
Effects of Transcutaneous Electrical Nerve Stimulation with Taping on Wrist Spasticity, Strength, and Upper Extremity Function in Patients with Stroke: A Randomized Control Trial




Abstract
:1. Introduction
2. Experimental Section
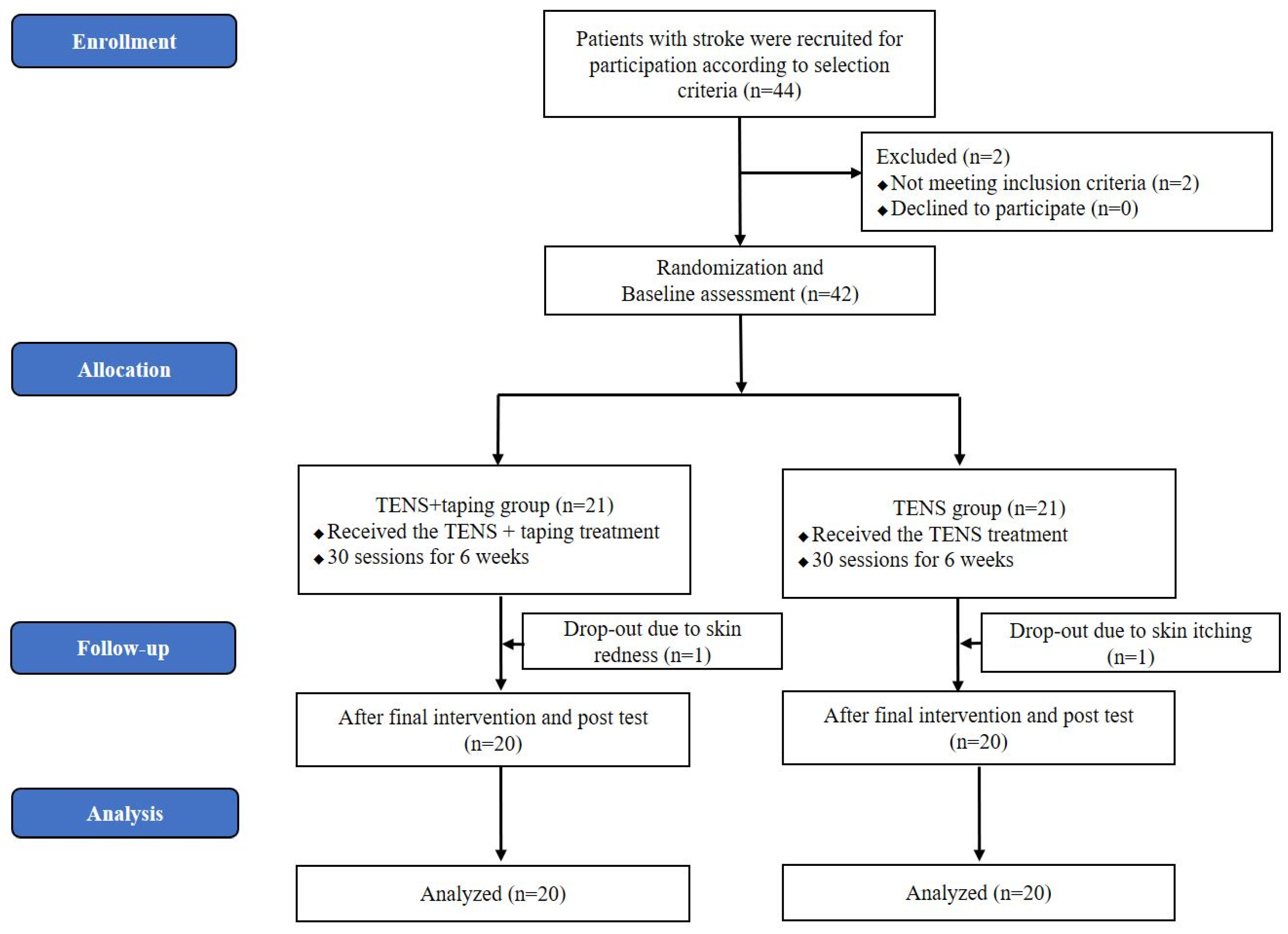
2.1. Participants
2.2. Intervention
2.3. Outcome Measure
2.4. Data Analysis
3. Results
3.1. Changes of Spasticity
3.2. Changes in Muscle Strength
3.3. Changes in Upper Extremity Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santello, M.; Baud-Bovy, G.; Jörntell, H. Neural bases of hand synergies. Front. Comput. Neurosci. 2013, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Pandyan, A.D.; Gregoric, M.; Barnes, M.P.; Wood, D.; Van Wijck, F.; Burridge, J.; Hermens, H.; Johnson, G. Spasticity: Clinical perceptions, neurological realities and meaningful measurement. Disabil. Rehabil. 2005, 27, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Bethoux, F. Spasticity Management after stroke. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 625–639. [Google Scholar] [CrossRef] [PubMed]
- Haung, Y.C.; Chen, P.C.; Tso, H.H.; Yang, Y.C.; Ho, T.L.; Leong, C.P. Effects of kinesio taping on hemiplegic hand in patients with upper limb post-stroke spasticity: A randomized controlled pilot study. Eur. J. Phys. Rehabil. Med. 2019, 55, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Langer, N.; von Bastian, C.C.; Wirz, H.; Oberauer, K.; Jäncke, L. The effects of working memory training on functional brain network efficiency. Cortex 2013, 49, 2424–2438. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Lee, M.J.; Kim, D.S.; Kim, Y.H. Functional reorganization and prediction of motor recovery after a stroke: A graph theoretical analysis of functional network. Restor. Neurol. Neurosci. 2015, 33, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Nijland, R.H.; Van Wegen, E.E.; Harmeling, B.C.; Kwakkel, G. Presence of finger extension and shoulder abduction within 72 hours after stroke predicts functional recovery: Early prediction of functional outcome after stroke: The EPOS cohort study. Stroke 2010, 41, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for adult stroke rehabilitation and recovery: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Elovic, E. Principles of pharmaceutical management of spastic hypertonia. Phys. Med. Rehabil. Clin. N. Am. 2001, 12, 793–816. [Google Scholar] [CrossRef]
- Santamato, A.; Micello, M.F.; Panza, F.; Fortunato, F.; Picelli, A.; Smania, N.; Logroscino, G.; Fiore, P.; Ranieri, M. Adhesive taping vs. daily manual muscle stretching and splinting after botulinum toxin type A injection for wrist and fingers spastic overactivity in stroke patients: A randomized controlled trial. Clin. Rehabil. 2015, 29, 50–58. [Google Scholar] [CrossRef]
