

Intradialytic Tolerance and Recovery Time in Different High-Efficiency Hemodialysis Modalities

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Dialysis Prescription and Equipment
2.4. Outcomes
2.4.1. Adverse Events
2.4.2. Dialysis Recovery Time
- i.
- Answers given in minutes were recorded directly.
- ii.
- Answers in hours were multiplied by 60.
- iii.
- Variants of “half a day”, including the “next day”, were given a value of 720 min.
- iv.
- Variants of “one day” were given a value of 1440 min.
- v.
- Variants of “more than a day” were given a value of 2160 min (36 h).
2.4.3. Hemodynamic Monitoring
2.4.4. Hydration State
2.5. Statistics
3. Results
3.1. Characteristics of Patients
3.2. Dialysis Parameters
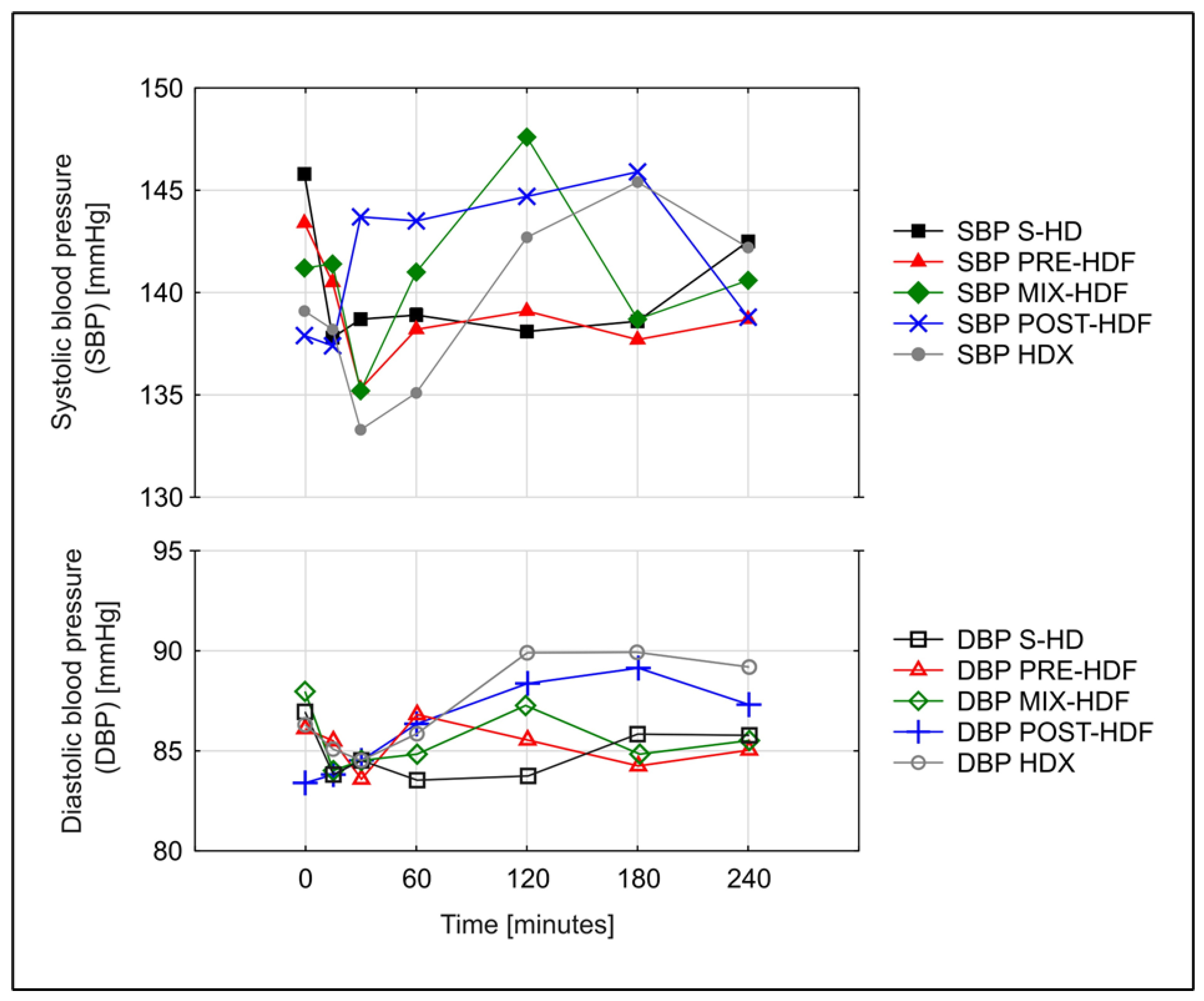
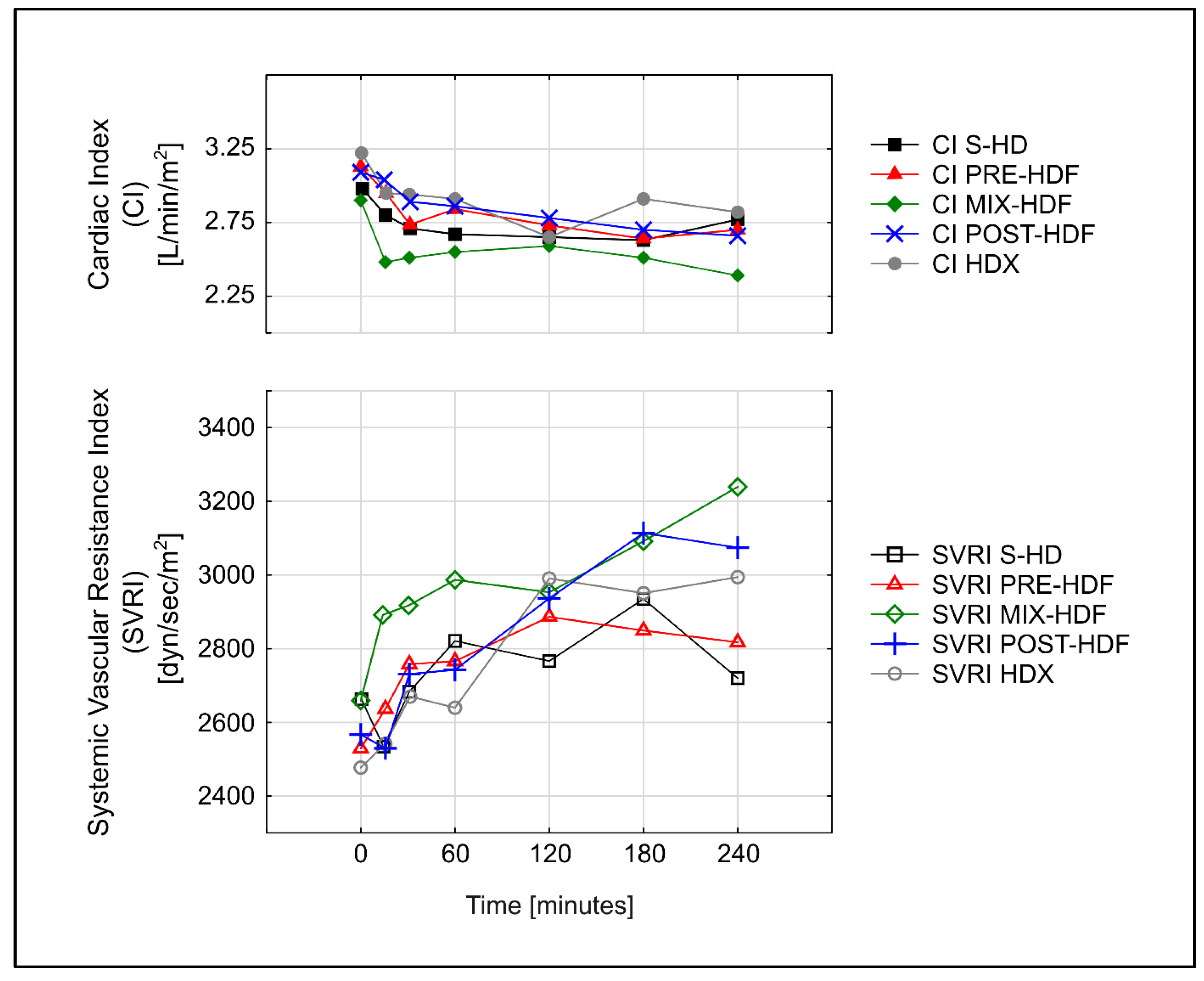
3.3. Hemodynamic Parameters
3.4. Adverse Events and Dialysis Recovery Time
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lang, T.; Zawada, A.M.; Theis, L.; Braun, J.; Ottillinger, B.; Kopperschmidt, P.; Gagel, A.; Kotanko, P.; Stauss-Grabo, M.; Kennedy, J.P.; et al. Hemodiafiltration: Technical and Medical Insights. Bioengineering 2023, 10, 145. [Google Scholar] [CrossRef] [PubMed]
- Pedreros-Rosales, C.; Jara, A.; Lorca, E.; Mezzano, S.; Pecoits-Filho, R.; Herrera, P. Unveiling the Clinical Benefits of High-Volume Hemodiafiltration: Optimizing the Removal of Medium-Weight Uremic Toxins and Beyond. Toxins 2023, 15, 531. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Yang, T.; Li, Y.; Li, J.; Yang, Q.; Wang, L.; Jiang, L.; Su, B. Effects of Expanded Hemodialysis with Medium Cut-Off Membranes on Maintenance Hemodialysis Patients: A Review. Membranes 2022, 12, 253. [Google Scholar] [CrossRef] [PubMed]
- Davenport, A.; Peters, S.A.; Bots, M.L.; Canaud, B.; Grooteman, M.P.; Asci, G.; Locatelli, F.; Maduell, F.; Morena, M.; Nubé, M.J.; et al. Higher convection volume exchange with online hemodiafiltration is associated with survival advantage for dialysis patients: The effect of adjustment for body size. Kidney Int. 2016, 89, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, K.; Hamano, T.; Wada, A.; Nakai, S.; Masakane, I. Predilution online hemodiafiltration is associated with improved survival compared with hemodialysis. Kidney Int. 2019, 95, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Blankestijn, P.J.; Vernooij, R.W.M.; Hockham, C.; Strippoli, G.F.M.; Canaud, B.; Hegbrant, J.; Barth, C.; Covic, A.; Cromm, K.; Cucui, A.; et al. