Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Research Setting
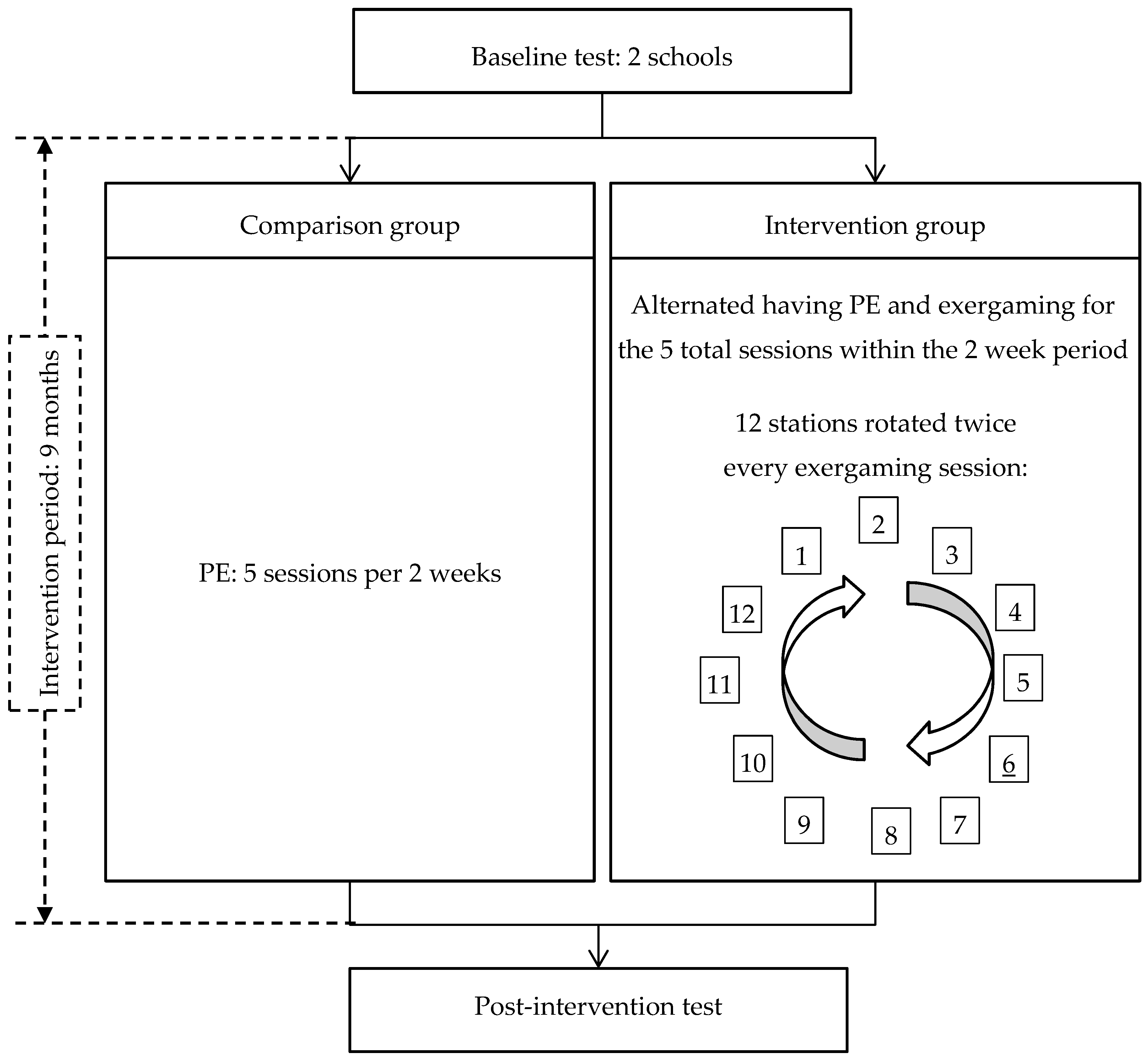
2.2. Procedures
2.3. Measures
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Roriz de Oliveira, M.S.; Seabra, A.; Garganta, R.; Ribeiro Maia, J.A. Decennial trend in passing rates of health-related physical fitness in children from Maia county, northern Portugal. Ann. Hum. Biol. 2012, 39, 453. [Google Scholar]
- Albon, H.M.; Hamlin, M.J.; Ross, J.J. Secular trends and distributional changes in health and fitness performance variables of 10–14-year-old children in New Zealand between 1991 and 2003. Br. J. Sport Med. 2010, 44, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Yang, Y.; Kong, Z.X.; Zhang, Y.M.; Zhuang, J. Prevalence of physical fitness in Chinese school-aged children: Findings from the 2016 physical activity and fitness in China-the Youth Study. J. Sport Health Sci. 2017, 6, 395–403. [Google Scholar] [CrossRef]
- Smith, J.J.; Eather, N.; Morgan, P.J.; Plotnikoff, R.C.; Faigenbaum, A.D.; Lubans, D.R. The health benefits of muscular fitness for children and adolescents: A systematic review and meta-analysis. Sports Med. 2014, 44, 1209–1223. [Google Scholar] [CrossRef] [PubMed]
- Casonatto, J.; Fernandes, R.A.; Batista, M.B.; Cyrino, E.S.; Coelho-e-Silva, M.J.; de Arruda, M.; Ronque, E.R.V. Association between health-related physical fitness and body mass index status in children. J. Child Health Care 2016, 20, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.L.; Chang, M.; Solmon, M.A. Physical activity, physical fitness, and health-related quality of life in school-aged children. J. Teach. Phys. Educ. 2016, 35, 117–126. [Google Scholar] [CrossRef]
- Venckunas, T.; Emeljanovas, A.; Mieziene, B.; Volbekiene, V. Secular trends in physical fitness and body size in Lithuanian children and adolescents between 1992 and 2012. J. Epidemiol. Commun. Health 2017, 71, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, F.K.; Prista, A.; Gomes, T.N.Q.F.; Daca, T.; Madeira, A.; Katzmarzyk, P.T.; Maia, J.A.R. Secular trends in physical fitness of Mozambican school-aged children and adolescents. Am. J. Hum. Biol. 2015, 27, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Soltani, P.; Vilas-Boas, J.P. Sport Exergames for physical education. In Encyclopedia of Information Science and Technology, 4th ed.; IGI Global: Calgary, AB, Canada, 2018; pp. 7358–7367. [Google Scholar]
- Barnett, L.M.; Van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Does childhood motor skill proficiency predict adolescent fitness? Med. Sci. Sport Exerc. 2008, 40, 2137–2144. [Google Scholar] [CrossRef] [PubMed]
- Re, A.H.N.; Cattuzzo, M.T.; Santos, F.M.C.; Monteiro, C.B.M. Anthropometric characteristics, field test scores and match-related technical performance in youth indoor soccer players with different playing status. Int. J. Perform. Anal. Sport 2014, 14, 482–492. [Google Scholar]
