


Elastic Compression Dressing after Total Hip Replacement Slightly Reduces Leg Swelling: A Randomized Controlled Trial


Abstract
:1. Introduction
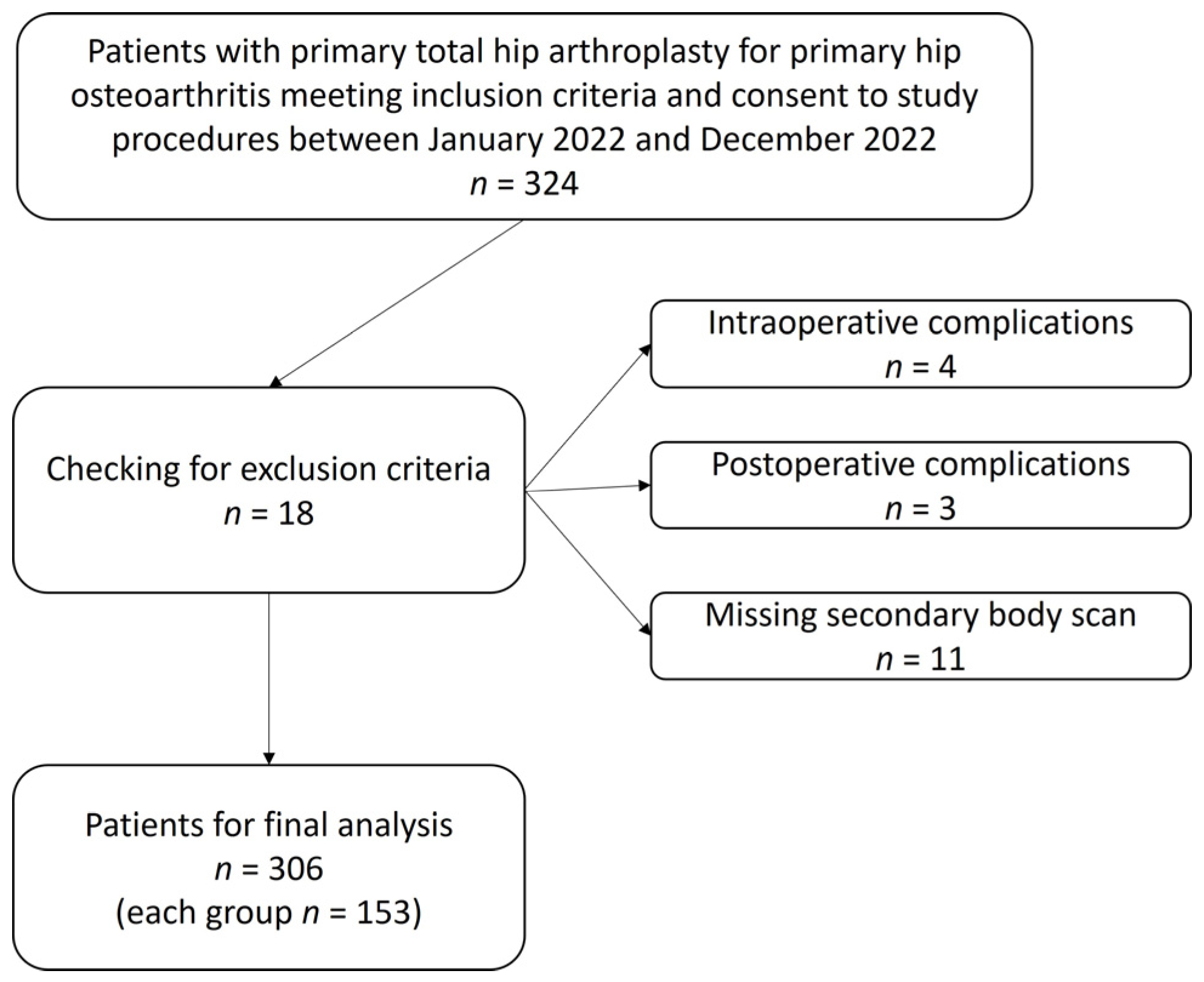
2. Materials and Methods
2.1. Leg Swelling
2.2. Blood Loss
2.3. Sample Size and Power
2.4. Statistical Analysis
3. Results
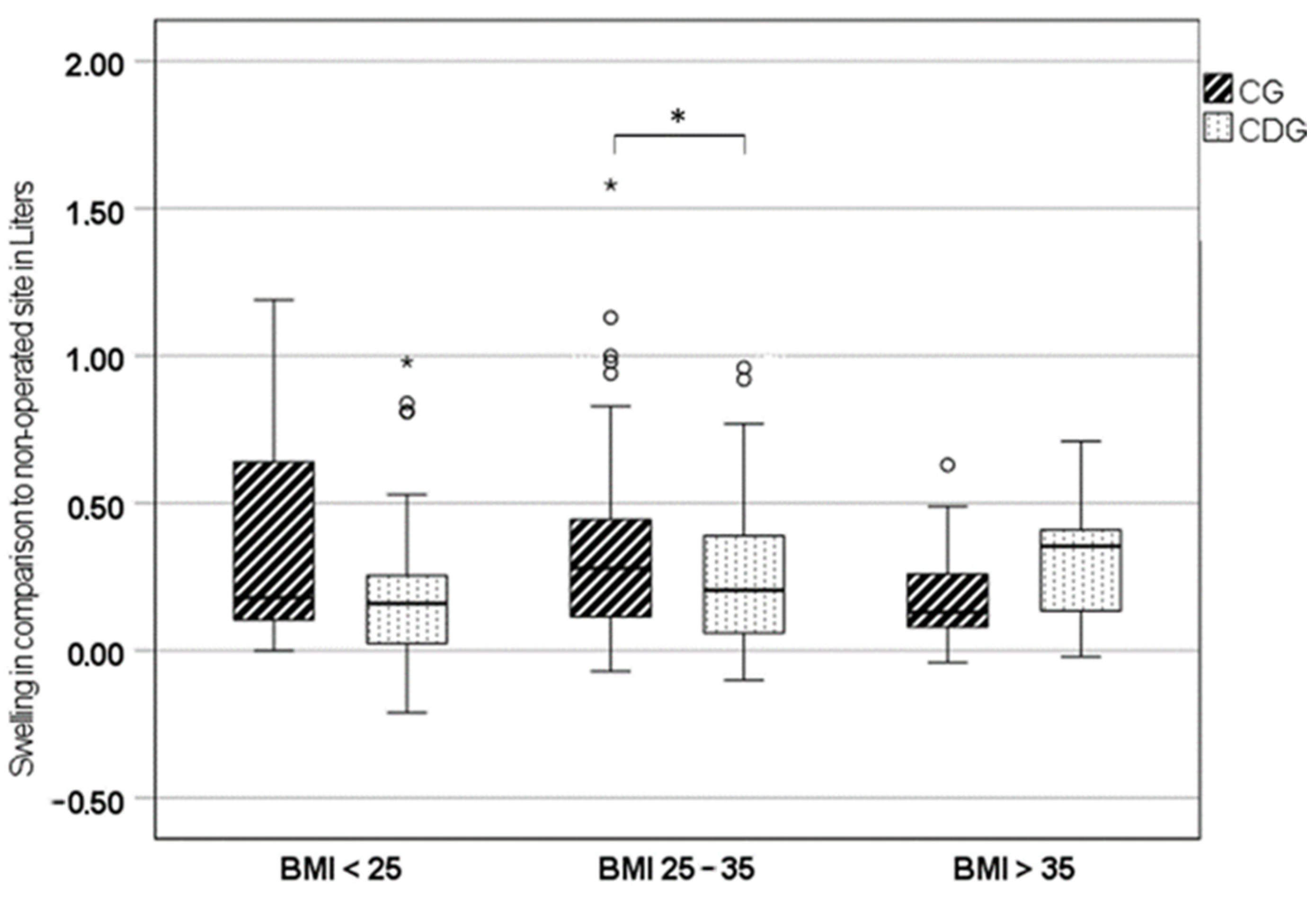
3.1. Leg Swelling
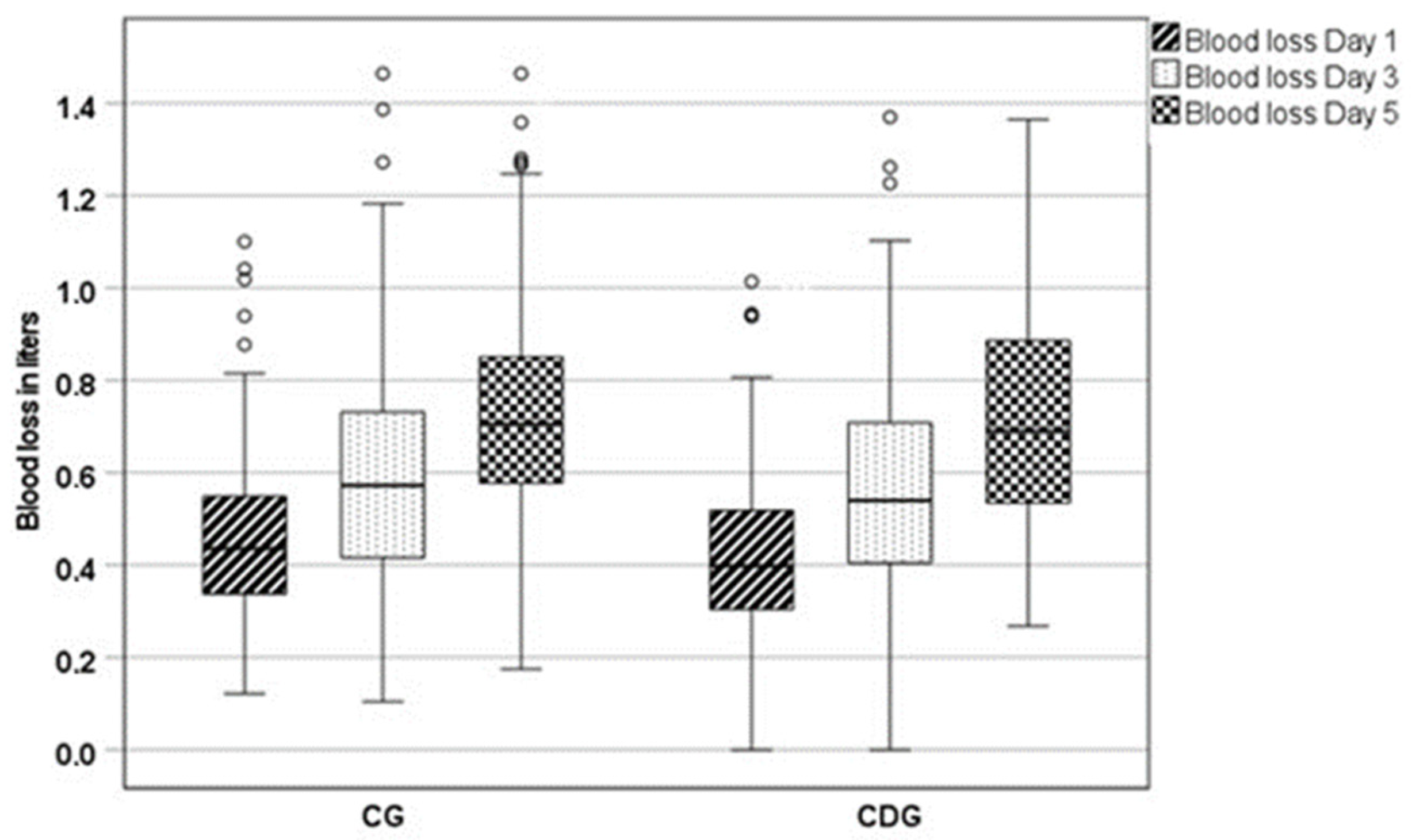
3.2. Blood Loss
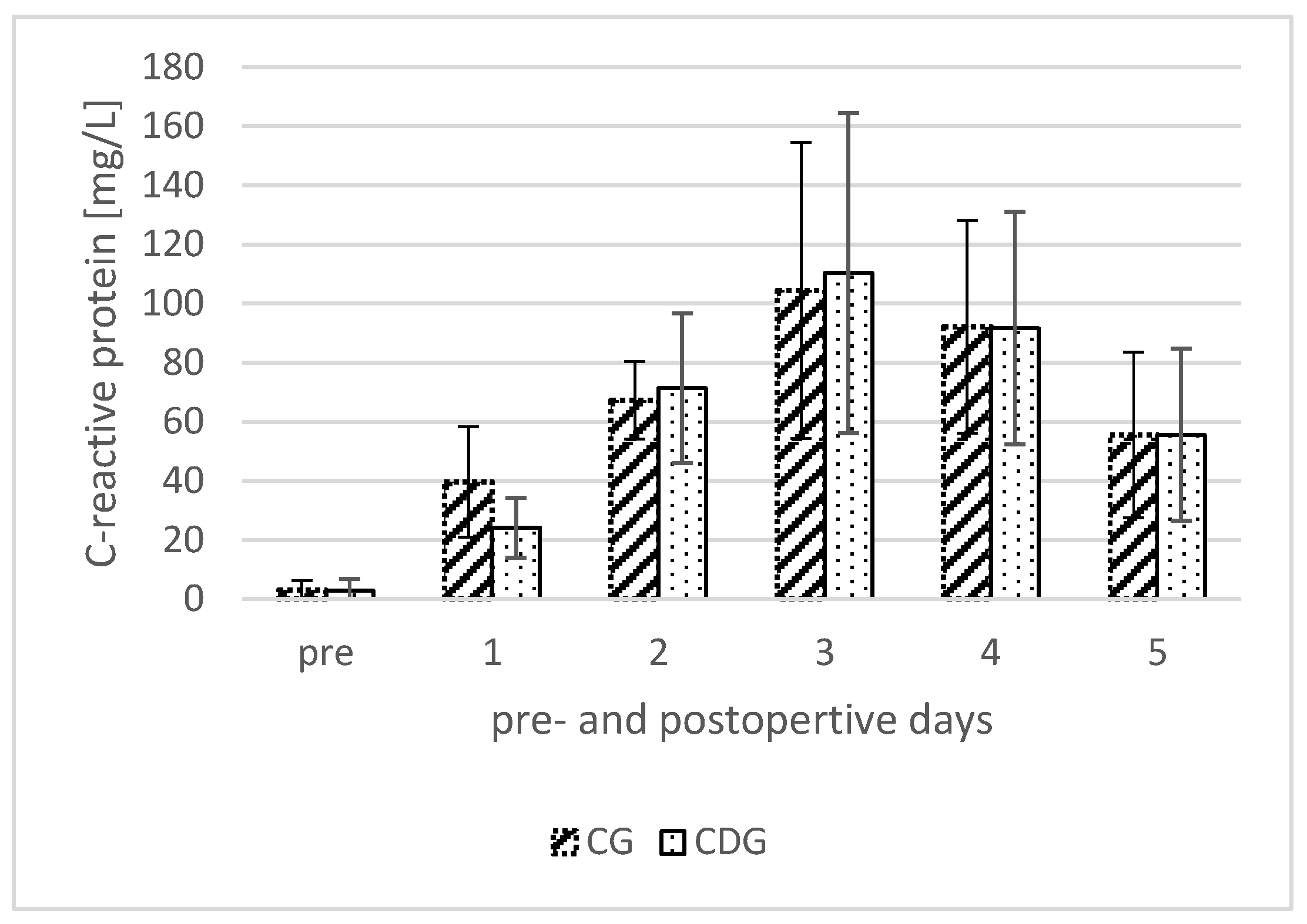
3.3. C-Reactive Protein (CRP)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rainer, W.G.; Kolz, J.M.; Wyles, C.C.; Houdek, M.T.; Perry, K.I.; Lewallen, D.G. Lymphedema Is a Significant Risk Factor for Failure After Primary Total Hip Arthroplasty. J. Bone Jt. Surg. Am. 2022, 104, 55–61. [Google Scholar] [CrossRef]
- Everhart, J.S.; Sojka, J.H.; Mayerson, J.L.; Glassman, A.H.; Scharschmidt, T.J. Perioperative Allogeneic Red Blood-Cell Transfusion Associated with Surgical Site Infection After Total Hip and Knee Arthroplasty. J. Bone Jt. Surg. Am. 2018, 100, 288–294. [Google Scholar] [CrossRef]
- Aziz, K.T.; Best, M.J.; Skolasky, R.L.; Ponnusamy, K.E.; Sterling, R.S.; Khanuja, H.S. Lupus and Perioperative Complications in Elective Primary Total Hip or Knee Arthroplasty. Clin. Orthop. Surg. 2020, 12, 37–42. [Google Scholar] [CrossRef]
- Akti, S.; Zeybek, H.; Bilekli, A.B.; Çelebi, N.Ö.; Erdem, Y.; Çankaya, D. The effect of tranexamic acid on hidden blood loss in total hip arthroplasty. Jt. Dis. Relat. Surg. 2022, 33, 102–108. [Google Scholar] [CrossRef]
