Perioperative Serum Calcium and Phosphorus Levels are Associated with Hospital Costs and Length of Stay after Major Abdominal Surgery

Abstract
:1. Introduction
2. Materials and Methods
2.1. Total Medical Costs for Major Abdominal Surgery
2.2. Measurements and Outcome
2.3. Ethics
2.4. Statistical Analysis
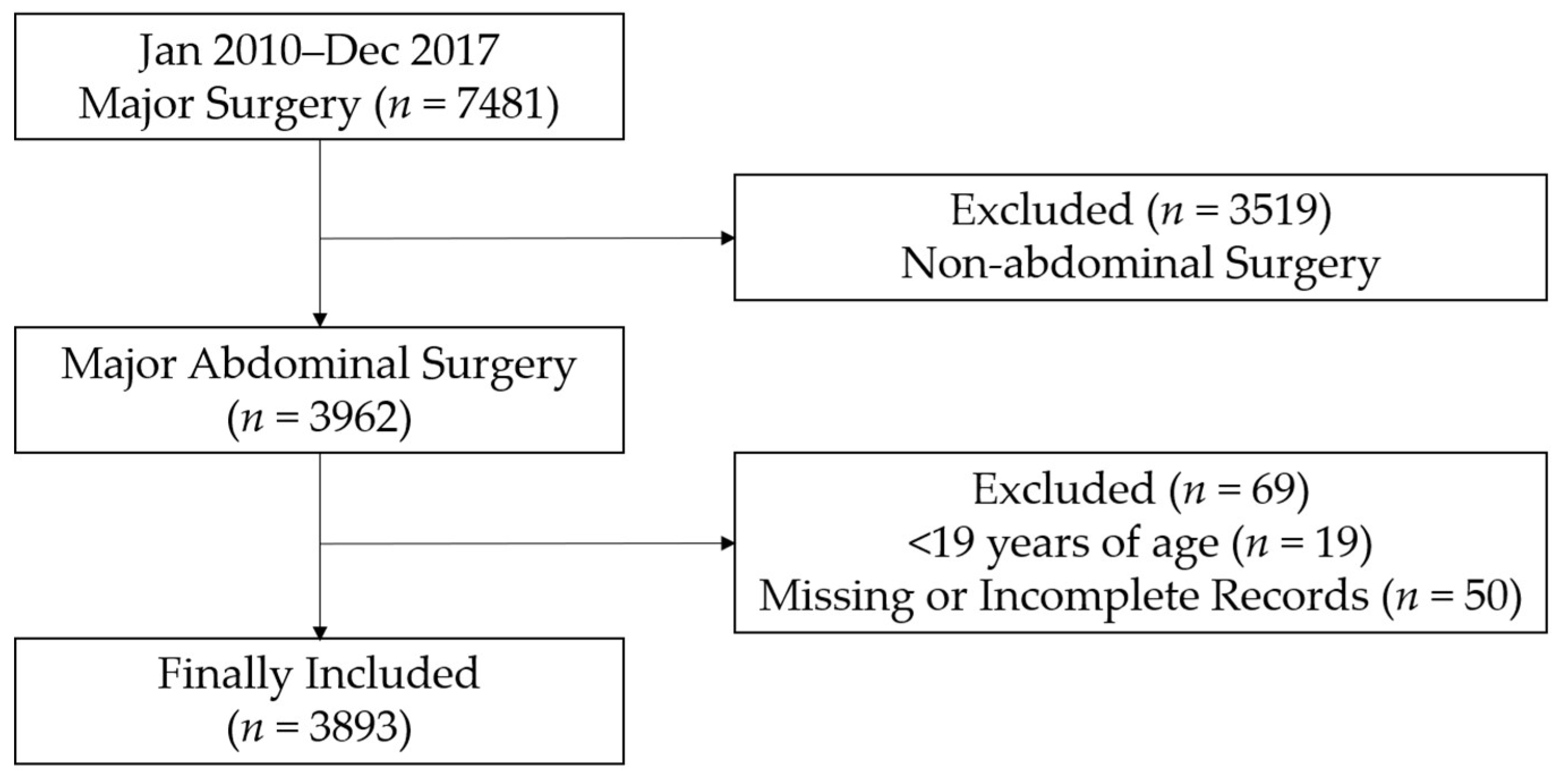
3. Results
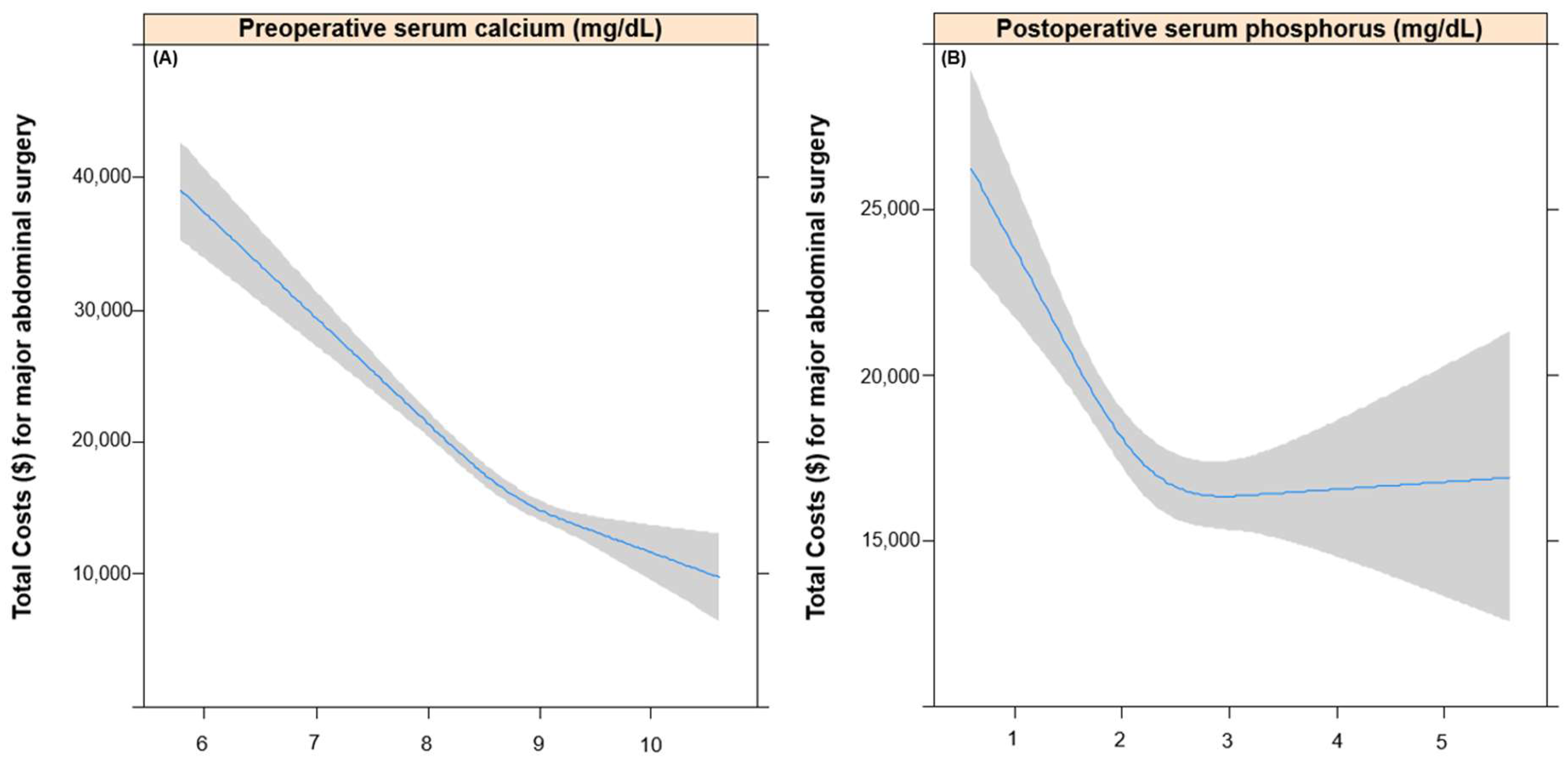
3.1. Total Costs according to Pre- and Postoperative Calcium and Phosphorus Levels
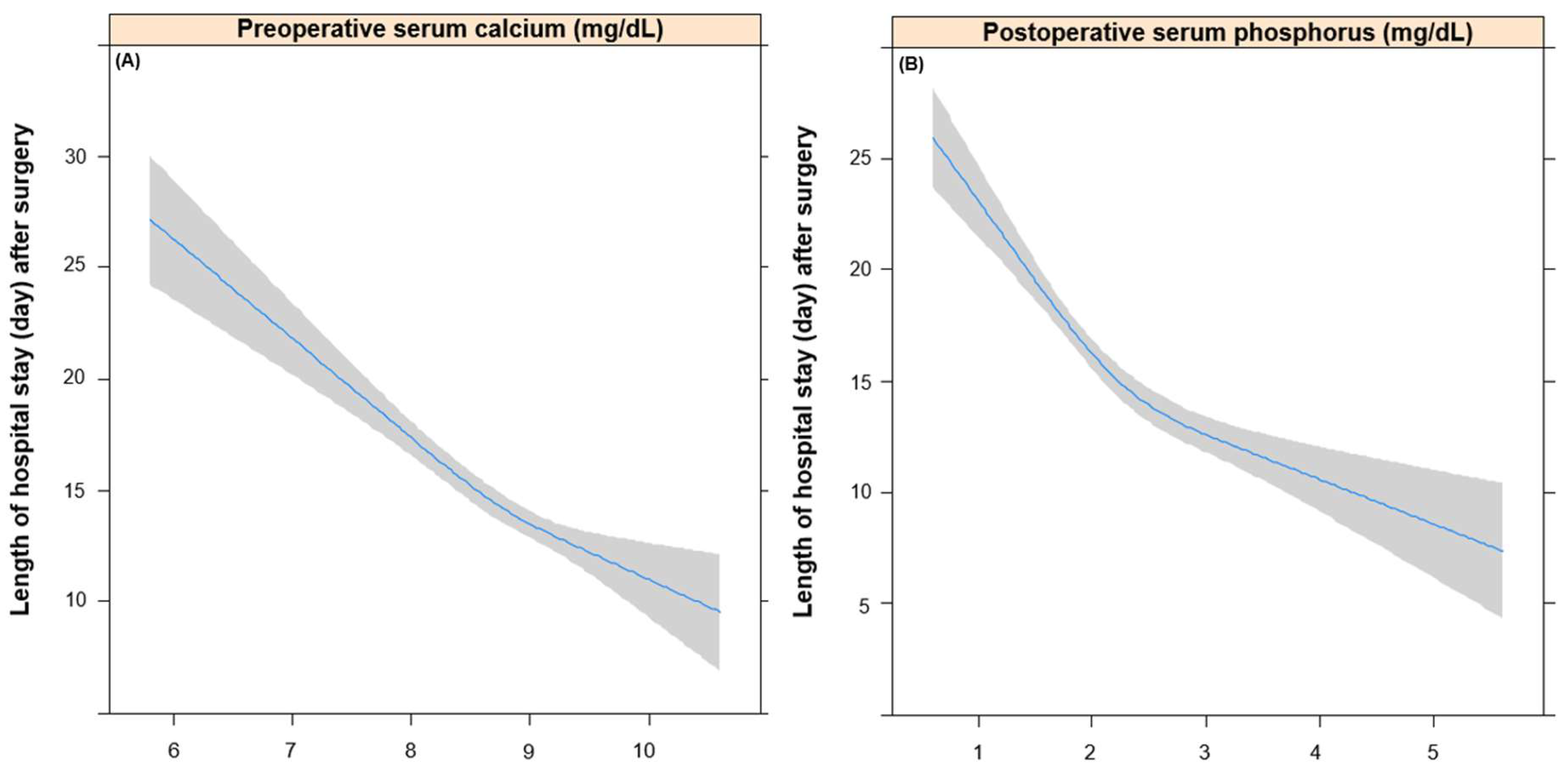
3.2. Length of Hospital Stay after Major Abdominal Surgery according to Pre- and Postoperative Calcium and Phosphorus Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rojer, A.G.; Kruizenga, H.M.; Trappenburg, M.C.; Reijnierse, E.M.; Sipila, S.; Narici, M.V.; Hogrel, J.Y.; Butler-Browne, G.; McPhee, J.S.; Paasuke, M.; et al. The prevalence of malnutrition according to the new espen definition in four diverse populations. Clin. Nutr. 2016, 35, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.D.; Hey, L.A.; Yu, C.S.; Klein, B.B.; Coufal, F.J.; Young, E.P.; Marshall, L.F.; Garfin, S.R. Perioperative nutrition and postoperative complications in patients undergoing spinal surgery. Spine 1996, 21, 2676–2682. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, V.; Gianotti, L.; Balzano, G.; Zerbi, A.; Braga, M. Complications of pancreatic surgery and the role of perioperative nutrition. Dig. Surg. 1999, 16, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.H.; Cajas-Monson, L.C.; Eisenstein, S.; Parry, L.; Cosman, B.; Ramamoorthy, S. Preoperative malnutrition assessments as predictors of postoperative mortality and morbidity in colorectal cancer: An analysis of ACS-NSQIP. Nutr. J. 2015, 14, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Pikul, J.; Sharpe, M.D.; Lowndes, R.; Ghent, C.N. Degree