PubMed]
- Kai, T.; Oka, S.; Hoshino, K.; Watanabe, K.; Nakamura, J.; Abe, M.; Watanabe, A. Renal Dysfunction as a Predictor of Slow-Flow/No-Reflow Phenomenon and Impaired ST Segment Resolution After Percutaneous Coronary Intervention in ST-Elevation Myocardial Infarction with Initial Thrombolysis in Myocardial Infarction Grade 0. Circ. J. 2021, 85, 1770–1778. [Google Scholar] [CrossRef] [PubMed]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in cardiovas-cular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Dellegrottaglie, S.; Furniss, A.L.; Gillespie, B.W.; Satayathum, S.; Lameire, N.; Saito, A.; Akiba, T.; Jadoul, M.; Ginsberg, N.; et al. Peripheral arterial disease in patients with end-stage renal disease: Observations from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Circulation 2006, 114, 1914–1922. [Google Scholar] [CrossRef]
- Morooka, H.; Tanaka, A.; Inaguma, D.; Maruyama, S. Peripheral artery disease at the time of dialysis initiation and mortality: A prospective observational multicenter study. BMJ Open 2020, 10, e042315. [Google Scholar] [CrossRef]
- Owens, C.D.; Ho, K.J.; Kim, S.; Schanzer, A.; Lin, J.; Matros, E.; Belkin, M.; Conte, M.S. Refinement of survival prediction in patients undergoing lower extremity bypass surgery: Stratification by chronic kidney disease classification. J. Vasc. Surg. 2007, 45, 944–952. [Google Scholar] [CrossRef]
- Schanzer, A.; Mega, J.; Meadows, J.; Samson, R.H.; Bandyk, D.F.; Conte, M.S. Risk stratification in critical limb ischemia: Derivation and validation of a model to predict amputation-free survival using multicenter surgical outcomes data. J. Vasc. Surg. 2008, 48, 1464–1471. [Google Scholar] [CrossRef] [PubMed]
- Conrad, M.F.; Kang, J.; Cambria, R.P.; Brewster, D.C.; Watkins, M.T.; Kwolek, C.J.; LaMuraglia, G.M. Infrapopliteal balloon angioplasty for the treatment of chronic occlusive disease. J. Vasc. Surg. 2009, 50, 799–805.e4. [Google Scholar] [CrossRef] [PubMed]
- Aulivola, B.; Gargiulo, M.; Bessoni, M.; Rumolo, A.; Stella, A. Infrapopliteal angioplasty for limb salvage in the setting of renal failure: Do results justify its use? Ann. Vasc. Surg. 2005, 19, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Baldwin, M.; Cornwall, J.; Marin, M.; Faries, P.; Vouyouka, A. Contemporary outcomes of surgical revascularization of the lower extremity in patients on dialysis. J. Vasc. Surg. 2017, 66, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Ambur, V.; Park, P.; Gaughan, J.P.; Golarz, S.; Schmieder, F.; Van Bemmelen, P.; Choi, E.; Dhanisetty, R. The impact of chronic kidney disease on lower extremity bypass outcomes in patients with critical limb ischemia. J. Vasc. Surg. 2019, 69, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.B.; Telles-Garcia, N.A.; Atkins, J.L.; Mina, G.S.; Abreo, A.P.; Virk, C.S.; Dominic, P.S. End-stage renal disease patients un-dergoing angioplasty and bypass for critical limb ischemia have worse outcomes compared to non-ESRD patients: Systematic review and meta-analysis. Catheter. Cardiovasc. Interv. 