- Migliorini, F.; Biagini, M.; Rath, B.; Meisen, N.; Tingart, M.; Eschweiler, J. Total hip arthroplasty: Minimally invasive surgery or not? Meta-analysis of clinical trials. Int. Orthop. 2019, 43, 1573–1582. [Google Scholar] [CrossRef]
- Johansson, T.; Pettersson, L.-G.; Lisander, B. Tranexamic acid in total hip arthroplasty saves blood and money: A randomized, double-blind study in 100 patients. Acta Orthop. 2005, 76, 314–319. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, X.; Chen, Y.; Wang, Q.; Jiang, Y.; Zeng, B. Hidden blood loss after total hip arthroplasty. J. Arthroplast. 2011, 26, 1100–1105.e1. [Google Scholar] [CrossRef]
- Kragh, J.F.; Walters, T.J.; Baer, D.G.; Fox, C.J.; Wade, C.E.; Salinas, J.; Holcomb, J.B. Practical use of emergency tourniquets to stop bleeding in major limb trauma. J. Trauma 2008, 64, S38–S49; discussion S49–S50. [Google Scholar] [CrossRef]
- Kolz, J.M.; Rainer, W.G.; Wyles, C.C.; Houdek, M.T.; Perry, K.I.; Lewallen, D.G. Lymphedema: A Significant Risk Factor for Infection and Implant Failure After Total Knee Arthroplasty. J. Am. Acad. Orthop. Surg. 2020, 28, 996–1002. [Google Scholar] [CrossRef]
- Grada, A.A.; Phillips, T.J. Lymphedema: Diagnostic workup and management. J. Am. Acad. Dermatol. 2017, 77, 995–1006. [Google Scholar] [CrossRef]
