Risk of Dementia in Older Patients with Type 2 Diabetes on Dipeptidyl-Peptidase IV Inhibitors Versus Sulfonylureas: A Real-World Population-Based Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Data Source
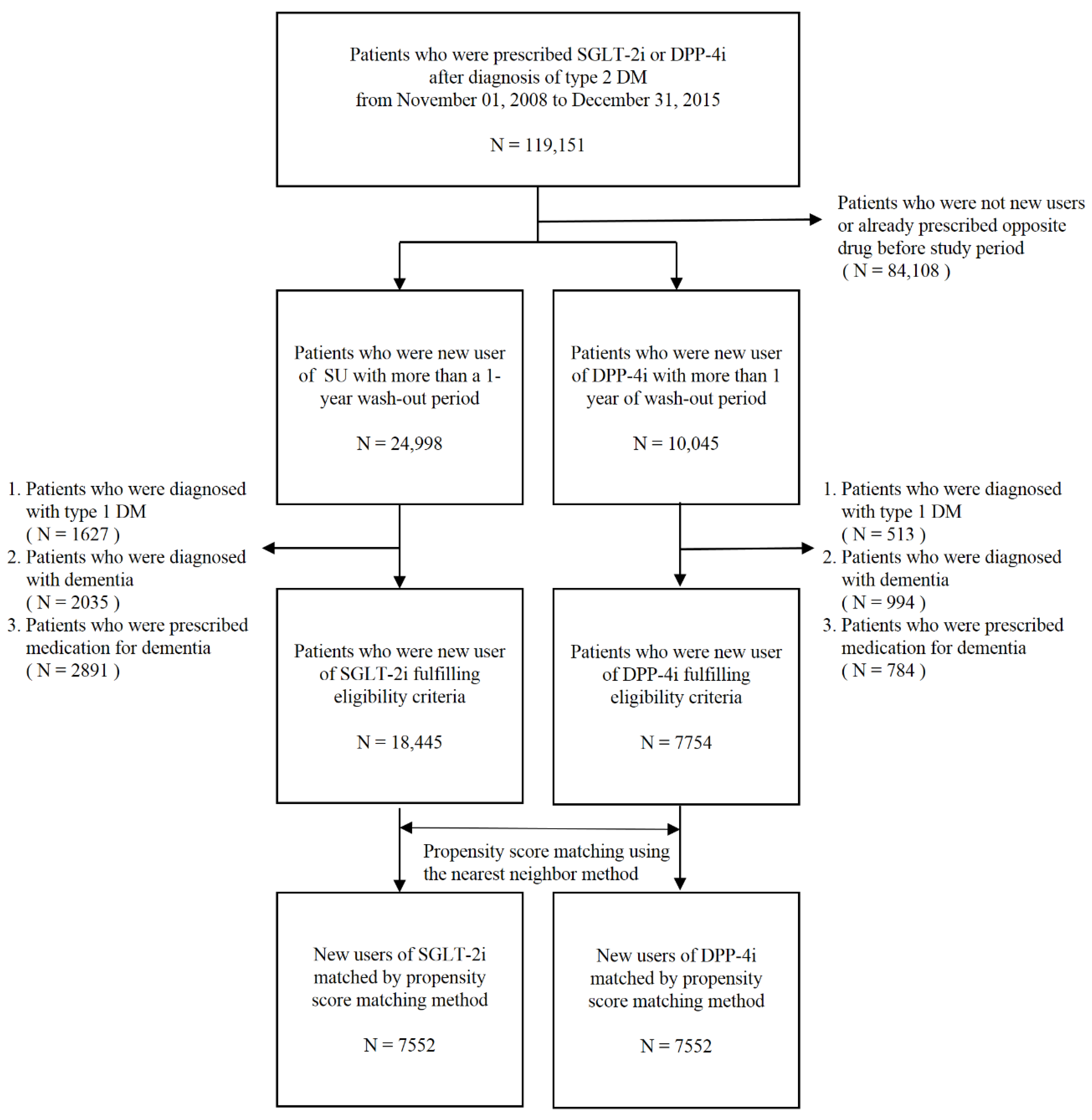
2.2. Inclusion and Exclusion Criteria
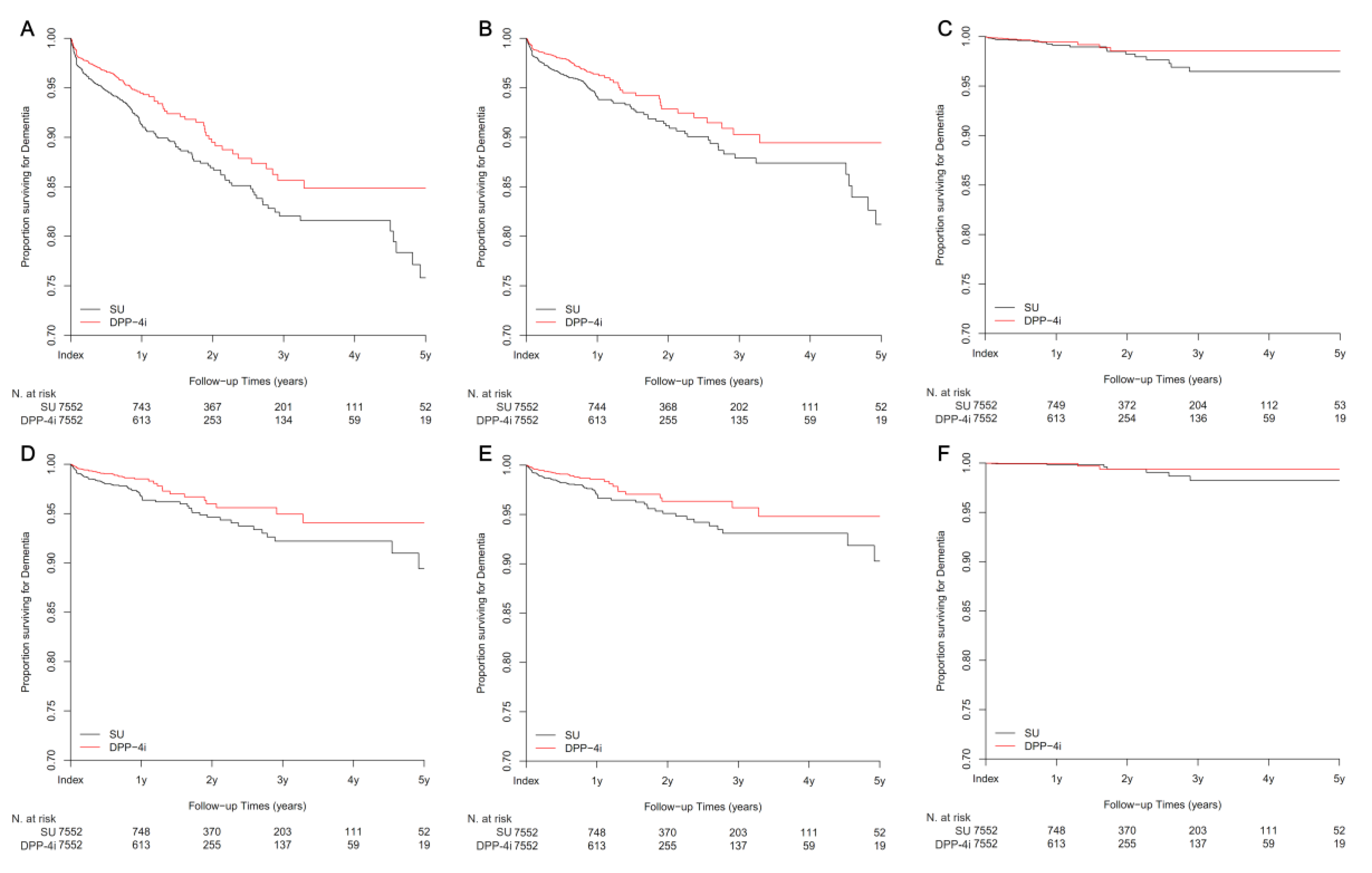
2.3. Study Outcome and Subgroup Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guariguata, L.; Whiting, D.R.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dementia [article online] 2012. Available online: http://www.who.int/mediacentre/factsheets/fs362/en/ (accessed on 13 February 2015).