of preoperative malnutrition is predictive of postoperative morbidity and mortality in liver transplant recipients. Transplantation 1994, 57, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Engelman, D.T.; Adams, D.H.; Byrne, J.G.; Aranki, S.F.; Collins, J.J., Jr.; Couper, G.S.; Allred, E.N.; Cohn, L.H.; Rizzo, R.J. Impact of body mass index and albumin on morbidity and mortality after cardiac surgery. J. Thorac. Cardiovasc. Surg. 1999, 118, 866–873. [Google Scholar] [CrossRef]
- Gibbs, J.; Cull, W.; Henderson, W.; Daley, J.; Hur, K.; Khuri, S.F. Preoperative serum albumin level as a predictor of operative mortality and morbidity: Results from the National VA Surgical Risk Study. Arch. Surg. 1999, 134, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.G.; Bushinsky, D.A. Calcium and phosphorus homeostasis. Blood Purif. 2009, 27, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Moe, S.M. Disorders involving calcium, phosphorus, and magnesium. Prim. Care 2008, 35, 215–237. [Google Scholar] [CrossRef] [PubMed]
- Dzik, W.H.; Kirkley, S.A. Citrate toxicity during massive blood transfusion. Transfus. Med. Rev. 1988, 2, 76–94. [Google Scholar] [CrossRef]
- Kwon, S. Thirty years of national health insurance in south korea: Lessons for achieving universal health care coverage. Health Policy Plan. 2009, 24, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Henderson, W.G.; Daley, J. Design and statistical methodology of the national surgical quality improvement program: Why is it what it is? Am. J. Surg. 2009, 198, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Lassen, K.; Coolsen, M.M.; Slim, K.; Carli, F.; de Aguilar-Nascimento, J.E.; Schafer, M.; Parks, R.W.; Fearon, K.C.; Lobo, D.N.; Demartines, N.; et al. Guidelines for perioperative care for