- Johansson, T.; Engquist, M.; Pettersson, L.-G.; Lisander, B. Blood loss after total hip replacement: A prospective randomized study between wound compression and drainage. J. Arthroplast. 2005, 20, 967–971. [Google Scholar] [CrossRef]
- Hörnberg, I.; Bengtsson, A.; Bergman, B. Kompressionsförband minskar behovet av allogent blod vid höftproteskirurgi. Lakartidningen 2002, 99, 397–399. [Google Scholar]
- Tan, M.; Wu, T.; Guo, J.; Zhang, C.; Fan, Z.; Guo, X. Hemostasis effect of compression dressing therapy after total hip arthroplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2016, 30, 416–420. [Google Scholar]
- Hahn, G.J.; Grant, D.; Bartke, C.; McCartin, J.; Carn, R.M. Wound complications after hip surgery using a tapeless compressive support. Orthop. Nurs. 1999, 18, 43–49. [Google Scholar] [CrossRef]
- Koval, K.J.; Egol, K.A.; Hiebert, R.; Spratt, K.F. Tape blisters after hip surgery: Can they be eliminated completely? Am. J. Orthop. 2007, 36, 261–265. [Google Scholar]
- Rothfusz, C.A.; Emara, A.K.; McLaughlin, J.P.; Molloy, R.M.; Krebs, V.E.; Piuzzi, N.S. Wound Dressings for Hip and Knee Total Joint Arthroplasty: A Narrative Review. JBJS Rev. 2021, 9, e20.00301. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Khan, M.A.; Nizam, I.; Haddad, F.S. Peri-operative interventions producing better functional outcomes and enhanced recovery following total hip and knee arthroplasty: An evidence-based review. BMC Med. 2013, 11, 37. [Google Scholar] [CrossRef]
- Goldstein, W.M.; Branson, J.J. Posterior-lateral approach to minimal incision total hip arthroplasty. Orthop. Clin. N. Am. 2004, 35, 131–136. [Google Scholar] [CrossRef]