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. N. Engl. J. Med. 2023, 389, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Nielsen, L.; Gendrot, L.; Fois, A.; Cataldo, E.; Cabiddu, G. Prescribing Hemodialysis or Hemodiafiltration: When One Size Does Not Fit All the Proposal of a Personalized Approach Based on Comorbidity and Nutritional Status. J. Clin. Med. 2018, 7, 331. [Google Scholar] [CrossRef]
- Zawierucha, J.; Małyszko, J.; Dębska-Ślizień, A.; Durlik, M.; Krajewska, M.; Chmiel, G.; Ciechanowski, K.; Klinger, M.; Małyszko, J.; Nowicki, M.; et al. Expert panel position statement on indication for hemodiafiltration (hdf) therapy in end stage renal disease patients. Nefrol. Dial. Pol. 2018, 22, 9–12. [Google Scholar]
- Schiffl, H. Online hemodiafiltration and mortality risk in end-stage renal disease patients: A critical appraisal of current evidence. Kidney Res. Clin. Pract. 2019, 38, 159–168. [Google Scholar] [CrossRef]
- Marcelli, D.; Scholz, C.; Ponce, P.; Sousa, T.; Kopperschmidt, P.; Grassmann, A.; Pinto, B.; Canaud, B. High-Volume Postdilution Hemodiafiltration Is a Feasible Option in Routine Clinical Practice. Artif. Organs 2015, 39, 142–149. [Google Scholar] [CrossRef]
- Smith, J.R.; Zimmer, N.; Bell, E.; Francq, B.G.; McConnachie, A.; Mactier, R. A Randomized, Single-Blind, Crossover Trial of Recovery Time in High-Flux Hemodialysis and Hemodiafiltration. Am. J. Kidney Dis. 2017, 69, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, R.M.; Heidenheim, P.A.; Nesrallah, G.; Garg, A.X.; Suri, R.; on behalf of the Daily Hemodialysis Study Group London Health Sciences Centre. Minutes to Recovery after a Hemodialysis Session. Clin. J. Am. Soc. Nephrol. 2006, 1, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Scherhag, A.; Kaden, J.J.; Kentschke, E.; Sueselbeck, T.; Borggrefe, M. Comparison of Impedance Cardiography and Thermodilution-Derived Measurements of Stroke Volume and Cardiac Output at Rest and During Exercise Testing. Cardiovasc. Drugs Ther. 2005, 19, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Moissl, U.M.; Wabel, P.; Chamney, P.W.; Bosaeus, I.; Levin, N.W.; Bosy-Westphal, A.; Korth, O.; Müller, M.J.; Ellegård, L.; Malmros, V.; et al. Body fluid volume determination via body composition spectroscopy in health and disease. Physiol. Meas. 2006, 27, 921–933. [Google Scholar] [CrossRef]
