High Betaine, a Trimethylamine N-Oxide Related Metabolite, Is Prospectively Associated with Low Future Risk of Type 2 Diabetes Mellitus in the PREVEND Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Methods
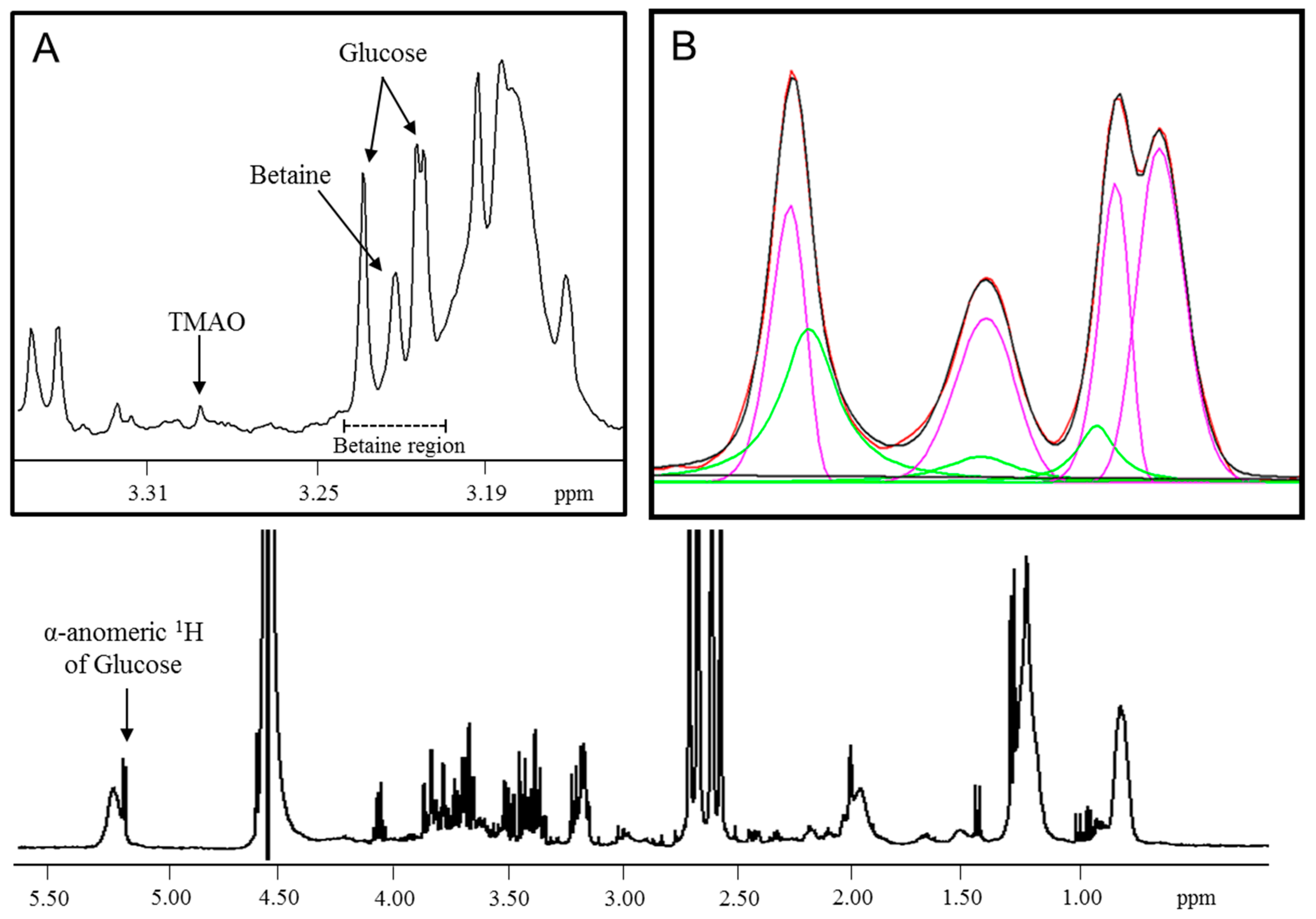
2.1. NMR Data Acquisition and Betaine Quantification by Peak Deconvolution
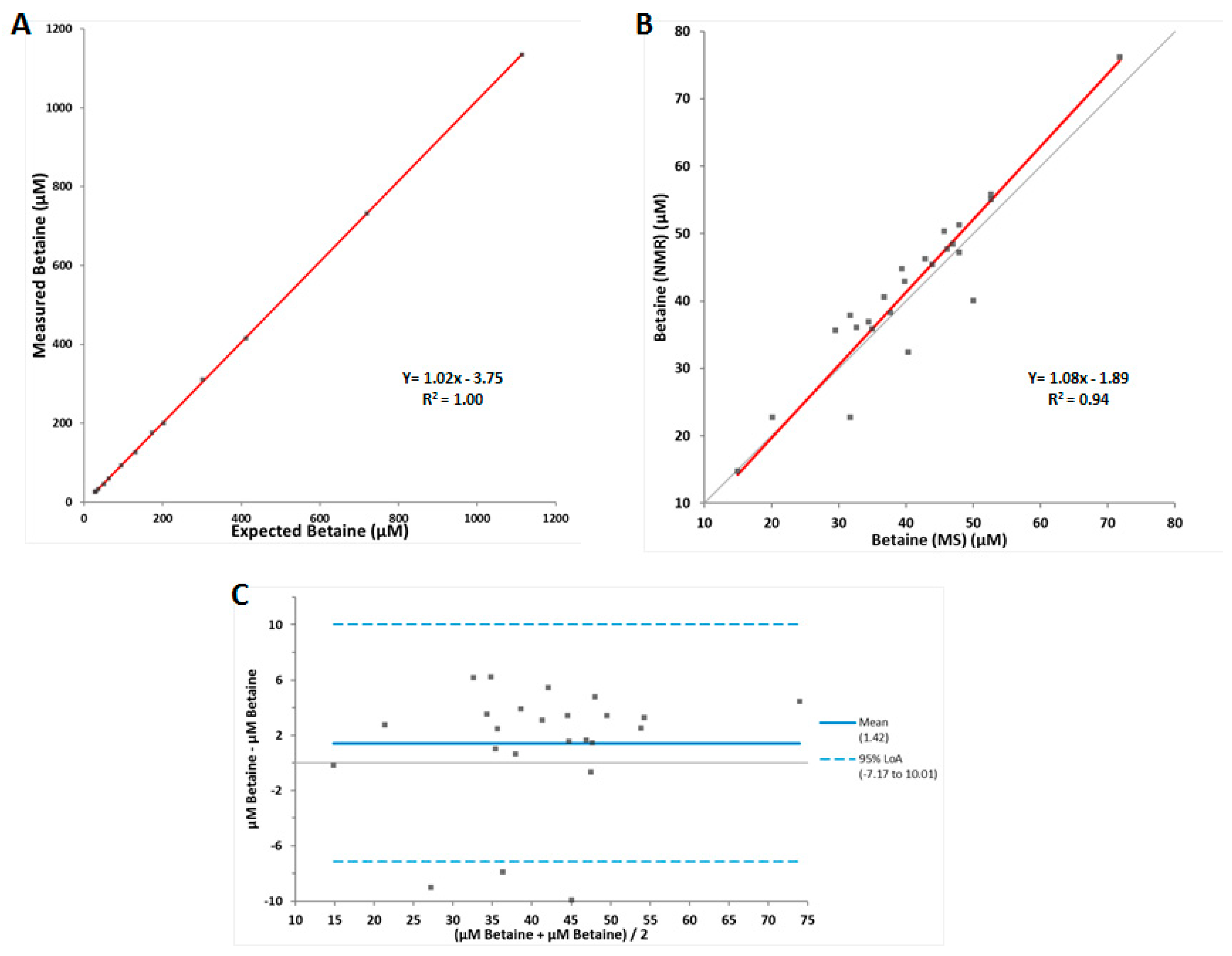
2.2. Assay Performance Testing
2.3. Cross-sectional and Prospective Analyses in Participants in the Prevention of Renal and Vascular End-Stage Disease (PREVEND) Study
2.4. Statistical Analyses
2.5. Ethic Approval and Consent to Participate
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lever, M.; Slow, S. The clinical significance of betaine, an osmolyte with a key role in methyl group metabolism. Clin. Biochem. 2010, 43, 732–744. [Google Scholar] [CrossRef] [PubMed]
- Day, C.R.; Kempson, S.A. Betaine chemistry, roles, and potential use in liver disease. Biochim. Biophys. Acta 2016, 1860, 1098–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sookoian, S.; Puri, P.; Castano, G.O.; Scian, R.; Mirshahi, F.; Sanyal, A.J.; Pirola, C.J. Nonalcoholic steatohepatitis is associated with a state of betaine-insufficiency. Liver Int. 2017, 37, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Dullaart, R.P.; Garcia, E.; Jeyarajah, E.; Gruppen, E.G.; Connelly, M.A. Plasma phospholipid transfer protein activity is inversely associated with betaine in diabetic and non-diabetic subjects. Lipids Health Dis. 2016, 15, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstantinova, S.V.; Tell, G.S.; Vollset, S.E.; Nygard, O.; Bleie, O.; Ueland, P.M. Divergent associations of plasma choline and betaine with components of metabolic syndrome in middle age and elderly men and women. J. Nutr. 2008, 138, 914–920. [Google Scholar] [CrossRef]
- Walford, G.A.; Ma, Y.; Clish, C.; Florez, J.C.; Wang, T.J.; Gerszten, R.E.; Diabetes Prevention Program Research Group. Metabolite Profiles of Diabetes Incidence and Intervention Response in the Diabetes Prevention Program. Diabetes 2016, 65, 1424–1433. [Google Scholar] [CrossRef] [Green Version]
- Svingen, G.F.; Schartum-Hansen, H.; Pedersen, E.R.; Ueland, P.M.; Tell, G.S.; Mellgren, G.; Njolstad, P.R.; Seifert, R.; Strand, E.; Karlsson, T.; et al. Prospective Associations of Systemic and Urinary Choline Metabolites with Incident Type 2 Diabetes. Clin. Chem. 2016, 62, 755–765. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.M.; Liu, Y.; Zhou, R.F.; Chen, X.L.; Wang, C.; Tan, X.Y.; Wang, L.J.; Zheng, R.D.; Zhang, H.W.; Ling, W.H.; et al. Associations of gut-flora-dependent metabolite trimethylamine-N-oxide, betaine and choline with non-alcoholic fatty liver disease in adults. Sci. Rep. 2016, 6, 19076. [Google Scholar] [CrossRef]
