Predicting Long-Term Health-Related Quality of Life after Bariatric Surgery Using a Conventional Neural Network: A Study Based on the Scandinavian Obesity Surgery Registry


Abstract
:1. Introduction
2. Material and Methods
2.1. Patients and Features
2.2. Feature Scaling
2.3. Conventional Neural Network
2.4. Model Validation and Evaluation
2.5. Software and Hardware
3. Results
3.1. Descriptive Analysis of the Data
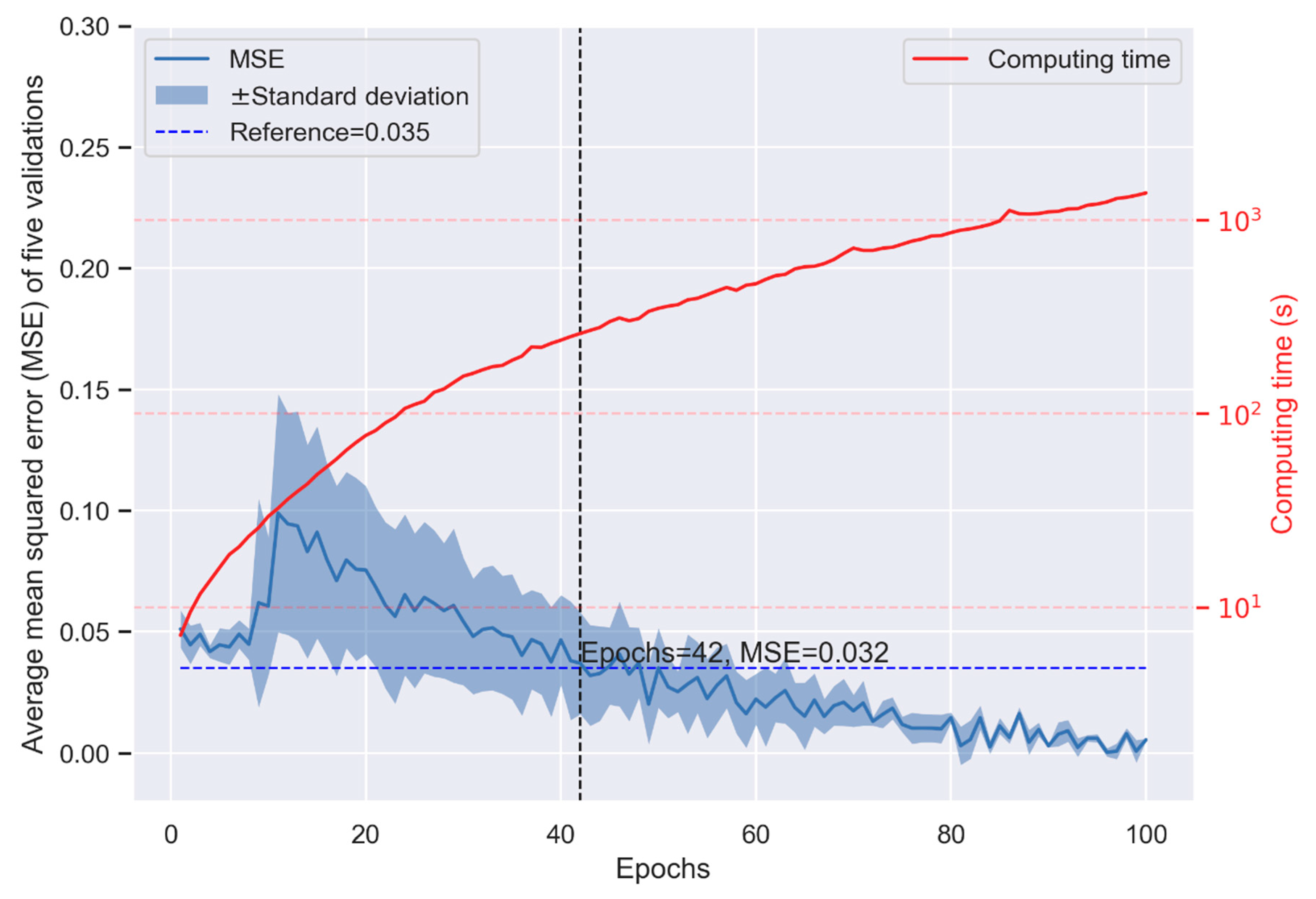
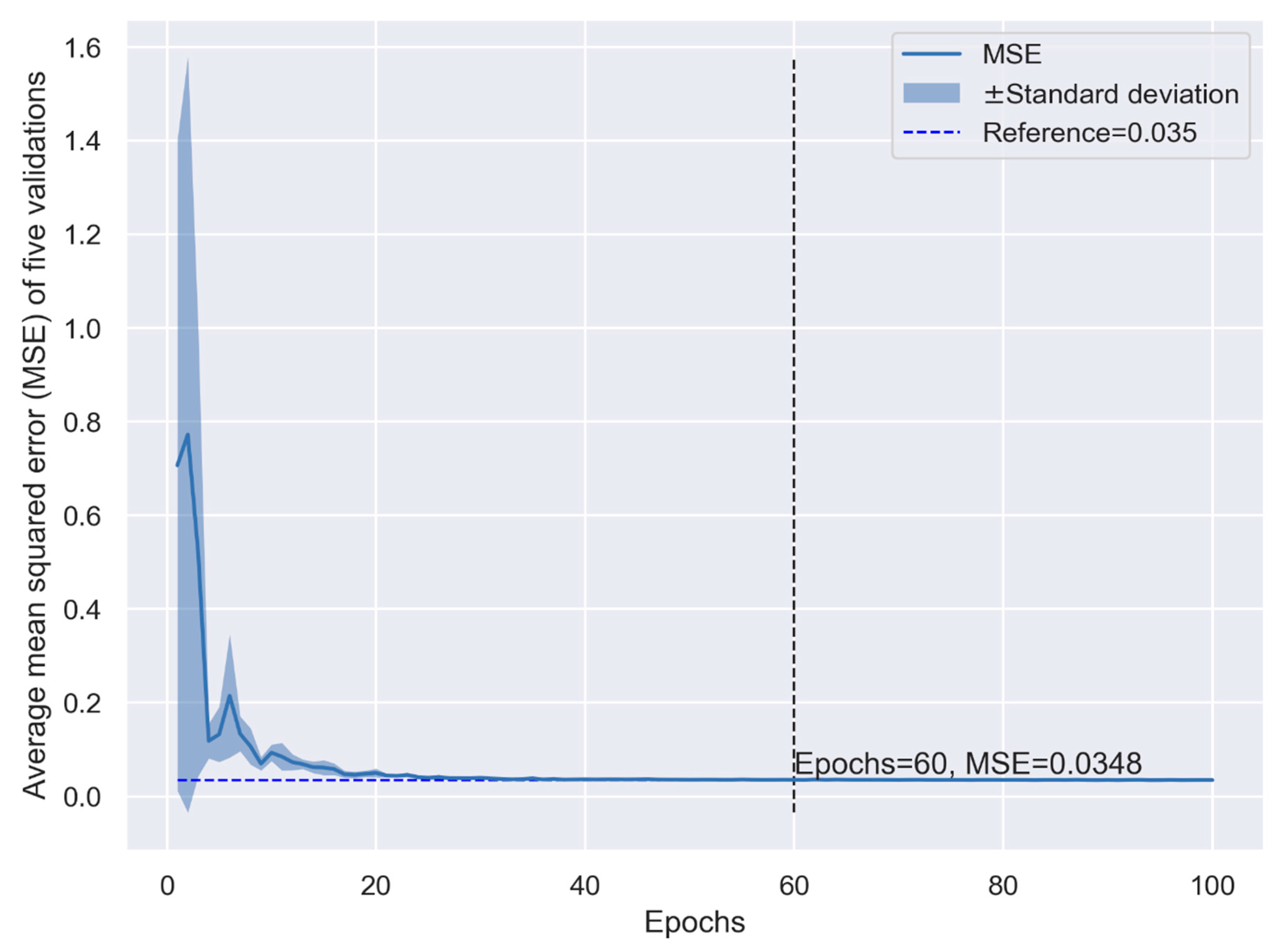
3.2. Performance of the CNN Model in the K-Fold Cross-Validation
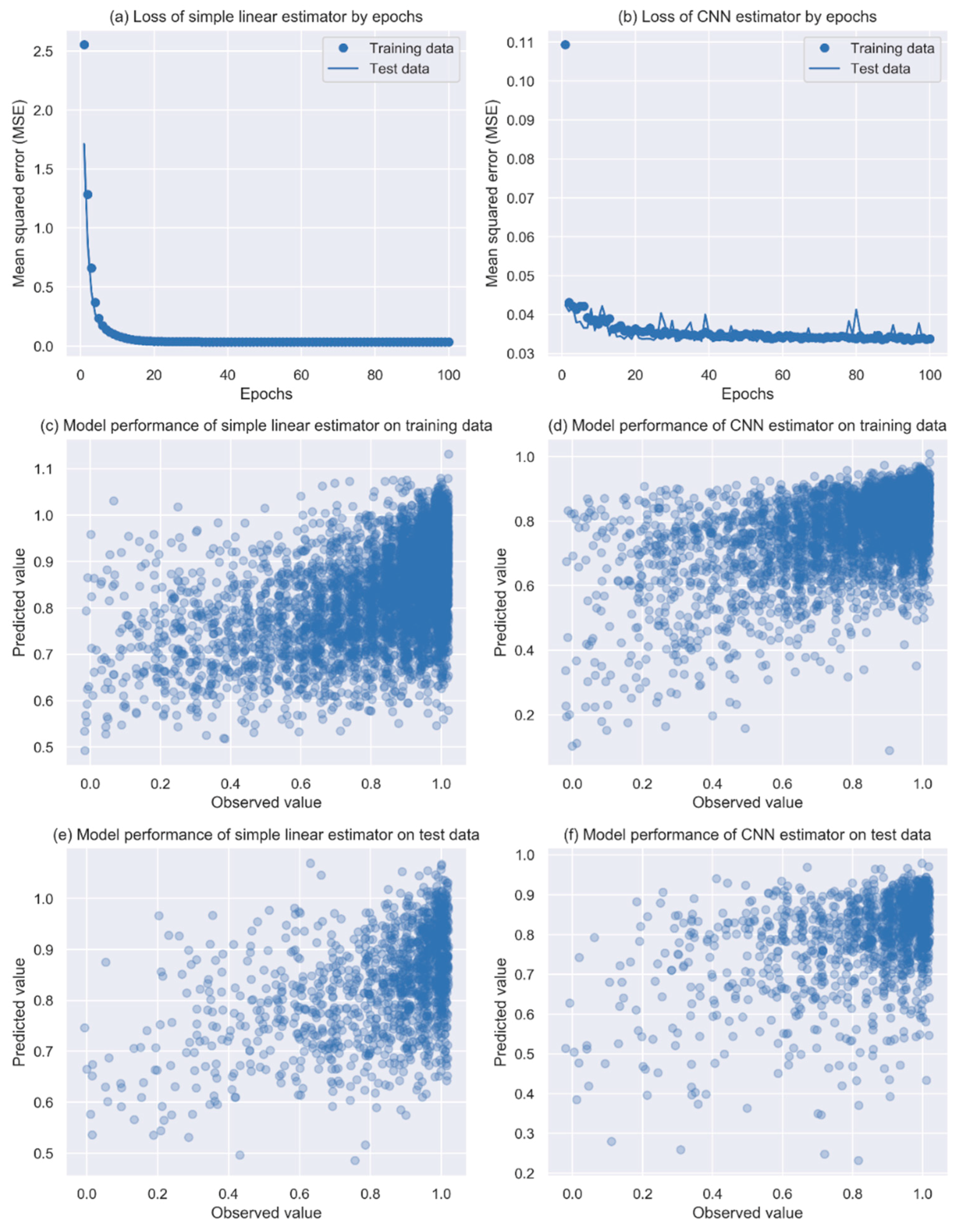
3.3. Performance of the CNN Model in the Final Evaluation
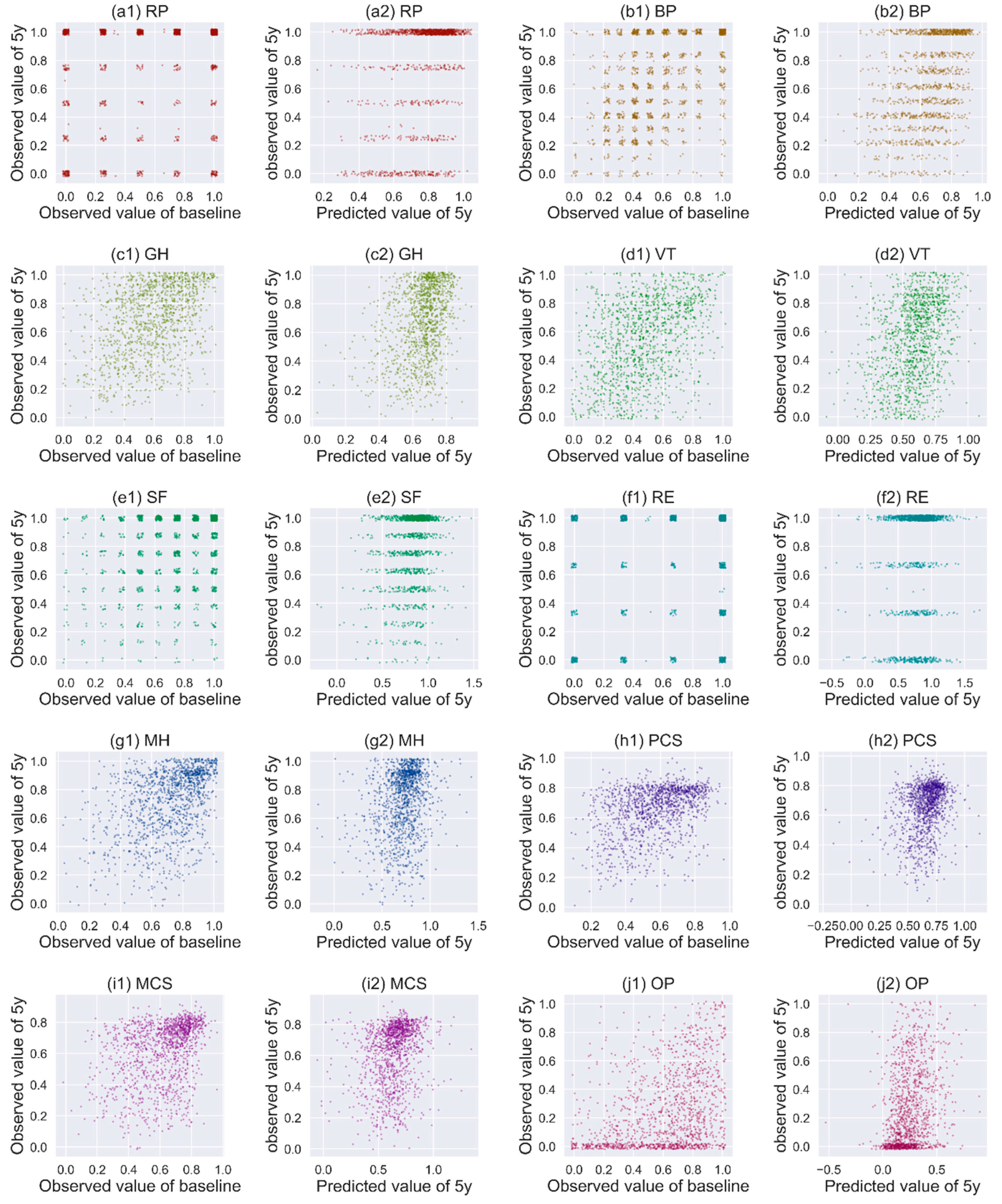
3.4. Performance of CNN in Predicting Other HRQoL Measures
3.5. Sensitivity Analysis and Computing Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kopelman, P.G.; Caterson, I.D.; Dietz, W.H. Clinical Obesity in Adults and Children; John Wiley & Sons: New York, NY, USA, 2009. [Google Scholar]
- Organization, W.H. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Prospective Studies Collaboration; Whitlock, G.; Lewington, S.; Sherliker, P.; Clarke, R.; Emberson, J.; Halsey, J.; Qizilbash, N.; Collins, R.; Peto, R. Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wawok, P. Evaluation of Quality of Life of patient with obesity after surgical procedure. Eur. J. Med. Res. 2009, 14, 114. [Google Scholar]