- Profenno, L.A.; Porsteinsson, A.P.; Faraone, S.V. Meta-analysis of Alzheimer’s disease risk with obesity, diabetes, and related disorders. Biol. Psychiatry 2010, 67, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Biessels, G.J.; Staekenborg, S.; Brunner, E.; Brayne, C.; Scheltens, P. Risk of dementia in diabetes mellitus: A systematic review. Lancet Neurol. 2006, 5, 64–74. [Google Scholar] [CrossRef]
- Gudala, K.; Bansal, D.; Schifano, F.; Bhansali, A. Diabetes mellitus and risk of dementia: A meta-analysis of prospective observational studies. J. Diabetes Investig. 2013, 4, 640–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strachan, M.W.; Reynolds, R.M.; Marioni, R.E.; Price, J.F. Cognitive function, dementia and type 2 diabetes mellitus in the elderly. Nat. Rev. Endocrinol. 2011, 7, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, T. Diabetes mellitus and dementia. Curr. Diab. Rep. 2014, 14, 487. [Google Scholar] [CrossRef] [PubMed]
- Femminella, G.D.; Bencivenga, L.; Petraglia, L.; Visaggi, L.; Gioia, L.; Grieco, F.V.; de Lucia, C.; Komici, K.; Corbi, G.; Edison, P.; et al. Antidiabetic Drugs in Alzheimer's Disease: Mechanisms of Action and Future Perspectives. J. Diabetes Res. 2017, 2017, 7420796. [Google Scholar] [CrossRef] [PubMed]
- Biessels, G.J.; Strachan, M.W.; Visseren, F.L.; Kappelle, L.J.; Whitmer, R.A. Dementia and cognitive decline in type 2 diabetes and prediabetic stages: Towards targeted interventions. Lancet Diabetes Endocrinol. 2014, 2, 246–255. [Google Scholar] [CrossRef]
- Phung, O.J.; Scholle, J.M.; Talwar, M.; Coleman, C.I. Effect of noninsulin antidiabetic drugs added to metformin therapy on glycemic control, weight gain, and hypoglycemia in type 2 diabetes. JAMA 2010, 303, 1410–1418. [Google Scholar] [CrossRef]
- Kosaraju, J.; Murthy, V.; Khatwal, R.B.; Dubala, A.; Chinni, S.; Muthureddy Nataraj, S.K.; Basavan, D. Vildagliptin: An anti-diabetes agent ameliorates cognitive deficits and pathology observed in streptozotocin-induced Alzheimer’s disease. J. Pharm. Pharmacol. 2013, 65, 1773–1784. [Google Scholar] [CrossRef]
- Kosaraju, J.; Gali, C.C.; Khatwal, R.B.; Dubala, A.; Chinni, S.; Holsinger, R.M.; Madhunapantula, V.S.; Muthureddy Nataraj, S.K.; Basavan, D. Saxagliptin: A dipeptidyl peptidase-4 inhibitor ameliorates streptozotocin induced Alzheimer’s disease. Neuropharmacology 2013, 72, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Sharma, B. Neuroprotective effect of selective DPP-4 inhibitor in experimental vascular dementia. Physiol. Behav. 2015, 152, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Zheng, T.; Qin, L.; Chen, B.; Hu, X.; Zhang, X.; Liu, Y.; Liu, H.; Qin, S.; Li, G.; Li, Q. Association of Plasma DPP4 Activity with Mild Cognitive Impairment in Elderly Patients With Type 2 Diabetes: Results from the GDMD Study in China. Diabetes Care 2016, 39, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Imfeld, P.; Bodmer, M.; Jick, S.S.; Meier, C.R. Metformin, other antidiabetic drugs, and risk of Alzheimer’s disease: A population-based case-control study. J. Am. Geriatr. Soc. 2012, 60, 916–921. [Google Scholar] [CrossRef] [PubMed]
