The Role of Vortioxetine in the Treatment of Depressive Symptoms in General Hospital Psychiatry: A Case-Series and PRISMA-Compliant Systematic Review of the Literature


 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Series
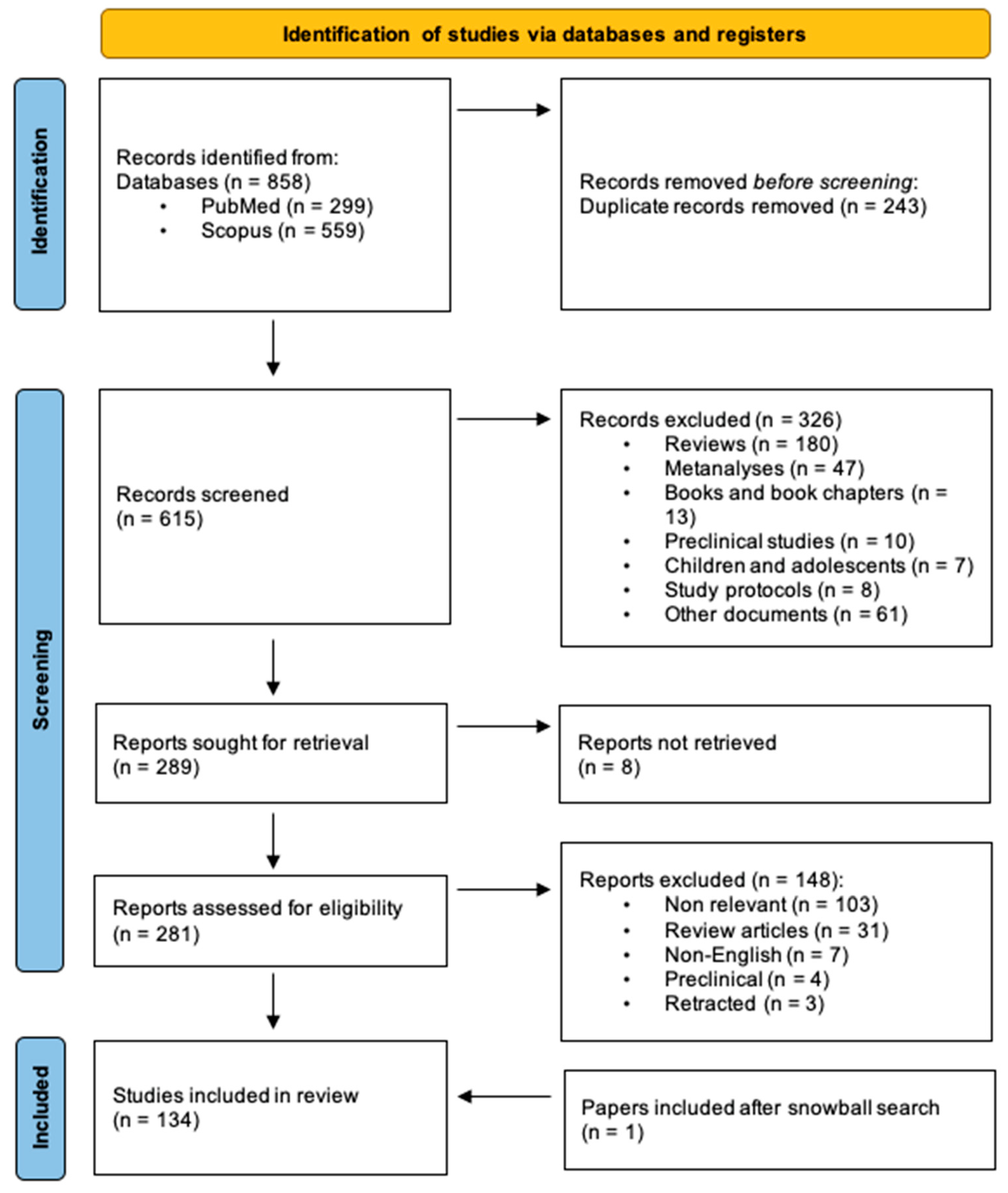
2.2. Systematic Review of the Literature
3. Results
3.1. Case Series
3.2. Systematic Review of the Literature
3.2.1. Experimental Studies

{kind=link}
| Study | Functional Outcome | Clinimetric Tools | Results |
|---|---|---|---|
| Theunissen et al., 2013 [66] | Actual driving Cognitive performance Psychomotor performance | Actual driving test (SDLP) Divided attention task Psychomotor vigilance task | MIRT significantly impairs driving on day 2 but not on day 16 and prolongs reaction times in psychomotor vigilance and divided attention tasks compared to VOR and PLA. |
| Jacobsen et al., 2015 [72] | TESD | CSFQ-14 | VOR: significantly associated with greater improvement in sexual function in previously SSRI-treated patients compared to ESC. |
| Chokka et al., 2019 [69] | Cognitive performance, workplace functioning, perceived disability | DSST, PDQ-D-20, WLQ, WPAI, SDS | VOR significantly improved outcomes in all clinimetric scales at 52 weeks. |
| Chokka et al., 2019 [70] | Cognitive performance, workplace functioning, perceived disability | DSST, PDQ-D-20, WLQ, WPAI, SDS | VOR significantly improved outcomes in all clinimetric scales at 12 weeks. |
| Jacobsen et al., 2019 [65] | TESD | CSFQ-14 | PAR: significantly higher incidence of TESD compared to VOR and PLA VOR: not significantly higher incidence of TESD compared to PLA. |
| Jacobsen et al., 2019 [68] | TESD | CSFQ-14 | VOR: significantly associated with greater improvement in sexual function in previously SSRI-treated patients compared to ESC. |
| Nierenberg et al., 2019 [71] | Cognitive performance | DSST | Both SSRI and VOR improved cognitive performance. VOR did not significantly outperformed standard SSRIs. |
| Lenze et al., 2020 [67] | Cognitive training augmentation | NIH Toolbox Cognition Battery Fluid Cognition Composite | Cognitive training plus VOR significantly improves performance compared to cognitive training plus PLA. |
| Study | Half-Life (Hours) | Tmax (Hours) | Observations |
|---|---|---|---|
| Chen et al., 2013 [89] | / | / | Vortioxetine has no effect on drug metabolism catalyzed by CYP2D6, CYP2C19 and CYP3A4. Vortioxetine metabolism is influenced by CYP2D6 inhibitors and CYP3A4 inducers. |
| Wang et al., 2013 [88] | 58.58 (10 mg) 56.41 (40 mg) | 8.10 (10 mg) 8.10 (40 mg) | Vortioxetine dosed 10 mg and 40 mg has no clinically significant effect on corrected QT. |
| Chen et al., 2015 [87] | / | / | Vortioxetine dosed 10 mg has no effect on aspirin or warfarin pharmacokinetics. |
| Wilson et al., 2015 [86] | / | / | Vortioxetine effects on sleep resemble those of paroxetine: reduced total sleep time, reduced total REM sleep, prolonged REM onset latency, and increased stage 1 sleep. |
| Chen et al., 2016 [85] | / | / | Vortioxetine has no effect on the pharmacokinetics of ethanol, diazepam and lithium and does not impact psychomotor performance compared with ethanol or diazepam alone. |
| Matsuno et al., 2018 [84] | 69.4 (5 mg) 66.0 (10 mg) 55.1 (20 mg) 56.6 (40 mg) | 10.0 (5 mg) 10.0 10 mg) 9.0 (20 mg) 6.3 (40 mg) | Vortioxetine metabolism does not differ between sexes. Vortioxetine exposure tends to be higher in the elderly. No food effect on the pharmacokinetics of vortioxetine. |
| Chen et al., 2018 [83] | / | / | Vortioxetine exposure tends to be about 25% higher in the elderly, blacks and females. Severe hepatic or renal impairment does not significantly alter vortioxetine disposition. |
| Study | Comparator | Significant TEAEs (Vortioxetine vs. Comparator) | Non-Significant TEAEs |
|---|---|---|---|
| Alvarez et al., 2012 [54] | Placebo | Nausea, Vomiting, Hyperhidrosis. | Headache, Dry mouth, Diarrhoea, Dizziness, Nasopharyngitis, Fatigue, Insomnia, Constipation, Blurred Vision, Anorgasmia. |
| Baldwin et al., 2012 [62] | Placebo | Nausea. | Headache, Diarrhoea, Vomiting, Dizziness, Dry mouth, Somnolence, Nasopharyngitis, Constipation, Fatigue, Hyperhidrosis, Insomnia, Decreased appetite. |
| Boulenger et al., 2012 [37] | Placebo | Nausea. | Headache, Nasopharyngitis, Dizziness, Dry mouth, Insomnia, Fatigue, Gastroenteritis. |
| Katona et al., 2012 [61] | Placebo | Nausea. | Headache, Dizziness, Fatigue, Constipation, Dry mouth Diarrhoea, Decreased appetite, Hyperhidrosis. |
| Boulenger et al., 2014 [60] | Placebo | Nausea, Dry mouth. | Headache, Diarrhoea, Dry mouth, Dizziness, Fatigue, Hyperhidrosis. |
| Wang et al., 2015 [53] | Venlafaxine | (Higher in venlafaxine: decreased appetite, insomnia) | Nausea, Dizziness, Headache, Dry mouth, Accidental overdose, Decreased appetite, Constipation. |
| Liebowitz et al., 2017 [22] | Placebo | Nausea. | Anxiety, Depression, Irritability, Decreased appetite, Difficulty achieving orgasm, Headache, Increased appetite, Increased sleep, Insomnia, Migraine, Headache, Tingling, Tiredness, Constipation, Diarrhoea. |
| Borhannejad et al., 2020 [52] | Sertraline | / | / |
| Study | Participants | Vortioxetine | Comparator 1 | Comparator 2 |
|---|---|---|---|---|
| Shin et al., 2023 [56] | Vortioxetine = 42 Escitalopram = 42 Desvenlafaxine = 40 | N = 1 (Vomiting = 1) | Escitalopram N = 2 | Desvenlafaxine N = 3 |
| Santi et al., 2023 [57] | Vortioxetine = 20 Escitalopram = 18 Vilazodone = 18 | N = 0 | Escitalopram N = 0 | Vilazodone N = 0 |
| McIntyre et al., 2023 [46] | Vortioxetine = 309 Desvenlafaxine = 293 | N = 6 | Desvenlafaxine N = 3 | / |
| Lee et al., 2022 [55] | Vortioxetine = 40 Escitalopram = 43 Desvenlafaxine = 38 | N = 2 (Vomiting = 1) (Fatigue = 1) | Escitalopram N = 3 | Desvenlafaxine N = 2 |
| Borhannejad et al., 2020 [52] | Vortioxetine = 30 Sertraline = 30 | N = 0 | Sertraline N = 0 | / |
| Levada et al., 2019 [49] | Vortioxetine = 41 Escitalopram = 25 | N = 0 | Escitalopram N = 0 | / |
| Vieta et al., 2018 [58] | Vortioxetine = 50 Escitalopram = 49 | N = 3 (Not available) | Escitalopram N = 1 | / |
| Baune et al., 2018 [50] | Vortioxetine = 48 Paroxetine = 54 Placebo = 48 | N = 3 (Nausea = 2) | Paroxetine N = 3 (2 serious adverse events) | Placebo N = 1 |
| Mahableshwarkar et al., 2015 [59] | Vortioxetine = 301 Duloxetine = 152 Placebo = 161 | N = 28 (Most common: nausea) | Duloxetine N = 10 | Placebo N = 4 |
| Mahableshwarkar et al., 2015 [51] | Vortioxetine = 198 Duloxetine = 210 Placebo = 194 | N = 7 | Duloxetine N = 13 | Placebo N = 7 |
| Wang et al., 2015 [53] | Vortioxetine = 211 Venlafaxine = 226 | N = 14 | Venlafaxine N = 32 | / |
| Boulenger et al., 2014 [60] | Vortioxetine = 302 Duloxetine = 147 Placebo = 158 | N = 27 * (Most common: nausea) | Duloxetine N = 7 | Placebo N = 7 |
| Montgomery et al., 2014 [44] | Vortioxetine = 253 Agomelatine = 246 | N = 15 (Most common: nausea and vomiting) | Agomelatine N = 23 (Most common: dizziness and headache) | / |
| Alvarez et al., 2012 [54] | Vortioxetine = 208 Venlafaxine = 113 Placebo = 105 | N = 10 (Not available) | Venlafaxine * N = 16 | Placebo N = 4 |
| Katona et al., 2012 [61] | Vortioxetine = 156 Duloxetine = 151 Placebo = 145 | N = 10 (Most common: nausea) | Duloxetine N = 15 | Placebo N = 6 |
| Baldwin et al., 2012 [62] | Vortioxetine = 463 Duloxetine = 155 Placebo = 148 | N = 43 | Duloxetine * N = 19 | Placebo N = 12 |
3.2.2. Analytical Observational Studies