- Kawatkar, A.A.; Nichol, M.B. The Impact of Obesity on Medical Expenditure and Health Related Quality of Life. Value Health 2009, 12, A134. [Google Scholar] [CrossRef] [Green Version]
- Kolotkin, R.L.; Williams, V.S.L.; Ervin, C.M.; Williams, N.; Meincke, H.H.; Qin, S.S.; Smith, L.V.; Fehnel, S.E. Validation of a new measure of quality of life in obesity trials: Impact of Weight on Quality of Life-Lite Clinical Trials Version. Clin. Obes. 2019, 9, e12310. [Google Scholar] [CrossRef]
- Dreber, H.; Thorell, A.; Reynisdottir, S.; Hemmingsson, E. Health-Related Quality of Life 5Years After Roux-en-Y Gastric Bypass in Young (18-25Years) Versus Older (26Years) Adults: A Scandinavian Obesity Surgery Registry Study. Obes. Surg. 2019, 29, 434–443. [Google Scholar] [CrossRef]
- Consensus Development Conference Panel. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann. Intern. Med. 1991, 115, 956–961. [Google Scholar] [CrossRef]
- Mazer, L.M.; Azagury, D.E.; Morton, J.M. Quality of Life After Bariatric Surgery. Curr. Obes. Rep. 2017, 6, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.R.; Aasprang, A.; Karlsen, T.I.; Natvig, G.K.; Vage, V.; Kolotkin, R.L. Health-related quality of life after bariatric surgery: A systematic review of prospective long-term studies. Surg. Obes. Relat. Dis. 2015, 11, 466–473. [Google Scholar] [CrossRef] [Green Version]
