Cardiac Biomarkers in the Emergency Department: The Role of Soluble ST2 (sST2) in Acute Heart Failure and Acute Coronary Syndrome—There is Meat on the Bone

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
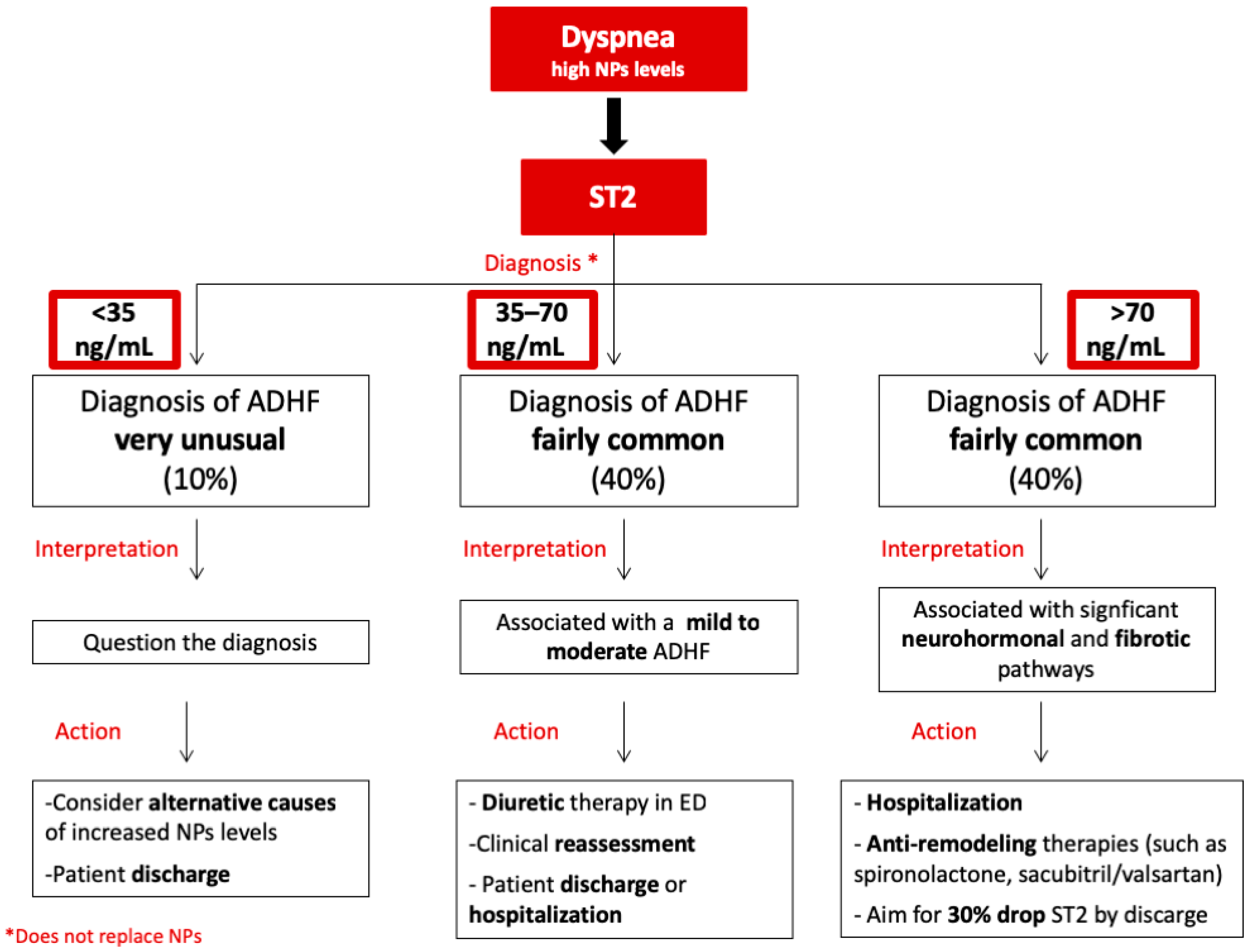
2. sST2 in Acute Decompensated Heart Failure (ADHF)
3. ST2 in Acute Myocardial Infarction
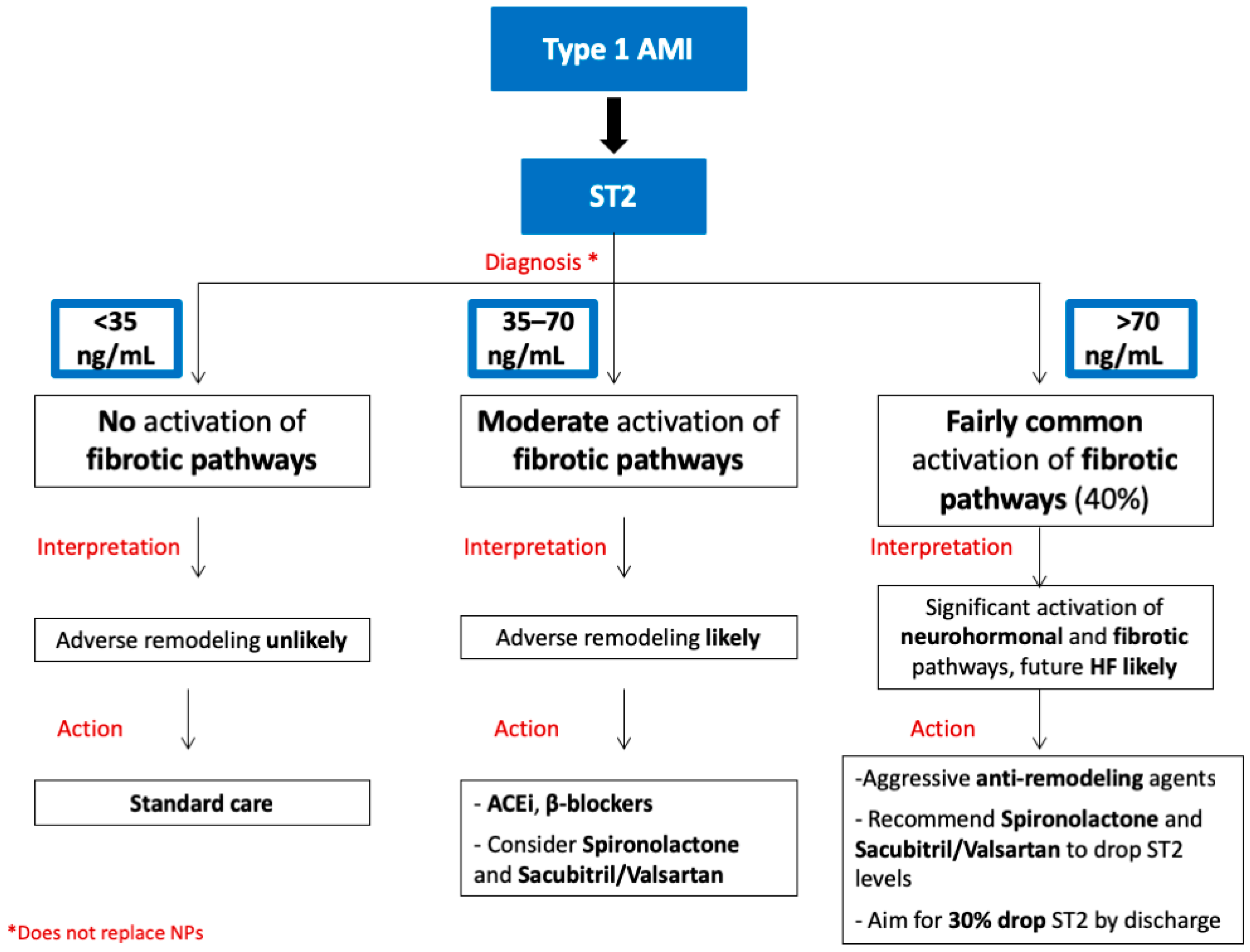
3.1. sST2 and Type 1 Myocardial Infarction
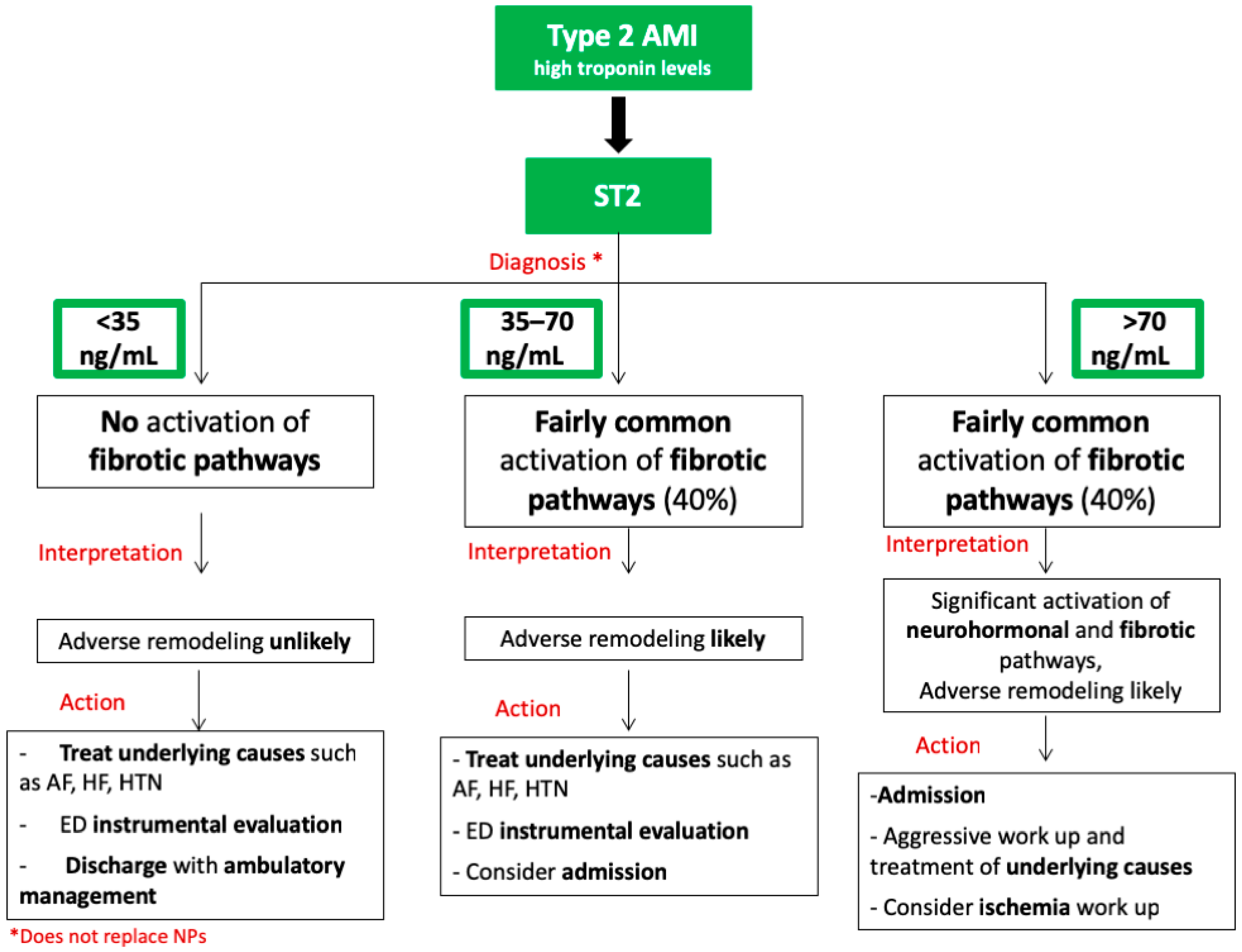
3.2. sST2 and Type 2 Myocardial Infarction
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Iwahana, H.; Yanagisawa, K.; Ito-Kosaka, A.; Kuroiwa, K.; Tago, K.; Komatsu, N.; Katashima, R.; Itakura, M.; Tominaga, S. Different promoter usage and multiple transcription initiation sites of the interleukin-1 receptor-related human ST2 gene in UT-7 and TM12 cells. Eur. J. Biochem. 1999, 264, 397–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, N.T. Martin MU Interleukin 33 is a guardian of barriers and a local alarmin. Nat. Immunol. 2016, 17, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.M.; Liew, F.Y. The IL-33/ST2 pathway—A new therapeutic target in cardiovascular disease. Pharmacol. Ther. 2011, 131, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, J.; Owyang, A.; Oldham, E.; Song, Y.; Murphy, E.; McClanahan, T.K.; Zurawski, G.; Moshrefi, M.; Qin, J.; Li, X.; et al. IL-33, an Interleukin-1-like Cytokine that Signals via the IL-1 Receptor-Related Protein ST2 and Induces T Helper Type 2-Associated Cytokines. Immunity 2005, 23, 479–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, A.M.; Xu, D.; Asquith, D.L.; Denby, L.; Li, Y.; Sattar, N.; Baker, A.H.; McInnes, I.B.; Liew, F.Y. IL-33 reduces the development of atherosclerosis. J. Exp. Med. 2008, 205, 339–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, A.M.; Asquith, D.L.; Hueber, A.J.; Anderson, L.A.; Holmes, W.M.; McKenzie, A.N.; Xu, D.; Sattar, N.; McInnes, I.B.; Liew, F.Y. Interleukin-33 Induces Protective Effects in Adipose Tissue Inflammation During Obesity in Mice. Circ. Res. 2010, 107, 650–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veeraveedu, P.T.; Sanada, S.; Okuda, K.; Fu, H.Y.; Matsuzaki, T.; Araki, R.; Yamato, M.; Yasuda, K.; Sakata, Y.; Yoshimoto, T.; et al. Ablation of IL-33 gene exacerbate myocardial remodeling in mice with heart failure induced by mechanical stress. Biochem. Pharmacol. 