- Petrofsky, J.; Laymon, M.; Lee, H. Low Level Continuous Heat Wraps can Increase the Efficiency of Transcutaneous Electrical Nerve Stimulation for Pain Management. Phys. Med. Rehab. Kurortmed. 2020, 30, 290–298. [Google Scholar] [CrossRef]
- Sheean, G.; McGuire, J.R. Spastic hypertonia and movement disorders: Pathophysiology, clinical presentation, and quantification. Phys. Med. Rehabil. 2009, 1, 827–833. [Google Scholar] [CrossRef]
- Wang, R.Y.; Chan, R.C.; Tsai, M.W. Effects of thoraco-lumbar electric sensory stimulation on knee extensor spasticity of persons who survived cerebrovascular accident (CVA). J. Rehabil. Res. Dev. 2000, 37, 73–79. [Google Scholar]
- Crone, C.; Nielsen, J.; Petersen, N.; Ballegaard, M.; Hultborn, H. Disynaptic reciprocal inhibition of ankle extensors in spastic patients. Brain 1994, 117, 1161–1168. [Google Scholar] [CrossRef]
- Tinazzi, M.; Zarattini, S.; Valeriani, M.; Romito, S.; Farina, S.; Moretto, G.; Smania, N.; Fiaschi, A.; Abbruzzese, G. Long-lasting modulation of human motor cortex following prolonged transcutaneous electrical nerve stimulation (TENS) of forearm muscles: Evidence of reciprocal inhibition and facilitation. Exp. Brain Res. 2005, 161, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Mima, T.; Oga, T.; Rothwell, J.; Satow, T.; Yamamoto, J.I.; Toma, K.; Fukuyama, H.; Shibasaki, H. Short-term high-frequency transcutaneous electrical nerve stimulation decreases human motor cortex excitability. Neurosci. Lett. 2004, 355, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, A.; Veluswamy, S.K.; Hombali, A.; Mullick, A.; Manikandan, N.; Solomon, J.M. Effect of Transcutaneous Electrical Nerve Stimulation on Spasticity in Adults With Stroke: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 751–768. [Google Scholar] [CrossRef] [PubMed]
- Fridén, J.; Lieber, R.L. Spastic muscle cells are shorter and stiffer than normal cells. Muscle Nerve 2003, 27, 157–164. [Google Scholar] [CrossRef]
- Abrams, R.A.; Tsai, A.M.; Watson, B.; Jamali, A.; Lieber, R.L. Skeletal muscle recovery after tenotomy and 7-day delayed muscle length restoration. Muscle Nerve 2000, 23, 707–714. [Google Scholar] [CrossRef]
- Toursel, T.; Stevens, L.; Granzier, H.; Mounier, Y. Passive tension of rat skeletal soleus muscle fibers: Effects of unloading conditions. J. Appl. Physiol. 2002, 92, 1465–1472. [Google Scholar] [CrossRef]
- Tan, B.; Jia, G.; Song, Y.; Jiang, W. Effect of kinesiotaping on pain relief and upper limb function in stroke survivors: A systematic review and meta-analysis. Am. J. Transl. Res. 2022, 14, 3372–3380. [Google Scholar] [PubMed]
- Baricich, A.; Carda, S.; Bertoni, M.; Maderna, L.; Cisari, C. A single-blinded, randomized pilot study of botulinum toxin type A combined with non-pharmacological treatment for spastic foot. J. Rehabil. Med. 2008, 40, 870–872. [Google Scholar] [CrossRef] [PubMed]