- Shroff, R.; Basile, C.; van der Sande, F.; Mitra, S.; EuDial Working Group of the European Renal Association. Haemodiafiltration for all: Are we convinced? Nephrol. Dial. Transplant. 2023, 38, 2663–2665. [Google Scholar] [CrossRef]
- Merkus, M.P.; Jager, K.J.; Dekker, F.W.; Boeschoten, E.W.; Stevens, P.; Krediet, R.T. Quality of life in patients on chronic dialysis: Self-assessment 3 months after the start of treatment. Am. J. Kidney Dis. 1997, 29, 584–592. [Google Scholar] [CrossRef]
- Bello, A.K.; Okpechi, I.G.; Osman, M.A.; Cho, Y.; Htay, H.; Jha, V.; Wainstein, M.; Johnson, D.W. Epidemiology of haemodialysis outcomes. Nat. Rev. Nephrol. 2022, 18, 378–395. [Google Scholar] [CrossRef]
- Puchalska-Reglińska, E.; Dębska-Ślizień, A.; Biedunkiewicz, B.; Tylicki, P.; Polewska, K.; Jagodziński, P.; Rutkowski, B.; Gellert, R.; Tylicki, L. Extremely high mortality in COVID-19 hemodialyzed patients in before anty-SARS-CoV-2 vaccination era. The first large database from Poland. Pol. Arch. Intern. Med. 2021, 131, 643–648. [Google Scholar] [CrossRef]
- Monardo, P.; Lacquaniti, A.; Campo, S.; Bucca, M.; Casuscelli di Tocco, T.; Rovito, S.; Ragusa, A.; Santoro, A. Updates on hemodialysis techniques with a common denominator: The personalization of the dialytic therapy. Semin. Dial. 2021, 34, 183–195. [Google Scholar] [CrossRef]
- Flythe, J.E.; Dorough, A.; Narendra, J.H.; Forfang, D.; Hartwell, L.; Abdel-Rahman, E. Perspectives on symptom experiences and symptom reporting among individuals on hemodialysis. Nephrol. Dial. Transplant. 2018, 33, 1842–1852. [Google Scholar] [CrossRef]
- Caplin, B.; Alston, H.; Davenport, A. Does Online Haemodiafiltration Reduce Intra-Dialytic Patient Symptoms? Nephron. Clin. Pract. 2013, 124, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Jhamb, M.; Argyropoulos, C.; Steel, J.L.; Plantinga, L.; Wu, A.W.; Fink, N.E.; Powe, N.R.; Meyer, K.B.; Unruh, M.L.; Mark, L.; et al. Correlates and Outcomes of Fatigue among Incident Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1779–1786. [Google Scholar] [CrossRef]
- Alvarez, L.; Brown, D.; Hu, D.; Chertow, G.M.; Vassalotti, J.A.; Prichard, S. Intradialytic Symptoms and Recovery Time in Patients on Thrice-Weekly In-Center Hemodialysis: A Cross-sectional Online Survey. Radiology 2020, 2, 125–130. [Google Scholar] [CrossRef]