- Wimmelmann, C.L.; Dela, F.; Mortensen, E.L. Psychological predictors of mental health and health-related quality of life after bariatric surgery: A review of the recent research. Obes. Res. Clin. Pract. 2014, 8, e314–e324. [Google Scholar] [CrossRef]
- Masheb, R.M.; White, M.A.; Toth, C.M.; Burke-Martindale, C.H.; Rothschild, B.; Grilo, C.M. The prognostic significance of depressive symptoms for predicting quality of life 12 months after gastric bypass. Compr. Psychiatry 2007, 48, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Hedenbro, J.L.; Naslund, E.; Boman, L.; Lundegardh, G.; Bylund, A.; Ekelund, M.; Laurenius, A.; Moller, P.; Olbers, T.; Sundbom, M.; et al. Formation of the Scandinavian Obesity Surgery Registry, SOReg. Obes. Surg. 2015, 25, 1893–1900. [Google Scholar] [CrossRef] [PubMed]
- Matsugu, M.; Mori, K.; Mitari, Y.; Kaneda, Y. Subject independent facial expression recognition with robust face detection using a convolutional neural network. Neural Netw. 2003, 16, 555–559. [Google Scholar] [CrossRef]
- Zeiler, M.D. ADADELTA: An adaptive learning rate method. arXiv 2012, arXiv:1212.5701. [Google Scholar]
- Raschka, S.; Mirjalili, V. Python Machine Learning; Packt Publishing Ltd.: Birmingham, UK, 2017. [Google Scholar]
- Wilson, A.C.; Roelofs, R.; Stern, M.; Srebro, N.; Recht, B. The Marginal Value of Adaptive Gradient Methods in Machine Learning. Adv. Neural Inf. 2017, 30, 4148–4158. [Google Scholar]
