The Incidence of Chronic Kidney Disease Three Years after Non-Severe Acute Kidney Injury in Critically Ill Patients: A Single-Center Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Acute Kidney Injury Classification
2.4. Exposure Variables
2.5. Long-Term Incidence of CKD at Three Years
2.6. Other Outcomes
2.7. Statistical Analysis
3. Results
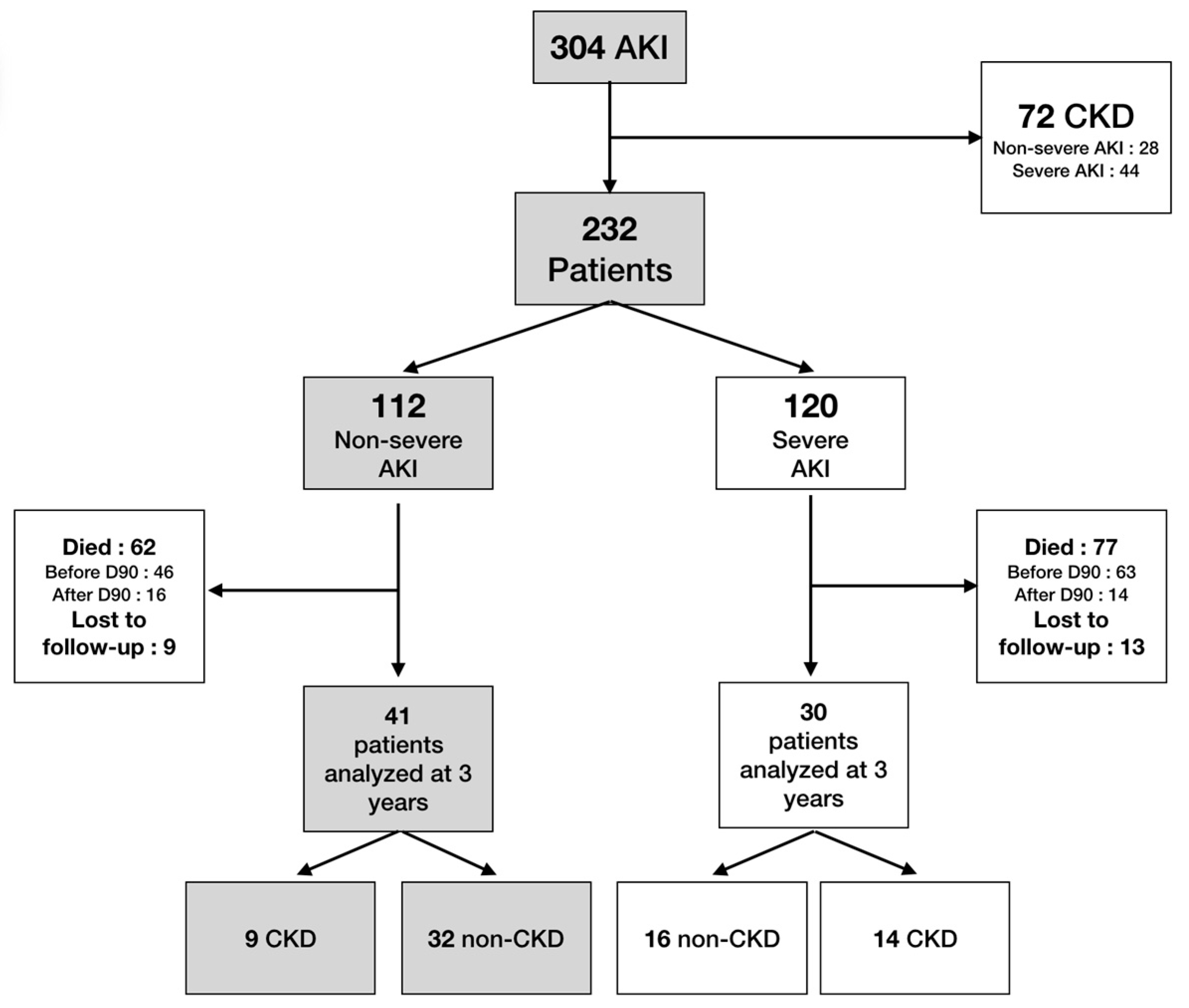
3.1. Participants
3.2. Follow-Up
3.3. Primary Outcome: Long-Term Incidence of CKD at Three Years
3.4. Secondary Outcomes
3.4.1. Risk Factors for CKD at Three Years
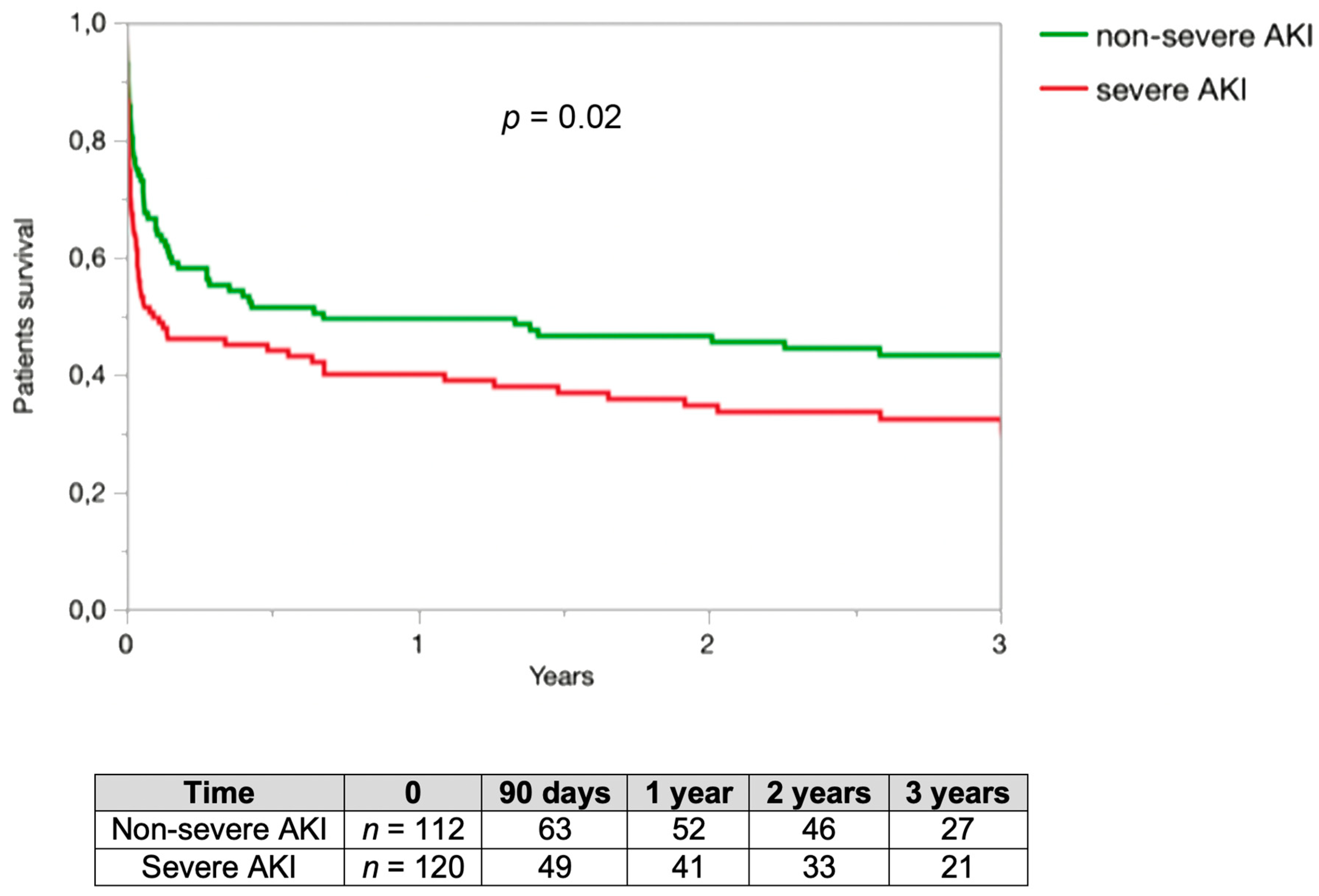
3.4.2. Patients Survival
3.4.3. Renal Specialist Following
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Hoste, E.A.J.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef] [PubMed]
- Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.S.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; et al. Beginning and Ending Supportive Therapy for the Kidney, I. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA J. Am. Med Assoc. 2005, 294, 813–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horkan, C.M.; Purtle, S.W.; Mendu, M.L.; Moromizato, T.; Gibbons, F.K.; Christopher, K.B. The Association of Acute Kidney Injury in the Critically Ill and Postdischarge Outcomes. Crit. Care Med. 2015, 43, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Delannoy, B.; Floccard, B.; Thiolliere, F.; Kaaki, M.; Badet, M.; Rosselli, S.; Ber, C.E.; Saez, A.; Flandreau, G.; Guérin, C. Six-month outcome in acute kidney injury requiring renal replacement therapy in the ICU: A multicentre prospective study. Intensive Care Med. 2009, 35, 1907–1915. [Google Scholar] [CrossRef]
- Schiffl, H.; Fischer, R. Five-year outcomes of severe acute kidney injury requiring renal replacement therapy. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2008, 23, 2235–2241. [Google Scholar] [CrossRef] [Green Version]
- Gammelager, H.; Christiansen, C.F.; Johansen, M.B.; Tønnesen, E.; Jespersen, B.; Sørensen, H.T. Five-year risk of end-stage renal disease among intensive care patients surviving dialysis-requiring acute kidney injury: A nationwide cohort study. Crit. Care 2013, 17, R145. [Google Scholar] [CrossRef] [Green Version]