- Lima, R.A.; Pfeiffer, K.; Larsen, L.R.; Bugge, A.; Moller, N.C.; Anderson, L.B.; Stodden, D.F. Physical activity and motor competence present a positive reciprocal longitudinal relationship across childhood and early adolescence. J. Phys. Act. Health 2017, 14, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Haga, M.; Gisladottir, T.; Sigmundsson, H. The relationship between motor competence and physical fitness is weaker in the 15-16 yr. adolescent age group than in younger age groups (4–5 yr. and 11–12 yr.). Percept. Mot. Skill 2015, 121, 900–912. [Google Scholar] [CrossRef] [PubMed]
- Wick, K.; Leeger-Aschmann, C.S.; Monn, N.D.; Radtke, T.; Ott, L.V.; Rebholz, C.E.; Cruz, S.; Gerber, N.; Schmutz, E.A.; Puder, J.J.; et al. Interventions to promote fundamental movement skills in childcare and kindergarten: A systematic review and meta-analysis. Sports Med. 2017, 47, 2045–2068. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.K.; Costigan, S.A.; Morgan, P.J.; Lubans, D.R.; Stodden, D.F.; Salmon, J.; Barnett, L.M. Do school-based interventions focusing on physical activity, fitness, or fundamental movement skill competency produce a sustained impact in these outcomes in children and adolescents? A systematic review of follow-up studies. Sports Med. 2014, 44, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Tompsett, C.; Sanders, R.; Taylor, C.; Cobley, S. Pedagogical approaches to and effects of fundamental movement skill interventions on health outcomes: A systematic review. Sports Med. 2017, 47, 1795–1819. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Barnett, L.M.; Cliff, D.P.; Okely, A.D.; Scott, H.A.; Cohen, K.E.; Lubans, D.R. Fundamental movement skill interventions in youth: A systematic review and meta-analysis. Pediatrics 2013, 132, E1361–E1383. [Google Scholar] [CrossRef] [PubMed]
- Butt, J.; Weinberg, R.S.; Breckon, J.D.; Claytor, R.P. Adolescent physical activity participation and motivational determinants across gender, age, and race. J. Phys. Act. Health 2011, 8, 1074–1083. [Google Scholar] [CrossRef] [PubMed]
- Kari, T. Promoting physical activity and fitness with exergames: Updated systematic review of systematic reviews. In Transforming Gaming and Computer Simulation Technologies across Industries; IGI Global: Calgary, AB, Canada, 2017; pp. 225–245. [Google Scholar]
- Chen, H.; Sun, H.C. Effects of active videogame and sports, play, and active recreation for kids physical education on children’s health-related fitness and enjoyment. Games Health J. 2017, 6, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Pasco, D.; Roure, C.; Kermarrec, G.; Pope, Z.; Gao, Z. The effects of a bike active video game on players’ physical activity and motivation. J. Sport Health Sci. 2017, 6, 25–32. [Google Scholar] [CrossRef]
