Systematic Review of the Role of Biomarkers in Predicting Anastomotic Leakage Following Gastroesophageal Cancer Surgery

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
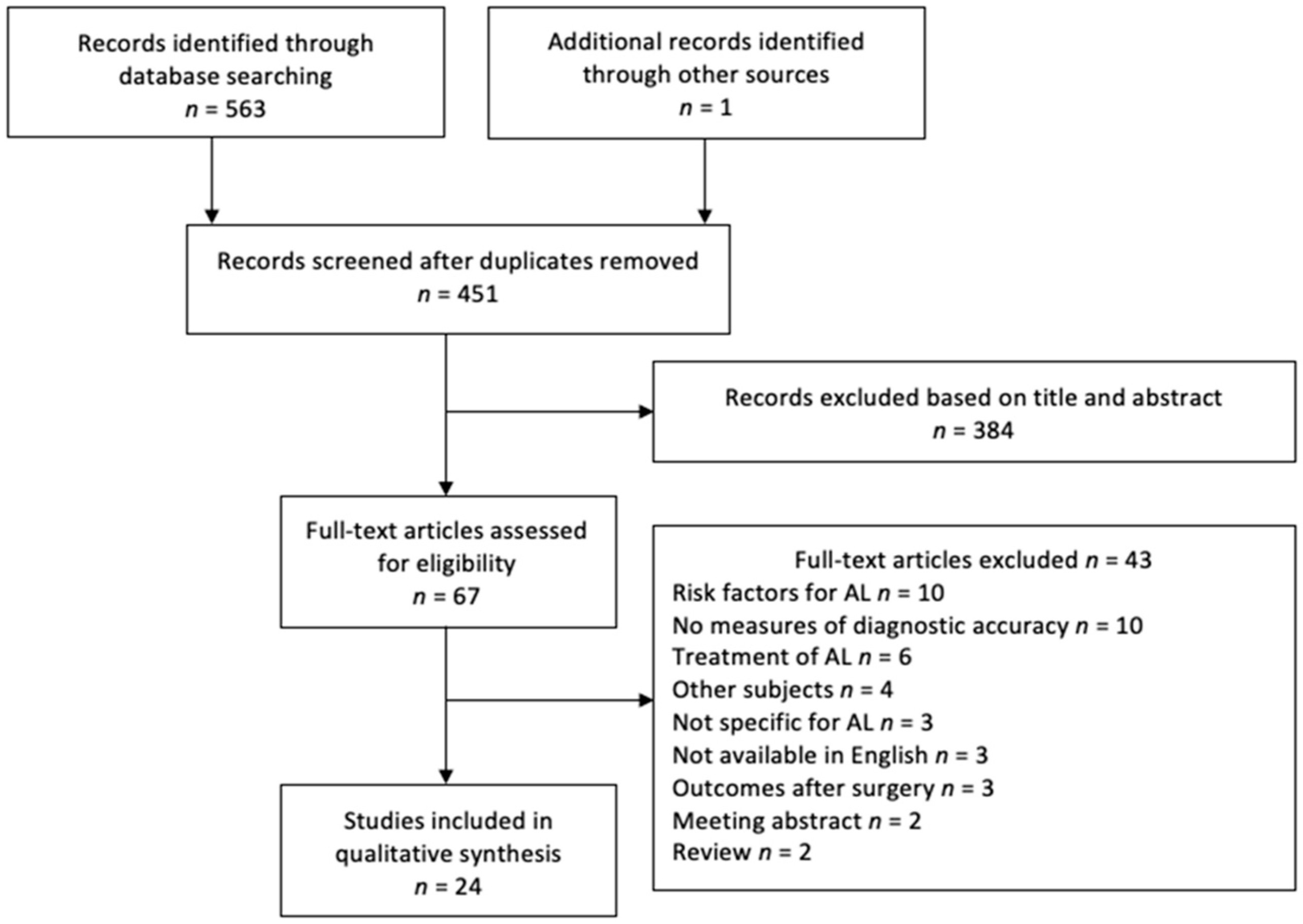
3.1. Study Selection
3.2. Study Characteristics
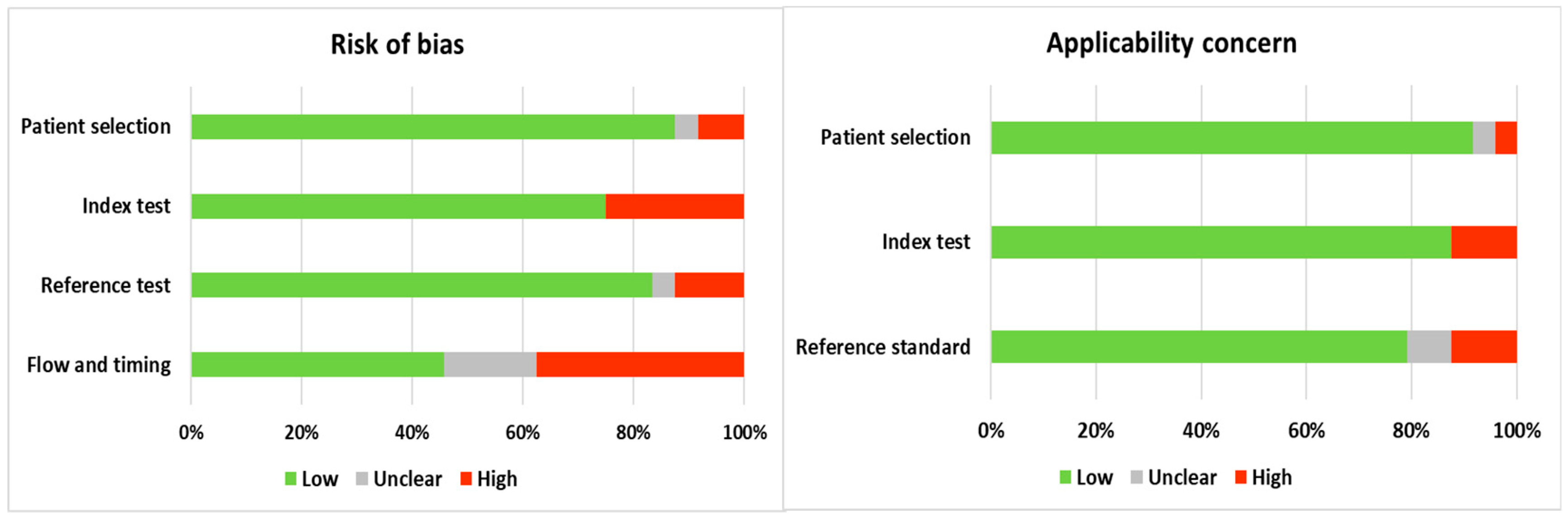
3.3. Validity Assessment
3.4. Definition of Anastomotic Leakage
3.5. Diagnostic Accuracy Biomarkers
3.5.1. Biomarkers of Inflammation
3.5.2. Biomarkers of Ischemia
3.5.3. Peritoneal Drain Fluid Biomarker
3.5.4. Combined Scores
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Gupta, B.; Kumar, N. Worldwide incidence, mortality and time trends for cancer of the oesophagus. Eur. J. Cancer. Prev. 2017, 26, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Rashid, O.M.; Wong, J. Surgical management of gastric cancer: The East vs. West perspective. J. Gastrointest. Oncol. 2015, 6, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Carboni, F.; Valle, M.; Federici, O.; Levi Sandri, G.B.; Camperchioli, I.; Lapenta, R.; Assisi, D.; Garofalo, A. Esophagojejunal anastomosis leakage after total gastrectomy for esophagogastric junction adenocarcinoma: Options of treatment. J. Gastrointest. Oncol. 2016, 7, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Robb, W.B.; Messager, M.; Goere, D.; Pichot-Delahaye, V.; Lefevre, J.H.; Louis, D.; Guiramand, J.; Kraft, K.; Mariette, C.; FREGAT Working Group–FRENCH. Predictive factors of postoperative mortality after junctional and gastric adenocarcinoma resection. JAMA Surg. 2013, 148, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Turrentine, F.E.; Denlinger, C.E.; Simpson, V.B.; Garwood, R.A.; Guerlain, S.; Agrawal, A.; Friel, C.M.; LaPar, D.J.; Stukenborg, G.J.; Jones, R.S. Morbidity, mortality, cost, and survival estimates of gastrointestinal anastomotic leaks. J. Am. Coll. Surg. 2015, 220, 195–206. [Google Scholar] [CrossRef]
- Sierzega, M.; Kolodziejczyk, P.; Kulig, J.; Polish Gastric Cancer Study Group. Impact of anastomotic leakage on long-term survival after total gastrectomy for carcinoma of the stomach. Br. J. Surg. 2010, 97, 1035–1042. [Google Scholar] [CrossRef]
- Lagarde, S.M.; de Boer, J.D.; ten Kate, F.J.; Busch, O.R.; Obertop, H.; van Lanschot, J.J. Postoperative complications after esophagectomy for adenocarcinoma of the esophagus are related to timing of death due to recurrence. Ann. Surg. 2008, 247, 71–76. [Google Scholar] [CrossRef]
- Sauvanet, A.; Mariette, C.; Thomas, P.; Lozac’h, P.; Segol, P.; Tiret, E.; Delpero, J.R.; Collet, D.; Leborgne, J.; Pradere, B.; et al. Mortality and morbidity after resection for adenocarcinoma of the gastroesophageal junction: Predictive factors. J. Am. Coll. Surg. 2005, 201, 253–262. [Google Scholar] [CrossRef]
- Inokuchi, M.; Otsuki, S.; Fujimori, Y.; Sato, Y.; Nakagawa, M.; Kojima, K. Systematic review of anastomotic complications of esophagojejunostomy after laparoscopic total gastrectomy. World J. Gastroenterol. 2015, 21, 9656–9665. [Google Scholar] [CrossRef]
- Weledji, E.P.; Verla, V. Failure to rescue patients from early critical complications of oesophagogastric cancer surgery. Ann. Med. Surg. (Lond.) 2016, 7, 34–41. [Google Scholar] [CrossRef]
- Watanabe, M.; Miyata, H.; Gotoh, M.; Baba, H.; Kimura, W.; Tomita, N.; Nakagoe, T.; Shimada, M.; Kitagawa, Y.; Sugihara, K.; et al. Total gastrectomy risk model: Data from 20,011 Japanese patients in a nationwide internet-based database. Ann. Surg. 2014, 260, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Junemann-Ramirez, M.; Awan, M.Y.; Khan, Z.M.; Rahamim, J.S. Anastomotic leakage post-esophagogastrectomy for esophageal carcinoma: Retrospective analysis of predictive factors, management and influence on longterm survival in a high volume centre. Eur. J. Cardio Thorac. Surg. 2005, 27, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.M.; Shaw, I.H.; Dresner, S.M. Early complications after Ivor Lewis subtotal esophagectomy with two-field lymphadenectomy: Risk factors and management. J. Am. Coll. Surg. 2002, 194, 285–297. [Google Scholar] [CrossRef]
- Bruce, J.; Krukowski, Z.H.; Al-Khairy, G.; Russell, E.M.; Park, K.G. Systematic review of the definition and measurement of anastomotic leak after gastrointestinal surgery. Br. J. Surg. 2001, 88, 1157–1168. [Google Scholar] [CrossRef] [PubMed]
- Goense, L.; van Rossum, P.S.; Tromp, M.; Joore, H.C.; van Dijk, D.; Kroese, A.C.; Ruurda, J.P.; van Hillegersberg, R. Intraoperative and postoperative risk factors for anastomotic leakage and pneumonia after esophagectomy for cancer. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2017, 30, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tabatabai, A.; Hashemi, M.; Mohajeri, G.; Ahmadinejad, M.; Khan, I.A.; Haghdani, S. Incidence and risk factors predisposing anastomotic leak after transhiatal esophagectomy. Ann. Thorac. Med. 2009, 4, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Oshi, M.; Kunisaki, C.; Miyamoto, H.; Kosaka, T.; Akiyama, H.; Endo, I. Risk Factors for Anastomotic Leakage of Esophagojejunostomy after Laparoscopy-Assisted Total Gastrectomy for Gastric Cancer. Dig. Surg. 2018, 35, 28–34. [Google Scholar] [CrossRef]