- Lafrance, J.-P.; Miller, D.R. Acute kidney injury associates with increased long-term mortality. J. Am. Soc. Nephrol. JASN 2010, 21, 345–352. [Google Scholar] [CrossRef]
- Heung, M.; Steffick, D.E.; Zivin, K.; Gillespie, B.W.; Banerjee, T.; Hsu, C.-Y.; Powe, N.R.; Pavkov, M.E.; Williams, D.E.; Saran, R.; et al. Centers for Disease Control and Prevention CKD Surveillance Team Acute Kidney Injury Recovery Pattern and Subsequent Risk of CKD: An Analysis of Veterans Health Administration Data. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2016, 67, 742–752. [Google Scholar] [CrossRef]
- Tomlinson, L.A.; Riding, A.M.; Payne, R.A.; Abel, G.A.; Tomson, C.R.; Wilkinson, I.B.; Roland, M.O.; Chaudhry, A.N. The accuracy of diagnostic coding for acute kidney injury in England—A single centre study. BMC Nephrol. 2013, 14, 58. [Google Scholar] [CrossRef] [Green Version]
- Sawhney, S.; Fraser, S.D. Epidemiology of AKI: Utilizing Large Databases to Determine the Burden of AKI. Adv. Chronic Kidney Dis. 2017, 24, 194–204. [Google Scholar] [CrossRef] [Green Version]
- Palevsky, P.M.; Liu, K.D.; Brophy, P.D.; Chawla, L.S.; Parikh, C.R.; Thakar, C.V.; Tolwani, A.J.; Waikar, S.S.; Weisbord, S.D. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for acute kidney injury. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2013, 61, 649–672. [Google Scholar] [CrossRef] [PubMed]
- Horne, K.L.; Shardlow, A.; Taal, M.W.; Selby, N.M. Long Term Outcomes after Acute Kidney Injury: Lessons from the ARID Study. Nephron 2015, 131, 102–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rewa, O.; Bagshaw, S.M. Acute kidney injury-epidemiology, outcomes and economics. Nat. Publ. Group 2014, 10, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Gaudry, S.; Hajage, D.; Schortgen, F.; Martin-Lefevre, L.; Pons, B.; Boulet, E.; Boyer, A.; Chevrel, G.; Lerolle, N.; Carpentier, D.; et al. AKIKI Study Group Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit. N. Engl. J. Med. 2016, 375, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Gansevoort, R.T.; Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J. Chronic Kidney Disease Prognosis Consortium Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011, 80, 93–104. [Google Scholar] [CrossRef] [Green Version]
- Heung, M.; Chawla, L.S. Acute kidney injury: Gateway to chronic kidney disease. Nephron Clin. Pract. 2014, 127, 30–34. [Google Scholar] [CrossRef]