- Konstantinova, S.V.; Tell, G.S.; Vollset, S.E.; Ulvik, A.; Drevon, C.A.; Ueland, P.M. Dietary patterns, food groups, and nutrients as predictors of plasma choline and betaine in middle-aged and elderly men and women. Am. J. Clin. Nutr. 2008, 88, 1663–1669. [Google Scholar] [CrossRef]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; Dugar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Koeth, R.A.; Wang, Z.; Levison, B.S.; Buffa, J.A.; Org, E.; Sheehy, B.T.; Britt, E.B.; Fu, X.; Wu, Y.; Li, L.; et al. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat. Med. 2013. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.; Wang, Z.; Levison, B.S.; Koeth, R.A.; Britt, E.B.; Fu, X.; Wu, Y.; Hazen, S.L. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N. Engl. J. Med. 2013, 368, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- Bennett, B.J.; de Aguiar Vallim, T.Q.; Wang, Z.; Shih, D.M.; Meng, Y.; Gregory, J.; Allayee, H.; Lee, R.; Graham, M.; Crooke, R.; et al. Trimethylamine-N-oxide, a metabolite associated with atherosclerosis, exhibits complex genetic and dietary regulation. Cell Metab. 2013, 17, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Tang, W.H.; Buffa, J.A.; Fu, X.; Britt, E.B.; Koeth, R.A.; Levison, B.S.; Fan, Y.; Wu, Y.; Hazen, S.L. Prognostic value of choline and betaine depends on intestinal microbiota-generated metabolite trimethylamine-N-oxide. Eur. Heart J. 2014, 35, 904–910. [Google Scholar] [CrossRef]
- Zhu, W.; Gregory, J.C.; Org, E.; Buffa, J.A.; Gupta, N.; Wang, Z.; Li, L.; Fu, X.; Wu, Y.; Mehrabian, M.; et al. Gut Microbial Metabolite TMAO Enhances Platelet Hyperreactivity and Thrombosis Risk. Cell 2016, 165, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Senthong, V.; Li, X.S.; Hudec, T.; Coughlin, J.; Wu, Y.; Levison, B.; Wang, Z.; Hazen, S.L.; Tang, W.H. Plasma Trimethylamine N-Oxide, a Gut Microbe-Generated Phosphatidylcholine Metabolite, Is Associated With Atherosclerotic Burden. J. Am. Coll. Cardiol. 2016, 67, 2620–2628. [Google Scholar] [CrossRef]
- Senthong, V.; Wang, Z.; Fan, Y.; Wu, Y.; Hazen, S.L.; Tang, W.H. Trimethylamine N-Oxide and Mortality Risk in Patients With Peripheral Artery Disease. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef]