- Cetin, D.A.; Gundes, E.; Ciyiltepe, H.; Aday, U.; Uzun, O.; Deger, K.C.; Duman, M. Risk factors and laboratory markers used to predict leakage in esophagojejunal anastomotic leakage after total gastrectomy. Turk. J. Surg. 2018, 1–6. [Google Scholar] [CrossRef]
- Deguchi, Y.; Fukagawa, T.; Morita, S.; Ohashi, M.; Saka, M.; Katai, H. Identification of risk factors for esophagojejunal anastomotic leakage after gastric surgery. World J. Surg. 2012, 36, 1617–1622. [Google Scholar] [CrossRef]
- Kim, S.H.; Son, S.Y.; Park, Y.S.; Ahn, S.H.; Park, D.J.; Kim, H.H. Risk Factors for Anastomotic Leakage: A Retrospective Cohort Study in a Single Gastric Surgical Unit. J. Gastric Cancer 2015, 15, 167–175. [Google Scholar] [CrossRef]
- Dorcaratto, D.; Grande, L.; Pera, M. Enhanced recovery in gastrointestinal surgery: Upper gastrointestinal surgery. Dig. Sur. 2013, 30, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Jo, D.H.; Jeong, O.; Sun, J.W.; Jeong, M.R.; Ryu, S.Y.; Park, Y.K. Feasibility study of early oral intake after gastrectomy for gastric carcinoma. J. Gastric Cancer 2011, 11, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, K.; Nilsson, M.; Slim, K.; Schafer, M.; Mariette, C.; Braga, M.; Carli, F.; Demartines, N.; Griffin, S.M.; Lassen, K.; et al. Consensus guidelines for enhanced recovery after gastrectomy: Enhanced Recovery After Surgery (ERAS(R)) Society recommendations. Br. J. Surg. 2014, 101, 1209–1229. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E. Diagnosis and management of anastomotic leaks after esophagectomy. J. Gastrointest. Surg. 2011, 15, 1319–1322. [Google Scholar] [CrossRef] [PubMed]
- Girard, E.; Messager, M.; Sauvanet, A.; Benoist, S.; Piessen, G.; Mabrut, J.Y.; Mariette, C. Anastomotic leakage after gastrointestinal surgery: Diagnosis and management. J. Visc. Surg. 2014, 151, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Markar, S.; Gronnier, C.; Duhamel, A.; Mabrut, J.Y.; Bail, J.P.; Carrere, N.; Lefevre, J.H.; Brigand, C.; Vaillant, J.C.; Adham, M.; et al. The Impact of Severe Anastomotic Leak on Long-term Survival and Cancer Recurrence After Surgical Resection for Esophageal Malignancy. Ann. Surg. 2015, 262, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group Prisma. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Šimundić, A.-M. Measures of Diagnostic Accuracy: Basic Definitions. EJIFCC 2009, 19, 203–211. [Google Scholar]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Campbell, J.M.; Klugar, M.; Ding, S.; Carmody, D.P.; Hakonsen, S.J.; Jadotte, Y.T.; White, S.; Munn, Z. Diagnostic test accuracy: Methods for systematic review and meta-analysis. Int. J. Evid. Based Healthc. 2015, 13, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Asti, E.; Bonitta, G.; Melloni, M.; Tornese, S.; Milito, P.; Sironi, A.; Costa, E.; Bonavina, L. Utility of C-reactive protein as predictive biomarker of anastomotic leak after minimally invasive esophagectomy. Langenbecks Arch. Surg. 2018, 403, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Baker, E.H.; Hill, J.S.; Reames, M.K.; Symanowski, J.; Hurley, S.C.; Salo, J.C. Drain amylase aids detection of anastomotic leak after esophagectomy. J. Gastrointest. Oncol. 2016, 7, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Fullarton, G.; Forshaw, M.; Horgan, P.G.; McMillan, D.C. Persistent elevation of C-reactive protein after gastro-oesophageal cancer resection as a predictor of post-operative intra-abdominal infective complications. Gastroenterology 2010, 138, S898. [Google Scholar] [CrossRef]
- Findlay, J.M.; Tilson, R.C.; Harikrishnan, A.; Sgromo, B.; Marshall, R.E.; Maynard, N.D.; Gillies, R.S.; Middleton, M.R. Attempted validation of the NUn score and inflammatory markers as predictors of esophageal anastomotic leak and major complications. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2015, 28, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Cross, A.J.; Foo, E.W.; Roberts, R.H. C-reactive protein is a useful negative predictor of anastomotic leak in oesophago-gastric resection. ANZ J. Surg. 2018, 88, 223–227. [Google Scholar] [CrossRef]
- Hoeboer, S.H.; Groeneveld, A.B.J.; Engels, N.; van Genderen, M.; Wijnhoven, B.P.L.; van Bommel, J. Rising C-Reactive Protein and Procalcitonin Levels Precede Early Complications After Esophagectomy. J. Gastrointest. Surg. 2015, 19, 613–624. [Google Scholar] [CrossRef] [Green Version]