| Study | Aim | Observation 1 | Observation 2 |
|---|---|---|---|
| Hughes et al., 2017 [126] | Screening of online reviews of antidepressant users and user satisfaction as a marker of drug acceptability. | VOR was associated with a higher frequency of itch, nausea, anxiety, agitation, crying, and headache compared to DUL and ESC. | VOR was associated with a lower frequency of insomnia, sexual complains, emotional numbing, and motor disorders compared to DUL and ESC. |
| Greenblatt et al., 2018 [125] | Comparison of VOR pharmacokinetics between obese subjects and control. | VOR accumulation and washout half-lives were significantly longer (about 50%) in obese individuals. | Possible pharmacodynamic interaction (serotonin toxicity) after VOR withdrawal might last longer than expected in obese individuals. |
| Mazhar et al., 2019 [133] | FAERS database vigilance study on antidepressants risk of hyponatremia. | VOR was significantly associated with a higher risk of hyponatremia (although probably overestimated). | Relative to VOR, the risk of hyponatremia was higher for CLO, TRI, MIRT, SSRIs and SNRIs. |
| Miao et al., 2019 [132] | Pharmacokinetics and safety of VOR in Chinese subjects compared to non-Chinese. | VOR exposure was higher in the Chinese than non-Chinese population, but difference did not reach significance. | Commonest side effects in 124 Chinese subjects were nausea (20.2%), dizziness (9.7%), dry mouth (5.6%), hyporexia (4%) and Diarrhoea (3.2%). |
| Woroń et al., 2019 [134] | 66 cases of interaction between antidepressants and cardiovascular medications. | VOR linked to a case of hyponatremia (+HCTZ) and a case of nose/urinary bleeding (+WARF). | Commonest interaction: bradycardia (SSRI + beta-blockers) and limb swelling (SSRI + amlodipine). |
| Bordet et al., 2020 [130] | QT prolongation: VOR vs. SSRIs. | The association between VOR and QT prolongation was non-significant. | VOR bears a lower risk of inducing QT prolongation than SSRIs. |
| Eugene., 2020 [131] | Association between 30 antidepressants and somnolence. | VOR showed the lowest risk of somnolence (but no risk for levomilnacipran). | Amoxapine showed the greatest association with somnolence, probably due to highest 5HT2A affinity. |
| Revet et al., 2020 [129] | Antidepressants and movement disorders. | VOR is significantly associated with bruxism (OR 4.71, 2.88–8.80). | SSRIs are associated with a higher risk of movement disorders compared to first-generation antidepressants. |
| Seifert et al., 2021 [128] | Psychotropic drug-induced hyponatremia | Out of 501 patients on VOR, 1 case of hyponatremia was registered. | Highest rates of hyponatremia were reported with CIT, VEN and ESC. |
| Ekhart et al., 2022 [123] | VOR TEAE reporting pattern and comparison with SSRIs. | Most frequent TEAE reported with VOR were nausea, vomiting, Diarrhoea and hypersensitivity (pruritus, rash). | Withdrawal syndrome, hyponatremia, tremor and paresthesia less often reported for VOR than SSRIs. |
| Healy et al., 2022 [127] | Adverse visual effects linked to antidepressants. | A case of blurred vision still present 26 days after a single VOR dose. | Most reports of persisting visual disorders involved SER, ESC, VEN, and FLU. |
| Quilichini et al., 2022 [124] | Withdrawal syndrome risk with different antidepressants. | VOR and AGO have the lowest risk of withdrawal syndrome. | PAR, DES, VEN, and DUL have the highest risk of withdrawal syndrome. |
3.2.3. Descriptive Observational Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gold, S.M.; Köhler-Forsberg, O.; Moss-Morris, R.; Mehnert, A.; Miranda, J.J.; Bullinger, M.; Steptoe, A.; Whooley, M.A.; Otte, C. Comorbid depression in medical diseases. Nat. Rev. Dis. Primers 2020, 6, 69. [Google Scholar] [CrossRef]
- Ishak, W.W.; Collison, K.; Danovitch, I.; Shek, L.; Kharazi, P.; Kim, T.; Jaffer, K.Y.; Naghdechi, L.; Lopez, E.; Nuckols, T. Screening for Depression in Hospitalized Medical Patients. J. Hosp. Med. 2017, 12, 118–125. [Google Scholar] [CrossRef]
- Jakobsen, J.C.; Gluud, C.; Kirsch, I. Should antidepressants be used for major depressive disorder? BMJ Evid. Based. Med. 2020, 25, 130. [Google Scholar] [CrossRef]
- Pennazio, F.; Brasso, C.; Villari, V.; Rocca, P. Current Status of Therapeutic Drug Monitoring in Mental Health Treatment: A Review. Pharmaceutics 2022, 14, 2674. [Google Scholar] [CrossRef] [PubMed]
- Bang-Andersen, B.; Olsen, C.K.; Sanchéz, C. The Discovery of the Antidepressant Vortioxetine and the Research that Uncovered Its Potential to Treat the Cognitive Dysfunction Associated with Depression. In Successful Drug Discovery; Wiley: Hoboken, NJ, USA, 2016; pp. 189–214. ISBN 9783527341153/9783527800315. [Google Scholar]
- Okada, M.; Okubo, R.; Fukuyama, K. Vortioxetine Subchronically Activates Serotonergic Transmission via Desensitization of Serotonin 5-HT(1A) Receptor with 5-HT(3) Receptor Inhibition in Rats. Int. J. Mol. Sci. 2019, 20, 6235. [Google Scholar] [CrossRef]
- El Mansari, M.; Lecours, M.; Blier, P. Effects of acute and sustained administration of vortioxetine on the serotonin system in the hippocampus: Electrophysiological studies in the rat brain. Psychopharmacology 2015, 232, 2343–2352. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Højer, A.-M.; Areberg, J.; Nomikos, G. Vortioxetine: Clinical Pharmacokinetics and Drug Interactions. Clin. Pharmacokinet. 2018, 57, 673–686. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, D.S.; Necking, O.; Schmidt, S.N.; Ren, H.; Reines, E.H. Efficacy and safety of vortioxetine in treatment of patients with major depressive disorder and common co-morbid physical illness. J. Affect. Disord. 2022, 311, 588–594. [Google Scholar] [CrossRef]
- Nomikos, G.G.; Tomori, D.; Zhong, W.; Affinito, J.; Palo, W. Efficacy, safety, and tolerability of vortioxetine for the treatment of major depressive disorder in patients aged 55 years or older. CNS Spectr. 2016, 22, 348–362. [Google Scholar] [CrossRef]
- De Diego-Adeliño, J.; Crespo, J.M.; Mora, F.; Neyra, A.; Iborra, P.; Gutiérrez-Rojas, L.; Salonia, S.F. Vortioxetine in major depressive disorder: From mechanisms of action to clinical studies. An updated review. Expert Opin. Drug Saf. 2021, 21, 673–690. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Guy, W. ECDEU Assessment Manual; American Psychological Association (APA): Rockville, ML, USA, 1976. [Google Scholar]
- Page, M.J.; Mckenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.; Moher, D. Updating Guidance for Reporting Systematic Reviews: Development of the PRISMA 2020 Statement; Center for Open Science: Charlottesville, VA, USA, 2020. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Grimes, D.A.; Schulz, K.F. An overview of clinical research: The lay of the land. Lancet 2002, 359, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Henigsberg, N.; Mahableshwarkar, A.R.; Jacobsen, P.; Chen, Y.; Thase, M.E. A Randomized, Double-Blind, Placebo-Controlled 8-Week Trial of the Efficacy and Tolerability of Multiple Doses of Lu AA21004 in Adults with Major Depressive Disorder. J. Clin. Psychiatry 2012, 73, 953–959. [Google Scholar] [CrossRef]
- Inoue, T.; Sasai, K.; Kitagawa, T.; Nishimura, A.; Inada, I. Randomized, double-blind, placebo-controlled study to assess the efficacy and safety of vortioxetine in Japanese patients with major depressive disorder. Psychiatry Clin. Neurosci. 2020, 74, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Florea, I.; Schmidt, S.N.; Areberg, J.; Ettrup, A. Intravenous vortioxetine to accelerate onset of effect in major depressive disorder: A 2-week, randomized, double-blind, placebo-controlled study. Int. Clin. Psychopharmacol. 2019, 34, 153–160. [Google Scholar] [CrossRef]