2017, 138, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Seppanen, E.; Patel, J.; Rodero, M.P.; Khosrotehrani, K. ST2 receptor invalidation maintains wound inflammation, delays healing and increases fibrosis. Exp. Dermatol. 2016, 25, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Villacorta, H.; Maisel, A.S.; Villacorta, H.; Maisel, A.S. Soluble ST2 Testing: A Promising Biomarker in the Management of Heart Failure. Arq. Bras. Cardiol. 2015, 106, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Emdin, M.; Aimo, A.; Vergaro, G.; Bayes-Genis, A.; Lupón, J.; Latini, R.; Meessen, J.; Anand, I.S.; Cohn, J.N.; Gravning, J.; et al. sST2 Predicts Outcome in Chronic Heart Failure Beyond NT−proBNP and High-Sensitivity Troponin T. J. Am. Coll. Cardiol. 2018, 72, 2309–2320. [Google Scholar] [CrossRef] [PubMed]
- Aimo, A.; Vergaro, G.; Ripoli, A.; Bayes-Genis, A.; Pascual Figal, D.A.; de Boer, R.A.; Lassus, J.; Mebazaa, A.; Gayat, E.; Breidthardt, T.; et al. Meta-Analysis of Soluble Suppression of Tumorigenicity-2 and Prognosis in Acute Heart Failure. JACC Hear Fail. 2017, 5, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.S.; Filippatos, G.S. Algorithms in Heart Failure; Jaypee, The Health Sciences Publisher: New Delhi, India, 2016. [Google Scholar]
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Lesyuk, W.; Kriza, C.; Kolominsky-Rabas, P. Cost-of-illness studies in heart failure: A systematic review 2004–2016. BMC Cardiovasc. Disord. 2018, 18, 74. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.; Allen, L.A.; Whellan, D.J. Economic burden of heart failure in the elderly. Pharmacoeconomics 2008, 26, 447–462. [Google Scholar] [CrossRef] [PubMed]