- Ip, B.; Ng, K.T.; Packer, S.; Paterson-Brown, S.; Couper, G.W. High serum lactate as an adjunct in the early prediction of anastomotic leak following oesophagectomy. Int. J. Surg. 2017, 46, 7–10. [Google Scholar] [CrossRef]
- Ji, L.; Wang, T.; Tian, L.; Gao, M. The early diagnostic value of C-reactive protein for anastomotic leakage post radical gastrectomy for esophagogastric junction carcinoma: A retrospective study of 97 patients. Int. J. Surg. 2016, 27, 182–186. [Google Scholar] [CrossRef]
- Li, H.; Wang, D.; Wei, W.; Ouyang, L.; Lou, N. The Predictive Value of Coefficient of PCT x BG for Anastomotic Leak in Esophageal Carcinoma Patients With ARDS After Esophagectomy. J. Intensive Care Med. 2017. [Google Scholar] [CrossRef]
- Noble, F.; Curtis, N.; Harris, S.; Kelly, J.J.; Bailey, I.S.; Byrne, J.P.; Underwood, T.J. Risk assessment using a novel score to predict anastomotic leak and major complications after oesophageal resection. J. Gastrointest. Surg. 2012, 16, 1083–1095. [Google Scholar] [CrossRef] [PubMed]
- Park, J.K.; Kim, J.J.; Moon, S.W. C-reactive protein for the early prediction of anastomotic leak after esophagectomy in both neoadjuvant and non-neoadjuvant therapy case: A propensity score matching analysis. J. Thorac. Dis. 2017, 9, 3693–3702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, J.Q.; He, Y.Z.; Fang, Y.; Wu, W.; Zhong, M. The predictive value of plasma cytokines on gastroesophageal anastomotic leakage at an early stage in patients undergoing esophagectomy. J. Thorac. Dis. 2017, 9, 2544–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edagawa, E.; Matsuda, Y.; Gyobu, K.; Lee, S.; Kishida, S.; Fujiwara, Y.; Hashiba, R.; Osugi, H.; Suehiro, S. C-reactive Protein is a Useful Marker for Early Prediction of Anastomotic Leakage after Esophageal Reconstruction. Osaka City Med. J. 2015, 61, 53–61. [Google Scholar] [PubMed]
- Gao, C.; Xu, G.; Wang, C.; Wang, D. Evaluation of preoperative risk factors and postoperative indicators for anastomotic leak of minimally invasive McKeown esophagectomy: A single-center retrospective analysis. J. Cardiothorac. Surg. 2019, 14, 46. [Google Scholar] [CrossRef]
- Giulini, L.; Dubecz, A.; Solymosi, N.; Tank, J.; Renz, M.; Thumfart, L.; Stein, H.J. Prognostic Value of Chest-Tube Amylase Versus C-Reactive Protein as Screening Tool for Detection of Early Anastomotic Leaks After Ivor Lewis Esophagectomy. J. Laparoendoscopic Adv. Surg. Tech. Part A 2019, 29, 192–197. [Google Scholar] [CrossRef]
- Berkelmans, G.H.K.; Kouwenhoven, E.A.; Smeets, B.J.J.; Weijs, T.J.; Silva Corten, L.C.; Van Det, M.J.; Nieuwenhuijzen, G.A.P.; Luyer, M.D.P. Diagnostic value of drain amylase for detecting intrathoracic leakage after esophagectomy. World J. Gastroenterol. 2015, 21, 9118–9125. [Google Scholar] [CrossRef]
- Machens, A.; Busch, C.; Bause, H.; Izbicki, J.R. Gastric tonometry and drain amylase analysis in the detection of cervical oesophagogastric leakage. Br. J. Surg. 1996, 83, 1614–1615. [Google Scholar] [CrossRef]
- Perry, Y.; Towe, C.W.; Kwong, J.; Ho, V.P.; Linden, P.A. Serial Drain Amylase Can Accurately Detect Anastomotic Leak After Esophagectomy and May Facilitate Early Discharge. Ann. Thorac Surg. 2015, 100, 2041–2046. [Google Scholar] [CrossRef]
- Schots, J.P.M.; Luyer, M.D.P.; Nieuwenhuijzen, G.A.P. Abdominal Drainage and Amylase Measurement for Detection of Leakage After Gastrectomy for Gastric Cancer. J. Gastrointest. Surg. 2018. [Google Scholar] [CrossRef]
- Yu, W.S.; Jung, J.; Shin, H.; Roh, Y.; Byun, G.E.; Kim, D.J.; Haam, S.; Park, S.Y. Amylase level in cervical drain fluid and anastomotic leakage after cervical oesophagogastrostomy. Eur. J. Cardio Thorac. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Paireder, M.; Jomrich, G.; Asari, R.; Kristo, I.; Gleiss, A.; Preusser, M.; Schoppmann, S.F. External validation of the NUn score for predicting anastomotic leakage after oesophageal resection. Sci. Rep. 2017, 7, 9725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellebaek, M.; Qvist, N.; Fristrup, C.; Mortensen, M.B. Mediastinal microdialysis in the diagnosis of early anastomotic leakage after resection for cancer of the esophagus and gastroesophageal junction. Am. J. Surg. 2014, 208, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Plat, V.D.; van Gaal, N.; Covington, J.A.; Neal, M.; de Meij, T.G.J.; van der Peet, D.L.; Zonderhuis, B.; Kazemier, G.; de Boer, N.K.H.; Daams, F. Non-Invasive Detection of Anastomotic Leakage Following Esophageal and Pancreatic Surgery by Urinary Analysis. Dig. Surg. 2019, 36, 173–180. [Google Scholar] [CrossRef]
- Miller, D.L.; Helms, G.A.; Mayfield, W.R. Evaluation of Esophageal Anastomotic Integrity With Serial Pleural Amylase Levels. Ann. Thorac. Surg. 2018, 105, 200–206. [Google Scholar] [CrossRef] [Green Version]