- O’Seaghdha, C.M.; Lyass, A.; Massaro, J.M.; Meigs, J.B.; Coresh, J.; D’Agostino, R.B.; Astor, B.C.; Fox, C.S. A risk score for chronic kidney disease in the general population. Am. J. Med. 2012, 125, 270–277. [Google Scholar] [CrossRef] [Green Version]
- McMahon, G.M.; Preis, S.R.; Hwang, S.-J.; Fox, C.S. Mid-adulthood risk factor profiles for CKD. J. Am. Soc. Nephrol. JASN 2014, 25, 2633–2641. [Google Scholar] [CrossRef] [Green Version]
- Tangri, N.; Grams, M.E.; Levey, A.S.; Coresh, J.; Appel, L.J.; Astor, B.C.; Chodick, G.; Collins, A.J.; Djurdjev, O.; Elley, C.R.; et al. CKD Prognosis Consortium Multinational Assessment of Accuracy of Equations for Predicting Risk of Kidney Failure: A Meta-analysis. JAMA J. Am. Med Assoc. 2016, 315, 164–174. [Google Scholar] [CrossRef] [Green Version]
- Jones, J.; Holmen, J.; De Graauw, J.; Jovanovich, A.; Thornton, S.; Chonchol, M. Association of complete recovery from acute kidney injury with incident CKD stage 3 and all-cause mortality. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2012, 60, 402–408. [Google Scholar] [CrossRef] [Green Version]
- Bucaloiu, I.D.; Kirchner, H.L.; Norfolk, E.R.; Hartle, J.E.; Perkins, R.M. Increased risk of death and de novo chronic kidney disease following reversible acute kidney injury. Kidney Int. 2012, 81, 477–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellum, J.A.; Sileanu, F.E.; Bihorac, A.; Hoste, E.A.J.; Chawla, L.S. Recovery after Acute Kidney Injury. Am. J. Respir. Crit. Care Med. 2017, 195, 784–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenberghe, W.; Hoste, E.A.J. Acute kidney injury survivors should have long-term follow-up. Crit. Care 2014, 18, 703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonelli, M.; Muntner, P.; Lloyd, A.; Manns, B.J.; Klarenbach, S.; Pannu, N.; James, M.T.; Hemmelgarn, B.R. Alberta Kidney Disease Network Risk of coronary events in people with chronic kidney disease compared with those with diabetes: A population-level cohort study. Lancet 2012, 380, 807–814. [Google Scholar] [CrossRef]