- Rayner, H.C.; Zepel, L.; Fuller, D.S.; Morgenstern, H.; Karaboyas, A.; Culleton, B.F.; Mapes, D.L.; Lopes, A.A.; Gillespie, B.W.; Hasegawa, T.; et al. Recovery Time, Quality of Life, and Mortality in Hemodialysis Patients: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2014, 64, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Morena, M.; Jaussent, A.; Chalabi, L.; Leray-Moragues, H.; Chenine, L.; Debure, A.; Thibaudin, D.; Azzouz, L.; Patrier, L.; Maurice, F.; et al. Treatment tolerance and patient-reported outcomes favor online hemodiafiltration compared to high-flux hemodialysis in the elderly. Kidney Int. 2017, 91, 1495–1509. [Google Scholar] [CrossRef] [PubMed]
- Schiffl, H. High-volume online haemodiafiltration treatment and outcome of end-stage renal disease patients: More than one mode. Int. Urol. Nephrol. 2020, 52, 1501–1506. [Google Scholar] [CrossRef] [PubMed]
- Maduell, F.; Moreso, F.; Pons, M.; Ramos, R.; Mora-Macià, J.; Carreras, J.; Soler, J.; Torres, F.; Campistol, J.M.; Martinez-Castelao, A.; et al. High-Efficiency Postdilution Online Hemodiafiltration Reduces All-Cause Mortality in Hemodialysis Patients. J. Am. Soc. Nephrol. 2013, 24, 487–497. [Google Scholar] [CrossRef]
- Ethier, I.; Nevis, I.; Suri, R.S. Quality of Life and Hemodynamic Effects of Switching from Hemodialysis to Hemodiafiltration: A Canadian Controlled Cohort Study. Can. J. Kidney Health Dis. 2021, 8, 1–9. [Google Scholar] [CrossRef]
- Locatelli, F.; Mastrangelo, F.; Redaelli, B.; Ronco, C.; Marcelli, D.; La Greca, G.; Orlandini, G. The Italian Cooperative Dialysis Study Group Effects of different membranes and dialysis technologies on patient treatment tolerance and nutritional parameters. Kidney Int. 1996, 50, 1293–1302. [Google Scholar] [CrossRef]
- Park, H.C.; Lee, Y.K. Who is the winner, pre-, post-, or mixed-dilution hemodiafiltration? Kidney Res. Clin. Pract. 2021, 40, 332–334. [Google Scholar] [CrossRef]
- Donauer, J.; Schweiger, C.; Rumberger, B.; Krumme, B.; Böhler, J. Reduction of hypotensive side effects during online-haemodiafiltration and low temperature haemodialysis. Nephrol. Dial. Transplant. 2003, 18, 1616–1622. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Altieri, P.; Andrulli, S.; Bolasco, P.; Sau, G.; Pedrini, L.A.; Basile, C.; David, S.; Feriani, M.; Montagna, G.; et al. Hemofiltration and Hemodiafiltration Reduce Intradialytic Hypotension in ESRD. J. Am. Soc. Nephrol. 2010, 21, 1798–1807. [Google Scholar] [CrossRef] [PubMed]