- Mcintyre, R.S.; Lophaven, S.; Olsen, C.K. A randomized, double-blind, placebo-controlled study of vortioxetine on cognitive function in depressed adults. Int. J. Neuropsychopharmacol. 2014, 17, 1557–1567. [Google Scholar] [CrossRef] [PubMed]
- Liebowitz, M.R.; Careri, J.; Blatt, K.; Draine, A.; Morita, J.; Moran, M.; Hanover, R. Vortioxetine versus placebo in major depressive disorder comorbid with social anxiety disorder. Depress. Anxiety 2017, 34, 1164–1172. [Google Scholar] [CrossRef]
- Jacobsen, P.L.; Mahableshwarkar, A.R.; Serenko, M.; Chan, S.; Trivedi, M.H. A Randomized, Double-Blind, Placebo-Controlled Study of the Efficacy and Safety of Vortioxetine 10 mg and 20 mg in Adults with Major Depressive Disorder. J. Clin. Psychiatry 2015, 76, 575–582. [Google Scholar] [CrossRef]
- Rancans, E.; Zambori, J.; Dalsgaard, M.; Baayen, C.; Areberg, J.; Ettrup, A.; Florea, I. Intravenous vortioxetine to accelerate onset of effect in major depressive disorder: A 7-day randomized, double-blind, placebo-controlled exploratory study. Int. Clin. Psychopharmacol. 2020, 35, 305–312. [Google Scholar] [CrossRef]
- Nishimura, A.; Aritomi, Y.; Sasai, K.; Kitagawa, T.; Mahableshwarkar, A.R. Randomized, double-blind, placebo-controlled 8-week trial of the efficacy, safety, and tolerability of 5, 10, and 20 mg/day vortioxetine in adults with major depressive disorder. Psychiatry Clin. Neurosci. 2017, 72, 64–72. [Google Scholar] [CrossRef]
- Inoue, T.; Nishimura, A.; Sasai, K.; Kitagawa, T. Randomized, 8-week, double-blind, placebo-controlled trial of vortioxetine in Japanese adults with major depressive disorder, followed by a 52-week open-label extension trial. Psychiatry Clin. Neurosci. 2017, 72, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Mahableshwarkar, A.R.; Jacobsen, P.L.; Serenko, M.; Chen, Y.; Trivedi, M.H. A Randomized, Double-Blind, Placebo-Controlled Study of the Efficacy and Safety of 2 Doses of Vortioxetine in Adults With Major Depressive Disorder. J. Clin. Psychiatry 2015, 76, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Mahableshwarkar, A.R.; Jacobsen, P.L.; Chen, Y.; Thase, M.E. A randomized, double-blind, placebo-controlled 6-wk trial of the efficacy and tolerability of 5 mg vortioxetine in adults with major depressive disorder. Int. J. Neuropsychopharmacol. 2012, 16, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.W.; Yoon, K.H.; Lee, C.H.; Moon, Y.S.; Kim, D.H. Vortioxetine Treatment for Depression in Alzheimer’s Disease: A Randomized, Double-blind, Placebo-controlled Study. Clin. Psychopharmacol. Neurosci. 2022, 20, 311–319. [Google Scholar] [CrossRef]
- Inoue, T.; Fujimoto, S.; Marumoto, T.; Kitagawa, T.; Ishida, K.; Nakajima, T.; Moriguchi, Y.; Fujikawa, K.; Watanabe, K. Early Improvement with Vortioxetine Predicts Response and Remission: A Post Hoc Analysis of Data from a Clinical Trial Conducted in Japan. Neuropsychiatr. Dis. Treat. 2021, 17, 3735–3741. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Fujimoto, S.; Marumoto, T.; Kitagawa, T.; Ishida, K.; Nakajima, T.; Moriguchi, Y.; Fujikawa, K.; Watanabe, K. Therapeutic Potential of Vortioxetine for Anxious Depression: A Post Hoc Analysis of Data from a Clinical Trial Conducted in Japan. Neuropsychiatr. Dis. Treat. 2021, 17, 3781–3790. [Google Scholar] [CrossRef]
- Watanabe, K.; Fujimoto, S.; Marumoto, T.; Kitagawa, T.; Ishida, K.; Nakajima, T.; Moriguchi, Y.; Fujikawa, K.; Inoue, T. Therapeutic Potential of Vortioxetine for Anhedonia-Like Symptoms in Depression: A Post Hoc Analysis of Data from a Clinical Trial Conducted in Japan. Neuropsychiatr. Dis. Treat. 2022, 18, 363–373. [Google Scholar] [CrossRef]
- Baune, B.T.; Sampson, E.; Louise, J.; Hori, H.; Schubert, K.O.; Clark, S.R.; Mills, N.T.; Fourrier, C. No evidence for clinical efficacy of adjunctive celecoxib with vortioxetine in the treatment of depression: A 6-week double-blind placebo controlled randomized trial. Eur. Neuropsychopharmacol. 2021, 53, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Mills, N.T.; Sampson, E.; Fourrier, C.; Baune, B.T. Clinical Switching Strategies of Various Antidepressants to Vortioxetine in the PREDDICT Trial. Int. J. Neuropsychopharmacol. 2020, 24, 314–321. [Google Scholar] [CrossRef]
- Thase, M.E.; Jacobsen, P.L.; Hanson, E.; Xu, R.; Tolkoff, M.; Murthy, N.V. Vortioxetine 5, 10, and 20 mg significantly reduces the risk of relapse compared with placebo in patients with remitted major depressive disorder: The RESET study. J. Affect. Disord. 2022, 303, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, P.; Zhong, W.; Xu, R.; Nomikos, G. A novel study design for investigating relapse prevention in major depressive disorder: Preliminary data from the open-label period of a phase 4 vortioxetine study. J. Affect. Disord. 2020, 266, 173–181. [Google Scholar] [CrossRef]
- Boulenger, J.-P.; Loft, H.; Florea, I. A randomized clinical study of Lu AA21004 in the prevention of relapse in patients with major depressive disorder. J. Psychopharmacol. 2012, 26, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Mattingly, G.W.; Necking, O.; Schmidt, S.N.; Reines, E.; Ren, H. Long-term safety and efficacy, including anhedonia, of vortioxetine for major depressive disorder: Findings from two open-label studies. Curr. Med. Res. Opin. 2023, 39, 613–619. [Google Scholar] [CrossRef]
- Vieta, E.; Loft, H.; Florea, I. Effectiveness of long-term vortioxetine treatment of patients with major depressive disorder. Eur. Neuropsychopharmacol. 2017, 27, 877–884. [Google Scholar] [CrossRef]
- Jacobsen, P.L.; Harper, L.; Chrones, L.; Chan, S.; Mahableshwarkar, A.R. Safety and tolerability of vortioxetine (15 and 20 mg) in patients with major depressive disorder: Results of an open-label, flexible-dose, 52-week extension study. Int. Clin. Psychopharmacol. 2015, 30, 255–264. [Google Scholar] [CrossRef]
- Alam, M.Y.; Jacobsen, P.L.; Chen, Y.; Serenko, M.; Mahableshwarkar, A.R. Safety, tolerability, and efficacy of vortioxetine (Lu AA21004) in major depressive disorder: Results of an open-label, flexible-dose, 52-week extension study. Int. Clin. Psychopharmacol. 2014, 29, 36–44. [Google Scholar] [CrossRef]
- Baldwin, D.S.; Hansen, T.; Florea, I. Vortioxetine (Lu AA21004) in the long-term open-label treatment of major depressive disorder. Curr. Med. Res. Opin. 2012, 28, 1717–1724. [Google Scholar] [CrossRef]
- Papakostas, G.I.; Nielsen, R.Z.; Dragheim, M.; Tonnoir, B. Efficacy and tolerability of vortioxetine versus agomelatine, categorized by previous treatment, in patients with major depressive disorder switched after an inadequate response. J. Psychiatr. Res. 2018, 101, 72–79. [Google Scholar] [CrossRef]
