Spectral Analysis of the QT Interval Increases the Prediction Accuracy of Clinical Variables in Brugada Syndrome


 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Population and Recording Protocol
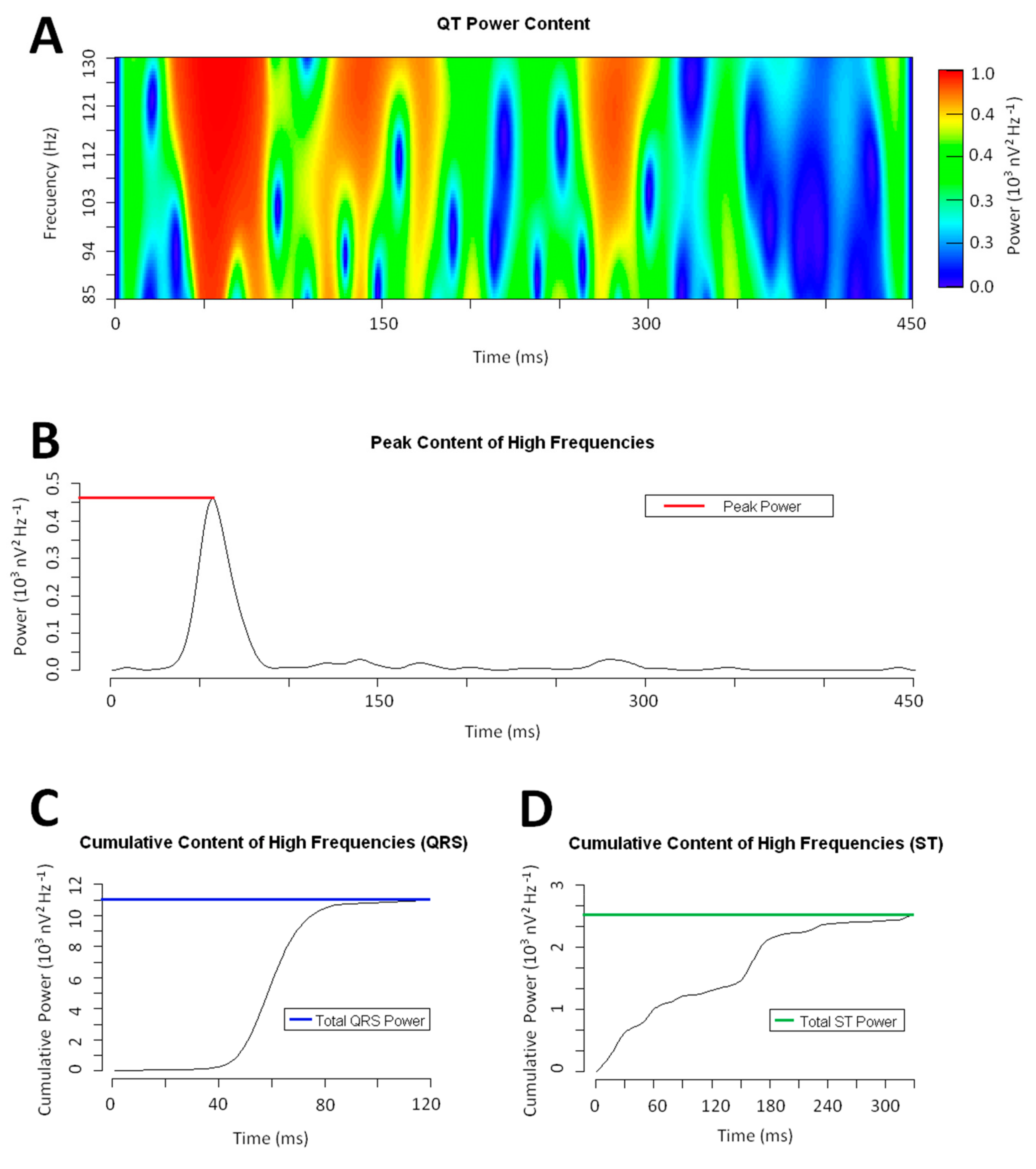
2.2. Signal Processing
2.3. Definitions
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patients and Clinical Variables
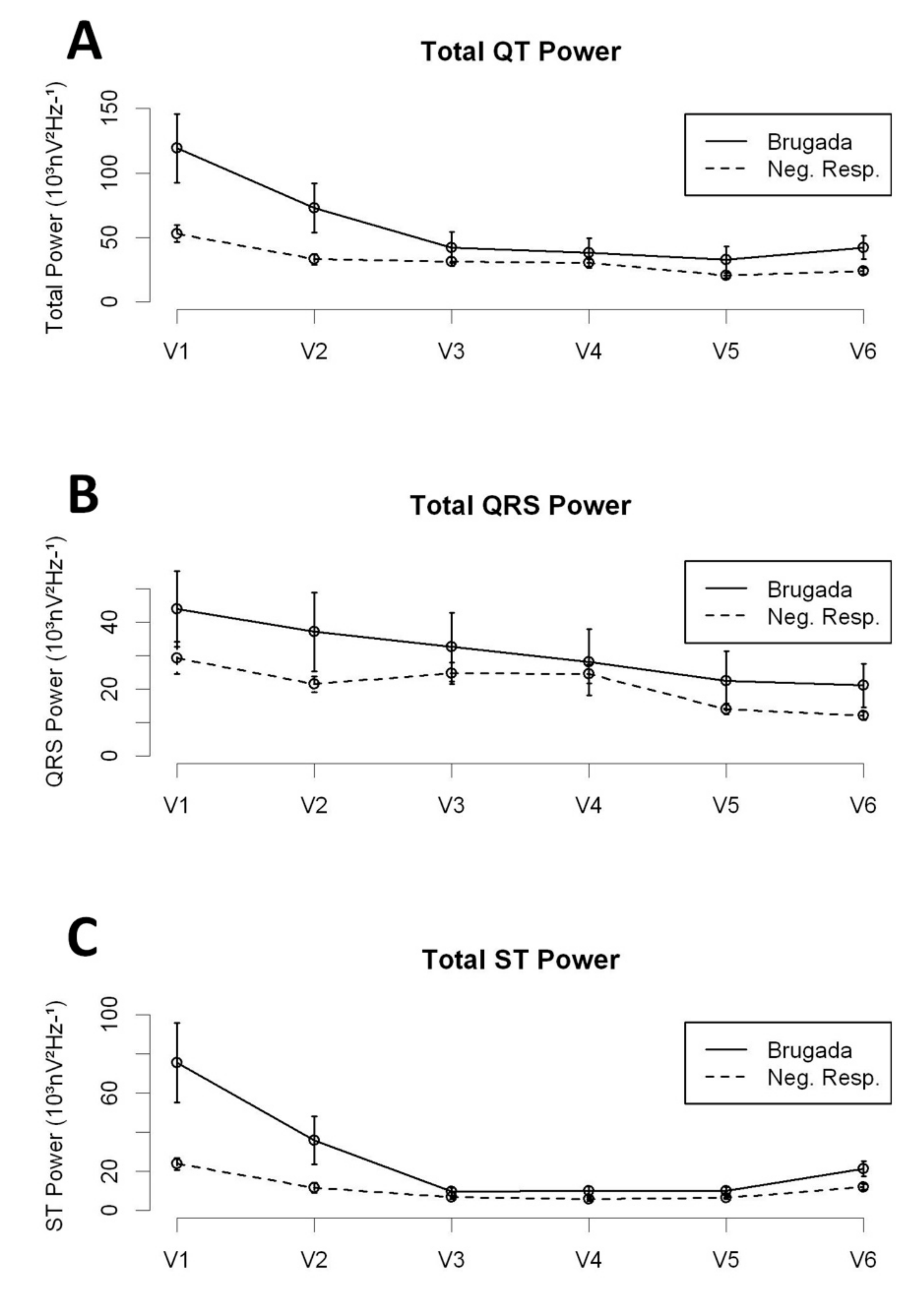
3.2. The High-Frequency Content along the QT Interval
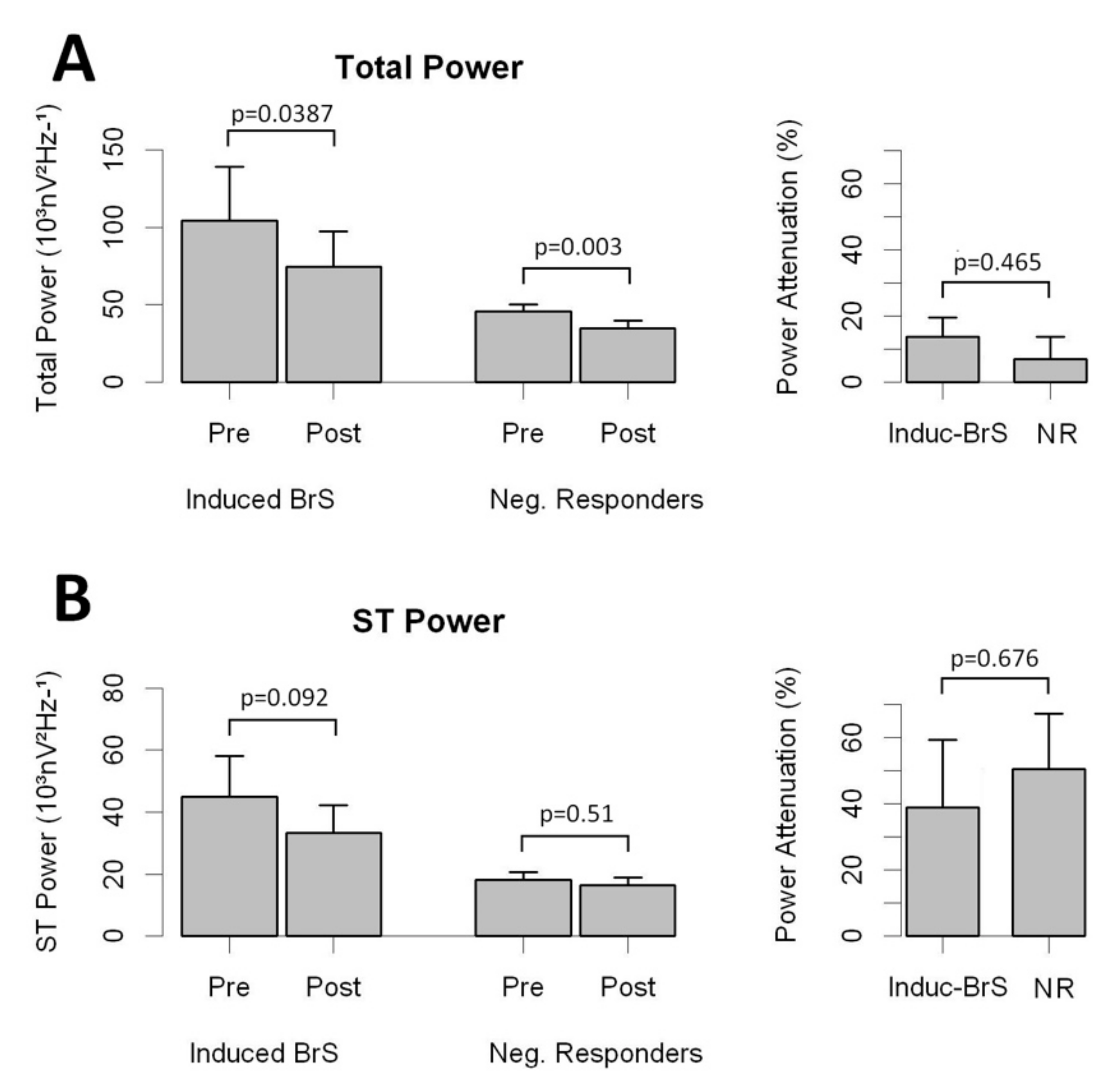
3.3. Drug Challenge and the High-Frequency Content
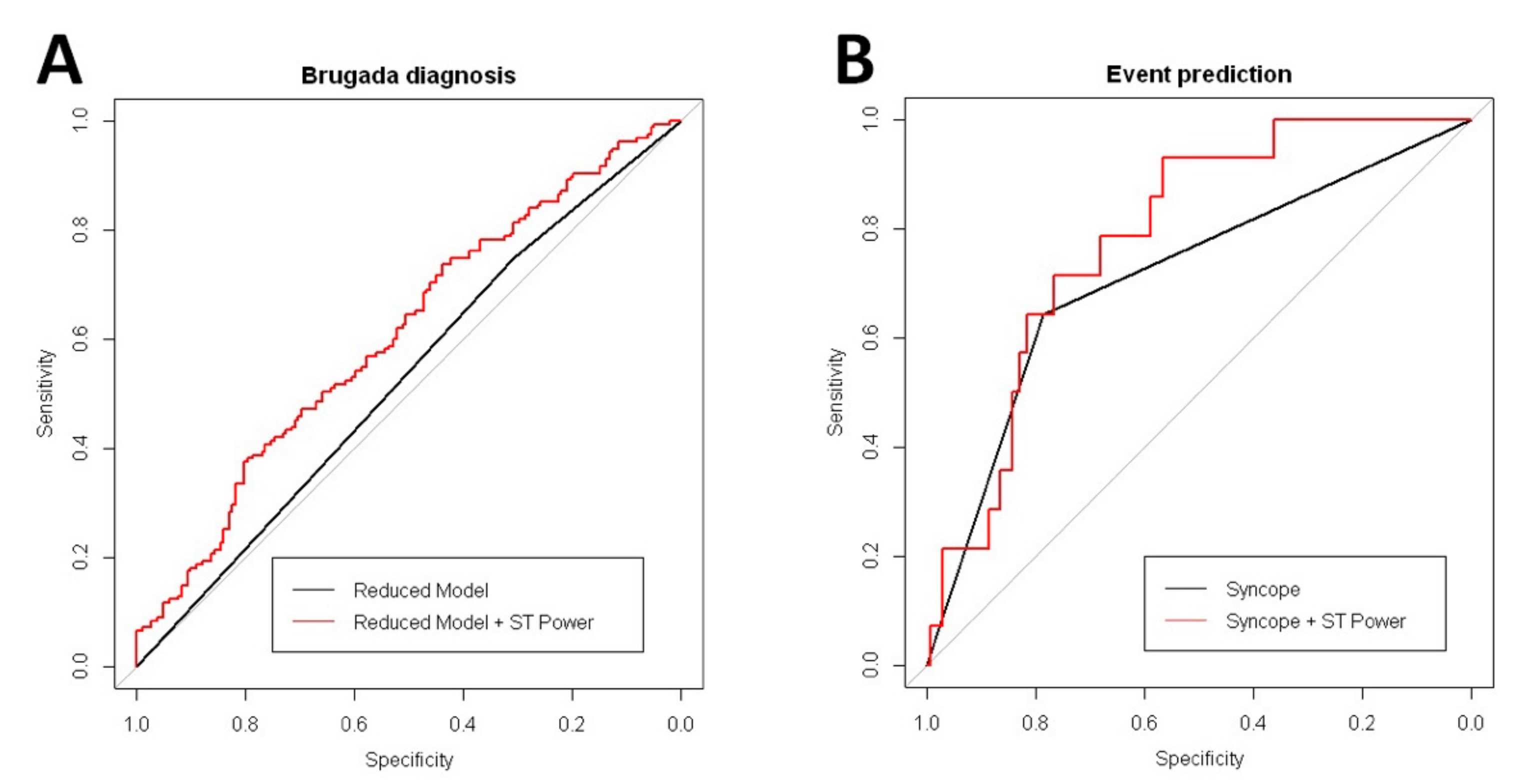
3.4. Prediction of Clinical Events During Follow-Up in Patients with Brugada Syndrome
4. Discussion