- Park, K.S.; Kang, E.W.; Chang, T.I.; Jo, W.; Park, J.T.; Yoo, T.-H.; Kang, S.-W.; Han, S.H. Mixed- versus predilution hemodiafiltration effects on convection volume and small and middle molecule clearance in hemodialysis patients: A prospective randomized controlled trial. Kidney Res. Clin. Pract. 2021, 40, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Bolton, S.; Gair, R.; Nilsson, L.-G.; Matthews, M.; Stewart, L.; McCullagh, N. Clinical Assessment of Dialysis Recovery Time and Symptom Burden: Impact of Switching Hemodialysis Therapy Mode. Patient Relat. Outcome Meas. 2021, 12, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Pongsittisak, W.; Satpanich, P.; Jaturapisanukul, S.; Keawvichit, R.; Prommool, S.; Trakranvanich, T.; Ngamvichukorn, T.; Kurathong, S. Medium Cut-Off versus Low-Flux Dialyzers in Hemodialysis Patients with COVID-19: Clinical Outcomes and Reduction in Interleukin-6. Blood Purif. 2023, 52, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Alarcon, J.C.; Bunch, A.; Ardila, F.; Zuñiga, E.; Vesga, J.I.; Rivera, A.; Sánchez, R.; Sanabria, R.M.; on behalf of the Colombian Registry of Expanded Hemodialysis Investigators. Impact of Medium Cut-Off Dialyzers on Patient-Reported Outcomes: Corexh Registry. Blood Purif. 2021, 50, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Penny, J.D.; Salerno, F.R.; Akbari, A.; McIntyre, C.W. Pruritus: Is there a grain of salty truth? Hemodial. Int. 2021, 25, E10–E14. [Google Scholar] [CrossRef]
- Jankowska, M.; Cobo, G.; Lindholm, B.; Stenvinkel, P. Inflammation and protein-energy wasting in the uremic milieu. Contrib. Nephrol. 2017, 191, 58–71. [Google Scholar] [CrossRef]
- Hadad-Arrascue, F.; Nilsson, L.G.; Rivera, A.S.; Bernardo, A.A.; Cabezuelo Romero, J.B. Expanded hemodialysis as effective alternative to on-line hemodiafiltration: A randomized mid-term clinical trial. Ther. Apher. Dial. 2022, 26, 37–44. [Google Scholar] [CrossRef]
- Kawai, Y.; Maeda, K.; Moriishi, M.; Kawanishi, H.; Masaki, T. Comparison of the pre-dilution and post-dilution methods for online hemodiafiltration. J. Artif. Organs 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Lee, Y.; Jang, M.-J.; Jeon, J.; Lee, J.E.; Huh, W.; Choi, B.S.; Park, C.W.; Chin, H.J.; Kang, C.L.; Kim, D.K.; et al. Cardiovascular Risk Comparison between Expanded Hemodialysis Using Theranova and Online Hemodiafiltration (CARTOON): A Multicenter Randomized Controlled Trial. Sci. Rep. 2021, 11, 10807. [Google Scholar] [CrossRef] [PubMed]