- Montgomery, S.A.; Nielsen, R.Z.; Poulsen, L.H.; Häggström, L. A randomised, double-blind study in adults with major depressive disorder with an inadequate response to a single course of selective serotonin reuptake inhibitor or serotonin-noradrenaline reuptake inhibitor treatment switched to vortioxetine or agomelatine. Hum. Psychopharmacol. 2014, 29, 470–482. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Zhao, K.; Reynaud-Mougin, C.; Loft, H.; Ren, H.; Eriksen, H.-L.F.; Ettrup, A. Successfully treated patients with vortioxetine versus venlafaxine: A simplified cost-effectiveness analysis based on a head-to-head study in Asian patients with major depressive disorder. Curr. Med. Res. Opin. 2020, 36, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Mcintyre, R.S.; Florea, I.; Pedersen, M.M.; Christensen, M.C. Head-To-Head Comparison of Vortioxetine Versus Desvenlafaxine in Patients with Major Depressive Disorder with Partial Response to SSRI Therapy. J. Clin. Psychiatry 2023, 84, 23m14780. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.C.; Loft, H.; Mcintyre, R.S. Vortioxetine improves symptomatic and functional outcomes in major depressive disorder: A novel dual outcome measure in depressive disorders. J. Affect. Disord. 2018, 227, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Shao, S.; Sun, B.; Sun, H. Clinical efficacy of Vortioxetine and escitalopram in the treatment of depression. Pak. J. Med. Sci. 2022, 38, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Levada, O.A.; Troyan, A.S. Cognitive-functional relationships in major depressive disorder: Crucial data from a Ukrainian open-label study of vortioxetine versus escitalopram. J. Affect. Disord. 2019, 250, 114–122. [Google Scholar] [CrossRef]
- Baune, B.T.; Sluth, L.B.; Olsen, C.K. The effects of vortioxetine on cognitive performance in working patients with major depressive disorder: A short-term, randomized, double-blind, exploratory study. J. Affect. Disord. 2018, 229, 421–428. [Google Scholar] [CrossRef]
- Mahableshwarkar, A.R.; Zajecka, J.; Jacobson, W.; Chen, Y.; Keefe, R.S.E. A Randomized, Placebo-Controlled, Active-Reference, Double-Blind, Flexible-Dose Study of the Efficacy of Vortioxetine on Cognitive Function in Major Depressive Disorder. Neuropsychopharmacology 2015, 40, 2025–2037. [Google Scholar] [CrossRef]
- Borhannejad, F.; Shariati, B.; Naderi, S.; Shalbafan, M.; Mortezaei, A.; Sahebolzamani, E.; Saeb, A.; Hosein Mortazavi, S.; Kamalzadeh, L.; Aqamolaei, A.; et al. Comparison of vortioxetine and sertraline for treatment of major depressive disorder in elderly patients: A double-blind randomized trial. J. Clin. Pharm. Ther. 2020, 45, 804–811. [Google Scholar] [CrossRef]
- Wang, G.; Gislum, M.; Filippov, G.; Montgomery, S. Comparison of vortioxetine versus venlafaxine XR in adults in Asia with major depressive disorder: A randomized, double-blind study. Curr. Med. Res. Opin. 2015, 31, 785–794. [Google Scholar] [CrossRef]
- Alvarez, E.; Perez, V.; Dragheim, M.; Loft, H.; Artigas, F. A double-blind, randomized, placebo-controlled, active reference study of Lu AA21004 in patients with major depressive disorder. Int. J. Neuropsychopharmacol. 2012, 15, 589–600. [Google Scholar] [CrossRef]
- Lee, S.H.; Jeon, S.W.; Shin, C.; Pae, C.U.; Patkar, A.A.; Masand, P.S.; An, H.; Han, C. Acute Efficacy and Safety of Escitalopram Versus Desvenlafaxine and Vortioxetine in the Treatment of Depression With Cognitive Complaint: A Rater-Blinded Randomized Comparative Study. Psychiatry Investig. 2022, 19, 268–280, Erratum in Psychiatry Investig. 2022, 19, 500. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.; Jeon, S.W.; Lee, S.-H.; Pae, C.-U.; Hong, N.; Lim, H.K.; Patkar, A.A.; Masand, P.S.; An, H.; Han, C. Efficacy and Safety of Escitalopram, Desvenlafaxine, and Vortioxetine in the Acute Treatment of Anxious Depression: A Randomized Rater-blinded 6-week Clinical Trial. Clin. Psychopharmacol. Neurosci. 2023, 21, 135–146. [Google Scholar] [CrossRef]
- Santi, N.S.; Biswal, S.B.; Naik, B.N.; Sahoo, J.P.; Rath, B. An Interim Analysis of a Randomized, Open-Label Study of Vilazodone, Escitalopram, or Vortioxetine for Major Depressive Disorder. Cureus 2023, 15, e37858. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Sluth, L.B.; Olsen, C.K. The effects of vortioxetine on cognitive dysfunction in patients with inadequate response to current antidepressants in major depressive disorder: A short-term, randomized, double-blind, exploratory study versus escitalopram. J. Affect. Disord. 2018, 227, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Mahableshwarkar, A.R.; Jacobsen, P.L.; Chen, Y.; Serenko, M.; Trivedi, M.H. A randomized, double-blind, duloxetine-referenced study comparing efficacy and tolerability of 2 fixed doses of vortioxetine in the acute treatment of adults with MDD. Psychopharmacology 2015, 232, 2061–2070. [Google Scholar] [CrossRef] [PubMed]
- Boulenger, J.-P.; Loft, H.; Olsen, C.K. Efficacy and safety of vortioxetine (Lu AA21004), 15 and 20 mg/day: A randomized, double-blind, placebo-controlled, duloxetine-referenced study in the acute treatment of adult patients with major depressive disorder. Int. Clin. Psychopharmacol. 2014, 29, 138–149. [Google Scholar] [CrossRef]
- Katona, C.; Hansen, T.; Olsen, C.K. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Int. Clin. Psychopharmacol. 2012, 27, 215–223. [Google Scholar] [CrossRef]
- Baldwin, D.S.; Loft, H.; Dragheim, M. A randomised, double-blind, placebo controlled, duloxetine-referenced, fixed-dose study of three dosages of Lu AA21004 in acute treatment of major depressive disorder (MDD). Eur. Neuropsychopharmacol. 2012, 22, 482–491. [Google Scholar] [CrossRef]
- Mahableshwarkar, A.R.; Jacobsen, P.L.; Chen, Y. A randomized, double-blind trial of 2.5 mg and 5 mg vortioxetine (Lu AA21004) versus placebo for 8 weeks in adults with major depressive disorder. Curr. Med. Res. Opin. 2013, 29, 217–226. [Google Scholar] [CrossRef]
- Cumbo, E.; Cumbo, S.; Torregrossa, S.; Migliore, D. Treatment effects of vortioxetine on cognitive functions in mild Alzheimer’s disease patients with depressive symptoms: A 12 month, open-label, observational study. J. Prev. Alzheimer’s Dis. 2019, 6, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, P.; Zhong, W.; Nomikos, G.; Clayton, A. Paroxetine, but not Vortioxetine, Impairs Sexual Functioning Compared with Placebo in Healthy Adults: A Randomized, Controlled Trial. J. Sex. Med. 2019, 16, 1638–1649. [Google Scholar] [CrossRef] [PubMed]
- Theunissen, E.L.; Street, D.; Højer, A.M.; Vermeeren, A.; Van Oers, A.; Ramaekers, J.G. A Randomized Trial on the Acute and Steady-State Effects of a New Antidepressant, Vortioxetine (Lu AA21004), on Actual Driving and Cognition. Clin. Pharmacol. Ther. 2013, 93, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Lenze, E.J.; Stevens, A.; Waring, J.D.; Pham, V.T.; Haddad, R.; Shimony, J.; Miller, J.P.; Bowie, C.R. Augmenting Computerized Cognitive Training with Vortioxetine for Age-Related Cognitive Decline: A Randomized Controlled Trial. Am. J. Psychiatry 2020, 177, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, P.L.; Nomikos, G.G.; Zhong, W.; Cutler, A.J.; Affinito, J.; Clayton, A. Clinical implications of directly switching antidepressants in well-treated depressed patients with treatment-emergent sexual dysfunction: A comparison between vortioxetine and escitalopram. CNS Spectr. 2019, 25, 50–63. [Google Scholar] [CrossRef]
- Chokka, P.; Bougie, J.; Proulx, J.; Tvistholm, A.H.; Ettrup, A. Long-term functioning outcomes are predicted by cognitive symptoms in working patients with major depressive disorder treated with vortioxetine: Results from the AtWoRC study. CNS Spectr. 2019, 24, 616–627. [Google Scholar] [CrossRef]
- Chokka, P.; Bougie, J.; Rampakakis, E.; Proulx, J. Assessment in Work Productivity and the Relationship with Cognitive Symptoms (AtWoRC): Primary analysis from a Canadian open-label study of vortioxetine in patients with major depressive disorder (MDD). CNS Spectr. 2019, 24, 338–347. [Google Scholar] [CrossRef]