- Senthong, V.; Wang, Z.; Li, X.S.; Fan, Y.; Wu, Y.; Tang, W.H.; Hazen, S.L. Intestinal Microbiota-Generated Metabolite Trimethylamine-N-Oxide and 5-Year Mortality Risk in Stable Coronary Artery Disease: The Contributory Role of Intestinal Microbiota in a COURAGE-Like Patient Cohort. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef]
- Suzuki, T.; Heaney, L.M.; Bhandari, S.S.; Jones, D.J.; Ng, L.L. Trimethylamine N-oxide and prognosis in acute heart failure. Heart 2016, 102, 841–848. [Google Scholar] [CrossRef]
- Tang, W.H.; Wang, Z.; Li, X.S.; Fan, Y.; Li, D.S.; Wu, Y.; Hazen, S.L. Increased Trimethylamine N-Oxide Portends High Mortality Risk Independent of Glycemic Control in Patients with Type 2 Diabetes Mellitus. Clin. Chem. 2017, 63, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Gruppen, E.G.; Garcia, E.; Connelly, M.A.; Jeyarajah, E.J.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F. TMAO is Associated with Mortality: Impact of Modestly Impaired Renal Function. Sci. Rep. 2017, 7, 13781. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.W.; Backhed, F.; Landmesser, U.; Hazen, S.L. Intestinal Microbiota in Cardiovascular Health and Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2089–2105. [Google Scholar] [CrossRef] [PubMed]
- Lever, M.; George, P.M.; Elmslie, J.L.; Atkinson, W.; Slow, S.; Molyneux, S.L.; Troughton, R.W.; Richards, A.M.; Frampton, C.M.; Chambers, S.T. Betaine and secondary events in an acute coronary syndrome cohort. PLoS ONE 2012, 7, e37883. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.; Hazen, S.L. The contributory role of gut microbiota in cardiovascular disease. J. Clin. Investig. 2014, 124, 4204–4211. [Google Scholar] [CrossRef]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef]
- Wang, Z.; Zhao, Y. Gut microbiota derived metabolites in cardiovascular health and disease. Protein Cell 2018, 9, 416–431. [Google Scholar] [CrossRef] [Green Version]
- Lever, M.; George, P.M.; Slow, S.; Bellamy, D.; Young, J.M.; Ho, M.; McEntyre, C.J.; Elmslie, J.L.; Atkinson, W.; Molyneux, S.L.; et al. Betaine and Trimethylamine-N-Oxide as Predictors of Cardiovascular Outcomes Show Different Patterns in Diabetes Mellitus: An Observational Study. PLoS ONE 2014, 9, e114969. [Google Scholar] [CrossRef]
- Papandreou, C.; Bullo, M.; Zheng, Y.; Ruiz-Canela, M.; Yu, E.; Guasch-Ferre, M.; Toledo, E.; Clish, C.; Corella, D.; Estruch, R.; et al. Plasma trimethylamine-N-oxide and related metabolites are associated with type 2 diabetes risk in the Prevencion con Dieta Mediterranea (PREDIMED) trial. Am. J. Clin. Nutr. 2018, 108, 163–173. [Google Scholar] [CrossRef]