- Hartzband, M.A. Posterolateral minimal incision for total hip replacement: Technique and early results. Orthop. Clin. N. Am. 2004, 35, 119–129. [Google Scholar] [CrossRef]
- Röttinger, H. Minimalinvasiver Zugang zum Hüftgelenk (OCM) zur Implantation von Hüftendoprothesen. Oper. Orthop. Traumatol. 2010, 22, 421–430. [Google Scholar] [CrossRef]
- Tischer, T.; Oye, S.; Wolf, A.; Feldhege, F.; Jacksteit, R.; Mittelmeier, W.; Bader, R.; Mau-Moeller, A. Measuring lower limb circumference and volume—Introduction of a novel optical 3D volumetric measurement system. Biomed. Tech. 2020, 65, 237–241. [Google Scholar] [CrossRef]
- Nadler, S.B.; Hidalgo, J.H.; Bloch, T. Prediction of blood volume in normal human adults. Surgery 1962, 51, 224–232. [Google Scholar]
- Donovan, R.L.; Lostis, E.; Jones, I.; Whitehouse, M.R. Estimation of blood volume and blood loss in primary total hip and knee replacement: An analysis of formulae for perioperative calculations and their ability to predict length of stay and blood transfusion requirements. J. Orthop. 2021, 24, 227–232. [Google Scholar] [CrossRef]
- Neumaier, M.; Metak, G.; Scherer, M.A. C-reactive protein as a parameter of surgical trauma: CRP response after different types of surgery in 349 hip fractures. Acta Orthop. 2006, 77, 788–790. [Google Scholar] [CrossRef]