- Nierenberg, A.A.; Loft, H.; Olsen, C.K. Treatment effects on residual cognitive symptoms among partially or fully remitted patients with major depressive disorder: A randomized, double-blinded, exploratory study with vortioxetine. J. Affect. Disord. 2019, 250, 35–42. [Google Scholar] [CrossRef]
- Jacobsen, P.L.; Mahableshwarkar, A.R.; Chen, Y.; Chrones, L.; Clayton, A.H. Effect of Vortioxetine vs. Escitalopram on Sexual Functioning in Adults with Well-Treated Major Depressive Disorder Experiencing SSRI-Induced Sexual Dysfunction. J. Sex. Med. 2015, 12, 2036–2048. [Google Scholar] [CrossRef]
- Moazen-Zadeh, E.; Bayanati, S.; Ziafat, K.; Rezaei, F.; Mesgarpour, B.; Akhondzadeh, S. Vortioxetine as adjunctive therapy to risperidone for treatment of patients with chronic schizophrenia: A randomised, double-blind, placebo-controlled clinical trial. J. Psychopharmacol. 2020, 34, 506–513. [Google Scholar] [CrossRef]
- Adamo, D.; Pecoraro, G.; Coppola, N.; Calabria, E.; Aria, M.; Mignogna, M. Vortioxetine versus other antidepressants in the treatment of burning mouth syndrome: An open-label randomized trial. Oral Dis. 2020, 27, 1022–1041. [Google Scholar] [CrossRef] [PubMed]
- Seddighnia, A.; Tadayon Najafabadi, B.; Ghamari, K.; Noorbala, A.A.; Ebrahimi Daryani, N.; Kashani, L.; Akhondzadeh, S. Vortioxetine effects on quality of life of irritable bowel syndrome patients: A randomized, double-blind, placebo-controlled trial. J. Clin. Pharm. Ther. 2019, 45, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.E.; Valle, S.; Cavic, E.; Redden, S.A.; Chamberlain, S.R. A double-blind, placebo-controlled study of vortioxetine in the treatment of binge-eating disorder. Int. J. Eat. Disord. 2019, 52, 786–794. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Lindsten, A.; Sluth, L.B.; Petersen, M.L.; Ettrup, A.; Eriksen, H.-L.F.; Fava, M. Vortioxetine for attention deficit hyperactivity disorder in adults: A randomized, double-blind, placebo-controlled, proof-of-concept study. J. Psychopharmacol. 2019, 33, 511–521. [Google Scholar] [CrossRef]
- Mahableshwarkar, A.R.; Jacobsen, P.L.; Serenko, M.; Chen, Y. A randomized, double-blind, fixed-dose study comparing the efficacy and tolerability of vortioxetine 2.5 and 10 mg in acute treatment of adults with generalized anxiety disorder. Hum. Psychopharmacol. Clin. Exp. 2014, 29, 64–72. [Google Scholar] [CrossRef]
- Mahableshwarkar, A.R.; Jacobsen, P.L.; Chen, Y.; Simon, J.S. A randomised, double-blind, placebo-controlled, duloxetine-referenced study of the efficacy and tolerability of vortioxetine in the acute treatment of adults with generalised anxiety disorder. Int. J. Clin. Pract. 2013, 68, 49–59. [Google Scholar] [CrossRef]
- Rothschild, A.J.; Mahableshwarkar, A.R.; Jacobsen, P.; Yan, M.; Sheehan, D.V. Vortioxetine (Lu AA21004) 5 mg in generalized anxiety disorder: Results of an 8-week randomized, double-blind, placebo-controlled clinical trial in the United States. Eur. Neuropsychopharmacol. 2012, 22, 858–866. [Google Scholar] [CrossRef]
- Bidzan, L.; Mahableshwarkar, A.R.; Jacobsen, P.; Yan, M.; Sheehan, D.V. Vortioxetine (Lu AA21004) in generalized anxiety disorder: Results of an 8-week, multinational, randomized, double-blind, placebo-controlled clinical trial. Eur. Neuropsychopharmacol. 2012, 22, 847–857. [Google Scholar] [CrossRef]
- Baldwin, D.S.; Loft, H.; Florea, I. Lu AA21004, a multimodal psychotropic agent, in the prevention of relapse in adult patients with generalized anxiety disorder. Int. Clin. Psychopharmacol. 2012, 27, 197–207. [Google Scholar] [CrossRef]
- Chen, G.; Nomikos, G.G.; Affinito, J.; Jacobson, W.; Zhao, Z.; Wang, S.; Xie, J. Effects of Intrinsic Factors on the Clinical Pharmacokinetics of Vortioxetine. Clin. Pharmacol. Drug Dev. 2018, 7, 880–888. [Google Scholar] [CrossRef]
- Matsuno, K.; Nakamura, K.; Aritomi, Y.; Nishimura, A. Pharmacokinetics, Safety, and Tolerability of Vortioxetine Following Single- and Multiple-Dose Administration in Healthy Japanese Adults. Clin. Pharmacol. Drug Dev. 2018, 7, 319–331. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Nomikos, G.G.; Affinito, J.; Zhao, Z. Lack of Effect of Vortioxetine on the Pharmacokinetics and Pharmacodynamics of Ethanol, Diazepam, and Lithium. Clin. Pharmacokinet. 2016, 55, 1115–1127. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.; Højer, A.-M.; Buchberg, J.; Areberg, J.; Nutt, D.J. Differentiated effects of the multimodal antidepressant vortioxetine on sleep architecture: Part 1, a pharmacokinetic/pharmacodynamic comparison with paroxetine in healthy men. J. Psychopharmacol. 2015, 29, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Zhang, W.; Serenko, M. Lack of effect of multiple doses of vortioxetine on the pharmacokinetics and pharmacodynamics of aspirin and warfarin. J. Clin. Pharmacol. 2015, 55, 671–679. [Google Scholar] [CrossRef]
- Wang, Y.; Nomikos, G.G.; Karim, A.; Munsaka, M.; Serenko, M.; Liosatos, M.; Harris, S. Effect of Vortioxetine on Cardiac Repolarization in Healthy Adult Male Subjects: Results of a Thorough QT/QTc Study. Clin. Pharmacol. Drug Dev. 2013, 2, 298–309. [Google Scholar] [CrossRef]
- Chen, G.; Lee, R.; Højer, A.-M.; Buchbjerg, J.K.; Serenko, M.; Zhao, Z. Pharmacokinetic drug interactions involving vortioxetine (Lu AA21004), a multimodal antidepressant. Clin. Drug Investig. 2013, 33, 727–736. [Google Scholar] [CrossRef]
- Yang, Y.K.; Chen, C.-S.; Tsai, C.-F.; Chang, C.-M.; Lai, T.-J.; Lee, C.-T.; Lin, C.-C.; Lan, T.-H.; Herr, K.J. A Taiwanese study on real-world evidence with vortioxetine in patients with major depression in Asia (TREVIDA). Curr. Med. Res. Opin. 2021, 37, 2163–2173. [Google Scholar] [CrossRef]
- Kim, H.; Baik, S.Y.; Kim, Y.W.; Lee, S.-H. Improved cognitive function in patients with major depressive disorder after treatment with vortioxetine: A EEG study. Neuropsychopharmacol. Rep. 2022, 42, 21–31. [Google Scholar] [CrossRef]
- Bose, R.; Hamdani, S.U.; Minhas, F.A.; Herr, K.J. A comparison of real-world effectiveness of vortioxetine along the treatment algorithm for major depressive disorder. Curr. Med. Res. Opin. 2022, 38, 661–671. [Google Scholar] [CrossRef]
- Mccue, M.; Sarkey, S.; Eramo, A.; François, C.; Parikh, S.V. Using the Goal Attainment Scale adapted for depression to better understand treatment outcomes in patients with major depressive disorder switching to vortioxetine: A phase 4, single-arm, open-label, multicenter study. BMC Psychiatry 2021, 21, 622. [Google Scholar] [CrossRef]
- De Carlo, V.; Vismara, M.; Grancini, B.; Benatti, B.; Bosi, M.F.; Colombo, A.; Viganò, C.A.; Dell’osso, B. Effectiveness, tolerability, and dropout rates of vortioxetine in comorbid depression: A naturalistic study. Hum. Psychopharmacol. Clin. Exp. 2020, 35, e2750. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Xiao, L.; Ren, H.; Simonsen, K.; Ma, J.; Xu, X.; Guo, P.; Wang, Z.; Bai, L.; Heldbo Reines, E.; et al. Effectiveness and Safety of Vortioxetine for Major Depressive Disorder in Real-World Clinical Practice: Results from the Single-Arm RELIEVE China Study. Neuropsychiatr. Dis. Treat. 2022, 18, 1939–1950. [Google Scholar] [CrossRef] [PubMed]
