Patterns of Occurrence and Outcomes of Contralateral Breast Cancer: Analysis of SEER Data

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients and Methods
2.2. Statistical Analysis
3. Results
3.1. Occurrence Pattern of CBC Incidence
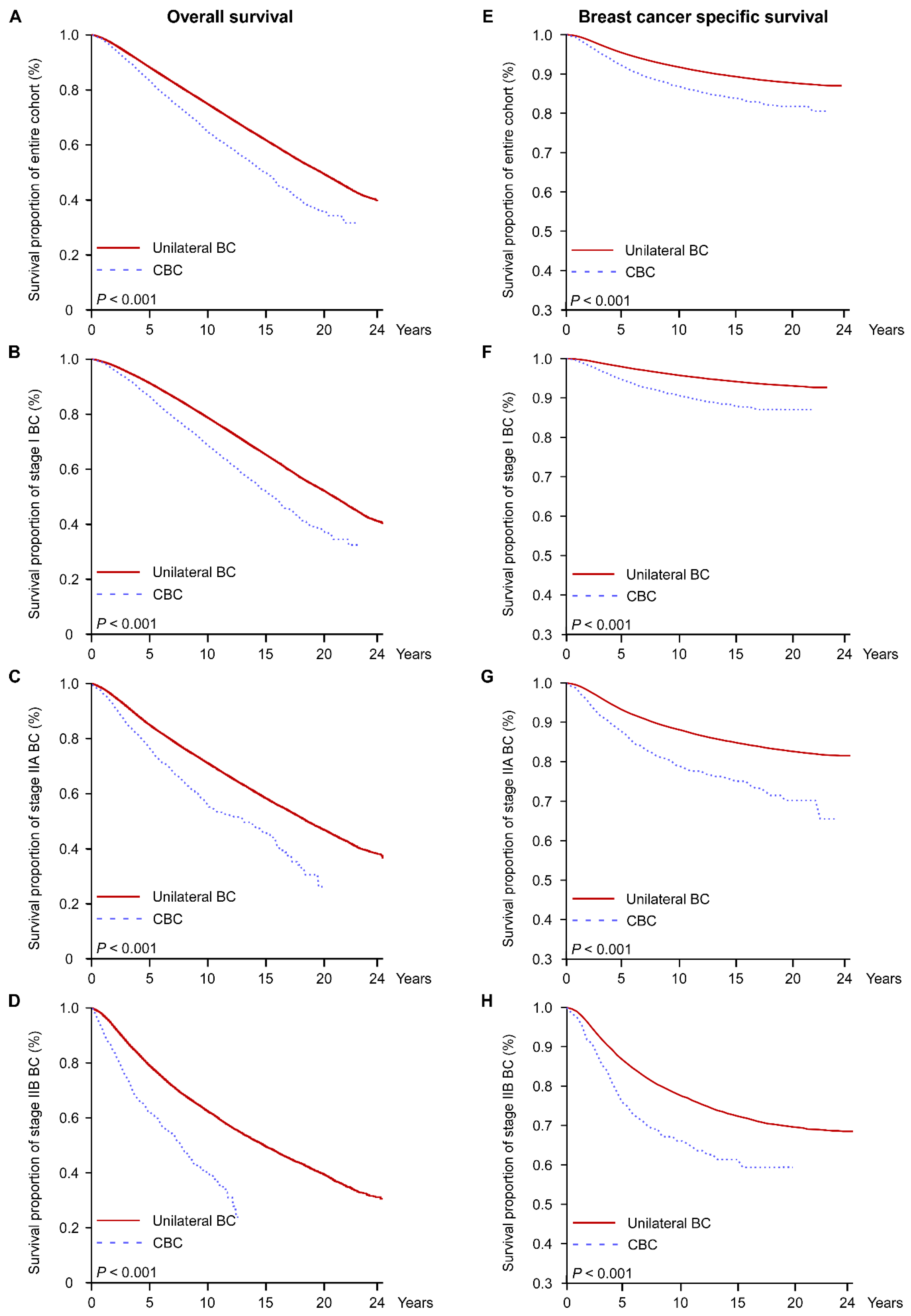
3.2. Overall and Cancer-Specific Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Lehman, C.D.; Gatsonis, C.; Kuhl, C.K.; Hendrick, R.E.; Pisano, E.D.; Hanna, L.; Peacock, S.; Smazal, S.F.; Maki, D.D.; Julian, T.B.; et al. MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N. Engl. J. Med. 2007, 356, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Heron, D.E.; Komarnicky, L.T.; Hyslop, T.; Schwartz, G.F.; Mansfield, C.M. Bilateral breast carcinoma: Risk factors and outcomes for patients with synchronous and metachronous disease. Cancer 2000, 88, 2739–2750. [Google Scholar] [CrossRef]
- Nichols, H.B.; Berrington de Gonzalez, A.; Lacey, J.V., Jr.; Rosenberg, P.S.; Anderson, W.F. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J. Clin. Oncol. 2011, 29, 1564–1569. [Google Scholar] [CrossRef] [PubMed]
- Hartman, M.; Czene, K.; Reilly, M.; Adolfsson, J.; Bergh, J.; Adami, H.O.; Dickman, P.W.; Hall, P. Incidence and prognosis of synchronous and metachronous bilateral breast cancer. J. Clin. Oncol. 2007, 25, 4210–4216. [Google Scholar] [CrossRef] [PubMed]
- Rusner, C.; Wolf, K.; Bandemer-Greulich, U.; Engel, J.; Stegmaier, C.; Holleczek, B.; Schubert-Fritschle, G.; Tillack, A.; Stang, A. Risk of contralateral second primary breast cancer according to hormone receptor status in Germany. Breast Cancer Res. 2014, 16, 452. [Google Scholar] [CrossRef] [PubMed]
- Knight, J.A.; Fan, J.; Malone, K.E.; John, E.M.; Lynch, C.F.; Langballe, R.; Bernstein, L.; Shore, R.E.; Brooks, J.D.; Reiner, A.S.; et al. Alcohol consumption and cigarette smoking in combination: A predictor of contralateral breast cancer risk in the WECARE study. Int. J. Cancer 2017, 141, 916–924. [Google Scholar] [CrossRef] [PubMed]
- Reiner, A.S.; Lynch, C.F.; Sisti, J.S.; John, E.M.; Brooks, J.D.; Bernstein, L.; Knight, J.A.; Hsu, L.; Concannon, P.; Mellemkjaer, L.; et al. Hormone receptor status of a first primary breast cancer predicts contralateral breast cancer risk in the WECARE study population. Breast Cancer Res. 2017, 19, 83. [Google Scholar] [CrossRef] [PubMed]