- Bosmans, J.W.; Jongen, A.C.; Bouvy, N.D.; Derikx, J.P. Colorectal anastomotic healing: Why the biological processes that lead to anastomotic leakage should be revealed prior to conducting intervention studies. BMC Gastroenterol. 2015, 15, 180. [Google Scholar] [CrossRef]
- Shomaf, M. Histopathology of human intestinal anastomosis. East Mediterr. Health J. 2003, 9, 413–421. [Google Scholar]
- Shogan, B.D.; Belogortseva, N.; Luong, P.M.; Zaborin, A.; Lax, S.; Bethel, C.; Ward, M.; Muldoon, J.P.; Singer, M.; An, G.; et al. Collagen degradation and MMP9 activation by Enterococcus faecalis contribute to intestinal anastomotic leak. Sci. Transl. Med. 2015, 7, 286ra268. [Google Scholar] [CrossRef] [Green Version]
- Shogan, B.D.; Carlisle, E.M.; Alverdy, J.C.; Umanskiy, K. Do we really know why colorectal anastomoses leak? J. Gastrointest. Surg. 2013, 17, 1698–1707. [Google Scholar] [CrossRef]
- Butt, I.; Shrestha, B.M. Two-hit hypothesis and multiple organ dysfunction syndrome. JNMA J. Nepal. Med. Assoc. 2008, 47, 82–85. [Google Scholar] [CrossRef]
- Kahokehr, A.; Sammour, T.; Srinivasa, S.; Hill, A.G. Metabolic response to abdominal surgery: The 2-wound model. Surgery 2011, 149, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Floodeen, H.; Hallbook, O.; Rutegard, J.; Sjodahl, R.; Matthiessen, P. Early and late symptomatic anastomotic leakage following low anterior resection of the rectum for cancer: Are they different entities? Colorectal Dis. 2013, 15, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Bolton, J.S.; Conway, W.C.; Abbas, A.E. Planned delay of oral intake after esophagectomy reduces the cervical anastomotic leak rate and hospital length of stay. J. Gastrointest. Surg. 2014, 18, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Gaines, S.; Shao, C.; Hyman, N.; Alverdy, J.C. Gut microbiome influences on anastomotic leak and recurrence rates following colorectal cancer surgery. Br. J. Surg. 2018, 105, e131–e141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cikot, M.; Kasapoglu, P.; Isiksacan, N.; Binboga, S.; Kones, O.; Gemici, E.; Kartal, B.; Alis, H. The importance of presepsin value in detection of gastrointestinal anastomotic leak: A pilot study. J. Surg. Res. 2018, 228, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Okamura, A.; Watanabe, M.; Imamura, Y.; Kamiya, S.; Yamashita, K.; Kurogochi, T.; Mine, S. Preoperative Glycosylated Hemoglobin Levels Predict Anastomotic Leak After Esophagectomy with Cervical Esophagogastric Anastomosis. World J. Surg. 2017, 41, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Reisinger, K.; Derikx, J.; Hulsewé, K.; Van Bijnen, A.A.; Von Meyenfeldt, M.; Poeze, M. Plasma markers for anastomotic leakage after colorectal surgery. Gastroenterology 2013, 144, S656. [Google Scholar] [CrossRef]
- Tanaka, Y.; Kanda, M.; Tanaka, C.; Kobayashi, D.; Mizuno, A.; Iwata, N.; Hayashi, M.; Niwa, Y.; Takami, H.; Yamada, S.; et al. Usefulness of preoperative estimated glomerular filtration rate to predict complications after curative gastrectomy in patients with clinical T2-4 gastric cancer. Gastric Cancer 2017, 20, 736–743. [Google Scholar] [CrossRef] [Green Version]
- Zawadzki, M.; Czarnecki, R.; Rzaca, M.; Obuszko, Z.; Velchuru, V.R.; Witkiewicz, W. C-reactive protein and procalcitonin predict anastomotic leaks following colorectal cancer resections—A prospective study. Videosurg. Miniinvasive Tech. 2015, 10, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Korner, H.; Nielsen, H.J.; Soreide, J.A.; Nedrebo, B.S.; Soreide, K.; Knapp, J.C. Diagnostic accuracy of C-reactive protein for intraabdominal infections after colorectal resections. J. Gastrointest. Surg. 2009, 13, 1599–1606. [Google Scholar] [CrossRef]
- Welsch, T.; Frommhold, K.; Hinz, U.; Weigand, M.A.; Kleeff, J.; Friess, H.; Buchler, M.W.; Schmidt, J. Persisting elevation of C-reactive protein after pancreatic resections can indicate developing inflammatory complications. Surgery 2008, 143, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.Y.; Yim, H.W.; Park, C.H.; Song, K.Y. C-reactive protein can be an early predictor of postoperative complications after gastrectomy for gastric cancer. Surg. Endosc. 2017, 31, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Shishido, Y.; Fujitani, K.; Yamamoto, K.; Hirao, M.; Tsujinaka, T.; Sekimoto, M. C-reactive protein on postoperative day 3 as a predictor of infectious complications following gastric cancer resection. Gastric Cancer 2016, 19, 293–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsujimoto, H.; Ono, S.; Takahata, R.; Hiraki, S.; Yaguchi, Y.; Kumano, I.; Matsumoto, Y.; Yoshida, K.; Aiko, S.; Ichikura, T.; et al. Systemic inflammatory response syndrome as a predictor of anastomotic leakage after esophagectomy. Surg. Today 2012, 42, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Van Genderen, M.E.; Lima, A.; de Geus, H.; Klijn, E.; Wijnhoven, B.; Gommers, D.; van Bommel, J. Serum C-reactive protein as a predictor of morbidity and mortality in intensive care unit patients after esophagectomy. Ann. Thorac. Surg. 2011, 91, 1775–1779. [Google Scholar] [CrossRef] [PubMed]