- Barnett, L.M.; Bangay, S.; McKenzie, S.; Ridgers, N.D. Active gaming as a mechanism to promote physical activity and fundamental movement skill in children. Front. Public Health 2013, 1, 74. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Pope, Z.; Lee, J.E.; Stodden, D.; Roncesvalles, N.; Pasco, D.; Huang, C.C.; Feng, D. Impact of exergaming on young children’s school day energy expenditure and moderate-to-vigorous physical activity levels. J. Sport Health Sci. 2017, 6, 11–16. [Google Scholar] [CrossRef]
- Chukhlantseva, N. Integration of active videogames in physical training of school students. Sci. Educ. 2017, 4, 14–20. [Google Scholar] [CrossRef]
- Arajuo, J.G.E.; Batista, C.; Moura, D.L. Exergames in physical education: A systematic review. Movimento 2017, 23, 529–542. [Google Scholar]
- Staiano, A.E.; Beyl, R.A.; Hsia, D.S.; Katzmarzyk, P.T.; Newton, R.L. Twelve weeks of dance exergaming in overweight and obese adolescent girls: Transfer effects on physical activity, screen time, and self-efficacy. J. Sport Health Sci. 2017, 6, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Norris, E.; Hamer, M.; Stamatakis, E. Active video games in schools and effects on physical activity and health: A systematic review. J. Pediatr. 2016, 172, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Ridgers, N.D.; Reynolds, J.; Hanna, L.; Salmon, J. Playing active video games may not develop movement skills: An intervention trial. Preve. Med. Rep. 2015, 2, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Hulteen, R.M.; Johnson, T.M.; Ridgers, N.D.; Mellecker, R.R.; Barnett, L.M. Children’s movement skills when playing active video games. Percept. Mot. Skill 2015, 121, 767–790. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Gao, Z. Effects of exergaming on fundamental movement skills among children and young adults: A systematic review. In Gaming: Trends, Perspectives and Impact on Health; Nova Science Publishers: Hauppauge, NY, USA, 2016; pp. 41–58. [Google Scholar]
- Edwards, J.; Jeffrey, S.; May, T.; Rinehart, N.J.; Barnett, L.M. Does playing a sports active video game improve object control skills of children with autism spectrum disorder? J. Sport Health Sci. 2017, 6, 17–24. [Google Scholar] [CrossRef]
- Vernadakis, N.; Papastergiou, M.; Zetou, E.; Antoniou, P. The impact of an exergame-based intervention on children’s fundamental motor skills. Comput. Educ. 2015, 83, 90–102. [Google Scholar] [CrossRef]
- Metzler, M. Instructional Models for Physical Education; Holocomb Hathaway: Scottsdale, AZ, USA, 2005. [Google Scholar]
- Lane, A.P.; Molina, S.L.; Tolleson, D.A.; Langendorfer, S.J.; Goodway, J.D.; Stodden, D.F. Developmental sequences for the standing long jump landing: A pre-longitudinal screening. J. Mot. Learn. Dev. 2018, 6, 114–129. [Google Scholar] [CrossRef]
- Nesbitt, D.R.; Molina, S.; Sacko, R.; Robinson, L.; Brian, A.; Stodden, D.F. Examining the feasibility of supine-to-stand as a measure of functional motor competence. J. Mot. Learn. Dev. 2018, in press. [Google Scholar] [CrossRef]