4.1. The Plausible Link between the High-Frequency Content and the Arrhythmogenic Substrate
4.2. The High-Frequency Content and Patient Prognosis in BrS
5. Limitations
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Antzelevitch, C.; Yan, G.-X.; Ackerman, M.J.; Borggrefe, M.; Corrado, D.; Guo, J.; Gussak, I.; Hasdemir, C.; Horie, M.; Huikuri, H.; et al. J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Europace 2017, 19, 665–694. [Google Scholar] [PubMed]
- Pablo Flórez, J.; García, D.; Valverde, I.; Rubín, J.; Pérez, D.; González-Vasserot, M.; Reguero, J.; María de la Hera, J.; Avanzas, P.; Gómez, J.; et al. Role of syncope in predicting adverse outcomes in patients with suspected Brugada syndrome undergoing standardized flecainide testing. EP Europace 2018, 20, f64–f71. [Google Scholar] [CrossRef] [PubMed]
- Veltmann, C.; Schimpf, R.; Echternach, C.; Eckardt, L.; Kuschyk, J.; Streitner, F.; Spehl, S.; Borggrefe, M.; Wolpert, C. A prospective study on spontaneous fluctuations between diagnostic and non-diagnostic ECGs in Brugada syndrome: Implications for correct phenotyping and risk stratification. Eur. Heart J. 2006, 27, 2544–2552. [Google Scholar] [CrossRef]
- García Iglesias, D.; Roqueñi Gutiérrez, N.; de Cos, J.F.; Calvo, D. Analysis of the High-Frequency Content in Human QRS Complexes by the Continuous Wavelet Transform: An Automatized Analysis for the Prediction of Sudden Cardiac Death. Sensors 2018, 18, 560. [Google Scholar] [CrossRef] [PubMed]
- Antzelevitch, C.; Brugada, P.; Borggrefe, M.; Brugada, J.; Brugada, R.; Corrado, D.; Shimizu, W. Brugada Syndrome: Report of the Second Consensus Conference. Circulation 2005, 111, 659–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo, D.; Rubín, J.M.; Pérez, D.; Gómez, J.; Flórez, J.P.; Avanzas, P.; García-Ruíz, J.M.; de la Hera, J.M.; Reguero, J.; Coto, E.; et al. Time-dependent responses to provocative testing with flecainide in the diagnosis of Brugada syndrome. Heart Rhythm 2015, 12, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Roesch, A.; Schmidbauer, H. WaveletComp: A Guided Tour through the R-Package. Available online: https://www.hs-stat.com/projects/WaveletComp/WaveletCom_guided_tour.pdf (accessed on 15 January 2019).