- Shen, H.; Zhang, N.; Zhang, X.; Ji, W. C-reactive protein levels after 4 types of arthroplasty. Acta Orthop. 2009, 80, 330–333. [Google Scholar] [CrossRef]
- Rykov, K.; Reininga, I.H.F.; Sietsma, M.S.; Knobben, B.A.S.; Have, B.L.E.F. ten. Posterolateral vs Direct Anterior Approach in Total Hip Arthroplasty (POLADA Trial): A Randomized Controlled Trial to Assess Differences in Serum Markers. J. Arthroplast. 2017, 32, 3652–3658.e1. [Google Scholar] [CrossRef]
- Tholen, D.W.; Linnet, K.; Kondratovich, M. Protocols for Determination of Limits of Detection and Limits of Quantitation; Approved Guideline, 2nd ed.; NCCLS: Wayne, PA, USA, 2004; Volume 24. [Google Scholar]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Rohe, S.; Röhner, E.; Windisch, C.; Matziolis, G.; Brodt, S.; Böhle, S. Sex Differences in Serum C-Reactive Protein Course after Total Hip Arthroplasty. Clin. Orthop. Surg. 2022, 14, 48–55. [Google Scholar] [CrossRef]
- Matthews, C.N.; Chen, A.F.; Daryoush, T.; Rothman, R.H.; Maltenfort, M.G.; Hozack, W.J. Does an Elastic Compression Bandage Provide Any Benefit After Primary TKA? Clin. Orthop. Relat. Res. 2019, 477, 134–144. [Google Scholar] [CrossRef]
- Liu, P.; Mu, X.; Zhang, Q.; Liu, Z.; Wang, W.; Guo, W. Should compression bandage be performed after total knee arthroplasty? A meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2020, 15, 52. [Google Scholar] [CrossRef]
- Seidel, A.C.; Belczak, C.E.Q.; Campos, M.B.; Campos, R.B.; Harada, D.S. The impact of obesity on venous insufficiency. Phlebology 2015, 30, 475–480. [Google Scholar] [CrossRef]