- Stodden, D.F.; Langendorfer, S.J.; Fleisig, G.S.; Andrews, J.R. Kinematic constraints associated with the acquisition of overarm throwing part I: Step and trunk actions. Res. Q. Exerc. Sport 2006, 77, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Langendorfer, S.J.; Fleisig, G.S.; Andrews, J.R. Kinematic constraints associated with the acquisition of overarm throwing part II: Upper extremity actions. Res. Q. Exerc. Sport 2006, 77, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Gao, Z.; Goodway, J.D.; Langendorfer, S.J. Dynamic relationships between motor skill competence and health-related fitness in youth. Pediatr. Exerc. Sci. 2014, 26, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Blimkie, C.; Castelli, D.; Corbin, C.B.; Daniels, S.R.; Kohl, H.W.; Malina, R.M.; Sacheck, J.; Stodden, D.F.; Whitt-Glover, M.; et al. Fitness measures and health outcomes in youth. In Institute of Medicine; Pillsbury, L., Oria, M., Pate, R., Eds.; National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Wind, A.E.; Takken, T.; Helders, P.J.M.; Engelbert, R.H.H. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults? Eur. J. Pediatr. 2010, 169, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Finco, M.D.; Reategui, E.; Zaro, M.A.; Sheehan, D.D.; Katz, L. Exergaming as an alternative for students unmotivated to participate in regular physical education classes. IJGBL 2015, 5, 1–10. [Google Scholar] [CrossRef]
- Sween, J.; Wallington, S.F.; Sheppard, V.; Taylor, T.; Llanos, A.A.; Adams-Campbell, L.L. The role of exergaming in improving physical activity: A review. J. Phys. Act. Health 2014, 11, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Salem, Y.; Gropack, S.J.; Coffin, D.; Godwin, E.M. Effectiveness of a low-cost virtual reality system for children with developmental delay: A preliminary randomised single-blind controlled trial. Physiotherapy 2012, 98, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z. Fight fire with fire? Promoting physical activity and health through active video games. J. Sport Health Sci. 2017, 6, 1–3. [Google Scholar] [CrossRef]
- Gao, Z.; Zhang, T.; Stodden, D. Children’s physical activity levels and psychological correlates in interactive dance versus aerobic dance. J. Sport Health Sci. 2013, 2, 146–151. [Google Scholar] [CrossRef]
- Maddison, R.; Mhurchu, C.N.; Jull, A.; Prapavessis, H.; Foley, L.S.; Jiang, Y.N. Active video games: The mediating effect of aerobic fitness on body composition. Int. J. Behav. Nutr. Phys. 2012, 9, 54. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Chen, S.; Pasco, D.; Pope, Z. A meta-analysis of active video games on health outcomes among children and adolescents. Obes. Rev. 2015, 16, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Christison, A.L.; Evans, T.A.; Bleess, B.B.; Wang, H.P.; Aldag, J.C.; Binns, H.J. Exergaming for health: A randomized study of community-based exergaming curriculum in pediatric weight management. Games Health J. 2016, 5, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Naugle, K.E.; Naugle, K.M.; Wikstrom, E.A. Cardiovascular and affective outcomes of active gaming: Using the Nintendo Wii as a cardiovascular training tool. J. Strength Cond. Res. 2014, 28, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Foley, L.; Jiang, Y.N.; Mhurchu, C.N.; Jull, A.; Prapavessis, H.; Rodgers, A.; Maddison, R. The effect of active video games by ethnicity, sex and fitness: Subgroup analysis from a randomised controlled trial. Int. J. Behav. Nutr. Phys. 2014, 11, 46. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; O’Hara, B.J.; Rogers, K.; St George, A.; Bauman, A. Contribution of organized and nonorganized activity to children’s motor skills and fitness. J. School Health 2014, 84, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Laitakari, J.; Vuori, I.; Oja, P. Is long-term maintenance of health-related physical activity possible? An analysis of concepts and evidence. Health Educ. Res. 1996, 11, 463–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabel, M.; Sjolund, A.; Broeren, J.; Arvidsson, D.; Saury, J.M.; Gillenstrand, J.; Emanuelson, I.; Blomgren, K.; Lannering, B. Effects of physically active video gaming on cognition and activities of daily living in childhood brain tumor survivors: A randomized pilot study. Neuro-Oncol. Pract. 2017, 4, 98–110. [Google Scholar] [CrossRef]
- Gao, Z. Motivated but not active: The dilemmas of incorporating interactive dance into gym class. J. Phys. Act. Health 2012, 9, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.M.; Ridgers, N.D.; Hulteen, R.M.; Mellecker, R.R.; Barnett, L.M. Does playing a sports active video game improve young children’s ball skill competence? J. Sci. Med. Sport 2016, 19, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.J.; Cooley, P.D.; Cruickshank, V.J. Caution regarding exergames: A skill acquisition perspective. Phys. Educ. Sport Pedagog. 2017, 22, 246–256. [Google Scholar] [CrossRef]
- Page, Z.E.; Barrington, S.; Edwards, J.; Barnett, L.M. Do active video games benefit the motor skill development of non-typically developing children and adolescents: A systematic review. J. Sci. Med. Sport 2017, 20, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Howie, E.K.; Campbell, A.C.; Abbott, R.A.; Straker, L.M. Understanding why an active video game intervention did not improve motor skill and physical activity in children with developmental coordination disorder: A quantity or quality issue? Res. Dev. Disabil. 2017, 60, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T. Exergaming: Hope for future physical activity? or blight on mankind? J. Sport Health Sci. 2017, 6, 44–46. [Google Scholar] [CrossRef]


{kind=link}
| Variables * | Baseline | Post-Intervention | ||||
|---|---|---|---|---|---|---|
| Comparison (n = 115) | Intervention (n = 135) | p Value ‡ | Comparison (n = 115) | Intervention (n = 135) | p Value ‡ | |
| Age (years) | 8.41 (0.71) | 8.14 (0.67) | 0.002 | / | / | / |
| Girls (counts) † | 59 (51.3) | 70 (51.9) | 0.931 | / | / | / |
| White American (counts) † | 69 (60.0) | 118 (87.4) | <0.001 | / | / | / |
| Height (cm) | 131.77 (7.59) | 129.46 (6.83) | 0.012 | 132.73 (7.24) | 132.80 (7.19) | 0.942 |