- Doenyas-Barak, K.; de Abreu, M.H.F.G.; Borges, L.E.; Filho, H.A.T.; Yunlin, F.; Yurong, Z.; Levin, N.W.; Kaufman, A.M.; Efrati, S.; Pereg, D.; et al. Non-invasive hemodynamic profiling of patients undergoing hemodialysis—A multicenter observational cohort study. BMC Nephrol. 2019, 20, 347. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, M.M.; Zeid, M.M.; Hamza, O.M.R.; Elkholy, N.M. Dialysis recovery time: Associated factors and its association with quality of life of hemodialysis patients. BMC Nephrol. 2022, 23, 298. [Google Scholar] [CrossRef] [PubMed]
- Davenport, A.; Guirguis, A.; Almond, M.; Day, C.; Chilcot, J.; Gane, M.D.S.; Fineberg, N.; Friedl, K.; Spencer, B.; Wellsted, D.; et al. Postdialysis recovery time is extended in patients with greater self-reported depression screening questionnaire scores. Hemodial. Int. 2018, 22, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Bossola, M.; Di Stasio, E.S.; Giungi, S.; Rosa, F.; Tazza, L. Fatigue Is Associated with Serum Interleukin-6 Levels and Symptoms of Depression in Patients on Chronic Hemodialysis. J. Pain Symptom Manag. 2015, 49, 578–585. [Google Scholar] [CrossRef]
- Yoowannakul, S.; Vongsanim, S.; Tangvoraphonkchai, K.; Davenport, A. Do patients dialysing with higher ultrafiltration rates report more intradialytic symptoms and longer postdialysis recovery times? Artif. Organs 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Vinson, A.J.; Collister, D.; Ahmed, S.; Tennankore, K. Underrepresentation of Women in Recent Landmark Kidney Trials: The Gender Gap Prevails. Kidney Int. Rep. 2022, 7, 2526–2529. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gender (men/women) | 11/1 |
| Causes of ESRD (n/%) | |
| Autosomal dominant polycystic kidney disease | 4/33.4 |
| Glomerulonephritis (primary or secondary) | 3/25.0 |
| Hypertensive nephropathy | 2/16.7 |
| Renal malformation | 1/8.3 |
| Interstitial nephropathy Other | 1/8.3 1/8.3 |
| Age (years) | 52.5 (15.5) |
| AACI (points) | 4.5 (2.2) |
| Dialysis vintage (months) | 42.5 (31.04) |
| Body mass index (kg/m2) Weight (kg) spKt/Vurea Hemoglobin (g/dL) Albumin (g/L) | 23.8 (3.6) 73.7 (14.2) 1.5 (0.3) 10.9 (0.9) 33.1 (4.9) |