- Bertelsen, L.; Bernstein, L.; Olsen, J.H.; Mellemkjaer, L.; Haile, R.W.; Lynch, C.F.; Malone, K.E.; Anton-Culver, H.; Christensen, J.; Langholz, B.; et al. Effect of systemic adjuvant treatment on risk for contralateral breast cancer in the Women's Environment, Cancer and Radiation Epidemiology Study. J. Nat. Cancer Inst. 2008, 100, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Langballe, R.; Mellemkjaer, L.; Malone, K.E.; Lynch, C.F.; John, E.M.; Knight, J.A.; Bernstein, L.; Brooks, J.; Andersson, M.; Reiner, A.S.; et al. Systemic therapy for breast cancer and risk of subsequent contralateral breast cancer in the WECARE Study. Breast Cancer Res. 2016, 18, 65. [Google Scholar] [CrossRef] [PubMed]
- Gierach, G.L.; Curtis, R.E.; Pfeiffer, R.M. Association of adjuvant tamoxifen and aromatase inhibitor therapy with contralateral breast cancer risk among us women with breast cancer in a general community setting. JAMA Oncol. 2017, 3, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Gronwald, J.; Robidoux, A.; Kim-Sing, C.; Tung, N.; Lynch, H.T.; Foulkes, W.D.; Manoukian, S.; Ainsworth, P.; Neuhausen, S.L.; Demsky, R.; et al. Duration of tamoxifen use and the risk of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat 2014, 146, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Narod, S.A.; Brunet, J.S.; Ghadirian, P.; Robson, M.; Heimdal, K.; Neuhausen, S.L.; Stoppa-Lyonnet, D.; Lerman, C.; Pasini, B.; de los Rios, P.; et al. Tamoxifen and risk of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers: A case-control study. Hereditary Breast Cancer Clinical Study Group. Lancet 2000, 356, 1876–1881. [Google Scholar] [CrossRef]
- Rosenberg, S.M.; Ruddy, K.J.; Tamimi, R.M.; Gelber, S.; Schapira, L.; Come, S.; Borges, V.F.; Larsen, B.; Garber, J.E.; Partridge, A.H. BRCA1 and BRCA2 Mutation Testing in Young Women With Breast Cancer. JAMA Oncol. 2016, 2, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Liederbach, E.; Wang, C.H.; Lutfi, W.; Kantor, O.; Pesce, C.; Winchester, D.J.; Yao, K. Survival Outcomes and Pathologic Features Among Breast Cancer Patients Who Have Developed a Contralateral Breast Cancer. Ann. Surg. Oncol. 2015, 22 (Suppl. 3), S412–S421. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology-Breast Cancer (Version 1.2018). Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf#page=2&zoom=auto,-247,476 (accessed on 20 March 2018).