pancreaticoduodenectomy: Enhanced recovery after surgery (ERAS®) society recommendations. Clin. Nutr. 2012, 31, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Sandrucci, S.; Beets, G.; Braga, M.; Dejong, K.; Demartines, N. Perioperative nutrition and enhanced recovery after surgery in gastrointestinal cancer patients. A position paper by the ESSO task force in collaboration with the ERAS society (ERAS coalition). Eur. J. Surg. Oncol. 2018, 44, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Cid Conde, L.; Fernandez Lopez, T.; Neira Blanco, P.; Arias Delgado, J.; Varela Correa, J.J.; Gomez Lorenzo, F.F. Hyponutrition prevalence among patients with digestive neoplasm before surgery. Nutr. Hosp. 2008, 23, 46–53. [Google Scholar] [PubMed]
- Oh, T.K.; Lee, J.; Hwang, J.W.; Do, S.H.; Jeon, Y.T.; Kim, J.H.; Kim, K.; Song, I.A. Value of preoperative modified body mass index in predicting postoperative 1-year mortality. Sci. Rep. 2018, 8, 4614–4622. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.H.; Kim, M.K.; Park, S.E.; Rhee, E.J.; Park, C.Y.; Lee, W.Y.; Baek, K.H.; Song, K.H.; Kang, M.I.; Oh, K.W. The association between daily calcium intake and sarcopenia in older, non-obese korean adults: The fourth korea national health and nutrition examination survey (KNHANES IV) 2009. Endocr. J. 2013, 60, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Lesourd, B.M. Nutrition and immunity in the elderly: Modification of immune responses with nutritional treatments. Am. J. Clin. Nutr. 1997, 66, 478–484. [Google Scholar] [CrossRef] [PubMed]