- de la Monte, S.M. Type 3 diabetes is sporadic Alzheimers disease: Mini-review. Eur. Neuropsychopharmacol. 2014, 24, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Kornelius, E.; Lin, C.L.; Chang, H.H.; Li, H.H.; Huang, W.N.; Yang, Y.S.; Lu, Y.L.; Peng, C.H.; Huang, C.N. DPP-4 Inhibitor Linagliptin Attenuates Abeta-induced Cytotoxicity through Activation of AMPK in Neuronal Cells. CNS Neurosci. Ther. 2015, 21, 549–557. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, M.; Di Filippo, C.; Marfella, R.; Abbatecola, A.M.; Ferraraccio, F.; Rossi, F.; Paolisso, G. Long-term inhibition of dipeptidyl peptidase-4 in Alzheimer's prone mice. Exp. Gerontol. 2010, 45, 202–207. [Google Scholar] [CrossRef]
- Pipatpiboon, N.; Pintana, H.; Pratchayasakul, W.; Chattipakorn, N.; Chattipakorn, S.C. DPP4-inhibitor improves neuronal insulin receptor function, brain mitochondrial function and cognitive function in rats with insulin resistance induced by high-fat diet consumption. Eur. J. Neurosci. 2013, 37, 839–849. [Google Scholar] [CrossRef]
- Pintana, H.; Apaijai, N.; Chattipakorn, N.; Chattipakorn, S.C. DPP-4 inhibitors improve cognition and brain mitochondrial function of insulin-resistant rats. J. Endocrinol. 2013, 218, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Gault, V.A.; Lennox, R.; Flatt, P.R. Sitagliptin, a dipeptidyl peptidase-4 inhibitor, improves recognition memory, oxidative stress and hippocampal neurogenesis and upregulates key genes involved in cognitive decline. Diabetes Obes. Metab. 2015, 17, 403–413. [Google Scholar] [CrossRef]
- Kim, D.H.; Huh, J.W.; Jang, M.; Suh, J.H.; Kim, T.W.; Park, J.S.; Yoon, S.Y. Sitagliptin increases tau phosphorylation in the hippocampus of rats with type 2 diabetes and in primary neuron cultures. Neurobiol. Dis. 2012, 46, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Tasci, I.; Naharci, M.I.; Bozoglu, E.; Safer, U.; Aydogdu, A.; Yilmaz, B.F.; Yilmaz, G.; Doruk, H. Cognitive and functional influences of vildagliptin, a DPP-4 inhibitor, added to ongoing metformin therapy in elderly with type 2 diabetes. Endocr. Metab. Immune Disord. Drug Targets 2013, 13, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.R.; Barbieri, M.; Boccardi, V.; Angellotti, E.; Marfella, R.; Paolisso, G. Dipeptidyl peptidase-4 inhibitors have protective effect on cognitive impairment in aged diabetic patients with mild cognitive impairment. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Isik, A.T.; Soysal, P.; Yay, A.; Usarel, C. The effects of sitagliptin, a DPP-4 inhibitor, on cognitive functions in elderly diabetic patients with or without Alzheimer’s disease. Diabetes Res. Clin. Pract. 2017, 123, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Barkas, F.; Elisaf, M.; Tsimihodimos, V.; Milionis, H. Dipeptidyl peptidase-4 inhibitors and protection against stroke: A systematic review and meta-analysis. Diabetes Metab. 