- Karadag-Saygi, E.; Cubukcu-Aydoseli, K.; Kablan, N.; Ofluoglu, D. The role of kinesiotaping combined with botulinum toxin to reduce plantar flexors spasticity after stroke. Top. Stroke Rehabil. 2010, 17, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Carda, S.; Invernizzi, M.; Baricich, A.; Cisari, C. Casting, taping or stretching after botulinum toxin type A for spastic equinus foot: A single-blind randomized trial on adult stroke patients. Clin. Rehabil. 2011, 25, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- In, T.S.; Jung, J.H.; Jung, K.S.; Cho, H.Y. Effectiveness of Transcutaneous Electrical Nerve Stimulation with Taping for Stroke Rehabilitation. Biomed. Res. Int. 2021, 25, 9912094. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, X.; Sun, C.; Xu, R. Effectiveness of kinesiology taping on the functions of upper limbs in patients with stroke: A meta-analysis of randomized trial. Neurol. Sci. 2022, 43, 4145–4156. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, A.; Livanelioglu, A.; Gunel, M.K. Reliability of Ashworth and Modified Ashworth scales in children with spastic cerebral palsy. BMC Musculoskelet. Disord. 2008, 9, 44. [Google Scholar] [CrossRef]
- Duncan, P.W.; Propst, M.; Nelson, S.G. Reliability of the Fugl-Meyer assessment of sensorimotor recovery following cerebrovascular accident. Phys. Ther. 1983, 63, 1606–1610. [Google Scholar] [CrossRef] [PubMed]
- Martins, F.L.; Carvalho, L.C.; Silva, C.C.; Brasileiro, J.S.; Souza, T.O.; Lindquist, A.R. Immediate effects of TENS and cryotherapy in the reflex excitability and voluntary activity in hemiparetic subjects: A randomized crossover trial. Rev. Bras. Fisioter. 2012, 16, 337–344. [Google Scholar] [CrossRef]
- Roman, N.; Miclaus, R.S.; Necula, R.; Dumistracel, A.; Cheregi, C.; Grigorescu, O.-D. Physiotherapy Efficiency in Post-stroke Upper Extremity Spasticity: TENS vs. Ultrasound vs. Paraffin. In Vivo 2023, 37, 916–923. [Google Scholar] [CrossRef]
- Ekiz, T.; Aslan, M.D.; Özgirgin, N.J. Effects of Kinesio Tape application to quadriceps muscles on isokinetic muscle strength, gait, and functional parameters in patients with stroke. J. Rehabil. Res. Dev. 2015, 52, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Seo, H.M.; Lee, H.D. Effect of taping method on ADL, range of motion, hand function and quality of life in post-stroke Patients for 5 weeks. Korean J. Rehabil. Nurs. 2002, 5, 7–17. [Google Scholar]
- Page, S.J.; Fulk, G.D.; Boyne, P. Clinically important differences for the upper-extremity Fugl-Meyer Scale in people with minimal to moderate impairment due to chronic stroke. Phys. Ther. 2012, 92, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Arya, K.N.; Verma, R.; Garg, R.K. Estimating the minimal clinically important difference of an upper extremity recovery measure in subacute stroke patients. Top. Stroke Rehabil. 2011, 18, 599–610. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | TENS + Taping Group (n = 20) | TENS Group (n = 20) | p |
|---|---|---|---|