- England, P.C.; Duari, M.; Tweedle, D.E.; Jones, R.A.; Gowland, E. Postoperative hypophosphataemia. Br. J. Surg. 1979, 66, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, L.; Wong, D.; Karalapillai, D.; Pearce, B.; Tan, C.O.; Tay, S.; Christophi, C.; McNicol, L.; Nikfarjam, M. The impact of fluid intervention on complications and length of hospital stay after pancreaticoduodenectomy (Whipple's procedure). BMC Anesthesiol. 2014, 14, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, K.; Barone, J.E.; Rogers, J.F. Severe hypophosphatemia in postoperative patients. Nutr. Clin. Pract. 1992, 7, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Pesta, D.H.; Tsirigotis, D.N.; Befroy, D.E.; Caballero, D.; Jurczak, M.J.; Rahimi, Y.; Cline, G.W.; Dufour, S.; Birkenfeld, A.L.; Rothman, D.L.; et al. Hypophosphatemia promotes lower rates of muscle atp synthesis. FASEB J. 2016, 30, 3378–3387. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (3893) | Mean (SD) |
|---|---|---|
| Age, year | 58.5 (14.6) | |
| Body mass index, kg m-2 | 23.9 (3.6) | |
| Sex: male | 2079 (53.4%) | |
| Preoperative comorbidities | ||
| Hypertension | 1096 (28.2%) | |
| Diabetes mellitus | 211 (5.4%) | |
| Ischemic heart disease | 75 (1.9%) | |
| Cerebrovascular disease | 84 (2.2%) | |
| Chronic kidney disease | 208 (5.3%) | |
| Liver disease (Hepatitis, LC, HCC) | 362 (9.3%) | |
| Cancer | 300 (7.7%) | |
| Information regarding surgical procedures | ||
| Surgery time, hour | 5.3 (2.4) | |
| Estimated blood loss, mL | 1310.5 (2154.2) | |
| Total RVUs a | 29,485.9 (33,927.1) | |
| Intraoperative remifentanil dosage, mg | 1.0 (1.8) | |
| Length of hospital stay, day | 14.6 (16.9) | |
| Type of surgery | ||
| Gastrointestinal tract surgery | 895 (23.0%) | |
| Hepato-biliary-pancreatic surgery | 971 (24.9%) | |
| Genitourinary surgery | 689 (17.7%) | |
| Obstetric and gynecologic surgery | 935 (24.0%) | |
| Major vascular surgery | 87 (2.2%) | |
| Exploratory laparotomy or bleeding control | 316 (8.1%) | |
| Laparoscopic surgery | 602 (15.5%) | |