- Fishman, G.I.; Chugh, S.S.; Dimarco, J.P.; Albert, C.M.; Anderson, M.E.; Bonow, R.O.; Buxton, A.E.; Chen, P.S.; Estes, M.; Jouven, X.; et al. Sudden cardiac death prediction and prevention: Report from a national heart, lung, and blood institute and heart rhythm society workshop. Circulation 2010, 122, 2335–2348. [Google Scholar] [CrossRef]
- Priori, S.G.; Wilde, A.A.; Horie, M.; Cho, Y.; Behr, E.R.; Berul, C.; Blom, N.; Brugada, J.; Chiang, C.-E.; Huikuri, H.; et al. Executive summary: HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. Heart Rhythm 2013, 10, 1932–1963. [Google Scholar] [CrossRef]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.-C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martín, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef]
- Nademanee, K.; Veerakul, G.; Chandanamattha, P.; Chaothawee, L.; Ariyachaipanich, A.; Jirasirirojanakorn, K.; Likittanasombat, K.; Bhuripanyo, K.; Ngarmukos, T. Prevention of ventricular fibrillation episodes in Brugada syndrome by catheter ablation over the anterior right ventricular outflow tract epicardium. Circulation 2011, 123, 1270–1279. [Google Scholar] [CrossRef]
- Pappone, C.; Ciconte, G.; Manguso, F.; Vicedomini, G.; Mecarocci, V.; Conti, M.; Giannelli, L.; Pozzi, P.; Borrelli, V.; Menicanti, L.; et al. Assessing the Malignant Ventricular Arrhythmic Substrate in Patients With Brugada Syndrome. J. Am. Coll. Cardiol. 2018, 71, 1631–1646. [Google Scholar] [CrossRef] [PubMed]
- Gramatikov, B.; Brinker, J.; Yi-Chun, S.; Thakor, N.V. Wavelet analysis and time-frequency distributions of the body surface ECG before and after angioplasty. Comput. Methods Programs Biomedi. 2000, 62, 87–98. [Google Scholar] [CrossRef]
- Gramatikov, B.; Iyer, V. Intra-QRS spectral changes accompany ST segment changes during episodes of myocardial ischemia. J. Electrocardiol. 2015, 48, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Vassilikos, V.P.; Mantziari, L.; Dakos, G.; Kamperidis, V.; Chouvarda, I.; Chatzizisis, Y.S.; Kalpidis, P.; Theofilogiannakos, E.; Paraskevaidis, S.; Karvounis, H.; et al. QRS analysis using wavelet transformation for the prediction of response to cardiac resynchronization therapy: A prospective pilot study. J. Electrocardiol. 2014, 47, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Magrans, R.; Gomis, P.; Voss, A.; Caminal, P. Effect of acute myocardial ischemia on different high-frequency bandwidths and temporal regions of the QRS. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2011, 2011, 7083–7086. [Google Scholar]
- Huang, Z.; Patel, C.; Li, W.; Xie, Q.; Wu, R.; Zhang, L.; Tang, R.; Wan, X.; Ma, Y.; Zhen, W.; et al. Role of signal-averaged electrocardiograms in arrhythmic risk stratification of patients with Brugada syndrome: A prospective study. Heart Rhythm 2009, 6, 1156–1162. [Google Scholar] [CrossRef] [PubMed]