- van Rij, A.M.; de Alwis, C.S.; Jiang, P.; Christie, R.A.; Hill, G.B.; Dutton, S.J.; Thomson, I.A. Obesity and impaired venous function. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 739–744. [Google Scholar] [CrossRef]
- Willenberg, T.; Clemens, R.; Haegeli, L.M.; Amann-Vesti, B.; Baumgartner, I.; Husmann, M. The influence of abdominal pressure on lower extremity venous pressure and hemodynamics: A human in-vivo model simulating the effect of abdominal obesity. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 849–855. [Google Scholar] [CrossRef]
- Zha, G.-C.; Zhu, X.-R.; Wang, L.; Li, H.-W. Tranexamic acid reduces blood loss in primary total hip arthroplasty performed using the direct anterior approach: A one-center retrospective observational study. J. Orthop. Traumatol. 2022, 23, 12. [Google Scholar] [CrossRef]
- Cao, G.; Huang, Q.; Huang, Z.; Zhang, S.; Luo, Z.; Lei, Y.; Zhou, Z.; Pei, F. The efficacy and safety of multiple-dose oral tranexamic acid on blood loss following total hip arthroplasty: A randomized controlled trial. Int. Orthop. 2019, 43, 299–305. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CDG | CG | p-Value | p-Value (Adjusted *) | |
|---|---|---|---|---|
| Total | 153 | 153 | 1.00 | |
| Male sex | 71 (46.4%) | 65 (42.5%) | 0.49 | |
| Age [y] | 64.07 ± 0.99 | 64.57 ± 11.75 | 0.81 | |
| Obesity | 38 (24.8%) | 34 (22.2%) | 0.59 | |
| Overweight | 118 (77.1%) | 116 (75.8%) | 0.87 | |