2017, 43, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Biessels, G.J.; Janssen, J.; van den Berg, E.; Zinman, B.; Espeland, M.A.; Mattheus, M.; Johansen, O.E.; investigators, C. Rationale and design of the CAROLINA(R)—Cognition substudy: A randomised controlled trial on cognitive outcomes of linagliptin versus glimepiride in patients with type 2 diabetes mellitus. BMC Neurol. 2018, 18, 7. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.H., Jr.; Fillenbaum, G.G.; Ezell, M.E. The accuracy of medicare claims data in identifying Alzheimer’s disease. J. Clin. Epidemiol. 2002, 55, 929–937. [Google Scholar] [CrossRef]
- Taylor, D.H., Jr.; Ostbye, T.; Langa, K.M.; Weir, D.; Plassman, B.L. The accuracy of Medicare claims as an epidemiological tool: The case of dementia revisited. J. Alzheimer's Dis. 2009, 17, 807–815. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| SU | DPP-4i | SMD | |
|---|---|---|---|
| N | 7552 | 7552 | |
| Age (SD) | 75.42 (5.31) | 75.39 (4.73) | 0.007 |
| Sex (Male, percent) | 44.01 | 43.39 | 0.013 |
| Socio-economic status (n, (%)) | 0.060 | ||
| 1st to 4th of 11 quantiles | 1892 (25.05) | 1892 (25.05) | |
| 5th to 8th of 11 quantiles | 2301 (30.47) | 2378 (31.49) | |
| 9th to 11th of 11 quantiles | 3359 (44.48) | 3282 (43.46) | |
| Hypertension | 79.61 | 80.39 | 0.020 |
| Dyslipidemia | 74.13 | 74.44 | 0.007 |
| Chronic kidney disease | 5.77 | 5.61 | 0.007 |
| End-stage renal disease | 2.56 | 2.49 | 0.004 |
| Any malignancy | 12.47 | 12.27 | 0.006 |
| Migraine | 4.86 | 4.89 | 0.001 |
| Asthma | 21.93 | 22.30 | 0.009 |
| Chronic obstructive pulmonary disease | 13.55 | 13.85 | 0.009 |
| Connective tissue disease | 6.50 | 6.46 | 0.002 |
| Atrial fibrillation | 4.97 | 4.67 | 0.014 |
| Heart failure | 8.74 | 8.91 | 0.006 |
| Osteoporosis | 25.08 | 25.52 | 0.010 |
| Cerebrovascular disease | |||
| Ischemic stroke | 11.30 | 11.40 | 0.003 |
| Hemorrhagic stroke | 0.91 | 0.91 | <0.001 |
| Transient ischemic attack | 3.42 | 3.34 | 0.004 |
| Acute myocardial infarction | 2.65 | 2.78 | 0.008 |
| Other ischemic heart disease | 25.20 | 25.77 | 0.013 |
| Other heart disease | 18.18 | 18.68 | 0.013 |
| Peripheral artery disease | 1.44 | 1.44 | <0.001 |
| Microvascular complications of diabetes | |||
| Neuropathy | 10.88 | 10.58 | 0.010 |
| Nephropathy | 5.79 | 5.75 | 0.002 |
| Retinopathy | 10.05 | 10.45 | 0.013 |
| Alcohol use † | 3.48 | 3.15 | 0.018 |
| Tobacco use † | 0.05 | 0.07 | 0.005 |
| Obesity † | 0.08 | 0.08 | <0.001 |
| Hypoglycemia | 2.73 | 2.32 | 0.026 |
| Medication use | |||
| Anti-diabetic medicine | |||
| Metformin | 93.98 | 93.95 | 0.001 |
| Thiazolidinedione | 5.27 | 5.08 | 0.008 |
| Alpha-glucosidase inhibitor | 15.21 | 15.39 | 0.005 |
| Meglitinide | 8.33 | 8.10 | 0.008 |
| SGLT2i | 0.54 | 0.87 | 0.039 |
| Insulin | 37.45 | 37.01 | 0.009 |
| Anti-hypertensive agent | |||
| Calcium channel blocker | 69.95 | 70.21 | 0.005 |
| ACEI | 32.56 | 32.94 | 0.008 |
| ARB | 72.64 | 72.91 | 0.006 |
| Beta blocker | 47.96 | 48.34 | 0.008 |