- Almeida, S.S.; Christensen, M.C.; Simonsen, K.; Adair, M. Effectiveness of vortioxetine in patients with major depressive disorder and co-morbid generalized anxiety disorder in routine clinical practice: A subgroup analysis of the RELIEVE study. J. Psychopharmacol. 2023, 37, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Mattingly, G.W.; Ren, H.; Christensen, M.C.; Katzman, M.A.; Polosan, M.; Simonsen, K.; Hammer-Helmich, L. Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice: Results of the RELIEVE Study. Front. Psychiatry 2022, 13, 824831. [Google Scholar] [CrossRef] [PubMed]
- Polosan, M.; Rabbani, M.; Christensen, M.C.; Simonsen, K.; Ren, H. Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice: French Cohort Results from the Global RELIEVE Study. Neuropsychiatr. Dis. Treat. 2022, 18, 1963–1974. [Google Scholar] [CrossRef]
- De Filippis, S.; Pugliese, A.; Christensen, M.C.; Rosso, G.; Di Nicola, M.; Simonsen, K.; Ren, H. Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice in Italy: Results from the RELIEVE Study. Neuropsychiatr. Dis. Treat. 2022, 18, 1665–1677. [Google Scholar] [CrossRef]
- Mattingly, G.; Brunner, E.; Chrones, L.; Lawrence, D.F.; Simonsen, K.; Ren, H. Effectiveness of vortioxetine for major depressive disorder in real-world clinical practice: US cohort results from the global RELIEVE study. Front. Psychiatry 2023, 13, 977560. [Google Scholar] [CrossRef]
- Di Nicola, M.; Pepe, M.; Montanari, S.; Spera, M.C.; Panaccione, I.; Simonetti, A.; Sani, G. Vortioxetine improves physical and cognitive symptoms in patients with post-COVID-19 major depressive episodes. Eur. Neuropsychopharmacol. 2023, 70, 21–28. [Google Scholar] [CrossRef]
- De Filippis, S.; Lombardozzi, G.; Matrone, M.; Amici, E.; Trovini, G.; Perrini, F.; Di Giovanni, A.; Giovanetti, V.; Kotzalidis, G.D. Differential Response to Three Antidepressants in Patients with Major Depressive Episode Who Suffered COVID-19-Related Trauma. Curr. Neuropharmacol. 2022, 20, 2393–2407. [Google Scholar] [CrossRef]
- Di Nicola, M.; Dell’osso, B.; Peduto, I.; Cipelli, R.; Pugliese, A.C.; Signorelli, M.S.; Ventriglio, A.; Martinotti, G. Adherence to, and Persistence of, Antidepressant Therapy in Patients with Major Depressive Disorder: Results from a Population-based Study in Italy. Curr. Neuropharmacol. 2023, 21, 727–739. [Google Scholar] [CrossRef]
- Moon, S.W.; Kim, J.W.; Kim, D.H.; Lee, K.Y.; Reines, E.H.; Lee, M.; Park, Y.J. Safety and effectiveness of vortioxetine for major depressive disorder: Real-world evidence from a population-based study in South Korea. Front. Psychiatry 2023, 14, 1075939. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.C.; Schmidt, S.; Grande, I. Effectiveness of vortioxetine in patients with major depressive disorder comorbid with generalized anxiety disorder: Results of the RECONNECT study. J. Psychopharmacol. 2022, 36, 566–577. [Google Scholar] [CrossRef] [PubMed]
- Di Nicola, M.; Pepe, M.; Panaccione, I.; Moccia, L.; Dattoli, L.; Molinaro, M.; Sani, G.; Janiri, L.; Mcintyre, R.S. Effect of vortioxetine in subjects with major depressive and alcohol use disorders: A 6-month retrospective analysis. CNS Spectr. 2020, 27, 73–81. [Google Scholar] [CrossRef] [PubMed]
- De Berardis, D.; Fornaro, M.; Anastasia, A.; Vellante, F.; Olivieri, L.; Rapini, G.; Serroni, N.; Orsolini, L.; Valchera, A.; Carano, A.; et al. Adjunctive vortioxetine for SSRI-resistant major depressive disorder: A “real-world” chart review study. Braz. J. Psychiatry 2020, 42, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Bruno, A.; Zoccali, R.A.; Troili, G.M.; Scala, L.; Pandolfo, G.; Cedro, C.; Mento, C.; Santoro, V.; Spina, E.; Muscatello, M.R.A. Vortioxetine on Cognition in Schizophrenia. J. Clin. Psychopharmacol. 2020, 40, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Reznik, A.M.; Syunyakov, T.S.; Mudrak, A.V.; Zakharov, N.B.; Popova, Z.B.; Khoroshilova, A.N.; Khurbatova, I.G.; Saifulina, A.M.; Eliseenko, A.M.; Matvievskaya, T.K.; et al. Treatment of Depression with Vortioxetine and Second Generation Antipsychotics During the Period of Remission Formation in Schizophrenia (Interim Data Analysis). Consort. Psychiatr. 2023, 4, 18–36. [Google Scholar] [CrossRef]
- Redaelli, S.; Porffy, L.; Oloyede, E.; Dzahini, O.; Lewis, G.; Lobo, M.; Whiskey, E.; Shergill, S.S. Vortioxetine as adjunctive therapy in the treatment of schizophrenia. Ther. Adv. Psychopharmacol. 2022, 12, 20451253221110014. [Google Scholar] [CrossRef] [PubMed]
- Siwek, M.; Chrobak, A.; Sołtys, Z.; Dudek, D.; Krupa, A.; Rybakowski, J. A naturalistic, 24-week, open-label, add-on study of vortioxetine in bipolar depression. Psychiatr. Pol. 2022, 56, 509–522. [Google Scholar] [CrossRef]
- Adamo, D.; Pecoraro, G.; Aria, M.; Favia, G.; Mignogna, M.D. Vortioxetine in the Treatment of Mood Disorders Associated with Burning Mouth Syndrome: Results of an Open-Label, Flexible-Dose Pilot Study. Pain Med. 2019, 21, 185–194. [Google Scholar] [CrossRef]
- Zizolfi, D.; Poloni, N.; Caselli, I.; Ielmini, M.; Lucca, G.; Diurni, M.; Cavallini, G.; Callegari, C. Resilience and recovery style: A retrospective study on associations among personal resources, symptoms, neurocognition, quality of life and psychosocial functioning in psychotic patients. Psychol. Res. Behav. Manag. 2019, 12, 385–395. [Google Scholar] [CrossRef]
- Shah, A.; Northcutt, J. An open-label, flexible dose adaptive study evaluating the efficacy of vortioxetine in subjects with panic disorder. Ann. Gen. Psychiatry 2018, 17, 19. [Google Scholar] [CrossRef] [PubMed]
- Cumbo, E.; Adair, M.; Åstrom, D.O.; Christensen, M.C. Effectiveness of vortioxetine in patients with major depressive disorder and comorbid Alzheimer’s disease in routine clinical practice: An analysis of a post-marketing surveillance study in South Korea. Front. Aging Neurosci. 2023, 14, 1037816. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.C.; Schmidt, S.N.; Grande, I. Effectiveness of vortioxetine in patients with major depressive disorder and early-stage dementia: The MEMORY study. J. Affect. Disord. 2023, 338, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.N.; Tan, C. Vortioxetine improves cognition in mild cognitive impairment. Int. Clin. Psychopharmacol. 2021, 36, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Santos García, D.; Alonso Losada, M.G.; Cimas Hernando, I.; Cabo López, I.; Yáñez Baña, R.; Alonso Redondo, R.; Paz González, J.M.; Cores Bartolomé, C.; Feal Painceiras, M.J.; Íñiguez Alvarado, M.C.; et al. Vortioxetine Improves Depressive Symptoms and Cognition in Parkinson’s Disease Patients with Major Depression: An Open-Label Prospective Study. Brain Sci. 2022, 12, 1466. [Google Scholar] [CrossRef] [PubMed]
- Gamberini, G.; Masuccio, F.G.; Ferriero, G.; Cattaneo, D.; Solaro, C. Safety and efficacy of vortioxetine on depressive symptoms and cognition in post-stroke patients: A pilot study. J. Affect. Disord. 2021, 286, 108–109. [Google Scholar] [CrossRef]
- Christensen, M.C.; Adair, M.; Loft, H.; Mcintyre, R.S. The Motivation and Energy Inventory (MEI): Analysis of the clinically relevant response threshold in patients with major depressive disorder and emotional blunting using data from the COMPLETE study. J. Affect. Disord. 2023, 323, 547–553. [Google Scholar] [CrossRef]
- Fagiolini, A.; Florea, I.; Loft, H.; Christensen, M.C. Effectiveness of Vortioxetine on Emotional Blunting in Patients with Major Depressive Disorder with inadequate response to SSRI/SNRI treatment. J. Affect. Disord. 2021, 283, 472–479. [Google Scholar] [CrossRef]