- Kakihara, J.; Takagi, M.; Hayashi, Y.; Tatsumi, H.; Doi, A.; Yoshiyama, M. Utility of 12-lead and signal-averaged Holter electrocardiograms after pilsicainide provocation for risk stratification in Brugada syndrome. Heart Vessels 2017, 32, 1151–1159. [Google Scholar] [CrossRef]
- Tereshchenko, L.G.; Josephson, M.E. Frequency content and characteristics of ventricular conduction. Proc. J. Electrocardiol. 2015, 48, 933–937. [Google Scholar] [CrossRef] [Green Version]
- Calvo, D.; Flórez, J.P.; Valverde, I.; Rubín, J.; Pérez, D.; Vasserot, M.G.; Rodríguez-Reguero, J.; Avanzas, P.; de la Hera, J.M.; Gómez, J.; et al. Surveillance after cardiac arrest in patients with Brugada syndrome without an implantable defibrillator: An alarm effect of the previous syncope. Int. J. Cardiol. 2016, 218, 69–74. [Google Scholar] [CrossRef]
- Zorzi, A.; Migliore, F.; Marras, E.; Marinelli, A.; Baritussio, A.; Allocca, G.; Leoni, L.; Perazzolo Marra, M.; Basso, C.; Buja, G.; et al. Should all individuals with a nondiagnostic Brugada-electrocardiogram undergo sodium-channel blocker test? Heart Rhythm 2012, 9, 909–916. [Google Scholar] [CrossRef]
- Letsas, K.P.; Asvestas, D.; Baranchuk, A.; Liu, T.; Georgopoulos, S.; Efremidis, M.; Korantzopoulos, P.; Bazoukis, G.; Tse, G.; Sideris, A.; et al. Prognosis, risk stratification, and management of asymptomatic individuals with Brugada syndrome: A systematic review. Pacing Clin. Electrophysiol. 2017, 40, 1332–1345. [Google Scholar] [CrossRef] [PubMed]
- Raju, H.; Papadakis, M.; Govindan, M.; Bastiaenen, R.; Chandra, N.; O’Sullivan, A.; Baines, G.; Sharma, S.; Behr, E.R. Low Prevalence of Risk Markers in Cases of Sudden Death Due to Brugada Syndrome. J. Am. Coll. Cardiol. 2011, 57, 2340. [Google Scholar] [CrossRef] [PubMed]
- Sacher, F.; Probst, V.; Maury, P.; Babuty, D.; Mansourati, J.; Komatsu, Y.; Loizeau, C. Outcome After Implantation of a Cardioverter-Defibrillator in Patients With Brugada Syndrome. Circulation 2013, 128, 1739–1747. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spont-BrS (N = 43) | Induc-BrS (N = 112) | NR Patients (N = 182) | p Value | |
|---|---|---|---|---|
| Clinical features | ||||
| Age (years) | 44.05 (12.3) | 43.61 (14.51) | 38.64 (14.98) | 0.004 |
| Male gender (%) | 30 (90.7) | 70 (62.5) | 137 (75.28) | 0.001 |
| Family history of SCD at age <45 years (%) | 18 (41.86) | 68 (60.71) | 73 (40.11) | 0.002 |
| Syncope (%) | 11 (25.58) | 28 (25) | 56 (30.77) | 0.521 |
| Cardiac syncope (%) | 7 (16.28) | 12 (10.71) | 5 (2.75) | 0.002 |
| SCA (%) | 5 (11.63) | 9 (8.04) | 1 (0.549) | 0.001 |
| Smoker (%) | 12 (27.9) | 29 (25.89) | 47 (25.82) | 0.96 |
| Hypertension (%) | 7 (16.28) | 18 (16.07) | 21 (11.54) | 0.473 |
| Diabetes mellitus (%) | 1 (2.33) | 4 (3.57) | 3 (1.65) | 0.575 |
| Dyslipidemia (%) | 8 (18.61) | 22 (19.64) | 14 (7.69) | 0.007 |
| Cardiomyopathy (%) † | 3 (6.98) | 3 (2.68) | 9 (4.95) | 0.455 |
| Cardiovascular drugs (%) ‡ | 11 (25.58) | 18 (16.07) | 23 (12.64) | 0.104 |
| PES Test performed | 26 (60.47) | 37 (33.04) | 3 (1.65) | <0.001 |