- Lee, S.K.; Son, Y.J.; Kim, J.; Kim, H.G.; Lee, J.I.; Kang, B.Y.; Cho, H.S.; Lee, S. Prediction Model for Health-Related Quality of Life of Elderly with Chronic Diseases using Machine Learning Techniques. Healthc. Inf. Res. 2014, 20, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Rana, M.L.; Verma, K.; Singh, N.; Sharma, A.K.; Maria, A.K.; Dhaliwal, G.S.; Khaira, H.K.; Saini, S. PrediQt-Cx: Post treatment health related quality of life prediction model for cervical cancer patients. PLoS ONE 2014, 9, e89851. [Google Scholar] [CrossRef] [Green Version]
- Persson, P.-V.; Rietz, H. Predicting and Analyzing Osteoarthritis Patient Outcomes with Machine Learning; Lund University: Lund, Sweden, 2017. [Google Scholar]
- Tao, W.; Holmberg, D.; Naslund, E.; Naslund, I.; Mattsson, F.; Lagergren, J.; Ljung, R. Validation of Obesity Surgery Data in the Swedish National Patient Registry and Scandinavian Obesity Registry (SOReg). Obes. Surg. 2016, 26, 1750–1756. [Google Scholar] [CrossRef]
- Hell, E.; Miller, K.A.; Moorehead, M.K.; Norman, S. Evaluation of health status and quality of life after bariatric surgery: Comparison of standard Roux-en-Y gastric bypass, vertical banded gastroplasty and laparoscopic adjustable silicone gastric banding. Obes. Surg. 2000, 10, 214–219. [Google Scholar] [CrossRef]
- Dymek, M.P.; Le Grange, D.; Neven, K.; Alverdy, J. Quality of life after gastric bypass surgery: A cross-sectional study. Obes. Res. 2002, 10, 1135–1142. [Google Scholar] [CrossRef] [Green Version]