2021, 98, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Gkremoutis, A.; Bisdas, T.; Torsello, G.; Schmitz-Rixen, T.; Tsilimparis, N.; Stavroulakis, K.; Collaborators, C. Early outcomes of patients with chronic kidney disease after revascularization for critical limb ischemia. J. Cardiovasc. Surg. 2021, 62, 104–110. [Google Scholar] [CrossRef]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein–energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef]
- Ishida, J.; Kato, A. Recent Advances in the Nutritional Screening, Assessment, and Treatment of Japanese Patients on Hemodialysis. J. Clin. Med. 2023, 12, 2113. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cederholm, T.; Avesani, C.M.; Bakker, S.J.; Bellizzi, V.; Cuerda, C.; Cupisti, A.; Sabatino, A.; Schneider, S.; Torreggiani, M.; et al. Nutritional status and the risk of malnutrition in older adults with chronic kidney disease—implications for low protein intake and nutritional care: A critical review endorsed by ERN-ERA and ESPEN. Clin. Nutr. 2023, 42, 443–457. [Google Scholar] [CrossRef]
- Kopple, J.D. McCollum Award Lecture, 1996, protein-energy malnutrition in maintenance dialysis patients. Am. J. Clin. Nutr. 1997, 65, 1544–1557. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Ito, Y.; Ishii, H.; Aoyama, T.; Kamoi, D.; Kasuga, H.; Yasuda, K.; Maruyama, S.; Matsuo, S.; Murohara, T.; et al. Geriatric nutritional risk index accurately predicts cardio-vascular mortality in incident hemodialysis patients. J. Cardiol. 2014, 64, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Hanna, R.M.; Ghobry, L.; Wassef, O.; Rhee, C.M.; Kalantar-Zadeh, K. A Practical Approach to Nutrition, Protein-Energy Wasting, Sarcopenia, and Cachexia in Patients with Chronic Kidney Disease. Blood Purif. 2020, 49, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, M.; Cobo, G.; Lindholm, B.; Stenvinkel, P. Inflammation and Protein-Energy Wasting in the Uremic Milieu. Contrib. Nephrol. 2017, 191, 58–71. [Google Scholar] [PubMed]
- Cobo, G.; Lindholm, B.; Stenvinkel, P. Chronic inflammation in end-stage renal disease and dialysis. Nephrol. Dial. Transplant. 2018, 33 (Suppl. S3), iii35–iii40. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, R.; Ito, Y.; Takahashi, H.; Ishii, H.; Kasuga, H.; Mizuno, M.; Suzuki, Y.; Yuzawa, Y.; Maruyama, S.; Murohara, T.; et al. Combined Values of Serum Albumin, C-Reactive Protein and Body Mass Index at Dialysis Initiation Accurately Predicts Long-Term Mortality. Am. J. Nephrol. 2012, 36, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Ishii, H.; Takahashi, H.; Ito, Y.; Aoyama, T.; Kamoi, D.; Sakakibara, T.; Umemoto, N.; Kumada, Y.; Suzuki, S.; Murohara, T. The Association of Ankle Brachial Index, Protein-Energy Wasting, and Inflammation Status with Cardiovascular Mortality in Patients on Chronic Hemodialysis. Nutrients 2017, 9, 416. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.-P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Takahashi, H.; Inoue, K.; Shimizu, K.; Hiraga, K.; Takahashi, E.; Otaki, K.; Yoshikawa, T.; Furuta, K.; Tokunaga, C.; Sakakibara, T.; et al. Comparison of Nutritional Risk Scores for Predicting Mortality in Japanese Chronic Hemodialysis Patients. J. Ren. Nutr. 2017, 27, 201–206. [Google Scholar] [CrossRef]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [CrossRef]