| S-HD | HDX | PRE-HDF | MIX-HDF | POST-HDF | p | |
|---|---|---|---|---|---|---|
| Time min | 240 | 240 | 240 | 240 | 240 | NA |
| Blood flow mL/min | 350 | 350 | 350 | 350 | 350 | NA |
| Dialysate flow mL/min | 500 | 500 | 500 | 500 | 500 | NA |
| Ultrafiltration mL | 2.12 (0.74) | 2.33 (0.62) | 2.45 (0.8) | 2.29 (0.74) | 2.19 (0.52) | p = 0.6 |
| Ultrafiltration/dry weight % | 0.028 | 0.032 | 0.034 | 0.031 | 0.029 | p = 0.56 |
| Total convection L | NA | NA | 61.5 (7.2) | 47.1 (11.4) | 25.6 (3.8) | NA |
| SBP predialysis mmHg | 147.7 (27.5) | 144.1 (20.3) | 147.7 (26.6) | 147.3 (20.3) | 144.3 (22.4) | p = 0.95 |
| DBP predialysis mmHg | 88.5 (18.8) | 88.3 (16.9) | 89.9 (20.4) | 89.9 (16.4) | 86.1 (18.0) | p = 0.93 |
| TBW predialysis l | 39.76 (8.04) | 41.64 (11.65) | 39.05 (6.84) | 40.15 (7.32) | 39.7 (8.4) | p = 0.93 |
| TBW postdialysis l | 38.17 (8.03) | 40.46 (12.51) | 37.5 (6.97) | 38.56 (7.29) | 37.44 (8.24) | p = 0.85 |
| ECW predialysis l | 19.1 (3.2) | 19.9 (3.3) | 20.1 (3.5) | 19.3 (3.5) | 18.9 (3.2) | p = 0.74 |
| ECW postdialysis l | 17.2 (3.1) | 17.43 (3.1) | 17.38 (2.9) | 18.2 (5.7) | 16.7 (2.9) | p = 0.77 |
| ICW predialysis l | 21.31 (5.6) | 23.3 (7.5) | 22.2 (5.1) | 20.7 (4.2) | 20.8 (5.4) | p = 0.62 |
| ICW postdialysis l | 21.33 (5.7) | 24.5 (8.8) | 24.2 (6.5) | 21.2 (4.7) | 20.7 (5.5) | p = 0.17 |
| S-HD | HDX | PRE-HDF | MIX-HDF | POST-HDF | p | |
|---|---|---|---|---|---|---|
| SBP 1st min mmHg | 145.8 (24.6) | 139.1 (17.2) | 143.4 (22.6) | 141.2 (18.0) | 137.9 (21.9) | p = 0.75 |
| SBP 240 min mmHg | 142.5 (35.5) | 142.2 (28.3) | 138.7 (35.7) | 140.6 (35.5) | 138.8 (29.2) | p = 0.98 |
| DBP 1st min mmHg | 87.0 (17.5) | 86.3 (14.3) | 86.1 (16.7) | 87.9 (16.6) | 83.4 (15.8) | p = 0.85 |
| DBP 240 min mmHg | 85.7 (17.1) | 89.1 (21.3) | 84.9 (17.3) | 85.3 (20.5) | 87.3 (18.7) | p = 0.91 |
| AUC SBP | 323 816.6 (72,781.6) | 318 930.3 (61,252.4) | 316 602.0 (68,292.8) | 305 190.3 (76,556.9) | 313 049.4 (80,028.1) | p = 0.8 |
| AUC DPB | 194,716.4 (37,664.1) | 192,651.0 (53,530.6) | 194,253.7 (33,794.1) | 190,661.9 (44,971.5) | 191,900.7 (44,991.7) | p = 0.88 |
| AUC MAP | 237,748.1 (46,888.6) | 230,184.4 (59,405.4) | 235,096.4 (42,932.1) | 231,486.3 (53 996.6) | 234,209.5 (47,871.5) | p = 0.23 |
| AUC CI | 6559.2 (1439.5) | 6770.9 (1271.3) | 6512.5 (1256.4) | 6093.9 (1282.4) | 6680.9 (1652.9) | p = 0.65 |