- Warschkow, R.; Tarantino, I.; Ukegjini, K.; Beutner, U.; Muller, S.A.; Schmied, B.M.; Steffen, T. Diagnostic study and meta-analysis of C-reactive protein as a predictor of postoperative inflammatory complications after gastroesophageal cancer surgery. Langenbecks Arch. Surg. 2012, 397, 727–736. [Google Scholar] [CrossRef] [Green Version]
- Aiolfi, A.; Asti, E.; Rausa, E.; Bonavina, G.; Bonitta, G.; Bonavina, L. Use of C-reactive protein for the early prediction of anastomotic leak after esophagectomy: Systematic review and Bayesian meta-analysis. PLoS ONE 2018, 13, e0209272. [Google Scholar] [CrossRef]
- Garcia-Granero, A.; Frasson, M.; Flor-Lorente, B.; Blanco, F.; Puga, R.; Carratala, A.; Garcia-Granero, E. Procalcitonin and C-reactive protein as early predictors of anastomotic leak in colorectal surgery: A prospective observational study. Dis. Colon Rectum 2013, 56, 475–483. [Google Scholar] [CrossRef]
- Hoeboer, S.H.; Alberts, E.; van den Hul, I.; Tacx, A.N.; Debets-Ossenkopp, Y.J.; Groeneveld, A.B. Old and new biomarkers for predicting high and low risk microbial infection in critically ill patients with new onset fever: A case for procalcitonin. J. Infect. 2012, 64, 484–493. [Google Scholar] [CrossRef]
- Lagoutte, N.; Facy, O.; Ravoire, A.; Chalumeau, C.; Jonval, L.; Rat, P.; Ortega-Deballon, P. C-reactive protein and procalcitonin for the early detection of anastomotic leakage after elective colorectal surgery: Pilot study in 100 patients. J. Visc. Surg. 2012, 149, e345–e349. [Google Scholar] [CrossRef]
- Mokart, D.; Merlin, M.; Sannini, A.; Brun, J.P.; Delpero, J.R.; Houvenaeghel, G.; Moutardier, V.; Blache, J.L. Procalcitonin, interleukin 6 and systemic inflammatory response syndrome (SIRS): Early markers of postoperative sepsis after major surgery. Br. J. Anaesth. 2005, 94, 767–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uzzan, B.; Cohen, R.; Nicolas, P.; Cucherat, M.; Perret, G.Y. Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: A systematic review and meta-analysis. Crit. Care Med. 2006, 34, 1996–2003. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Sato, N.; Kojika, M.; Yaegashi, Y.; Suzuki, Y.; Suzuki, K.; Endo, S. Serum procalcitonin levels are elevated in esophageal cancer patients with postoperative infectious complications. Eur. Surg. Res. 2005, 37, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.M.; Lamb, P.J.; Dresner, S.M.; Richardson, D.L.; Hayes, N. Diagnosis and management of a mediastinal leak following radical oesophagectomy. Br. J. Surg. 2001, 88, 1346–1351. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Chen, J.; Su, K.; Dong, Z. Abdominal drainage versus no drainage post-gastrectomy for gastric cancer. Cochrane Database Syst. Rev. 2015, CD008788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Lee, J.; Hyung, W.J.; Cheong, J.H.; Chen, J.; Choi, S.H.; Noh, S.H. Gastric cancer surgery without drains: A prospective randomized trial. J. Gastrointest. Surg. 2004, 8, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; Allum, W.; De Manzoni, G.; Ferri, L.; Immanuel, A.; Kuppusamy, M.; Law, S.; Lindblad, M.; Maynard, N.; Neal, J.; et al. Guidelines for Perioperative Care in Esophagectomy: Enhanced Recovery After Surgery (ERAS((R))) Society Recommendations. World J. Surg. 2019, 43, 299–330. [Google Scholar] [CrossRef]
- Hall, B.R.; Flores, L.E.; Parshall, Z.S.; Shostrom, V.K.; Are, C.; Reames, B.N. Risk factors for anastomotic leak after esophagectomy for cancer: A NSQIP procedure-targeted analysis. J. Surg. Oncol. 2019, 120, 661–669. [Google Scholar] [CrossRef]
- Lainas, P.; Fuks, D.; Gaujoux, S.; Machroub, Z.; Fregeville, A.; Perniceni, T.; Mal, F.; Dousset, B.; Gayet, B. Preoperative imaging and prediction of oesophageal conduit necrosis after oesophagectomy for cancer. Br. J. Surg. 2017, 104, 1346–1354. [Google Scholar] [CrossRef]
- Raymond, D.P.; Seder, C.W.; Wright, C.D.; Magee, M.J.; Kosinski, A.S.; Cassivi, S.D.; Grogan, E.L.; Blackmon, S.H.; Allen, M.S.; Park, B.J.; et al. Predictors of Major Morbidity or Mortality After Resection for Esophageal Cancer: A Society of Thoracic Surgeons General Thoracic Surgery Database Risk Adjustment Model. Ann. Thorac. Surg. 2016, 102, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Tenny, S.; Hoffman, R.M. Prevalence. Updated 27 March 2019. In StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2019. Available online: https://www.ncbi.nlm.nih.gov/books/NBK430867 (accessed on 10 November 2019).