- Major, P.; Matlok, M.; Pedziwiatr, M.; Migaczewski, M.; Budzynski, P.; Stanek, M.; Kisielewski, M.; Natkaniec, M.; Budzynski, A. Quality of Life After Bariatric Surgery. Obes. Surg. 2015, 25, 1703–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Liu, S.J.; Kingsbury, P.; Sohn, S.; Storlie, C.B.; Habermann, E.B.; Naessens, J.M.; Larson, D.W.; Liu, H.F. Deep learning and alternative learning strategies for retrospective real-world clinical data. NPJ Digit. Med. 2019, 2, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.Y.; Hung, C.K.; Chang, Y.Y.; Tai, C.M.; Lin, J.T.; Wang, J.D. Health-related quality of life in adult patients with morbid obesity coming for bariatric surgery. Obes. Surg. 2010, 20, 1121–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolotkin, R.L.; Crosby, R.D.; Williams, G.R. Health-related quality of life varies among obese subgroups. Obes. Res. 2002, 10, 748–756. [Google Scholar] [CrossRef] [PubMed]
- White, M.A.; O’Neil, P.M.; Kolotkin, R.L.; Byrne, T.K. Gender, race, and obesity-related quality of life at extreme levels of obesity. Obes. Res. 2004, 12, 949–955. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preoperative | Five Years after Bariatric Surgery | |||
|---|---|---|---|---|
| Original | Scaled | Original | Scaled | |
| Age (year) | 42.7 (11.0) | 0.494 (0.197) | 47.7 (11.0) | 0.494 (0.197) |
| BMI (kg/m2) | 42.3 (5.2) | 0.241 (0.103) | 30.3 (5.2) | 0.358 (0.127) |
| Female | 5259 (77%) | NA | 5259 (77%) | NA |
| SAS | 680 (10%) | NA | NA | NA |