- Garcia, E.; Wolak-Dinsmore, J.; Wang, Z.; Li, X.S.; Bennett, D.W.; Connelly, M.A.; Otvos, J.D.; Hazen, S.L.; Jeyarajah, E.J. NMR quantification of trimethylamine-N-oxide in human serum and plasma in the clinical laboratory setting. Clin. Biochem. 2017, 50, 947–955. [Google Scholar] [CrossRef]
- Matyus, S.P.; Braun, P.J.; Wolak-Dinsmore, J.; Jeyarajah, E.J.; Shalaurova, I.; Xu, Y.; Warner, S.M.; Clement, T.S.; Connelly, M.A.; Fischer, T.J. NMR measurement of LDL particle number using the Vantera Clinical Analyzer. Clin. Biochem. 2014, 47, 203–210. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. CLSI Document EP9-A2: Method Comaprison and Bias Estimation Using Patient Samples; Approved Guideline, 2nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2002. [Google Scholar]
- Wang, Z.; Levison, B.S.; Hazen, J.E.; Donahue, L.; Li, X.M.; Hazen, S.L. Measurement of trimethylamine-N-oxide by stable isotope dilution liquid chromatography tandem mass spectrometry. Anal. Biochem. 2014, 455C, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Koeth, R.A.; Lam-Galvez, B.R.; Kirsop, J.; Wang, Z.; Levison, B.S.; Gu, X.; Copeland, M.F.; Bartlett, D.; Cody, D.B.; Dai, H.J.; et al. l-Carnitine in omnivorous diets induces an atherogenic gut microbial pathway in humans. J. Clin. Investig. 2019, 129, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Lambers Heerspink, H.J.; Brantsma, A.H.; de Zeeuw, D.; Bakker, S.J.; de Jong, P.E.; Gansevoort, R.T.; Group, P.S. Albuminuria assessed from first-morning-void urine samples versus 24-hour urine collections as a predictor of cardiovascular morbidity and mortality. Am. J. Epidemiol. 2008, 168, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.; Corpeleijn, E.; Postmus, D.; Gansevoort, R.T.; de Jong, P.E.; Gans, R.O.; Struck, J.; Hillege, H.L.; Stolk, R.P.; Navis, G.; et al. Plasma procalcitonin and risk of type 2 diabetes in the general population. Diabetologia 2011, 54, 2463–2465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef]
- Gruppen, E.G.; Connelly, M.A.; Sluiter, W.J.; Bakker, S.J.L.; Dullaart, R.P.F. Higher plasma GlycA, a novel pro-inflammatory glycoprotein biomarker, is associated with reduced life expectancy: The PREVEND study. Clin. Chim. Acta 2019, 488, 7–12. [Google Scholar] [CrossRef]
- Corsetti, J.P.; Bakker, S.J.; Sparks, C.E.; Dullaart, R.P. Apolipoprotein A-II influences apolipoprotein E-linked cardiovascular disease risk in women with high levels of HDL cholesterol and C-reactive protein. PLoS ONE 2012, 7, e39110. [Google Scholar] [CrossRef]