- Piper, S.E.; Sherwood, R.A.; Amin-Youssef, G.F.; Shah, A.M.; McDonagh, T.A. Serial soluble ST2 for the monitoring of pharmacologically optimised chronic stable heart failure. Int. J. Cardiol. 2015, 178, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J.L.; Peacock, W.F.; Maisel, A.S.; Chae, C.U.; Jesse, R.L.; Baggish, A.L.; O’Donoghue, M.; Sakhuja, R.; Chen, A.A.; van Kimmenade, R.R.; et al. Measurement of the Interleukin Family Member ST2 in Patients With Acute Dyspnea. J. Am. Coll. Cardiol. 2007, 50, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, T.; Dieplinger, B.; Gegenhuber, A.; Poelz, W.; Pacher, R.; Haltmayer, M. Increased Plasma Concentrations of Soluble ST2 are Predictive for 1-Year Mortality in Patients with Acute Destabilized Heart Failure. Clin. Chem. 2008, 54, 752–756. [Google Scholar] [CrossRef] [Green Version]
- Lassus, J.; Gayat, E.; Mueller, C.; Peacock, W.F.; Spinar, J.; Harjola, V.P.; van Kimmenade, R.; Pathak, A.; Mueller, T.; Disomma, S.; et al. Incremental value of biomarkers to clinical variables for mortality prediction in acutely decompensated heart failure: The Multinational Observational Cohort on Acute Heart Failure (MOCA) study. Int. J. Cardiol. 2013, 168, 2186–2194. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of Amer. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef]
- Bayes-Genis, A.; Zamora, E.; de Antonio, M.; Galán, A.; Vila, J.; Urrutia, A.; Díez, C.; Coll, R.; Altimir, S.; Lupón, J. Soluble ST2 Serum Concentration and Renal Function in Heart Failure. J. Card. Fail. 2013, 19, 768–775. [Google Scholar] [CrossRef]
- Nishimura, M.; Brann, A.; Chang, K.-W.; Maisel, A.S. The Confounding Effects of Non-cardiac Pathologies on the Interpretation of Cardiac Biomarkers. Curr. Heart Fail. Rep. 2018, 15, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.S.; Di Somma, S. Do we need another heart failure biomarker: Focus on soluble suppression of tumorigenicity 2 (sST2). Eur. Heart J. 2016, 38, ehw462. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.B.; Wians, F.; Jaffe, A.; Francisco, S. Biological variation of galectin-3 and soluble ST2 for chronic heart failure: Implication on interpretation of test results. Am. Heart J. 2013, 165, 995–999. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.S.; Richards, A.M.; Pascual-Figal, D.; Mueller, C. Serial ST2 Testing in Hospitalized Patients With Acute Heart Failure. Am. J. Cardiol. 2015, 115, 32B–37B. [Google Scholar] [CrossRef]
- Henry-Okafor, Q.; Collins, S.P.; Jenkins, C.A.; Miller, K.F.; Maron, D.J.; Naftilan, A.J.; Weintraub, N.; Fermann, G.J.; McPherson, J.; Menon, S.; et al. Soluble ST2 as a Diagnostic and Prognostic Marker for Acute Heart Failure Syndromes. Open Biomark. J. 2012, 2012, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J.L.; Camargo, C.A.; Anwaruddin, S.; Baggish, A.L.; Chen, A.A.; Krauser, D.G.; Tung, R.; Cameron, R.; Nagurney, J.T.; Chae, C.U.; et al. The N-terminal Pro-BNP Investigation of Dyspnea in the Emergency department (PRIDE) study. Am. J. Cardiol. 2005, 95, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Fernández, S.; Mueller, T.; Pascual-Figal, D.; Truong, Q.A.; Januzzi, J.L. Usefulness of soluble concentrations of interleukin family member ST2 as predictor of mortality in patients with acutely decompensated heart failure relative to left ventricular ejection fraction. Am. J. Cardiol. 2011, 107, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J.L.; Mebazaa, A.; Disomma, S. ST2 and Prognosis in Acutely Decompensated Heart Failure: The International ST2 Consensus Panel. Am. J. Cardiol. 2015, 115, 26B–31B. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Figal, D.A.; Manzano-Fernández, S.; Boronat, M.; Casas, T.; Garrido, I.P.; Bonaque, J.C.; Pastor-Perez, F.; Valdés, M.; Januzzi, J.L. Soluble ST2, high-sensitivity troponin T- and N-terminal pro-B-type natriuretic peptide: Complementary role for risk stratification in acutely decompensated heart failure. Eur. J. Heart Fail. 2011, 13, 718–725. [Google Scholar] [CrossRef]
- Breidthardt, T.; Balmelli, C.; Twerenbold, R.; Mosimann, T.; Espinola, J.; Haaf, P.; Thalmann, G.; Moehring, B.; Mueller, M.; Meller, B.; et al. Heart failure therapy-induced early ST2 changes may offer long-term therapy guidance. J. Card. Fail. 2013, 19, 821–828. [Google Scholar] [CrossRef]