- Conte, M.S.; Geraghty, P.J.; Bradbury, A.W.; Hevelone, N.D.; Lipsitz, S.R.; Moneta, G.L.; Nehler, M.R.; Powell, R.J.; Sidawy, A.N. Suggested objective performance goals and clinical trial design for evaluating catheter-based treatment of critical limb ischemia. J. Vasc. Surg. 2009, 50, 1462–1473. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172; discussion 207–212. [Google Scholar] [CrossRef] [PubMed]
- Kumada, Y.; Kawai, N.; Ishida, N.; Mori, A.; Ishii, H.; Ohshima, S.; Ito, R.; Umemoto, N.; Takahashi, H.; Murohara, T. Impact of Hemodialysis on Clinical Outcomes in Patients Undergoing Lower Extremity Bypass Surgery for Peripheral Artery Disease—10-year Follow-Up Study. Angiology 2022, 73, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Kumada, Y.; Nogaki, H.; Ishii, H.; Aoyama, T.; Kamoi, D.; Takahashi, H.; Murohara, T. Clinical outcome after infrapopliteal bypass surgery in chronic hemodialysis patients with critical limb ischemia. J. Vasc. Surg. 2015, 61, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.L., Sr.; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G. Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk stratification based on Wound, Ischemia, and foot Infection (WIfI). J. Vasc. Surg. 2014, 59, 220–234.e2. [Google Scholar] [CrossRef] [PubMed]
- Ono, K.; Tsuchida, A.; Kawai, H.; Matsuo, H.; Wakamatsu, R.; Maezawa, A.; Yano, S.; Kawada, T.; Nojima, Y. Ankle-brachial blood pressure index predicts all-cause and cardiovascular mortality in hemodialysis patients. J. Am. Soc. Nephrol. 2003, 14, 1591–1598. [Google Scholar] [CrossRef]
- Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W., Jr.; Kemper, A.R.; Kubik, M.; et al. Screening for Peripheral Artery Disease and Cardiovascular Disease Risk Assessment with the Ankle-Brachial Index: US Preventive Services Task Force Recommendation Statement. US Preventive Services Task Force. JAMA 2018, 320, 177–183. [Google Scholar]
- Sekikawa, A.; Ueshima, H.; Kadowaki, T.; El-Saed, A.; Okamura, T.; Takamiya, T.; Kashiwagi, A.; Edmundowicz, D.; Murata, K.; Sutton-Tyrrell, K.; et al. Less Subclinical Atherosclerosis in Japanese Men in Japan than in White Men in the United States in the Post-World War II Birth Cohort. Am. J. Epidemiol. 2007, 165, 617–624. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GNRI | |||||
|---|---|---|---|---|---|
| All Patients (n = 800) | <88.1 (n = 269) | 88.1–96.7 (n = 264) | >96.7 (n = 267) | p Value | |
| Male gender (%) | 66.9 | 62.5 | 67.4 | 70.7 | 0.12 |
| Age (years) | 67 ± 10 | 69 ± 10 | 67 ± 9 | 66 ± 10 | 0.0024 |