- Laryea, M.D.; Steinhagen, F.; Pawliczek, S.; Wendel, U. Simple method for the routine determination of betaine and N,N-dimethylglycine in blood and urine. Clin. Chem. 1998, 44, 1937–1941. [Google Scholar] [Green Version]
- Awwad, H.M.; Kirsch, S.H.; Geisel, J.; Obeid, R. Measurement of concentrations of whole blood levels of choline, betaine, and dimethylglycine and their relations to plasma levels. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2014, 957, 41–45. [Google Scholar] [CrossRef]
- Shalaurova, I.; Connelly, M.A.; Garvey, W.T.; Otvos, J.D. Lipoprotein insulin resistance index: A lipoprotein particle-derived measure of insulin resistance. Metab. Syndr. Relat. Disord. 2014, 12, 422–429. [Google Scholar] [CrossRef]
- Matyus, S.P.; Braun, P.J.; Wolak-Dinsmore, J.; Saenger, A.K.; Jeyarajah, E.J.; Shalaurova, I.; Warner, S.M.; Fischer, T.J.; Connelly, M.A. HDL particle number measured on the Vantera(R), the first clinical NMR analyzer. Clin. Biochem. 2015, 48, 148–155. [Google Scholar] [CrossRef]
- Otvos, J.D.; Shalaurova, I.; Wolak-Dinsmore, J.; Connelly, M.A.; Mackey, R.H.; Stein, J.H.; Tracy, R.P. GlycA: A Composite Nuclear Magnetic Resonance Biomarker of Systemic Inflammation. Clin. Chem. 2015, 61, 714–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolak-Dinsmore, J.; Gruppen, E.G.; Shalaurova, I.; Matyus, S.P.; Grant, R.P.; Gegen, R.; Bakker, S.J.L.; Otvos, J.D.; Connelly, M.A.; Dullaart, R.P.F. A novel NMR-based assay to measure circulating concentrations of branched-chain amino acids: Elevation in subjects with type 2 diabetes mellitus and association with carotid intima media thickness. Clin. Biochem. 2018, 54, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Li, X.S.; Wang, Z.; Cajka, T.; Buffa, J.A.; Nemet, I.; Hurd, A.G.; Gu, X.; Skye, S.M.; Roberts, A.B.; Wu, Y.; et al. Untargeted metabolomics identifies trimethyllysine, a TMAO-producing nutrient precursor, as a predictor of incident cardiovascular disease risk. J. Clin. Investig. Insight 2018, 3, e99096. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.; Hazen, S.L. Microbiome, trimethylamine N-oxide, and cardiometabolic disease. Transl. Res. 2017, 179, 108–115. [Google Scholar] [CrossRef]
- Org, E.; Blum, Y.; Kasela, S.; Mehrabian, M.; Kuusisto, J.; Kangas, A.J.; Soininen, P.; Wang, Z.; Ala-Korpela, M.; Hazen, S.L.; et al. Relationships between gut microbiota, plasma metabolites, and metabolic syndrome traits in the METSIM cohort. Genome Biol. 2017, 18, 70. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Imprecision | Betaine (µM) | ||
|---|---|---|---|
| Low | Medium | High | |
| Within-lab a | |||
| Mean | 45.2 | 97.2 | 205.9 |