| BMI [kg/m2] | 28.66 ± 4.95 | 28.96 ± 5.34 | 0.31 | |
| Diabetes | 22 (14.4%) | 21 (13.7%) | 0.87 | |
| Renal failure | 6 (3.9%) | 11 (7.2%) | 0.21 | |
| Osteoporosis | 12 (7.8%) | 11 (7.2%) | 0.83 | |
| Hypertension | 97 (63.4%) | 91 (59.5%) | 0.48 | |
| Coronary disease | 8 (5.2%) | 8 (5.2%) | 1.00 | |
| Length of stay [d] | 5.93 ± 0.67 | 5.91 ± 0.84 | 0.38 | |
| Surgery time [min] | 51.39 ± 17.39 | 55.40 ± 21.76 | 0.04 | |
| Anterolateral approach | 130 (85.0%) | 132 (86.3%) | 0.87 | |
| Dorsolateral approach | 23 (15.0%) | 21 (13.7%) | 0.81 | |
| Blood transfusion | 0 | 0 | - | |
| p.o. Leg swelling [L] | 0.24 ± 0.23 | 0.31 ± 0.29 | 0.01 | 0.04 |
| EBV [L] | 5.01 ± 1.04 | 4.85 ± 0.97 | 0.09 | - |
| EBL p.o. day 1 [L] | 0.43 ± 0.19 | 0.46 ± 0.18 | 0.05 | 0.24 |
| EBL p.o. day 3 [L] | 0.56 ± 0.25 | 0.61 ± 0.25 | 0.04 | 0.24 |
| EBL p.o. day 5 [L] | 0.72 ± 0.26 | 0.73 ± 0.23 | 0.38 | - |
| CDG | CG | p-Value | |
|---|---|---|---|
| BMI < 25 kg/m2 [n] | 35 | 36 | |
| Leg swelling [L] | 0.22 ± 0.28 | 0.35 ± 0.34 | 0.04 |
| Blood loss p.o. day 1 [L] | 0.34 ± 0.16 | 0.45 ± 0.17 | 0.01 |
| Blood loss p.o. day 3 [L] | 0.50 ± 0.24 | 0.61 ± 0.21 | 0.06 |
| Blood loss p.o. day 5 [L] | 0.62 ± 0.24 | 0.68 ± 0.17 | 0.14 |
| BMI 25–35 kg/m2 [n] | 96 | 106 | |
| Leg swelling [L] | 0.24 ± 0.22 | 0.32 ± 0.28 | 0.02 |
| Blood loss p.o. day 1 [L] | 0.45 ± 0.19 | 0.46 ± 0.18 | 0.33 |
| Blood loss p.o. day 3 [L] | 0.56 ± 0.23 | 0.60 ± 0.26 | 0.10 |