| Total hospital costs, dollar | 16,807.3 (21,665.3) | |
| Preoperative serum Ca, mg/dL | 8.7 (0.7) | |
| Preoperative serum P, mg/dL | 3.5 (0.8) | |
| Postoperative serum Ca, mg/dL | 6.2 (2.6) | |
| Postoperative serum P, mg/dL | 2.3 (0.8) |
| Characteristics | Total Costs ($) | Length of Hospital Stay (day) | ||
|---|---|---|---|---|
| Coefficient (95% CI) | p-Value | Coefficient (95% CI) | p-Value | |
| Sex: male (vs. female) | 5393.8 (4035.3, 6752.3) | <0.01 | 3.2 (2.2, 4.3) | <0.01 |
| Age, year | 125.7 (78.9, 172.5) | <0.01 | 0.2 (0.1, 0.2) | <0.01 |
| Body mass index, kg/m2 | −248.7 (−442.2, −55.2) | 0.01 | −0.4 (−0.5, −0.2) | <0.01 |
| Hypertension | 1496.8 (−19.2, 3012.7) | 0.05 | 3.4 (0.2, 4.6) | <0.01 |
| Diabetes mellitus | 4440.6 (1429.5, 7451.8) | <0.01 | 2.4 (0.2, 4.8) | 0.05 |
| Cerebrovascular disease | 6245.1 (1295.4, 11,194.8) | 0.01 | 10.5 (6.6, 14.3) | <0.01 |
| Ischemic heart disease | 8967.5 (4289.8, 13,645.3) | <0.01 | 4.3 (0.6, 8.0) | 0.02 |
| Chronic kidney disease | 21,735.9 (18,765.0, 24,706.8) | <0.01 | 6.8 (4.4, 9.2) | <0.01 |
| Liver disease | 19,687.8 (17,423.3, 21,952.4) | <0.01 | 2.0 (0.1, 3.8) | 0.04 |
| Cancer | 1936.2 (−620.5, 4493.0) | 0.14 | 2.4 (0.4, 4.5) | 0.02 |
| Surgery time, hour | 2295.7 (2026.6, 2564.7) | <0.01 | 1.9 (1.6, 2.1) | <0.01 |
| Estimated blood loss, 100 mL | 330 (304, 362) | <0.01 | 1.0 (1.0, 1.1) | <0.01 |
| General surgery (vs. non-GS) | 13,683.2 (12,368.0, 14,998.4) | <0.01 | 7.6 (6.5, 8.6) | <0.01 |
| Laparoscopy | −5005.3 (−6884.0, −3126.6) | <0.01 | −4.1 (−5.5, −2.6) | <0.01 |
| Total RVUs a, 10000 points | 2544.5 (2380.3, 2708.7) | <0.01 | 0.53 (0.38, 0.68) | <0.01 |
| Intraop rmFTN dosage, 1 mg | −139.3 (−479.0, 200.4) | 0.42 | 0.96 (0.68, 1.23) | <0.01 |
| Total Costs ($) | Length of Hospital Stay (day) | |||
|---|---|---|---|---|