| Hypertension | 1851 (27%) | NA | NA | NA |
| Diabetes | 990 (15%) | NA | NA | NA |
| Depression | 884 (13%) | NA | NA | NA |
| Dyslipidemia | 747 (11%) | NA | NA | NA |
| PF | 61.6 (21.9) | 0.616 (0.219) | 84.2 (20.7) | 0.842 (0.207) |
| RP | 60.2 (38.9) | 0.602 (0.389) | 77.8 (36.6) | 0.778 (0.366) |
| BP | 56.0 (26.8) | 0.560 (0.268) | 65.1 (30.8) | 0.651 (0.308) |
| GH | 58.2 (21.4) | 0.582 (0.214) | 68.0 (24.7) | 0.680 (0.247) |
| VT | 47.3 (23.0) | 0.473 (0.230) | 54.5 (26.9) | 0.545 (0.269) |
| SF | 74.8 (26.1) | 0.748 (0.261) | 79.5(26.5) | 0.795 (0.265) |
| RE | 75.9 (36.2) | 0.759 (0.362) | 76.7 (37.9) | 0.767 (0.379) |
| MH | 71.5 (19.4) | 0.715 (0.194) | 72.0 (23.0) | 0.720 (0.230) |
| PCS | 38.3 (10.7) | 0.567 (0.177) | 47.6 (11.1) | 0.653 (0.163) |
| MCS | 46.8 (11.7) | 0.621 (0.172) | 44.6 (13.8) | 0.621 (0.192) |
| OP | 61.0 (26.3) | 0.610 (0.263) | 25.6 (27.4) | 0.256 (0.274) |
| HRQoL Measure | Training Data | Test Data | ||
|---|---|---|---|---|
| CNN Model | Linear Regression Model | CNN Model | Linear Regression Model | |
| PF | 0.0316 | 0.0329 | 0.0350 | 0.0343 |
| RP | 0.1078 | 0.1178 | 0.1324 | 0.1211 |
| BP | 0.0604 | 0.0763 | 0.0898 | 0.0772 |
| GH | 0.0280 | 0.0497 | 0.0618 | 0.0508 |
| VT | 0.0303 | 0.0572 | 0.0914 | 0.0625 |
| SF | 0.0213 | 0.0600 | 0.0995 | 0.0588 |
| RE | 0.0393 | 0.1275 | 0.2118 | 0.1269 |
| MH | 0.0119 | 0.0427 | 0.0807 | 0.0416 |
| PCS | 0.0087 | 0.0210 | 0.0333 | 0.0219 |