- Okholm, C.; Goetze, J.P.; Svendsen, L.B.; Achiam, M.P. Inflammatory response in laparoscopic vs. open surgery for gastric cancer. Scand. J. Gastroenterol. 2014, 49, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Shu, Z.B.; Cao, H.P.; Li, Y.C.; Sun, L.B. Influences of laparoscopic-assisted gastrectomy and open gastrectomy on serum interleukin-6 levels in patients with gastric cancer among Asian populations: A systematic review. BMC Gastroenterol. 2015, 15, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, K.; Watanabe, M.; Mine, S.; Toihata, T.; Fukudome, I.; Okamura, A.; Yuda, M.; Hayami, M.; Ishizuka, N.; Imamura, Y. Minimally invasive esophagectomy attenuates the postoperative inflammatory response and improves survival compared with open esophagectomy in patients with esophageal cancer: A propensity score matched analysis. Surg. Endosc. 2018. [Google Scholar] [CrossRef] [PubMed]
- Honda, M.; Kuriyama, A.; Noma, H.; Nunobe, S.; Furukawa, T.A. Hand-sewn versus mechanical esophagogastric anastomosis after esophagectomy: A systematic review and meta-analysis. Ann. Surg. 2013, 257, 238–248. [Google Scholar] [CrossRef]
- Hulscher, J.B.; Tijssen, J.G.; Obertop, H.; van Lanschot, J.J. Transthoracic versus transhiatal resection for carcinoma of the esophagus: A meta-analysis. Ann. Thorac. Surg. 2001, 72, 306–313. [Google Scholar] [CrossRef]
- Messager, M.; Warlaumont, M.; Renaud, F.; Marin, H.; Branche, J.; Piessen, G.; Mariette, C. Recent improvements in the management of esophageal anastomotic leak after surgery for cancer. Eur. J. Surg. Oncol. 2017, 43, 258–269. [Google Scholar] [CrossRef]
- Klink, C.D.; Binnebosel, M.; Otto, J.; Boehm, G.; von Trotha, K.T.; Hilgers, R.D.; Conze, J.; Neumann, U.P.; Jansen, M. Intrathoracic versus cervical anastomosis after resection of esophageal cancer: A matched pair analysis of 72 patients in a single center study. World J. Surg. Oncol. 2012, 10, 159. [Google Scholar] [CrossRef] [Green Version]
- Zargar-Shoshtari, K.; Sammour, T.; Kahokehr, A.; Connolly, A.B.; Hill, A.G. Randomized clinical trial of the effect of glucocorticoids on peritoneal inflammation and postoperative recovery after colectomy. Br. J. Surg. 2009, 96, 1253–1261. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference | Resection | Study Design b | Study Period | MI Approach (%) | Patients (n) | AL (n) | N CRT (n) | Marker Type | Biomarkers |
|---|---|---|---|---|---|---|---|---|---|
| Asti et al. [32] | Esophageal | Retrospective | 2012–2017 | 100 | 243 | 29 | 96 | Serum | CRP, PCT, leucocytes and PN |
| Baker et al. [33] | Esophageal | Retrospective | 2009–2014 | 93 | 100 | 13 | 68 | Serum and drain | Amylase and leucocytes |
| Berkelmans et al. [47] | Esophageal | Retrospective | 2013–2014 | 100 | 89 | 15 | 84 | Drain | Amylase |
| Dutta et al. [34] | Esophagogastric | Retrospective | 2005–2009 | NR | 136 | 17 | 80 | Serum | CRP |
| Edagawa et al. [44] | Esophageal | Retrospective | 2007–2009 | 66 | 204 | 44 | NR | Serum | CRP, FIB |
| Ellebaek et al. [53] | Esophagogastric | Prospective | 2006–2010 | 0 | 54 | 7 | 29 | Mediastinal microdialysis | Lactate, pyruvate, glucose, glycerol a and pyrovate |
| Findlay et al. [35] | Esophagogastric | Retrospective | 2008–2013 | 0 | 248 | 21 | 189 | Serum and drain | CRP a, leucocytes, albumin a and NUn score |
| Gao et al. [45] | Esophageal | Retrospective | 2016–2017 | 100 | 96 | 12 | 38 | Serum and drain | Amylase and prealbumin |
| Giulini et al. [46] | Esophageal | Retrospective | 2015–2017 | 64 | 80 | 6 | 40 | Serum and drain | Amylase and CRP |
| Gordon et al. [36] | Esophagogastric | Retrospective | 2004–2014 | 0 | 145 | 13 | NR | Serum | CRP |
| Hoeboer et al. [37] | Esophageal | Prospective | 2011–2012 | 10 | 45 | 10 | 40 | Serum | CRP, PCT and leucocytes a |
| Ip et al. [38] | Esophageal | Retrospective | 2012–2014 | 7 | 136 | 18 | 70 | Serum | Lactate |
| Ji et al. [39] | Esophagogastric | Retrospective | 2014 | 0 | 97 | 10 | NR | Serum | CRP |
| Li et al. [40] | Esophageal | Retrospective | 2013–2016 | 8 | 71 | 47 | 5 | Serum and respiratory | CRP a, PCT, leucocytes a, albumin, Hb a, PLT a, BG, pO2 a and fiO2 a |
| Machens et al. [48] | Esophageal | Retrospective | 1992–1994 | 0 | 26 | 14 | NR | Drain | amylase and ph a |
| Miller et al. [55] | Esophageal | Retospective | 2015–2016 | 100 | 45 | 3 | 27 | Drain | Amylase |
| Noble et al. [41] | Esophageal | Retrospective | 2005–2011 | NR | 258 | 26 | 156 | Serum and score | CRP, leucocytes, albumin and NUn score |
| Paireder et al. [52] | Esophageal | Retrospective | 2003–2014 | 28 | 258 | 32 | 177 | Score | NUn score |
| Park et al. [42] | Esophageal | Retrospective | 2009–2016 | 56 | 201 | 23 | 45 | Serum | CRP and leucocytes a |
| Perry et al. [49] | Esophageal | Retrospective | 2007–2014 | 58 | 146 | 35 | NR | Drain | Amylase |
| Plat et al. [54] | Esophageal | Prospective | 2015–2016 | NR | 31 | 9 | 29 | Urine | VOC |