| Blood loss p.o. day 5 [L] | 0.72 ± 0.24 | 0.72 ± 0.23 | 0.47 |
| BMI > 35 kg/m2 [n] | 12 | 21 | |
| Leg swelling [L] | 0.31 ± 0.21 | 0.20 ± 0.18 | 0.06 |
| Blood loss p.o. day 1 [L] | 0.49 ± 0.20 | 0.49 ± 0.17 | 0.49 |
| Blood loss p.o. day 3 [L] | 0.68 ± 0.38 | 0.63 ± 0.31 | 0.33 |
| Blood loss p.o. day 5 [L] | 0.98 ± 0.27 | 0.82 ± 0.25 | 0.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rohe, S.; Böhle, S.; Matziolis, G.; Layher, F.; Brodt, S. Elastic Compression Dressing after Total Hip Replacement Slightly Reduces Leg Swelling: A Randomized Controlled Trial. J. Clin. Med. 2024, 13, 2207. https://doi.org/10.3390/jcm13082207
Rohe S, Böhle S, Matziolis G, Layher F, Brodt S. Elastic Compression Dressing after Total Hip Replacement Slightly Reduces Leg Swelling: A Randomized Controlled Trial. Journal of Clinical Medicine. 2024; 13(8):2207. https://doi.org/10.3390/jcm13082207
Chicago/Turabian StyleRohe, Sebastian, Sabrina Böhle, Georg Matziolis, Frank Layher, and Steffen Brodt. 2024. "Elastic Compression Dressing after Total Hip Replacement Slightly Reduces Leg Swelling: A Randomized Controlled Trial" Journal of Clinical Medicine 13, no. 8: 2207. https://doi.org/10.3390/jcm13082207
APA StyleRohe, S., Böhle, S., Matziolis, G., Layher, F., & Brodt, S. (2024). Elastic Compression Dressing after Total Hip Replacement Slightly Reduces Leg Swelling: A Randomized Controlled Trial. Journal of Clinical Medicine, 13(8), 2207. https://doi.org/10.3390/jcm13082207