- Socrates, T.; DeFilippi, C.; Reichlin, T.; Twerenbold, R.; Breidhardt, T.; Noveanu, M.; Potocki, M.; Reiter, M.; Arenja, N.; Heinisch, C.; et al. Interleukin family member ST2 and mortality in acute dyspnoea. J. Intern. Med. 2010, 268, 493–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual-Figal, D.; Wachter, R.; Senni, M.; Belohlavek, J.; Noè, A.; Carr, D.; Butylin, D. Rationale and design of TRANSITION: A randomized trial of pre-discharge vs. post-discharge initiation of sacubitril/valsartan. ESC Hear Fail. 2018, 5, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Van Vark, L.C.; Lesman-Leegte, I.; Baart, S.J.; Postmus, D.; Pinto, Y.M.; Orsel, J.G.; Westenbrink, B.D.; Brunner-la Rocca, H.P.; van Miltenburg, A.J.M.; Boersma, E.; et al. Prognostic Value of Serial ST2 Measurements in Patients With Acute Heart Failure. J. Am. Coll. Cardiol. 2017, 70, 2378–2388. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.W.; Wu, Y.; Grodin, J.L.; Hsu, A.P.; Hernandez, A.F.; Butler, J.; Metra, M.; Voors, A.A.; Felker, G.M.; Troughton, R.W.; et al. Prognostic Value of Baseline and Changes in Circulating Soluble ST2 Levels and the Effects of Nesiritide in Acute Decompensated Heart Failure. JACC Hear Fail. 2016, 4, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Fernández, S.; Januzzi, J.L.; Pastor-Pérez, F.J.; Bonaque-González, J.C.; Boronat-Garcia, M.; Pascual-Figal, D.A.; Montalban-Larrea, S.; Navarro-Peñalver, M.; Andreu-Cayuelas, J.M.; Valdés, M. Serial Monitoring of Soluble Interleukin Family Member ST2 in Patients with Acutely Decompensated Heart Failure. Cardiology 2012, 122, 158–166. [Google Scholar] [CrossRef]
- Boisot, S.; Beede, J.; Isakson, S.; Chiu, A.; Clopton, P.; Januzzi, J.; Maisel, A.S.; Fitzgerald, R.L. Serial Sampling of ST2 Predicts 90-Day Mortality Following Destabilized Heart Failure. J. Card. Fail. 2008, 14, 732–738. [Google Scholar] [CrossRef]