- Surveillance, E.; Results, E. (SEER) Program Research Data (1973-2013), National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, Released April 2016, Based on the November 2015 Submission. Available online: http://www.seer.cancer.gov (accessed on 15 August 2016).
- Li, G.; Zhang, P.; Wang, J.; An, Y.; Gong, Q.; Gregg, E.W.; Yang, W.; Zhang, B.; Shuai, Y.; Hong, J.; et al. Cardiovascular mortality, all-cause mortality, and diabetes incidence after lifestyle intervention for people with impaired glucose tolerance in the Da Qing Diabetes Prevention Study: A 23-year follow-up study. Lancet Diabetes Endocrinol. 2014, 2, 474–480. [Google Scholar] [CrossRef]
- SEER*Stat Software. Available online: https://seer.cancer.gov/seerstat/ (accessed on 29 May 2018).
- Joinpoint Regression Program, Version 4.5.0.1. Statistical Research and Applications Branch, National Cancer Institute. Available online: https://surveillance.cancer.gov/joinpoint/download (accessed on 12 June 2017).
- Chen, Y.; Thompson, W.; Semenciw, R.; Mao, Y. Epidemiology of contralateral breast cancer. Cancer Epidemiol. Biomark. Prev. 1999, 8, 855–861. [Google Scholar]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.L.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. Cancer J. Clin. 2016, 66, 43–73. [Google Scholar] [CrossRef] [PubMed]
- Van der Hage, J.A.; Mieog, J.S.; van de Velde, C.J.; Putter, H.; Bartelink, H.; van de Vijver, M.J. Impact of established prognostic factors and molecular subtype in very young breast cancer patients: Pooled analysis of four EORTC randomized controlled trials. Breast Cancer Res. 2011, 13, R68. [Google Scholar] [CrossRef] [PubMed]
- Arrington, A.K.; Voci, A.; Reparaz, L.; Fry, W. Factors and outcomes associated with surgical treatment options of contralateral breast cancer. Am J. Surg. 2014, 208, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.M.; Sepucha, K.; Ruddy, K.J.; Tamimi, R.M.; Gelber, S.; Meyer, M.E.; Schapira, L.; Come, S.E.; Borges, V.F.; Golshan, M.; et al. Local Therapy Decision-Making and Contralateral Prophylactic Mastectomy in Young Women with Early-Stage Breast Cancer. Ann. Surg. Oncol. 2015, 22, 3809–3815. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.; Gershman, S.; Lynch, H.T.; Ghadirian, P.; Tung, N.; Kim-Sing, C.; Olopade, O.I.; Domchek, S.; McLennan, J.; Eisen, A.; et al. Predictors of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. Br. J. Cancer 2011, 104, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. Jama 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Kurian, A.W.; McClure, L.A.; John, E.M.; Horn-Ross, P.L.; Ford, J.M.; Clarke, C.A. Second primary breast cancer occurrence according to hormone receptor status. J. Nat. Cancer Inst. 2009, 101, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Coombes, R.C.; Hall, E.; Gibson, L.J.; Paridaens, R.; Jassem, J.; Delozier, T.; Jones, S.E.; Alvarez, I.; Bertelli, G.; Ortmann, O.; et al. A randomized trial of exemestane after two to three years of tamoxifen therapy in postmenopausal women with primary breast cancer. N. Engl. J. Med. 2004, 350, 1081–1092. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.F.; Sestak, I.; Howell, A.; Bonanni, B.; Bundred, N.; Levy, C.; von Minckwitz, G.; Eiermann, W.; Neven, P.; Stierer, M.; et al. Anastrozole versus tamoxifen for the prevention of locoregional and contralateral breast cancer in postmenopausal women with locally excised ductal carcinoma in situ (IBIS-II DCIS): A double-blind, randomised controlled trial. Lancet 2016, 387, 866–873. [Google Scholar] [CrossRef]