| Diabetes (%) | 63.3 | 63.2 | 64.7 | 61.8 | 0.78 |
| Hypertension (%) | 62.1 | 58.0 | 61.7 | 66.7 | 0.12 |
| Dyslipidemia (%) | 24.5 | 18.2 | 25.8 | 29.6 | 0.0076 |
| Smoking (%) | 25.7 | 18.6 | 31.4 | 27.2 | 0.0078 |
| Body mass index (kg/m2) | 21.2 ± 3.3 | 19.2 ± 2.9 | 21.0 ± 2.6 | 23.3 ± 3.0 | <0.0001 |
| Coronary artery disease (%) | 63.5 | 58.7 | 63.9 | 67.8 | 0.092 |
| Stroke (%) | 16.9 | 18.6 | 15.5 | 16.5 | 0.63 |
| Indications (%) | <0.0001 | ||||
| Claudication | 47.1 | 36.8 | 43.9 | 60.4 | |
| Rest pain | 12.3 | 13.6 | 11.5 | 11.9 | |
| Ulcer/gangrene | 40.6 | 49.6 | 44.6 | 27.7 | |
| GNRI | 92.0 ± 9.8 | 81.4 ± 5.8 | 92.3 ± 2.4 | 102.4 ± 5.3 | <0.0001 |
| CRP (mg/L) | 5.1 (2.0–20.0) | 11.3 (2.9–44.5) | 4.0 (1.0–14.0) | 3.0 (1.0–12.0) | <0.0001 |
| Preprocedural ABI | 0.62 (0.45–0.79) | 0.65 (0.41–0.87) | 0.57 (0.44–0.79) | 0.64 (0.49–0.77) | 0.35 |
| Procedure (%) | <0.0001 | ||||
| Bypass surgery | 33.1 | 38.7 | 39.8 | 21.0 | |
| Endovascular therapy | 66.9 | 61.3 | 60.2 | 79.0 | |
| Number of lesions | 825 | 282 | 271 | 272 | |
| Target artery (%) | <0.0001 | ||||
| Iliac | 18.1 | 22.7 | 17.6 | 14.3 | |
| Femoropopliteal | 62.1 | 52.8 | 59.1 | 72.8 | |
| Below-knee | 21.3 | 24.5 | 23.3 | 12.9 | |
| Serum CRP | ||||
|---|---|---|---|---|
| <2.0 mg/L (n = 270) | 2.0–12.6 mg/L (n = 266) | >12.6 mg/L (n = 264) | p Value | |
| Male gender (%) | 62.6 | 69.2 | 68.9 | 0.19 |
| Age (years) | 66 ± 10 | 67 ± 10 | 69 ± 10 | 0.046 |
| Diabetes (%) | 60.4 | 60.9 | 63.3 | 0.091 |
| Hypertension (%) | 63.7 | 61.7 | 61.0 | 0.80 |
| Dyslipidemia (%) | 25.9 | 24.8 | 22.7 | 0.68 |
| Smoking (%) | 27.5 | 24.8 | 24.9 | 0.75 |
| Body mass index (kg/m2) | 20.9 ± 3.1 | 21.2 ± 3.0 | 21.5 ± 3.7 | 0.15 |
| Coronary artery disease (%) | 63.2 | 65.0 | 63.5 | 0.78 |
| Stroke (%) | 18.6 | 18.4 | 13.6 | 0.22 |
| Indications (%) | <0.0001 | |||
| Claudication | 61.9 | 49.6 | 29.6 | |
| Rest pain | 14.6 | 15.9 | 6.5 | |
| Ulcer/gangrene | 23.5 | 34.5 | 63.9 | |
| GNRI | 94.3 ± 9.4 | 93.1 ± 9.7 | 89.1 ± 10.1 | <0.0001 |
| CRP (mg/L) | 1.0 (1.0–2.0) | 5.9 (3.9–8.0) | 39.5 (20.0–70.0) | <0.0001 |
| Preprocedural ABI | 0.65 (0.47–0.79) | 0.63 (0.44–0.82) | 0.57 (0.43–0.76) | 0.23 |
| Procedure (%) | <0.0001 | |||
| Bypass surgery | 22.2 | 30.5 | 47.0 | |
| Endovascular therapy | 77.8 | 69.5 | 53.0 | |
| Number of lesions | 274 | 271 | 280 | |
| Target artery (%) | <0.0001 | |||
| Iliac | 22.3 | 18.5 | 13.6 | |
| Femoropopliteal | 69.7 | 64.6 | 52.1 | |
| Below-knee | 8.0 | 17.0 | 34.3 | |
| Non-Adjusted | Adjusted ** | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Amputation or death | ||||
| GNRI (vs. T3) | <0.0001 * | 0.0070 * | ||
| T2 | 1.46 (1.03–2.09) | 0.031 | 1.42 (0.97–2.09) | 0.070 |
| T1 | 2.18 (1.57–3.07) | <0.0001 | 1.78 (1.24–2.59) | 0.0016 |
| CRP (vs. T1) | <0.0001 * | 0.0026 * | ||
| T2 | 1.32 (0.93–1.89) | 0.11 | 130 (0.90–1.91) | 0.15 |
| T3 | 2.33 (1.67–3.27) | <0.0001 | 1.86 (1.30–2.70) | 0.0007 |
| Amputation | ||||