| SD | 2.5 | 4.0 | 5.2 |
| CV (%) | 5.5 | 4.1 | 2.5 |
| Within-run b | |||
| Mean | 44.1 | 95.6 | 205.6 |
| SD | 1.9 | 3.1 | 3.1 |
| CV (%) | 4.3 | 3.2 | 1.5 |
| Percentile | Normal Healthy Adult Volunteers (n = 501) | Normal Healthy Adult Volunteers Female (n = 292) | Normal Healthy Adult Volunteers Male (n = 209) | PREVEND Study Participants (n = 5621) |
|---|---|---|---|---|
| 0th | <13.2 a | <13.2 a | 24.6 | 13.3 |
| 2.5th | 23.8 | 22.0 | 28.5 | 21.0 |
| 25.0th | 34.1 | 32.4 | 37.3 | 30.8 |
| 50.0th | 41.0 | 39.1 | 44.6 | 36.8 |
| 75.0th | 49.5 | 46.9 | 52.4 | 43.8 |
| 97.5th | 74.7 | 74.4 | 75.3 | 63.0 |
| 100th | 104.1 | 101.6 | 104.1 | 190.7 |
| Mean (SD) | 42.9 (12.6) | 40.7 (12.4) | 46.0 (12.2) | 38.1 (11.2) |
| Overall | Tertiles of betaine | p-Value | |||
|---|---|---|---|---|---|
| T1 | T2 | T3 | |||
| Participants, n | 4336 | 1445 | 1446 | 1445 | |
| Betaine, µM | 36.9 (31.0–44.0) | 28.7 (25.3–31.0) | 36.9 (35.1–38.8) | 47.3 (44.0–52.6) | |
| Participants, n | 4236 | 1398 | 1418 | 1420 | |
| TMAO, µM | 4.6 ± 5.9 | 4.6 ± 5.1 | 4.7 ± 6.3 | 4.6 ± 6.4 | |
| General characteristics | |||||
| Age, years | 52.6 ± 11.5 | 51.3 ± 10.9 | 52.8 ± 11.4 | 53.7 ± 12.1 | <0.001 |
| Male sex, n (%) | 2159 (49.8) | 456 (31.6) | 750 (51.9) | 953 (66.0) | <0.001 |
| Ethnicity, Caucasian, n (%) | 4164 (96.0) | 1403 (97.1) | 1400 (96.8) | 1361 (94.2) | 0.001 |
| BMI, kg/m2 | 26.4 ± 4.2 | 26.7 ± 4.3 | 26.6 ± 4.2 | 26.0 ± 4.1 | <0.001 |
| Smoking status, n (%) | 0.008 | ||||
| Never | 1286 (29.7) | 420 (29.1) | 424 (29.3) | 442 (30.6) | |
| Former | 1828 (42.2) | 574 (39.7) | 639 (44.2) | 615 (42.6) | |
| Current | 1165 (26.9) | 438 (30.3) | 358 (24.8) | 369 (25.5) | |
| Alcohol consumption, never, n (%) | 1004 (23.2) | 329 (22.8) | 351 (24.3) | 324 (22.4) | 0.26 |
| eGFR, mL/min/1.73m2 | 93.5 ± 16.3 | 94.5 ± 15.9 | 93.1 ± 16.7 | 93.0 ± 16.3 | 0.02 |
| Hypertension, n (%) | 1280 (29.5) | 406 (28.1) | 443 (30.6) | 431 (29.8) | 0.33 |
| Hypercholesterolemia, n (%) | 1235 (28.5) | 468 (32.4) | 390 (27.0) | 377 (26.1) | <0.001 |
| Parental history of CKD, n (%) | 20 (0.5) | 8 (0.6) | 7 (0.5) | 5 (0.3) | 0.70 |
| Circulation | |||||
| SBP, mmHg | 124.8 ± 18.1 | 123.9 ± 17.8 | 125.4 ± 18.2 | 125.1 ± 18.3 | 0.06 |
| DBP, mmHg | 73.0 ± 9.0 | 72.5 ± 9.1 | 73.4 ± 8.8 | 72.3 ± 9.0 | 0.02 |
| Laboratory parameters | |||||
| Total cholesterol, mmol/L | 5.4 ± 1.0 | 5.6 ± 1.1 | 5.4 ± 1.0 | 5.2 ± 1.0 | <0.001 |
| HDL cholesterol, mmol/L | 1.3 ± 0.3 | 1.2 ± 0.3 | 1.3 ± 0.3 | 1.2 ± 0.3 | <0.001 |
| Triglycerides, mmol/L | 1.1 (0.8–1.6) | 1.2 (0.8–1.7) | 1.1 (0.8–1.6) | 1.0 (0.8–1.5) | 0.005 |