- Talman, V.; Ruskoaho, H. Cardiac fibrosis in myocardial infarction-from repair and remodeling to regeneration. Cell Tissue Res. 2016, 365, 563–581. [Google Scholar] [CrossRef]
- Dattagupta, A.; Immaneni, S. ST2: Current status. Indian Heart J. 2018, 70, S96–S101. [Google Scholar] [CrossRef]
- Firth, B.G.; Dunnmon, P.M. Left ventricular dilatation and failure post-myocardial infarction: Pathophysiology and possible pharmacologic interventions. Cardiovasc. Drugs Ther. 1990, 4, 1363–1374. [Google Scholar] [CrossRef]
- Heineke, J.; Molkentin, J.D. Regulation of cardiac hypertrophy by intracellular signalling pathways. Nat. Rev. Mol. Cell. Biol. 2006, 7, 589–600. [Google Scholar] [CrossRef]
- Everett, B.M.; Zeller, T.; Glynn, R.J.; Ridker, P.M.; Blankenberg, S. High-Sensitivity Cardiac Troponin I and B-Type Natriuretic Peptide as Predictors of Vascular Events in Primary Prevention. Circulation 2015, 131, 1851–1860. [Google Scholar] [CrossRef]
- Weinberg, E.O.; Shimpo, M.; De Keulenaer, G.W.; MacGillivray, C.; Tominaga, S.; Solomon, S.D.; Rouleau, J.L.; Lee, R.T. Expression and regulation of ST2, an interleukin-1 receptor family member, in cardiomyocytes and myocardial infarction. Circulation 2002, 106, 2961–2966. [Google Scholar] [CrossRef] [PubMed]
- Bartunek, J.; Delrue, L.; Van Durme, F.; Muller, O.; Casselman, F.; De Wiest, B.; Croes, R.; Verstreken, S.; Goethals, M.; de Raedt, H.; et al. Nonmyocardial Production of ST2 Protein in Human Hypertrophy and Failure Is Related to Diastolic Load. J. Am. Coll. Cardiol. 2008, 52, 2166–2174. [Google Scholar] [CrossRef] [Green Version]
- Altara, R.; Ghali, R.; Mallat, Z.; Cataliotti, A.; Booz, G.W.; Zouein, F.A. Conflicting vascular and metabolic impact of the IL-33/sST2 axis. Cardiovasc. Res. 2018, 114, 1578–1594. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.; Cortese, F.; Gesualdo, M.; Riccardi, R.; Di Nunzio, D.; Moncelli, M.; Iacoviello, M.; Scicchitano, P. A Novel Cardiac Bio-Marker: ST2: A Review. Molecules 2013, 18, 15314–15328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimpo, M.; Morrow, D.A.; Weinberg, E.O.; Sabatine, M.S.; Murphy, S.A.; Antman, E.M.; Lee, R.T. Serum