| Positive PES | 8 (18.6) | 4 (3.57) | 0 (0) | <0.001 |
| ICD implanted | 22 (51.16) | 23 (20.54) | 2 (1.1) | <0.001 |
| ECG pattern at the time of the digital record | ||||
| BrS type I (%) | 38 (88.37) | 0 | 0 | <0.001 |
| BrS type II (%) | 3 (6.98) | 59 (52.68) | 36 (19.78) | <0.001 |
| BrS type III (%) | 0 | 22 (19.64) | 39 (21.43) | 0.004 |
| BrS type II–III (%) | 3 (6.98) | 81 (72.62) | 75 (41.21) | <0.001 |
| Normal (%) | 0 | 25 (22.32) | 75 (41.21 | <0.001 |
| Spont-BrS | Induct-BrS | NR Patients | p Value | |
|---|---|---|---|---|
| All precordial leads | ||||
| Peak Power | 0.734 (0.616–0.852) | 1.439 (0.916–1.962) | 0.871 (0.786–0.956) | 0.677 |
| Total Power | 46.693 (34.811–58.575) | 62.188 (46.143–78.233) | 32.161 (29.752–34.57) | 0.095 |
| Total QRS Power | 18.567 (15.884–21.25) | 35.553 (22.559–48.547) | 21.031 (19.119–22.943) | 0.623 |
| Total ST Power | 28.126 (17.793–38.459) | 26.635 (21.19–32.08) | 11.13 (10.009–12.251) | 0.002 |
| QRS to ST Total Power | 5.256 (3.947–6.565) | 5.762 (4.931–6.593) | 9.724 (8.075–11.373) | 0.045 |
| Right precordial leads | ||||
| Peak Power | 0.897 (0.74–1.054) | 1.705 (1.127–2.283) | 0.917 (0.801–1.033) | 0.468 |
| Total Power | 84.216 (52.704–115.728) | 100.581 (77.381–123.781) | 43.111 (38.832–47.39) | 0.017 |
| Total QRS Power | 25.48 (21.46–29.5) | 46.147 (30.805–61.489) | 25.35 (22.267–28.433) | 0.451 |
| Total ST Power | 58.736 (30.649–86.823) | 54.434 (40.921–67.947) | 17.761 (15.586–19.936) | 0.003 |
| QRS to ST Total Power | 4.142 (3.075–5.209) | 4.06 (3.445–4.675) | 6.023 (5.067–6.979) | 0.133 |
| ECG Type I | ECG Type II or III | |||
|---|---|---|---|---|
| BrS Patients | BrS Patients | NR Patients | p | |
| All precordial leads | ||||
| Peak Power | 0.629 (0.421–0.836) | 1.518 (0.186–2.85) | 1.07 (0.762–1.379) | 0.517 |
| Total Power | 47.415 (20.269–74.561) | 69.721 (28.191–111.251) | 36.259 (27.264–45.253) | 0.121 |
| Total QRS Power | 16.665 (11.358–21.972) | 38.651 (5.058–72.244) | 25.458 (18.461–32.455) | 0.446 |
| Total ST Power | 30.75 (7.171–54.329) | 31.07 (16.856–45.283) | 10.8 (7.248–14.352) | 0.007 |
| QRS to ST Total Power | 3.849 (2.131–5.566) | 5.853 (3.926–7.779) | 12.132 (6.002–18.262) | 0.055 |
| Right precordial leads | ||||
| Peak Power | 0.886 (0.529–1.244) | 1.948 (0.43–3.466) | 1.209 (0.771–1.647) | 0.355 |
| Total Power | 89.832 (17.724–161.941) | 120.243 (59.55–180.936) | 51.683 (35.198–68.167) | 0.033 |
| Total QRS Power | 25.041 (15.957–34.126) | 53.695 (13.362–94.027) | 32.757 (20.998–44.516) | 0.324 |
| Total ST Power | 64.791 (0.574–129.008) | 66.549 (31.128–101.969) | 18.926 (11.609–26.242) | 0.01 |
| QRS to ST Total Power | 3.471 (1.768–5.173) | 4.284 (2.783–5.785) | 7.666 (3.581–11.751) | 0.125 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR | p | HR | p | |
| Model for prediction of positive response to the drug challenge | ||||
| Peak Power | 3.251 (0.8–13.209) | 0.099 | ||
| Total Power | 1.054 (1.019–1.091) | 0.003 | ||