| Fasting glucose, mmol/L | 4.7 (4.4–5.2) | 4.7 (4.4–5.2) | 4.7 (4.4–5.2) | 4.7 (4.4–5.2) | 0.34 |
| C-reactive protein, mg/L | 1.2 (0.6–2.8) | 1.4 (0.6–3.0) | 1.2 (0.5–2.6) | 1.1 (0.5–2.8) | 0.005 |
| Medication | |||||
| Antihypertensive drugs, n (%) | 716 (16.5) | 221 (15.3) | 239 (16.5) | 256 (17.7) | 0.12 |
| Lipid lowering drug use, n (%) | 304 (7.0) | 62 (4.3) | 94 (6.5) | 148 (10.2) | <0.001 |
| Betaine as Continuous Variable (2log) | Tertiles of Betaine | ||||||
|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | |||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| Diabetes, no. of events (%) | 224 (5.2%) | 93 (6.4%) | 74 (5.1%) | 57 (3.9%) | |||
| Crude | 0.79 (0.59–1.05) | 0.10 | 1.00 (ref) | 0.78 (0.57–1.05) | 0.10 | 0.61 (0.44–0.85) | 0.004 |
| Model 1 | 0.60 (0.46–0.79) | <0.001 | 1.00 (ref) | 0.64 (0.47–0.88) | 0.005 | 0.45 (0.32–0.64) | <0.001 |
| Model 2 | 0.59 (0.45–0.78) | <0.001 | 1.00 (ref) | 0.61 (0.45–0.84) | 0.002 | 0.42 (0.29–0.59) | <0.001 |
| Model 3 | 0.63 (0.47–0.85) | 0.002 | 1.00 (ref) | 0.68 (0.50–0.94) | 0.02 | 0.47 (0.33–0.66) | <0.001 |
| Model 4 | 0.69 (0.46–1.02) | 0.06 | 1.00 (ref) | 0.65 (0.43–0.96) | 0.03 | 0.50 (0.32–0.80) | 0.004 |
| Betaine as Continuous Variable (2log) | Tertiles of Betaine | ||||||
|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | |||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| Men | |||||||
| Diabetes, no. of events (%) | 139 (6.4%) | 54 (2.5%) | 46 (2.1%) | 39 (1.8%) | |||
| Crude | 0.41 (0.26–0.64) | <0.001 | 1.00 (ref) | 0.49 (0.33–0.73) | <0.001 | 0.34 (0.22–0.51) | <0.001 |
| Model 1 | 0.40 (0.26–0.62) | <0.001 | 1.00 (ref) | 0.49 (0.33–0.72) | <0.001 | 0.32 (0.21–0.49) | <0.001 |
| Model 2 | 0.41 (0.26–0.65) | <0.001 | 1.00 (ref) | 0.46 (0.31–0.69) | <0.001 | 0.32 (0.21–0.48) | <0.001 |
| Model 3 | 0.56 (0.35–0.90) | 0.02 | 1.00 (ref) | 0.54 (0.36–0.82) | 0.003 | 0.43 (0.28–0.65) | <0.001 |
| Model 4 | 0.44 (0.24–0.80) | 0.007 | 1.00 (ref) | 0.43 (0.25–0.74) | 0.003 | 0.36 (0.20–0.65) | 0.001 |
| Women | |||||||
| Diabetes, no. of events (%) | 85 (3.9%) | 39 (1.8%) | 28 (1.3%) | 18 (0.8%) | |||
| Crude | 0.96 (0.59–1.53) | 0.85 | 1.00 (ref) | 1.01 (0.62–1.63) | 0.98 | 0.95 (0.54–1.66) | 0.86 |
| Model 1 | 0.81 (0.52–1.27) | 0.35 | 1.00 (ref) | 0.89 (0.55–1.45) | 0.65 | 0.83 (0.47–1.45) | 0.51 |
| Model 2 | 0.74 (0.48–1.15) | 0.18 | 1.00 (ref) | 0.86 (0.53–1.41) | 0.56 | 0.67 (0.37–1.22) | 0.19 |
| Model 3 | 0.73 (0.47–1.15) | 0.18 | 1.00 (ref) | 0.96 (0.58–1.56) | 0.85 | 0.62 (0.33–1.15) | 0.13 |