- Li, C.I.; Daling, J.R.; Porter, P.L.; Tang, M.T.; Malone, K.E. Adjuvant hormonal therapy for breast cancer and risk of hormone receptor-specific subtypes of contralateral breast cancer. Cancer Res. 2009, 69, 6865–6870. [Google Scholar] [CrossRef] [PubMed]
- Goss, P.E.; Ingle, J.N.; Pritchard, K.I.; Robert, N.J.; Muss, H.; Gralow, J.; Gelmon, K.; Whelan, T.; Strasser-Weippl, K.; Rubin, S.; et al. Extending Aromatase-Inhibitor Adjuvant Therapy to 10 Years. N. Engl. J. Med. 2016, 375, 209–219. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Univariate | Multivariate a | |||||
|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | P Value | HR | 95% CI | P Value |
| Age | ||||||
| <40 | 1 | 1 | ||||
| 40–49 | 0.708 | 0.656–0.763 | <0.001 | 0.707 | 0.652–0.768 | <0.001 |
| 50–59 | 0.706 | 0.656–0.760 | <0.001 | 0.709 | 0.654–0.768 | <0.001 |
| 60–69 | 0.747 | 0.694–0.805 | <0.001 | 0.759 | 0.700–0.824 | <0.001 |
| ≥70 | 0.703 | 0.652–0.758 | <0.001 | 0.746 | 0.686–0.811 | <0.001 |
| Race | ||||||
| Black | 1 | 1 | ||||
| White | 0.739 | 0.693–0.788 | <0.001 | 0.762 | 0.709–0.819 | <0.001 |
| Other | 0.734 | 0.670–0.803 | <0.001 | 0.744 | 0.674–0.822 | <0.001 |
| Year of diagnosis | ||||||
| 1990–1994 | 1 | 1 | ||||
| 1995–1999 | 1.062 | 1.011–1.115 | 0.016 | 1.038 | 0.983–1.095 | 0.181 |
| 2000–2004 | 1.04 | 0.985–1.097 | 0.158 | 0.994 | 0.937–1.055 | 0.85 |
| 2005–2009 | 0.867 | 0.808-0.930 | <0.001 | 0.837 | 0.775–0.903 | <0.001 |
| Stage | ||||||
| I | 1 | 1 | ||||
| IIA | 0.928 | 0.889–0.969 | 0.01 | 0.91 | 0.868–0.954 | <0.001 |
| IIB | 0.935 | 0.872–1.002 | 0.056 | 0.936 | 0.868–1.008 | 0.079 |
| Hormone receptor status | ||||||
| + vs. − | 0.814 | 0.775–0.855 | <0.001 | 0.839 | 0.797–0.883 | <0.001 |
| Radiotherapy | ||||||
| Yes vs. No/Refused | 1.261 | 1.213–1.310 | <0.001 | 1.258 | 1.206–1.312 | <0.001 |
| Sex | ||||||
| Male vs. Female | 0.332 | 0.209–0.526 | <0.001 | 0.363 | 0.215–0.613 | <0.001 |
| Characteristic | Total | |||||
|---|---|---|---|---|---|---|
| Trend 1 | Trend 2 | Trend 3 | ||||
| Period | APC (95% CI) | Period | APC (95% CI) | Period | APC (95% CI) | |
| Total | 1–11 | 3.7 *, (2.9–4.5) | 11–21 | 1.1, ((−0.4)–2.7) | 21–24 | −8.5 ((−24)–10.1) |
| Age | ||||||
| <40 | 1–4 | 51.4 *, (12.8–103.1) | 4–24 | 0.6, ((−1.6)–3.0) | NA | NA |
| 40–49 | 1–11 | 8.0 *, (6.1–10.0) | 11–24 | 1.5, ((−0.8)–3.9) | NA | NA |
| 50–59 | 1–12 | 8.5 *, (6.8–10.2) | 12–24 | 1.2, ((−1.8)–4.4) | NA | NA |
| 60–69 | 1–11 | 6.4 *, (4.8–8.0) | 11–23 | −0.2, ((−2.6)–2.4) | NA | NA |
| ≥70 | 1–9 | 5.7 *, (3.0–8.5) | 9–23 | −4.3 *, ((−8.2)–(−0.2)) | NA | NA |
| Race | ||||||
| Black | 1–7 | 17.7 *, (11.1–24.6) | 7–23 | −0.5, ((−3.0)–2.1) | NA | NA |
| White | 1-10 | 7.1 *, (6.2–7.9) | 10–24 | 1.0 *, (0.1–2.0) | NA | NA |