- Shiao, C.-C.; Wu, P.-C.; Huang, T.-M.; Lai, T.-S.; Yang, W.-S.; Wu, C.-H.; Lai, C.-F.; Wu, V.-C.; Chu, T.-S.; Wu, K.-D. National Taiwan University Hospital Study Group on Acute Renal Failure (NSARF) and the Taiwan Consortium for Acute Kidney Injury and Renal Diseases (CAKs) Long-term remote organ consequences following acute kidney injury. Crit. Care 2015, 19, 438. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics of Patients | Patients Enrolled n = 232 (%) | Non-Severe AKI n = 112 (%) | Severe AKI n = 120 (%) | p Value |
|---|---|---|---|---|
| Males | 142 (63) | 71 (63) | 71 (59) | 0.5 |
| Age | 62 ± 16 | 62 ± 16 | 62 ± 16 | 0.8 |
| Smoker | 97 (42) | 50 (45) | 47 (39) | 0.4 |
| Hypertension | 115 (50) | 62 (55) | 53 (44) | 0.1 |
| Diabetes | 55 (24) | 31 (28) | 24 (20) | 0.2 |
| Heart failure | 42 (18) | 20 (18) | 22 (18) | 0.9 |
| Stroke | 21 (9) | 12 (11) | 9 (8) | 0.4 |
| PAD | 17 (7) | 6 (5) | 11 (9) | 0.3 |
| IHD | 33 (14) | 19 (17) | 14 (11) | 0.2 |
| Basal SCr | 78 ± 18 | 78 ± 19 | 77 ± 17 | 0.6 |
| Sepsis | 118 (51) | 56 (50) | 62 (52) | 0.8 |
| Contrast agent | 55 (24) | 26 (23) | 29 (24) | 0.9 |
| Aminosid use | 84 (36) | 43 (38) | 42 (35) | 0.6 |
| NIV or HFNC | 192 (83) | 6 (5) | 5 (4) | 0.7 |
| Orotracheal intubation | 192 (83) | 92 (82) | 100 (83) | 0.8 |
| Catecholamine use | 191 (82) | 89 (79) | 102 (85) | 0.3 |
| SAPS II | 62 ± 19 | 59 ± 17 | 65 ± 20 | 0.01 |
| Maximal SCr (µmol/L) | 266 ± 181 | 153 ± 56 | 371 ± 195 | <0.001 |
| AKI stage: | ||||
| 1 | 62 (27) | 62 (55) | 0 (0) | |
| 2 | 50 (21) | 50 (45) | 0 (0) | |
| 3 | 120 (52) | 120 (100) | ||
| RRT | 0 | 73 (61) | ||
| CVVHD | 0 | 57 (48) | ||
| IHH | 0 | 16 (13) | ||
| Renal recovery | 90/141 (64) | 68/78 (87) | 22/63 (35) | <0.001 |
| ICU length of stay (days) | 9 ± 10 | 9 ± 10 | 9 ± 11 | 0.9 |
| Intra-ICU deaths | 91 (39) | 34 (30) | 57 (48) | 0.01 |
| Hospital length of stay (days) | 36 ± 100 | 37 ± 109 | 34 ± 91 | 0.8 |
| CKD Stages At 3 Years | Non-Severe AKI at Inclusion n = 41 (%) | Severe AKI at Inclusion n = 30 (%) | Total n = 71 (%) |
|---|---|---|---|
| CKD3 (60 < eGFR < 30) | 7 (17) | 10 (33) | 17 (24) |
| CKD4 (30 < eGFR < 15) | 2 (5) | 1 (3) | 3 (4) |
| CKD5 (eGFR < 15)) | 0 | 3 (10) | 3 (4) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Odds Ratio eGFR < 60 (mL/min/1.73 m2) | Confidence Interval 5% | Odds Ratio eGFR < 60 (mL/min/1.73 m2) | Confidence Interval 5% | |
| Male | 0.5 | (0.2–1.4) | ||
| Age | 1.1 | (0.99–1.2) | ||