| Sex (male/female) Type (infarction/hemorrhage) | 13/7 | 14/6 | 0.736 b |
| 12/8 | 11/9 | 0.749 | |
| Involved side (left/right) | 9/11 | 10/10 | 0.752 |
| Age (years) | 52.4 ± 9.3 a (39–70) | 53.5 ± 10.8 (39–74) | 0.755 c |
| Height (cm) | 165.4 ± 9.6 | 166.0 ± 10.4 | 0.851 |
| Weight (kg) | 62.6 ± 8.1 | 63.8 ± 8.3 | 0.634 |
| Stroke duration (months) | 8.1 ± 2.1 | 8.2 ± 2.4 | 0.889 |
| MAS | 2.1 ± 0.4 | 2.1 ± 0.5 | 0.575 |
| TENS + Taping Group | Difference | TENS Group | Difference | p-Value | |||
|---|---|---|---|---|---|---|---|
| Pretest | Posttest | Pretest | Posttest | ||||
| MAS (score) | 2.1 ± 0.4 | 1.5 ± 0.5 * | -0.6 ± 0.4 | 2.1 ± 0.5 | 1.8 ± 0.6 * | −0.2 ± 0.4 | 0.004 |
| TENS + Taping Group | Difference | TENS Group | Difference | p-Value | |||
|---|---|---|---|---|---|---|---|
| Pretest | Posttest | Pretest | Posttest | ||||
| Muscle strength (kg) | 4.4 ± 3.0 | 5.9 ± 4.7 * | 1.5 ± 3.0 | 5.5 ± 4.2 | 6.7 ± 4.4 | 1.2 ± 2.9 | 0.737 |
| TENS + Taping Group | Difference | TENS Group | Difference | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Pretest | Posttest | Pretest | Posttest | |||||
| FMA-UE (score) | Shoulder/Elbow/Forearm | 26.5 ± 4.1 | 31.3 ± 3.0 | 4.8 ± 2.1 | 27.3 ± 3.5 | 29.3 ± 5.5 | 2.0 ± 2.0 | |
| Wrist | 3.4 ± 2.8 | 5.3 ± 3.0 | 1.9 ± 3.5 | 4.1 ± 2.5 | 4.2 ± 3.3 | 0.1 ± 1.4 | ||
| Hand | 4.2 ± 2.4 | 5.0 ± 2.1 | 0.8 ± 2.5 | 4.4 ± 3.1 | 4.9 ± 2.4 | 0.5 ± 2.1 | ||
| Coordination | 3.1 ± 1.2 | 3.6 ± 1.1 | 0.5 ± 0.5 | 3.3 ± 1.2 | 3.4 ± 2.1 | 0.1 ± 1.5 | ||
| Total | 37.2 ± 5.5 | 45.2 ± 4.1 * | 8.0 ± 5.2 | 39.1 ± 6.8 | 41.8 ± 6.9 * | 2.7 ± 1.2 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, K.-s.; Jung, J.-h.; Cho, H.-y.; In, T.-s. Effects of Transcutaneous Electrical Nerve Stimulation with Taping on Wrist Spasticity, Strength, and Upper Extremity Function in Patients with Stroke: A Randomized Control Trial. J. Clin. Med. 2024, 13, 2229. https://doi.org/10.3390/jcm13082229
Jung K-s, Jung J-h, Cho H-y, In T-s. Effects of Transcutaneous Electrical Nerve Stimulation with Taping on Wrist Spasticity, Strength, and Upper Extremity Function in Patients with Stroke: A Randomized Control Trial. Journal of Clinical Medicine. 2024; 13(8):2229. https://doi.org/10.3390/jcm13082229
Chicago/Turabian StyleJung, Kyoung-sim, Jin-hwa Jung, Hwi-young Cho, and Tae-sung In. 2024. "Effects of Transcutaneous Electrical Nerve Stimulation with Taping on Wrist Spasticity, Strength, and Upper Extremity Function in Patients with Stroke: A Randomized Control Trial" Journal of Clinical Medicine 13, no. 8: 2229. https://doi.org/10.3390/jcm13082229
APA StyleJung, K.-s., Jung, J.-h., Cho, H.-y., & In, T.-s. (2024). Effects of Transcutaneous Electrical Nerve Stimulation with Taping on Wrist Spasticity, Strength, and Upper Extremity Function in Patients with Stroke: A Randomized Control Trial. Journal of Clinical Medicine, 13(8), 2229. https://doi.org/10.3390/jcm13082229