| AUC SVRI | 6,176,119.3 (1,325,662.8) | 6,456,193.4 (1,473,702.1) | 6,256,567.9 (999,108.8) | 7,075,464.9 (1,930,210.7) | 6,301,942.5 (1,337,688.1) | p = 0.34 |
| S-HD | HDX | PRE-HDF | MIX-HDF | POST-HDF | p | |
|---|---|---|---|---|---|---|
| Symptomatic hypotension n | 0 | 0 | 0 | 0 | 0 | p = 1.0 |
| AEs potentially related to BP/fluid shifts n | 0 | 1 | 1 | 2 | 4 | p = 0.39 |
| AEs potentially not related to BP/fluid shifts n | 7 | 4 | 5 | 5 | 2 | p = 0.47 |
| Intradialytic clotting events n | 1 | 1 | 2 | 2 | 4 | p = 0.51 |
| All AEs n (%) | 8 (33.3%) | 6 (25%) | 7 (29.2%) | 9 (37.5%) | 10 (41.7%) | p = 0.76 |
| Immediate DRT n (%) | 11 (45.8%) | 12 (50%) | 15 (62.5%) | 9 (37.5%) | 10 (41.7%) | p = 0.10 |
| Delayed DRT min | 360.0 (180–720) | 180 (120–390) | 60 (30–600) | 360 (180–360) | 390 (60–720) | p = 0.37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakrzewska, A.; Biedunkiewicz, J.; Komorniczak, M.; Jankowska, M.; Jasiulewicz, K.; Płonka, N.; Biedunkiewicz, B.; Małgorzewicz, S.; Tarasewicz, A.; Puchalska-Reglińska, E.; et al. Intradialytic Tolerance and Recovery Time in Different High-Efficiency Hemodialysis Modalities. J. Clin. Med. 2024, 13, 326. https://doi.org/10.3390/jcm13020326
Zakrzewska A, Biedunkiewicz J, Komorniczak M, Jankowska M, Jasiulewicz K, Płonka N, Biedunkiewicz B, Małgorzewicz S, Tarasewicz A, Puchalska-Reglińska E, et al. Intradialytic Tolerance and Recovery Time in Different High-Efficiency Hemodialysis Modalities. Journal of Clinical Medicine. 2024; 13(2):326. https://doi.org/10.3390/jcm13020326
Chicago/Turabian StyleZakrzewska, Agnieszka, Jan Biedunkiewicz, Michał Komorniczak, Magdalena Jankowska, Katarzyna Jasiulewicz, Natalia Płonka, Bogdan Biedunkiewicz, Sylwia Małgorzewicz, Agnieszka Tarasewicz, Ewelina Puchalska-Reglińska, and et al. 2024. "Intradialytic Tolerance and Recovery Time in Different High-Efficiency Hemodialysis Modalities" Journal of Clinical Medicine 13, no. 2: 326. https://doi.org/10.3390/jcm13020326
APA StyleZakrzewska, A., Biedunkiewicz, J., Komorniczak, M., Jankowska, M., Jasiulewicz, K., Płonka, N., Biedunkiewicz, B., Małgorzewicz, S., Tarasewicz, A., Puchalska-Reglińska, E., Siebert, J., Dębska-Ślizień, A., & Tylicki, L. (2024). Intradialytic Tolerance and Recovery Time in Different High-Efficiency Hemodialysis Modalities. Journal of Clinical Medicine, 13(2), 326. https://doi.org/10.3390/jcm13020326