| Variables | Coefficient (95% CI) | p-Value | Coefficient (95% CI) | p-Value |
| Unadjusted | ||||
| Preoperative Ca | −6190.0 (−7132.9, −5247.1) | <0.01 | −3.7 (−4.5, −3.0) | <0.01 |
| Preoperative P | −672.9 (−1594.6, 248.8) | 0.15 | −0.6 (−1.2, 0.1) | 0.11 |
| Postoperative Ca | 658.6 (385.2. 932.0) | <0.01 | 0.2 (0.0, 0.4) | 0.07 |
| Postoperative P | −2076.3 (−3008.1, −1144.5) | <0.01 | −3.7 (−4.4, −3.0) | <0.01 |
| Adjusted | ||||
| Preoperative Ca | −3997.9 (−4900.5, −3095.3) | <0.01 | −2.9 (−3.7, −2.1) | <0.01 |
| Preoperative P | −512.4 (−1451.6, 426.7) | 0.29 | 0.6 (−0.3, 1.4) | 0.18 |
| Postoperative Ca | 3.8 (−247.9, 255.4) | 0.98 | −0.2 (−0.4, 0.0) | 0.098 |
| Postoperative P | −702.5 (−1274.5, −67.3) | 0.03 | −3.4 (−4.2, −2.6) | <0.01 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, T.K.; Jo, J.; Oh, A.-Y. Perioperative Serum Calcium and Phosphorus Levels are Associated with Hospital Costs and Length of Stay after Major Abdominal Surgery. J. Clin. Med. 2018, 7, 299. https://doi.org/10.3390/jcm7100299
Oh TK, Jo J, Oh A-Y. Perioperative Serum Calcium and Phosphorus Levels are Associated with Hospital Costs and Length of Stay after Major Abdominal Surgery. Journal of Clinical Medicine. 2018; 7(10):299. https://doi.org/10.3390/jcm7100299
Chicago/Turabian StyleOh, Tak Kyu, Jihoon Jo, and Ah-Young Oh. 2018. "Perioperative Serum Calcium and Phosphorus Levels are Associated with Hospital Costs and Length of Stay after Major Abdominal Surgery" Journal of Clinical Medicine 7, no. 10: 299. https://doi.org/10.3390/jcm7100299
APA StyleOh, T. K., Jo, J., & Oh, A. -Y. (2018). Perioperative Serum Calcium and Phosphorus Levels are Associated with Hospital Costs and Length of Stay after Major Abdominal Surgery. Journal of Clinical Medicine, 7(10), 299. https://doi.org/10.3390/jcm7100299