| Schots et al. [50] | Gastric | Retrospective | 2013–2017 | 70 | 107 | 8 | 71 | Drain | Amylase and CRP a |
| Song et al. [43] | Esophageal | Retrospective | 2015–2016 | 67 | 183 | 16 | 50 | Plasma | TNF-, IL-2R, IL-6, IL-8 and IL-10 |
| Yu et al. [51] | Esophageal | Retrospective | 2014–2017 | NR | 99 | 10 | 17 | Drain | Amylase |
| Reference | Definition of Anastomotic Leakage |
|---|---|
| Asti et al. [32] | AL was suspected by the presence of clinical signs and confirmed by extravasation of oral contrast at gastrografin swallow study and/or computed tomography (CT), and/or visualization of anastomotic defect at upper gastrointestinal endoscopy. |
| Baker et al. [33] | AL was defined by contrast extravasation on postoperative CT esophagram or the presence of empyema on chest CT. |
| Berkelmans et al. [47] | AL was defined as any sign of leakage of the esophagogastric anastomosis on endoscopy, reoperation, and radiographic investigations, post mortal examination or when gastrointestinal contents were found in drain fluid. |
| Dutta et al. [34] | AL was confirmed by radiology (i.e., contrast enhanced multi-detector CT scan or conventional radiology with water soluble contrast), endoscopy, or during surgical exploration. |
| Edagawa et al. [44] | AL was defined as discontinuity of the esophagogastric anastomosis as detected by GIF, esophagography, or CT. The clinical significance of the leakage was not considered in this study. |
| Ellebaek et al. [53] | AL was suspected by the presence of clinical symptoms or alterations in blood samples indicating complications and checked by CT scan with oral contrast, followed by endoscopy. |
| Findlay et al. [35] | AL was defined in two ways: first as clinical or radiological evidence of a leak plus symptoms and second as any clinical or radiological evidence of a leak, irrespective of symptoms. |
| Gao et al. [45] | AL was defined as a gastroesophageal defect involving esophagus, anastomosis and conduit. |
| Giulini et al. [46] | AL was defined as a full-thickness lesion involving the anastomosis or the gastric conduit (staple line) requiring intervention or reiteration (grade III complication according to the Clavien–Dindo Classification) occurring within postoperative day (POD) 5. |
| Gordon et al. [36] | AL was defined as extravasation of oral contrast on cross-sectional imaging or an anastomotic defect visualized intraoperatively on return to theatre. Endoscopy was not used to diagnose AL. |
| Hoeboer et al. [37] | AL was defined as esophago-enteric leak confirmed by endoscopy or esophageal contrast videography that requires local treatment, surgical treatment, or removal of conduit. |
| Ip et al. [38] | AL was diagnosed by the presence of enteric content in the chest drain, endoscopic visualization of a defect in the esophagogastric anastomosis, or by extravasation of oral contrast at fluoroscopy or CT. |
| Ji et al. [39] | When postoperative AL was suspicious, methylene blue was administered orally. If the fluid from the abdominal drain was contaminated with blue dye, diagnosis of AL was confirmed. |
| Li et al. [40] | AL was defined as disruption of the esophagogastric anastomosis, the gastric staple line, or both identified by radiographic contrast examination, operative exploration, or both. Established by 3 methods: (1) oral methylene blue, (2) oral contrast computed tomography, and (3) endoscopy or operative exploration. |
| Machens et al. [48] | Cervical leaks confirmed on exploration of the neck wound were termed ‘major’, in contrast to those ‘minor’ leaks identified only in routine contrast studies. |
| Miller et al. [55] | No definition of AL reported. Anastomotic integrity was tested by a fluoroscopic water-soluble contrast agent or barium contrast agent, or both. Thoracic CT scans were performed if a leak was suspected or not clearly demonstrated on the swallow. |
| Noble et al. [41] | AL was defined as a leak sufficient to cause symptoms and confirmed by radiology (contrast-enhanced multi-detector CT scan with on-table contrast or water-soluble contrast studies), endoscopy or surgical exploration. |
| Paireder et al. [52] | No clear definition of AL given. Some ALs were diagnosed with routine contrast swallow. Article work based on the NUn score in Findlay and colleagues [35]. |
| Park et al. [42] | AL was defined as the disruption of the anastomosis that leads to outflow of the intraluminal content, which is obvious leaks, as well as leaks without the presence of any clinical symptoms but with only occult leaks detected with esophagography followed by chest CT. |
| Perry et al. [49] | AL was defined as clinical or radiologic evidence of a full-thickness gastrointestinal defect involving the esophagus, anastomosis, staple line, or conduit. |
| Plat et al. [54] | AL was defined as a full thickness defect involving the esophageal anastomosis (the Esophagectomy Complications Consensus Group). |