| Other | 1-24 | 6.6 *, (5.2–8.0) | NA | NA | NA | NA |
| Year of diagnosis | ||||||
| 1990–1994 | 1–4 | 14.7 *, (2.8–28) | 4–24 | 2.1 *, (1.3–2.8) | NA | NA |
| 1995–1999 | 1–3 | 24.1, ((−2.2)–57.5) | 3–19 | 4.2 *, (3.1–5.2) | NA | NA |
| 2000–2004 | 1–14 | 6.7 *, (5.5–8.0) | NA | NA | NA | NA |
| 2005–2009 | 1–3 | –16.5, ((−43.4)–23.1) | 3–9 | 21.0 *, (10.3–32.7) | NA | NA |
| Stage | ||||||
| I | 1–8 | 8.8 *, (7.6–10.0) | 8–19 | 2.1 *, (1.2–3.0) | 19–24 | −5.6 *, ((−13.6)–3.2) |
| IIA | 1–10 | 7.0 *, (5.2–8.9) | 10–24 | 1.4, ((−0.6)–3.4) | NA | NA |
| IIB | 1–23 | 5.4 *, (4.2–6.6) | NA | NA | NA | NA |
| Hormone receptor status | ||||||
| + | 1–3 | 2.3, ((−7.2)–12.9) | 3–11 | 8.4 *, (6.9–9.8) | 11–24 | 0.8, ((−0.4)–2.1) |
| – | 1–3 | 44.1 *, (7.0–94.0) | 3–24 | 1.5 *, (0.2–2.7) | NA | NA |
| RT | ||||||
| Yes | 1–4 | 18.5 *, (10.9–26.5) | 4–11 | 8.0 *, (6.0–10.2) | 11–24 | 2.9 *, (1.5–4.4) |
| No/Refused | 1–4 | −2.5, ((−9.8)–5.4) | 4–7 | 10.2, ((−6.9)–30.4) | 7–24 | −0.3, ((−1.6)–1.0) |
| Stage | Unadjusted a | Multivariate-Adjusted a,b | PS-Adjusted a,b | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | P Value | HR (95% CI) | P Value | HR (95% CI) | P Value | |
| Overall survival | ||||||
| All | 0.676 (0.648–0.706) | <0.001 | 0.776 (0.743–0.810) | <0.001 | 0.815 (0.780–0.852) | <0.001 |
| I | 0.638 (0.606–0.673) | <0.001 | 0.777 (0.737–0.820) | <0.001 | 0.825 (0.782–0.870) | <0.001 |
| IIA | 0.627 (0.575–0.684) | <0.001 | 0.754 (0.691–0.823) | <0.001 | 0.790 (0.724–0.863) | <0.001 |
| IIB | 0.604 (0.520–0.702) | <0.001 | 0.750 (0.645–0.873) | <0.001 | 0.716 (0.616–0.833) | <0.001 |
| Breast cancer-specific survival | ||||||
| All | 0.630 (0.586–0.678) | <0.001 | 0.482 (0.447–0.520) | <0.001 | 0.510 (0.474–0.549) | <0.001 |
| I | 0.457 (0.414–0.505) | <0.001 | 0.427 (0.385–0.474) | <0.001 | 0.445 (0.402–0.494) | <0.001 |
| IIA | 0.559 (0.492–0.634) | <0.001 | 0.521 (0.458–0.594) | <0.001 | 0.552 (0.486–0.627) | <0.001 |
| IIB | 0.609 (0.502–0.740) | <0.001 | 0.572 (0.467–0.701) | <0.001 | 0.594 (0.488–0.723) | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, Z.; Yang, L.; Deng, G.; Huang, X.; Li, X.; Xie, X.; Wang, J.; Shuang, Z.; Wang, X. Patterns of Occurrence and Outcomes of Contralateral Breast Cancer: Analysis of SEER Data. J. Clin. Med. 2018, 7, 133. https://doi.org/10.3390/jcm7060133
Xiong Z, Yang L, Deng G, Huang X, Li X, Xie X, Wang J, Shuang Z, Wang X. Patterns of Occurrence and Outcomes of Contralateral Breast Cancer: Analysis of SEER Data. Journal of Clinical Medicine. 2018; 7(6):133. https://doi.org/10.3390/jcm7060133
Chicago/Turabian StyleXiong, Zhenchong, Lin Yang, Guangzheng Deng, Xinjian Huang, Xing Li, Xinhua Xie, Jin Wang, Zeyu Shuang, and Xi Wang. 2018. "Patterns of Occurrence and Outcomes of Contralateral Breast Cancer: Analysis of SEER Data" Journal of Clinical Medicine 7, no. 6: 133. https://doi.org/10.3390/jcm7060133
APA StyleXiong, Z., Yang, L., Deng, G., Huang, X., Li, X., Xie, X., Wang, J., Shuang, Z., & Wang, X. (2018). Patterns of Occurrence and Outcomes of Contralateral Breast Cancer: Analysis of SEER Data. Journal of Clinical Medicine, 7(6), 133. https://doi.org/10.3390/jcm7060133