- Aşçibaşi, K.; Çökmüş, F.P.; Dikici, D.S.; Özkan, H.M.; Alçi, D.; Altunsoy, N.; Kuru, E.; Yüzeren, S.; Aydemir, Ö. Evaluation of Emotional Adverse Effects of Antidepressants. J. Clin. Psychopharmacol. 2020, 40, 594–598. [Google Scholar] [CrossRef]
- Ekhart, C.; Van Hunsel, F.; Van Puijenbroek, E.; Chandler, R.; Meldau, E.-L.; Taavola, H.; Norén, G.N. Post-Marketing Safety Profile of Vortioxetine Using a Cluster Analysis and a Disproportionality Analysis of Global Adverse Event Reports. Drug Saf. 2022, 45, 145–153. [Google Scholar] [CrossRef]
- Quilichini, J.-B.; Revet, A.; Garcia, P.; Bouquié, R.; Hamard, J.; Yrondi, A.; Montastruc, F. Comparative effects of 15 antidepressants on the risk of withdrawal syndrome: A real-world study using the WHO pharmacovigilance database. J. Affect. Disord. 2022, 297, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Greenblatt, D.J.; Harmatz, J.S.; Chow, C.R. Vortioxetine Disposition in Obesity. J. Clin. Psychopharmacol. 2018, 38, 172–179. [Google Scholar] [CrossRef]
- Hughes, S.; Lacasse, J.; Fuller, R.R.; Spaulding-Givens, J. Adverse effects and treatment satisfaction among online users of four antidepressants. Psychiatry Res. 2017, 255, 78–86. [Google Scholar] [CrossRef]
- Healy, D.; Mangin, D.; Lochhead, J. Development and persistence of patient-reported visual problems associated with serotonin reuptake inhibiting antidepressants. Int. J. Risk Saf. Med. 2022, 33, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Seifert, J.; Letmaier, M.; Greiner, T.; Schneider, M.; Deest, M.; Eberlein, C.K.; Bleich, S.; Grohmann, R.; Toto, S. Psychotropic drug-induced hyponatremia: Results from a drug surveillance program—An update. J. Neural Transm. 2021, 128, 1249–1264. [Google Scholar] [CrossRef] [PubMed]
- Revet, A.; Montastruc, F.; Roussin, A.; Raynaud, J.-P.; Lapeyre-Mestre, M.; Nguyen, T.T.H. Antidepressants and movement disorders: A postmarketing study in the world pharmacovigilance database. BMC Psychiatry 2020, 20, 308. [Google Scholar] [CrossRef]
- Bordet, C.; Rousseau, V.; Montastruc, F.; Montastruc, J.-L. QT prolongation and vortioxetine: A post-marketing study and comparison with other serotonin reuptake inhibitors. Psychopharmacol 2020, 237, 1245–1247. [Google Scholar] [CrossRef]
- Eugene, A.R. Association of sleep among 30 antidepressants: A population-wide adverse drug reaction study, 2004-2019. PeerJ 2020, 8, e8748. [Google Scholar] [CrossRef]
- Miao, J.; Wang, G.; Hou, J.; Areberg, J.; Zhao, Y.; Højer, A.-M.; Ettrup, A. Pharmacokinetics and Safety of Vortioxetine in the Chinese Population. Adv. Ther. 2019, 36, 3134–3146. [Google Scholar] [CrossRef]
- Mazhar, F.; Pozzi, M.; Gentili, M.; Scatigna, M.; Clementi, E.; Radice, S.; Carnovale, C. Association of Hyponatraemia and Antidepressant Drugs: A Pharmacovigilance–Pharmacodynamic Assessment Through an Analysis of the US Food and Drug Administration Adverse Event Reporting System (FAERS) Database. CNS Drugs 2019, 33, 581–592. [Google Scholar] [CrossRef]
- Woroń, J.; Siwek, M.; Gorostowicz, A. Adverse effects of interactions between antidepressants and medications used in treatment of cardiovascular disorders. Psychiatr. Pol. 2019, 53, 977–995. [Google Scholar] [CrossRef]
- Ozkan, H.M. Galactorrhea and hyperprolactinemia during vortioxetine use: Case report. Turk. J. Biochem. 2018, 44, 105–107. [Google Scholar] [CrossRef]
- Okumus, B. A serious dermatological side effect due to vortioxetine: A case report. J. Psychiatry Neurol Sci. 2020, 33, 87–91. [Google Scholar] [CrossRef]
- Cetin, M.; Kose, S. Serious dermatological adverse effects of vortioxetine: Two cases. Psychiatry Clin. Psychopharmacol. 2018, 28, 355–357. [Google Scholar] [CrossRef]
- Ay, R.; Aytas, O. Acneiform eruption associated with the use of vortioxetine. Psychiatry Clin. Psychopharmacol. 2018, 29, 226–228. [Google Scholar] [CrossRef]
- Woroń, J.; Jurkiewicz, D.; Rapiejko, P.; Lorkowska- Zawicka, B.; Tymiński, R.; Wordliczek, J. Drug-induced diseases in otolaryngology—Causes, clinical signs, treatment. Otolaryngol. Pol. 2021, 75, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.H. Rapid onset of hemoptysis in a young man treated with vortioxetine. Psychiatry Clin. Neurosci. 2021, 75, 266–267. [Google Scholar] [CrossRef]
- Romigi, A.; Vitrani, G.; Caccamo, M.; Centonze, D. Restless Legs Syndrome Related to Vortioxetine. J. Clin. Psychopharmacol. 2019, 39, 514–516. [Google Scholar] [CrossRef]
- Moodliar, S.; Naguy, A.; Alkhadhari, S. Vortioxetine-Related Call–Fleming Syndrome. Am. J. Ther. 2019, 28, e258–e260. [Google Scholar] [CrossRef]
- Kocamer Şahin, Ş.; Elboga, G.; Altindag, A. Meige Syndrome Related to Vortioxetine in 2 Sisters. J. Clin. Psychopharmacol. 2019, 39, 679–681. [Google Scholar] [CrossRef]
- Tunc, E.B.; Tunc, S. Vortioxetine Induced Hypomania: A Case Presentation and Review of the Literature. Clin. Psychopharmacol. Neurosci. 2022, 20, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Sobreira, G.; Oliveira, J.; Brissos, S. Vortioxetine-induced manic mood switch in patient with previously unknown bipolar disorder. Braz. J. Psychiatry 2017, 39, 86. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M.G.; Rossetti, A.; Botti, E.R.; Clerici, M. Vortioxetine overdose in a suicidal attempt: A case report. Medicine 2018, 97, e10788. [Google Scholar] [CrossRef]
- Siwek, M.; Gorostowicz, A.; Bosak, M.; Dudek, D. Case Report: Vortioxetine in the Treatment of Depressive Symptoms in Patients with Epilepsy-Case Series. Front. Pharmacol. 2022, 13, 852042. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Jiang, J.; Ng, C.H.; Wu, L.; Zhang, P.; Xi, C.; Lai, J.; Xu, Y.; Hu, S.; Wang, Z. Vortioxetine improves rapid eye movement sleep behavior disorder: A case report. Medicine 2020, 99, e21003. [Google Scholar] [CrossRef]
- Crapanzano, C.; Politano, A.; Amendola, C.; Koukouna, D.; Casolaro, I. Vortioxetine-induced nausea and its treatment: A case report. Arch. Clin. Psychiatry 2020, 47, 160–161. [Google Scholar] [CrossRef]
- Pelayo-Terán, J.M.; Martínez-Pérez, M.M.; Zapico-Merayo, Y. Safety in the use of antidepressants: Vortioxetine-induce hyponatremia in a case report. Rev. Psiquiatr. Salud Ment. Engl. Ed. 2017, 10, 219–220. [Google Scholar] [CrossRef] [PubMed]
- Schweimer, J.V.; Brouard, J.T.; Li, Y.; Sánchez, C.; Sharp, T. In vivo electrophysiological study of the targeting of 5-HT(3) receptor-expressing cortical interneurons by the multimodal antidepressant, vortioxetine. Eur. J. Neurosci. 2022, 55, 1409–1423. [Google Scholar] [CrossRef]
- Riga, M.S.; Sánchez, C.; Celada, P.; Artigas, F. Involvement of 5-HT 3 receptors in the action of vortioxetine in rat brain: Focus on glutamatergic and GABAergic neurotransmission. Neuropharmacology 2016, 108, 73–81. [Google Scholar] [CrossRef]
- Bétry, C.; Pehrson, A.L.; Etiévant, A.; Ebert, B.; Sánchez, C.; Haddjeri, N. The rapid recovery of 5-HT cell firing induced by the antidepressant vortioxetine involves 5-HT3 receptor antagonism. Int. J. Neuropsychopharmacol. 2013, 16, 1115–1127. [Google Scholar] [CrossRef]
- Foster, P.; Oxman, T. A descriptive study of adjustment disorder diagnoses in general hospital patients. Ir. J. Psychol. Med. 1994, 11, 153–157. [Google Scholar] [CrossRef]
- O’donnell, M.L.; Agathos, J.A.; Metcalf, O.; Gibson, K.; Lau, W. Adjustment Disorder: Current Developments and Future Directions. Int. J. Environ. Res. Public Health 2019, 16, 2537. [Google Scholar] [CrossRef]