| Total QRS Power | 1.045 (0.991–1.102) | 0.101 | ||
| Total ST Power | 1.106 (1.043–1.174) | 0.001 | 1.251 (1.082–1.447) | 0.003 |
| QRS to ST Total Power ratio | 0.678 (0.407–1.13) | 0.136 | ||
| Age | 1.005 (1.002–1.009) | 0.006 | 1.005 (1.001–1.008) | 0.014 |
| Male | 0.865 (0.766–0.977) | 0.02 | 0.925 (0.814–1.05) | 0.225 |
| Familiar History of SCD | 1.215 (1.089–1.356) | 0.001 | ||
| Familiar History of BrS | 1.203 (1.066–1.358) | 0.003 | 1.158 (1.019–1.317) | 0.025 |
| Syncope | 0.936 (0.827–1.059) | 0.289 | 0.914 (0.81–1.032) | 0.146 |
| Model for prediction of arrhythmic events during follow-up | ||||
| Peak Power | 0.997 (0.414–2.398) | 0.994 | ||
| Total Power | 1.011 (0.991–1.031) | 0.285 | ||
| Total QRS Power | 0.999 (0.967–1.033) | 0.967 | ||
| Total ST Power | 1.025 (0.996–1.056) | 0.096 | 1.041 (0.966–1.123) | 0.291 |
| QRS to ST Total Power ratio | 0.536 (0.27–1.065) | 0.075 | ||
| Age | 1 (0.997–1.003) | 0.905 | ||
| Spontaneous Type I Pattern | 1.037 (0.936–1.148) | 0.488 | 1.026 (0.923–1.141) | 0.629 |
| Male | 1.036 (0.938–1.145) | 0.482 | 1.041 (0.939–1.155) | 0.441 |
| Familiar History of SCD | 0.955 (0.871–1.047) | 0.322 | 0.951 (0.869–1.041) | 0.278 |
| Familiar History of BrS | 0.928 (0.842–1.023) | 0.133 | ||
| Syncope | 1.206 (1.09–1.335) | <0.001 | 1.197 (1.079–1.329) | 0.001 |
| Positive PES | 0.907 (0.765–1.075) | 0.259 | 0.898 (0.756–1.067) | 0.219 |
| SCN5a Mutation | 0.96 (0.86–1.073) | 0.472 | 0.975 (0.873–1.089) | 0.652 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Iglesias, D.; de Cos, F.J.; Romero, F.J.; Polana, S.; Rubín, J.M.; Pérez, D.; Reguero, J.; de la Hera, J.M.; Avanzas, P.; Gómez, J.; et al. Spectral Analysis of the QT Interval Increases the Prediction Accuracy of Clinical Variables in Brugada Syndrome. J. Clin. Med. 2019, 8, 1629. https://doi.org/10.3390/jcm8101629
García-Iglesias D, de Cos FJ, Romero FJ, Polana S, Rubín JM, Pérez D, Reguero J, de la Hera JM, Avanzas P, Gómez J, et al. Spectral Analysis of the QT Interval Increases the Prediction Accuracy of Clinical Variables in Brugada Syndrome. Journal of Clinical Medicine. 2019; 8(10):1629. https://doi.org/10.3390/jcm8101629
Chicago/Turabian StyleGarcía-Iglesias, Daniel, Francisco Javier de Cos, Francisco Javier Romero, Srujana Polana, José Manuel Rubín, Diego Pérez, Julián Reguero, Jesús María de la Hera, Pablo Avanzas, Juan Gómez, and et al. 2019. "Spectral Analysis of the QT Interval Increases the Prediction Accuracy of Clinical Variables in Brugada Syndrome" Journal of Clinical Medicine 8, no. 10: 1629. https://doi.org/10.3390/jcm8101629
APA StyleGarcía-Iglesias, D., de Cos, F. J., Romero, F. J., Polana, S., Rubín, J. M., Pérez, D., Reguero, J., de la Hera, J. M., Avanzas, P., Gómez, J., Coto, E., Morís, C., & Calvo, D. (2019). Spectral Analysis of the QT Interval Increases the Prediction Accuracy of Clinical Variables in Brugada Syndrome. Journal of Clinical Medicine, 8(10), 1629. https://doi.org/10.3390/jcm8101629