| Model 4 | 0.97 (0.55–1.71) | 0.93 | 1.00 (ref) | 1.02 (0.56–1.89) | 0.94 | 0.74 (0.35–1.60) | 0.45 |
| Betaine as Continuous Variable (2log) | Tertiles of Betaine | ||||||
|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | |||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| Diabetes, no. of events (%) | 112 (4.0%) | 48 (4.9%) | 39 (4.2%) | 25 (2.8%) | |||
| Crude | 0.75 (0.51–1.10) | 0.14 | 1.00 (ref) | 0.84 (0.55–1.28) | 0.41 | 0.58 (0.36–0.93) | 0.03 |
| Model 1 | 0.57 (0.41–0.81) | 0.002 | 1.00 (ref) | 0.69 (0.45–1.05) | 0.09 | 0.41 (0.25–0.67) | <0.001 |
| Model 2 | 0.59 (0.40–0.80) | 0.001 | 1.00 (ref) | 0.69 (0.45–1.05) | 0.08 | 0.41 (0.25–0.67) | <0.001 |
| Model 3 | 0.62 (0.42–0.93) | 0.02 | 1.00 (ref) | 0.75 (0.49–1.15) | 0.19 | 0.50 (0.31–0.82) | 0.006 |
| Model 4 | 0.69 (0.43–1.10) | 0.12 | 1.00 (ref) | 0.89 (0.55–1.46) | 0.65 | 0.57 (0.32–1.04) | 0.07 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, E.; Osté, M.C.J.; Bennett, D.W.; Jeyarajah, E.J.; Shalaurova, I.; Gruppen, E.G.; Hazen, S.L.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F.; et al. High Betaine, a Trimethylamine N-Oxide Related Metabolite, Is Prospectively Associated with Low Future Risk of Type 2 Diabetes Mellitus in the PREVEND Study. J. Clin. Med. 2019, 8, 1813. https://doi.org/10.3390/jcm8111813
Garcia E, Osté MCJ, Bennett DW, Jeyarajah EJ, Shalaurova I, Gruppen EG, Hazen SL, Otvos JD, Bakker SJL, Dullaart RPF, et al. High Betaine, a Trimethylamine N-Oxide Related Metabolite, Is Prospectively Associated with Low Future Risk of Type 2 Diabetes Mellitus in the PREVEND Study. Journal of Clinical Medicine. 2019; 8(11):1813. https://doi.org/10.3390/jcm8111813
Chicago/Turabian StyleGarcia, Erwin, Maryse C. J. Osté, Dennis W. Bennett, Elias J. Jeyarajah, Irina Shalaurova, Eke G. Gruppen, Stanley L. Hazen, James D. Otvos, Stephan J. L. Bakker, Robin P.F. Dullaart, and et al. 2019. "High Betaine, a Trimethylamine N-Oxide Related Metabolite, Is Prospectively Associated with Low Future Risk of Type 2 Diabetes Mellitus in the PREVEND Study" Journal of Clinical Medicine 8, no. 11: 1813. https://doi.org/10.3390/jcm8111813
APA StyleGarcia, E., Osté, M. C. J., Bennett, D. W., Jeyarajah, E. J., Shalaurova, I., Gruppen, E. G., Hazen, S. L., Otvos, J. D., Bakker, S. J. L., Dullaart, R. P. F., & Connelly, M. A. (2019). High Betaine, a Trimethylamine N-Oxide Related Metabolite, Is Prospectively Associated with Low Future Risk of Type 2 Diabetes Mellitus in the PREVEND Study. Journal of Clinical Medicine, 8(11), 1813. https://doi.org/10.3390/jcm8111813