- Koenig, H.G.; O’connor, C.M.; Guarisco, S.A.; Zabel, K.M.; Ford, S.M. Depressive Disorder in Older Medical Inpatients on General Medicine and Cardiology Services at a University Teaching Hospital. Am. J. Geriatr. Psychiatry 1993, 1, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Koenig, H.G. Depression in Elderly Hospitalized Patients with Medical Illness. Arch. Intern. Med. 1988, 148, 1929. [Google Scholar] [CrossRef] [PubMed]
- Wetterling, T.; Junghanns, K. Affective disorders in older inpatients. Int. J. Geriatr. Psychiatry 2004, 19, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, M.; Martinez, J.H.; Dalrymple, K.; Chelminski, I.; Young, D. “Subthreshold” Depression. J. Clin. Psychiatry 2013, 74, 470–476. [Google Scholar] [CrossRef]
- Massa, E.; Donisi, C.; Liscia, N.; Madeddu, C.; Impera, V.; Mariani, S.; Scartozzi, M.; Lai, E. The Difficult Task of Diagnosing Depression in Elderly People with Cancer: A Systematic Review. Clin. Pract. Epidemiol. Ment. Health 2021, 17, 295–306. [Google Scholar] [CrossRef]
- Snyder, S.; Strain, J.J.; Wolf, D. Differentiating major depression from adjustment disorder with depressed mood in the medical setting. Gen. Hosp. Psychiatry 1990, 12, 159–165. [Google Scholar] [CrossRef]
- Casey, P.; Maracy, M.; Kelly, B.D.; Lehtinen, V.; Ayuso-Mateos, J.-L.; Dalgard, O.S.; Dowrick, C. Can adjustment disorder and depressive episode be distinguished? Results from ODIN. J. Affect. Disord. 2006, 92, 291–297. [Google Scholar] [CrossRef]
- Undurraga, J.; Vázquez, G.H.; Tondo, L.; Baldessarini, R.J. Antidepressant responses in direct comparisons of melancholic and non-melancholic depression. J. Psychopharmacol. 2020, 34, 1335–1341. [Google Scholar] [CrossRef]
- Parker, G. ‘New’ and ‘old’ antidepressants: All equal in the eyes of the lore? Br. J. Psychiatry 2001, 179, 95–96. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: A systematic review and network meta-analysis. Lancet 2018, 391, 1357–1366. [Google Scholar] [CrossRef] [PubMed]
- Citrome, L. Vortioxetine for major depressive disorder: An indirect comparison with duloxetine, escitalopram, levomilnacipran, sertraline, venlafaxine, and vilazodone, using number needed to treat, number needed to harm, and likelihood to be helped or harmed. J. Affect. Disord. 2016, 196, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Kishi, T.; Ikuta, T.; Sakuma, K.; Okuya, M.; Hatano, M.; Matsuda, Y.; Iwata, N. Antidepressants for the treatment of adults with major depressive disorder in the maintenance phase: A systematic review and network meta-analysis. Mol. Psychiatry 2023, 28, 402–409. [Google Scholar] [CrossRef]
- Behlke, L.M.; Lenze, E.J.; Carney, R.M. The Cardiovascular Effects of Newer Antidepressants in Older Adults and Those with or At High Risk for Cardiovascular Diseases. CNS Drugs 2020, 34, 1133–1147. [Google Scholar] [CrossRef]
- He, H.; Wang, W.; Lyu, J.; Zheng, J.; Guo, L.; An, X.; Fan, Y.; Ma, X. Efficacy and tolerability of different doses of three new antidepressants for treating major depressive disorder: A PRISMA-compliant meta-analysis. J. Psychiatr. Res. 2018, 96, 247–259. [Google Scholar] [CrossRef]
- Wagner, G.; Schultes, M.-T.; Titscher, V.; Teufer, B.; Klerings, I.; Gartlehner, G. Efficacy and safety of levomilnacipran, vilazodone and vortioxetine compared with other second-generation antidepressants for major depressive disorder in adults: A systematic review and network meta-analysis. J. Affect. Disord. 2018, 228, 1–12. [Google Scholar] [CrossRef]

| Patient | Age | Sex | Medical Comorbidity | Surgery during Hospitalization |
|---|---|---|---|---|
| P01 | 65 | M | High-grade retroperitoneal sarcoma Pleuropulmonary infection Pulmonary embolism | En-bloc resection of sarcoma (including the head of pancreas, duodenum, right kidney, right adrenal gland and right colon) |
| P02 | 77 | M | Complicated diverticulosis Chronic ischemic heart disease Atrial fibrillation COPD Chronic anemia Type 2 diabetes mellitus | Sigmoidectomy |
| P03 | 64 | F | Advanced endometrial carcinoma Intestinal occlusion Multiple electrolyte imbalance | Decompressive colostomy |
| P04 | 77 | M | Class 3 obesity Type 2 diabetes mellitus Systemic arterial hypertension Atrial fibrillation Respiratory insufficiency Burns (15% TBSA) | Multiple escharotomies and reconstructive procedures |
| P05 | 74 | F | Chronic kidney disease Recurrent urinary infections Polymetastatic thyroid carcinoma | None |
| P06 | 73 | M | Ischemic heart disease Atrial fibrillation Long QT Thigh sarcoma Type 2 diabetes mellitus | Thigh sarcoma excision (limb-sparing surgery) |
| Patient | Vortioxetine Dose | Observation Length | Associated Psychotropics | Non-Psychiatric Pharmacotherapy |
|---|---|---|---|---|
| P01 | 5 mg | 4 weeks | None | Bisoprolol Pantoprazole Enoxaparin Ondansetron |
| P02 | 5 mg | 4 weeks | Delorazepam 0.5 mg/day | Pantoprazole Metoprolol Amiodarone Linagliptin Furosemide Umeclidinium Mesalazine Warfarin |
| P03 | 10 mg | 1 week | Morphine 40 mg/day Buprenorphine Patch 70 mg/h Pregabalin 75 mg/night | Ondansetron Domperidone Chemotherapy (Doxorubicin and Cisplatin) |
| P04 | 10 mg | 6 weeks | Melatonin 2 mg/night Pregabalin 150 mg/day | Pantoprazole Olmesartan Amlodipine Furosemide Amiodarone |
| P05 | 10 mg | 1 week | Lorazepam 1 mg/night | Ursodeoxycholic acid Fondaparinux Metoclopramide Pantoprazole Levothyroxine |
| P06 | 10 mg | 8 weeks | Divalproex 750 mg/day Delorazepam 0.5 mg/night | Metformin Ranolazine Zofenopril/HCTZ Pantoprazole Metoprolol Furosemide Rivaroxaban |
| Patient | CGI-S Baseline | CGI-S Follow-Up | CGI-I | CGI-EI | Safety Issues | Discharge |
|---|---|---|---|---|---|---|
| P01 | 4 | 3 | 2 | 1 | None | Discharged to home |
| P02 | 3 | 2 | 2 | 5 | None | Discharged to home |
| P03 | 4 | 4 | 4 | 13 | None | Transferred to palliative care facility |
| P04 | 4 | 3 | 3 | 9 | None | Transferred to intermediate care facility |
| P05 | 3 | 2 | 2 | 5 | None | Discharged to home |
| P06 | 5 | 3 | 2 | 5 | Nausea | Discharged to home |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weiss, F.; Pacciardi, B.; D’Alessandro, G.; Caruso, V.; Maremmani, I.; Pini, S.; Perugi, G. The Role of Vortioxetine in the Treatment of Depressive Symptoms in General Hospital Psychiatry: A Case-Series and PRISMA-Compliant Systematic Review of the Literature. J. Clin. Med. 2024, 13, 531. https://doi.org/10.3390/jcm13020531
Weiss F, Pacciardi B, D’Alessandro G, Caruso V, Maremmani I, Pini S, Perugi G. The Role of Vortioxetine in the Treatment of Depressive Symptoms in General Hospital Psychiatry: A Case-Series and PRISMA-Compliant Systematic Review of the Literature. Journal of Clinical Medicine. 2024; 13(2):531. https://doi.org/10.3390/jcm13020531
Chicago/Turabian StyleWeiss, Francesco, Bruno Pacciardi, Giulia D’Alessandro, Valerio Caruso, Icro Maremmani, Stefano Pini, and Giulio Perugi. 2024. "The Role of Vortioxetine in the Treatment of Depressive Symptoms in General Hospital Psychiatry: A Case-Series and PRISMA-Compliant Systematic Review of the Literature" Journal of Clinical Medicine 13, no. 2: 531. https://doi.org/10.3390/jcm13020531
APA StyleWeiss, F., Pacciardi, B., D’Alessandro, G., Caruso, V., Maremmani, I., Pini, S., & Perugi, G. (2024). The Role of Vortioxetine in the Treatment of Depressive Symptoms in General Hospital Psychiatry: A Case-Series and PRISMA-Compliant Systematic Review of the Literature. Journal of Clinical Medicine, 13(2), 531. https://doi.org/10.3390/jcm13020531