| GNRI (vs. T3) | <0.0001 * | 0.032 * | ||
| T2 | 1.11 (0.78–2.44) | 0.79 | 1.05 (0.46–2.39) | 0.89 |
| T1 | 3.17 (1.70–6.37) | 0.0002 | 2.01 (1.04–4.12) | 0.034 |
| CRP (vs. T1) | 0.0003 * | 0.045 * | ||
| T2 | 1.26 (0.58–2.79) | 0.54 | 1.01 (0.45–2.23) | 0.98 |
| T3 | 3.35 (1.75–6.85) | 0.0001 | 2.02 (1.02–4.25) | 0.042 |
| Mortality | ||||
| GNRI (vs. T3) | 0.0002 * | 0.0083 * | ||
| T2 | 1.51 (1.03–2.23) | 0.032 | 1.51 (0.99–2.33) | 0.052 |
| T1 | 2.12 (1.48–3.09) | <0.0001 | 1.87 (1.25–2.84) | 0.0020 |
| CRP (vs. T1) | 0.0004 * | 0.043 * | ||
| T2 | 1.30 (0.89–1.90) | 0.17 | 1.29 (0.86–1.94) | 0.20 |
| T3 | 2.03 (1.42–2.93) | <0.0001 | 1.64 (1.11–2.45) | 0.012 |
| C-Index (95% CI) | p Value | NRI | p Value | IDI | p Value | |
|---|---|---|---|---|---|---|
| Established risk factors * | 0.661 | reference | reference | reference | ||
| +GNRI | 0.710 | 0.0060 | 0.456 | <0.0001 | 0.037 | <0.0001 |
| +CRP | 0.681 | 0.0034 | 0.217 | 0.0063 | 0.014 | 0.0001 |
| +GNRI and CRP | 0.716 | 0.0021 | 0.508 | <0.0001 | 0.042 | <0.0001 |
| +GNRI and CRP vs. +GNRI | 0.006 ** | 0.047 | 0.145 | 0.047 | 0.006 | 0.035 |
| +GNRI and CRP vs. +CRP | 0.035 ** | 0.038 | 0.427 | <0.0001 | 0.029 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumada, Y.; Kawai, N.; Ishida, N.; Nakamura, Y.; Takahashi, H.; Ohshima, S.; Ito, R.; Izawa, H.; Murohara, T.; Ishii, H. Combined Prognostic Value of Preprocedural Protein–Energy Wasting and Inflammation Status for Amputation and/or Mortality after Lower-Extremity Revascularization in Hemodialysis Patients with Peripheral Arterial Disease. J. Clin. Med. 2024, 13, 126. https://doi.org/10.3390/jcm13010126
Kumada Y, Kawai N, Ishida N, Nakamura Y, Takahashi H, Ohshima S, Ito R, Izawa H, Murohara T, Ishii H. Combined Prognostic Value of Preprocedural Protein–Energy Wasting and Inflammation Status for Amputation and/or Mortality after Lower-Extremity Revascularization in Hemodialysis Patients with Peripheral Arterial Disease. Journal of Clinical Medicine. 2024; 13(1):126. https://doi.org/10.3390/jcm13010126
Chicago/Turabian StyleKumada, Yoshitaka, Norikazu Kawai, Narihiro Ishida, Yasuhito Nakamura, Hiroshi Takahashi, Satoru Ohshima, Ryuta Ito, Hideo Izawa, Toyoaki Murohara, and Hideki Ishii. 2024. "Combined Prognostic Value of Preprocedural Protein–Energy Wasting and Inflammation Status for Amputation and/or Mortality after Lower-Extremity Revascularization in Hemodialysis Patients with Peripheral Arterial Disease" Journal of Clinical Medicine 13, no. 1: 126. https://doi.org/10.3390/jcm13010126
APA StyleKumada, Y., Kawai, N., Ishida, N., Nakamura, Y., Takahashi, H., Ohshima, S., Ito, R., Izawa, H., Murohara, T., & Ishii, H. (2024). Combined Prognostic Value of Preprocedural Protein–Energy Wasting and Inflammation Status for Amputation and/or Mortality after Lower-Extremity Revascularization in Hemodialysis Patients with Peripheral Arterial Disease. Journal of Clinical Medicine, 13(1), 126. https://doi.org/10.3390/jcm13010126