| MCS | 0.0075 | 0.0301 | 0.0584 | 0.0305 |
| OP | 0.0450 | 0.0625 | 0.0750 | 0.0608 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, Y.; Raoof, M.; Montgomery, S.; Ottosson, J.; Näslund, I. Predicting Long-Term Health-Related Quality of Life after Bariatric Surgery Using a Conventional Neural Network: A Study Based on the Scandinavian Obesity Surgery Registry. J. Clin. Med. 2019, 8, 2149. https://doi.org/10.3390/jcm8122149
Cao Y, Raoof M, Montgomery S, Ottosson J, Näslund I. Predicting Long-Term Health-Related Quality of Life after Bariatric Surgery Using a Conventional Neural Network: A Study Based on the Scandinavian Obesity Surgery Registry. Journal of Clinical Medicine. 2019; 8(12):2149. https://doi.org/10.3390/jcm8122149
Chicago/Turabian StyleCao, Yang, Mustafa Raoof, Scott Montgomery, Johan Ottosson, and Ingmar Näslund. 2019. "Predicting Long-Term Health-Related Quality of Life after Bariatric Surgery Using a Conventional Neural Network: A Study Based on the Scandinavian Obesity Surgery Registry" Journal of Clinical Medicine 8, no. 12: 2149. https://doi.org/10.3390/jcm8122149
APA StyleCao, Y., Raoof, M., Montgomery, S., Ottosson, J., & Näslund, I. (2019). Predicting Long-Term Health-Related Quality of Life after Bariatric Surgery Using a Conventional Neural Network: A Study Based on the Scandinavian Obesity Surgery Registry. Journal of Clinical Medicine, 8(12), 2149. https://doi.org/10.3390/jcm8122149