| Alpha blocker | 13.33 | 13.04 | 0.009 |
| Diuretics | 67.00 | 66.71 | 0.006 |
| Aspirin | 73.38 | 73.90 | 0.012 |
| P2Y12 inhibitor | 32.79 | 32.93 | 0.003 |
| Warfarin | 5.95 | 5.55 | 0.017 |
| Other antiplatelet | 25.73 | 25.45 | 0.006 |
| NOAC | 3.30 | 3.63 | 0.018 |
| Lipid-lowering agent | |||
| Statin | 72.22 | 73.20 | 0.022 |
| Fibrate | 15.28 | 15.04 | 0.007 |
| Ezetimibe | 7.79 | 8.00 | 0.008 |
| N | Events | HR | Lower CI | Upper CI | p-Value | |
|---|---|---|---|---|---|---|
| Event defined with diagnosis codes | ||||||
| All-cause dementia | 15,104 | 565 | 0.66 | 0.56 | 0.78 | <0.001 |
| Alzheimer’s disease | 15,104 | 367 | 0.64 | 0.52 | 0.79 | <0.001 |
| Vascular dementia | 15,104 | 54 | 0.66 | 0.38 | 1.14 | 0.14 |
| Event defined with diagnosis codes and medication | ||||||
| All-cause dementia | 15,104 | 184 | 0.54 | 0.40 | 0.73 | <0.001 |
| Alzheimer’s disease | 15,104 | 164 | 0.54 | 0.39 | 0.75 | <0.001 |
| Vascular dementia | 15,104 | 14 | 0.46 | 0.14 | 1.46 | 0.18 |
| N | Events | HR | Lower CI | Upper CI | p-Value | |
|---|---|---|---|---|---|---|
| Male | 6601 | 202 | 0.60 | 0.45 | 0.80 | <0.001 |
| Female | 8503 | 363 | 0.69 | 0.56 | 0.85 | <0.001 |
| Patients aged ≥75 years | 7662 | 376 | 0.61 | 0.50 | 0.76 | <0.001 |
| Patients aged <75 years | 7442 | 189 | 0.77 | 0.58 | 1.03 | 0.08 |
| Patients with DM microvascular complication | 3418 | 144 | 0.74 | 0.53 | 1.03 | 0.07 |
| Patients without DM microvascular complication | 11686 | 421 | 0.64 | 0.52 | 0.78 | <0.001 |
| Patients with DM macrovascular complication | 5487 | 227 | 0.67 | 0.51 | 0.87 | 0.003 |
| Patients without DM macrovascular complication | 9617 | 338 | 0.65 | 0.52 | 0.81 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-G.; Jeon, J.Y.; Kim, H.J.; Kim, D.J.; Lee, K.-W.; Moon, S.Y.; Han, S.J. Risk of Dementia in Older Patients with Type 2 Diabetes on Dipeptidyl-Peptidase IV Inhibitors Versus Sulfonylureas: A Real-World Population-Based Cohort Study. J. Clin. Med. 2019, 8, 28. https://doi.org/10.3390/jcm8010028
Kim Y-G, Jeon JY, Kim HJ, Kim DJ, Lee K-W, Moon SY, Han SJ. Risk of Dementia in Older Patients with Type 2 Diabetes on Dipeptidyl-Peptidase IV Inhibitors Versus Sulfonylureas: A Real-World Population-Based Cohort Study. Journal of Clinical Medicine. 2019; 8(1):28. https://doi.org/10.3390/jcm8010028
Chicago/Turabian StyleKim, Young-Gun, Ja Young Jeon, Hae Jin Kim, Dae Jung Kim, Kwan-Woo Lee, So Young Moon, and Seung Jin Han. 2019. "Risk of Dementia in Older Patients with Type 2 Diabetes on Dipeptidyl-Peptidase IV Inhibitors Versus Sulfonylureas: A Real-World Population-Based Cohort Study" Journal of Clinical Medicine 8, no. 1: 28. https://doi.org/10.3390/jcm8010028
APA StyleKim, Y. -G., Jeon, J. Y., Kim, H. J., Kim, D. J., Lee, K. -W., Moon, S. Y., & Han, S. J. (2019). Risk of Dementia in Older Patients with Type 2 Diabetes on Dipeptidyl-Peptidase IV Inhibitors Versus Sulfonylureas: A Real-World Population-Based Cohort Study. Journal of Clinical Medicine, 8(1), 28. https://doi.org/10.3390/jcm8010028