| Smoker | 1.8 | (0.6–4.8) | ||
| Hypertension | 3.5 | (1.2–10.5) | ||
| Diabetes | 3.6 | (1.2–10.3) | 3.3 | (1.3–8.3) |
| Heart failure | 2.3 | (0.6–9.1) | ||
| Stroke | 0.3 | (0.04–2.7) | ||
| PAD | 2.1 | (0.3–16.3) | ||
| IHD | 1.8 | (0.4–7.3) | ||
| Sepsis | 1.7 | (0.6–4.6) | ||
| Contrast agent | 1.3 | (0.4–3.8) | ||
| Aminosid use | 2.1 | (0.8–5.8) | ||
| Orotracheal intubation | 0.7 | (0.2–2.1) | ||
| Vasopressor | 1.6 | (0.4–6.5) | ||
| SAPS II | 1.5 | (0.2–12.9) | ||
| Length of hospitalization in ICU (days) | 0.97 | (0.94–1.04) | ||
| Hospital length of stay (days) | 0.99 | (0.98–1.01) | ||
| Maximum SCr | 1.007 | (1.002–1.01) | ||
| Non-severe AKI | 1 | 1 | ||
| Severe AKI | 3 | (1.1–8.5) | 1.96 | (0.8–5) |
| AKI stage 1 | 0.2 | (0.05–0.4) | ||
| AKI stage 2 | 0.5 | (0.2–1.5) | ||
| AKI stage 3 | 1 | |||
| RRT | 2.7 | (0.9–8.2) | ||
| CVVHD | 0.8 | (0.2–3.1) | ||
| Readmission at hospital during follow-up | 1.5 | (0.5–4.3) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubin, S.; Orieux, A.; Clouzeau, B.; Rigothier, C.; Combe, C.; Gruson, D.; Boyer, A. The Incidence of Chronic Kidney Disease Three Years after Non-Severe Acute Kidney Injury in Critically Ill Patients: A Single-Center Cohort Study. J. Clin. Med. 2019, 8, 2215. https://doi.org/10.3390/jcm8122215
Rubin S, Orieux A, Clouzeau B, Rigothier C, Combe C, Gruson D, Boyer A. The Incidence of Chronic Kidney Disease Three Years after Non-Severe Acute Kidney Injury in Critically Ill Patients: A Single-Center Cohort Study. Journal of Clinical Medicine. 2019; 8(12):2215. https://doi.org/10.3390/jcm8122215
Chicago/Turabian StyleRubin, Sébastien, Arthur Orieux, Benjamin Clouzeau, Claire Rigothier, Christian Combe, Didier Gruson, and Alexandre Boyer. 2019. "The Incidence of Chronic Kidney Disease Three Years after Non-Severe Acute Kidney Injury in Critically Ill Patients: A Single-Center Cohort Study" Journal of Clinical Medicine 8, no. 12: 2215. https://doi.org/10.3390/jcm8122215
APA StyleRubin, S., Orieux, A., Clouzeau, B., Rigothier, C., Combe, C., Gruson, D., & Boyer, A. (2019). The Incidence of Chronic Kidney Disease Three Years after Non-Severe Acute Kidney Injury in Critically Ill Patients: A Single-Center Cohort Study. Journal of Clinical Medicine, 8(12), 2215. https://doi.org/10.3390/jcm8122215