| Weight (kg) | 30.77 (9.12) | 31.69 (8.69) | 0.417 | 33.73 (9.65) | 32.95 (9.72) | 0.524 |
| Motor skill competence | ||||||
| Kicking (m/s) | 10.95 (1.79) | 11.06 (2.46) | 0.691 | 12.06 (1.87) | 11.84 (1.92) | 0.360 |
| Throwing (m/s) | 14.10 (3.82) | 14.55 (3.35) | 0.317 | 14.74 (3.87) | 14.48 (3.69) | 0.586 |
| Standing long jump (%) | 0.93 (0.15) | 0.93 (0.17) | 0.979 | 0.93 (0.15) | 0.91 (0.17) | 0.390 |
| Hops (%) | 0.64 (0.12) | 0.62 (0.14) | 0.190 | 0.67 (0.12) | 0.70 (0.14) | 0.124 |
| Health-related fitness | ||||||
| PACER (laps) | 22.92 (11.15) | 14.04 (7.08) | <0.001 | 26.87 (13.24) | 20.67 (9.30) | <0.001 |
| Grip strength (kg) | 13.90 (2.96) | 14.50 (3.48) | 0.143 | 12.86 (3.66) | 16.22 (4.01) | <0.001 |
| Push-ups (counts) | 7.47 (6.26) | 6.24 (6.07) | 0.116 | 9.32 (6.47) | 8.65 (6.23) | 0.409 |
| Curl-ups (counts) | 34.60 (26.57) | 23.49 (21.86) | <0.001 | 18.58 (18.93) | 21.33 (19.65) | 0.262 |
| BMI (kg/cm2) | 17.60 (3.78) | 18.72 (3.67) | 0.019 | 18.88 (3.89) | 18.42 (3.87) | 0.346 |
| Tests | Conditions | Baseline T-Scored Mean (SD) | Post-Test T-Scored Mean (SD) | Diff. Mean (SD) | F | p | η2 |
|---|---|---|---|---|---|---|---|
| MSC | |||||||
| Locomotor | Intervention (n = 135) | 49.34 (7.23) | 50.11 (7.21) | 0.77 (4.64) | 1.03 | 0.311 | 0.00 |
| Comparison (n = 115) | 49.77 (6.68) | 49.98 (6.68) | 0.20 (4.16) | ||||
| Object control | Intervention (n = 135) | 49.02 (9.21) | 50.87 ‡ (9.01) | 1.85 (5.51) | 6.77 | 0.010 | 0.03 |
| Comparison (n = 115) | 48.20 (8.45) | 51.73 ‡ (8.66) | 3.54 (4.59) | ||||
| HRF | |||||||
| PACER | Intervention (n = 135) | 44.23 † (6.33) | 49.00 ‡ (8.56) | 4.77 (6.40) | 1.77 | 0.184 | 0.01 |
| Comparison (n = 115) | 52.21 (9.95) | 55.69 ‡ (11.84) | 3.48 (8.93) | ||||
| Musculoskeletal fitness | Intervention (n = 135) | 49.37 (6.74) | 51.25 ‡ (7.08) | 1.88 (5.19) | 38.33 | <0.001 | 0.13 |
| Comparison (n = 115) | 50.83 (7.64) | 48.30 ‡ (6.08) | −2.53 (6.08) | ||||
| Body mass index | Intervention (n = 135) | 50.81 * (9.76) | 50.01 † (10.31) | −0.80 (4.33) | 61.39 | <0.001 | 0.20 |
| Comparison (n = 115) | 47.83 (10.06) | 51.24 ‡ (10.35) | 3.41 (4.12) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, S.; Lee, J.E.; Stodden, D.F.; Gao, Z. Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study. J. Clin. Med. 2018, 7, 261. https://doi.org/10.3390/jcm7090261
Ye S, Lee JE, Stodden DF, Gao Z. Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study. Journal of Clinical Medicine. 2018; 7(9):261. https://doi.org/10.3390/jcm7090261
Chicago/Turabian StyleYe, Sunyue, Jung Eun Lee, David F. Stodden, and Zan Gao. 2018. "Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study" Journal of Clinical Medicine 7, no. 9: 261. https://doi.org/10.3390/jcm7090261
APA StyleYe, S., Lee, J. E., Stodden, D. F., & Gao, Z. (2018). Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study. Journal of Clinical Medicine, 7(9), 261. https://doi.org/10.3390/jcm7090261