| Schots et al. [50] | AL was defined as any sign of leakage of the gastrojejunostomy or esophagojejunostomy, entero-enterostomy, duodenal stump, or pancreas diagnosed by CT scan, endoscopy, or during reoperation. |
| Song et al. [43] | AL was diagnosed when one of the three following conditions was met: (1) chest radiography or computerized tomography obtained the presence of intra-thoracic collection of swallowing contrast agent adjacent to the anastomosis; (2) extravasation of gastrointestinal tract content through a wound or drainage tube; (3) direct observation of AL by postoperative gastroscopy examination; (4) intraoperative diagnosis. |
| Yu et al. [51] | AL was defined as clinical or radiological evidence of a full-thickness gastrointestinal defect involving the esophagus, anastomosis, staple line or conduit. |
| Reference | Biomarker | POD | Cut-Off Values | AUROC | Sensitivity | SPECIFICITY | NPV | PPV | AL (n) |
|---|---|---|---|---|---|---|---|---|---|
| Asti et al. [32] | CRP | 5 | 83 mg/L | 0.818 | 89.3% | 60.8% | 97.7% | 23.1% | 29/243 |
| Dutta et al. [34] | CRP | 3 | 180 mg/L | 0.808 | 82.0% | 63.0% | NR | NR | 17/136 |
| 4 | 180 mg/L | 0.857 | 71.0% | 83.0% | NR | NR | 17/136 | ||
| Giulini et al. [46] | CRP | 2 | 299 mg/L | 0.902 | 100.0% | 75.0% | NR | NR | 4/80 |
| Gordon et al. [36] | CRP | 2 | 209 mg/L | 0.819 | 100.0% | 64.0% | 100.0% | 21.0% | 13/145 |
| 3 | 190 mg/L | 0.836 | 100.0% | 61.0% | 100.0% | 20.0% | 13/145 | ||
| 6 | 154 mg/L | 0.907 | 100.0% | 80.0% | 100.0% | 33.0% | 13/145 | ||
| Hoeboer et al. [37] | CRP | Δ0-3 | 55 | 0.820 | 80.0% | 80.0% | 94.0% | 50.0% | 10/45 |
| Ji et al. [39] | CRP | 1 | 117 mg/L | 0.994 | 90.0% | 89.0% | NR | NR | 10/97 |
| 2 | 177 mg/L | 0.908 | 90.0% | 95.0% | NR | NR | 10/97 | ||
| 3 | 153 mg/L | 0.936 | 90.0% | 89.0% | NR | NR | 10/97 | ||
| 4 | 89 mg/L | 0.917 | 90.0% | 95.0% | NR | NR | 10/97 | ||
| 5 | 92 mg/L | 0.881 | 90.0% | 95.0% | NR | NR | 10/97 | ||
| Park et al. [42] | CRP (non-NT) | 3 | 171.2 mg/L | 0.822 | 69.2% | 78.1% | NR | NR | 15/156 |
| CRP (non-NT/MIE) | 3 | 128.6 mg/L | 0.800 | 83.3% | 64.9% | NR | NR | NR/89 | |
| CRP (non-NT/OE) | 3 | 179.4 mg/L | 0.834 | 71.4% | 72.0% | NR | NR | NR/67 |
| Reference | Biomarker | POD | Cut-off Values | AUROC | Sensitivity | Specificity | NPV | PPV | AL (n) |
|---|---|---|---|---|---|---|---|---|---|
| Gao et al. [45] | Prealbumin | 5 | 128 g/L | 0.824 | 100.0% | 50.0% | NR | NR | 12/96 |
| Hoeboer et al. [37] | PCT | 3 | 0.35 ng/ml | 0.860 | 67.0% | 80.0% | 87.0% | 55.0% | 10/45 |
| Noble et al. [41] | NUn score | 4 | 10 | 0.801 | 95.0% | 49.0% | NR | NR | 26/258 |
| Asti et al. [32] | PCT | 5 | 0.380 ng/ml | 0.751 | 77.8% | 71.4% | 94.2% | 35.0% | 29/243 |
| Hoeboer et al. [37] | PCT | 1 | 1.82 ng/ml | 0.760 | 22.0% | 100.0% | 83.0% | 100.0% | 10/45 |
| Li et al. [40] | BG | Any | 93 pg/mL | 0.773 | 61.7% | 83.3% | 72.3% | 66.7% | 47/71 |
| PCT | Any | 3 ng/mL | 0.752 | 72.3% | 67.7% | 63.8% | 83.3% | 47/71 | |
| PCT × BG | Any | 261 | 0.773 | 72.3% | 91.7% | 72.3% | 91.7% | 47/71 | |
| Noble et al. [41] | Albumin | 5 | 22.5 g/L | 0.742 | 76.0% | 56.0% | NR | NR | 26/258 |
| WCC | 5 | 8.95 (x10/L) | 0.715 | 78.0% | 58.0% | NR | NR | 26/258 | |
| NUn score | 5 | 10 | 0.796 | 88.0% | 55.0% | NR | NR | 26/258 | |
| Song et al. [43] | IL-6 | 1 | 74.6 pg/mL | 0.735 | 100.0% | 45.7% | NR | NR | 16/183 |
| IL-8 | 1 | 61.1 pg/mL | 0.720 | 60.0% | 45.7% | NR | NR | 16/183 | |
| IL-10 | 1 | 17.2 pg/mL | 0.784 | 66.7% | 84.8% | NR | NR | 16/183 | |
| Giulini et al. [46] | Amylase | 1 | 335 IU/L | 0.814 | 75.0% | 100.0% | NR | NR | 4/80 |
| Schots et al. [50] | Amylase | 1 | 750 IU/L | 0.703 | 71.4% | 81.4% | 96.0% | 31.3% | 8/293 |
| Optimal ROC | 1000 IU/L | 0.805 | 71.4% | 94.9% | 96.6% | 62.5% | 8/293 | ||
| Yu et al. [51] | Amylase | 3 | 544 IU/L | 0.778 | 66.7% | 83.8% | NR | NR | 10/99 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Mooij, C.M.; Maassen van den Brink, M.; Merry, A.; Tweed, T.; Stoot, J. Systematic Review of the Role of Biomarkers in Predicting Anastomotic Leakage Following Gastroesophageal Cancer Surgery. J. Clin. Med. 2019, 8, 2005. https://doi.org/10.3390/jcm8112005
de Mooij CM, Maassen van den Brink M, Merry A, Tweed T, Stoot J. Systematic Review of the Role of Biomarkers in Predicting Anastomotic Leakage Following Gastroesophageal Cancer Surgery. Journal of Clinical Medicine. 2019; 8(11):2005. https://doi.org/10.3390/jcm8112005
Chicago/Turabian Stylede Mooij, Cornelis Maarten, Martijn Maassen van den Brink, Audrey Merry, Thais Tweed, and Jan Stoot. 2019. "Systematic Review of the Role of Biomarkers in Predicting Anastomotic Leakage Following Gastroesophageal Cancer Surgery" Journal of Clinical Medicine 8, no. 11: 2005. https://doi.org/10.3390/jcm8112005
APA Stylede Mooij, C. M., Maassen van den Brink, M., Merry, A., Tweed, T., & Stoot, J. (2019). Systematic Review of the Role of Biomarkers in Predicting Anastomotic Leakage Following Gastroesophageal Cancer Surgery. Journal of Clinical Medicine, 8(11), 2005. https://doi.org/10.3390/jcm8112005