Levels of the Interleukin-1 Receptor Family Member ST2 Predict Mortality and Clinical Outcome in Acute Myocardial Infarction. Circulation 2004, 109, 2186–2190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabatine, M.S.; Morrow, D.A.; Higgins, L.J.; MacGillivray, C.; Guo, W.; Bode, C.; Rifai, N.; Cannon, C.P.; Gerszten, R.E.; Lee, R.T. Complementary roles for biomarkers of biomechanical strain ST2 and N-terminal prohormone B-type natriuretic peptide in patients with ST-elevation myocardial infarction. Circulation 2008, 117, 1936–1944. [Google Scholar] [CrossRef]
- Kohli, P.; Bonaca, M.P.; Kakkar, R.; Kudinova, A.Y.; Scirica, B.M.; Sabatine, M.S.; Murphy, S.A.; Braunwald, E.; Lee, R.T.; Morrow, D.A. Role of ST2 in Non–ST-Elevation Acute Coronary Syndrome in the MERLIN-TIMI 36 Trial. Clin. Chem. 2012, 58, 257. [Google Scholar] [CrossRef]
- Weir, R.A.P.; Miller, A.M.; Murphy, G.E.J.; Clements, S.; Steedman, T.; Connell, J.M.; McInnes, I.B.; Dargie, H.J.; McMurray, J.J. Serum Soluble ST2: A Potential Novel Mediator in Left Ventricular and Infarct Remodeling After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2010, 55, 243–250. [Google Scholar] [CrossRef]
- Jenkins, W.S.; Roger, V.L.; Jaffe, A.S.; Weston, S.A.; AbouEzzeddine, O.F.; Jiang, R.; Manemann, S.M.; Enriquez-Sarano, M. Prognostic Value of Soluble ST2 After Myocardial Infarction: A Community Perspective. Am. J. Med. 2017, 130, 1112.e9–1112.e15. [Google Scholar] [CrossRef]
- Greenslade, J.H.; Adikari, T.; Mueller, C.; Sandovall, Y.; Nestelberger, T.; Parsonage, W.; Hawkins, T.; Cullen, L. Characteristics and occurrence of type 2 myocardial infarction in emergency department patients: A prospective study. Emerg. Med. J. 2018, 35, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Radovanovic, D.; Pilgrim, T.; Seifert, B.; Urban, P.; Pedrazzini, G.; Erne, P. Type 2 myocardial infarction. J. Cardiovasc. Med. 2017, 18, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.R.; Shah, A.S.V.; Lee, K.K.; Anand, A.; Francis, O.; Adamson, P.; McAllister, D.A.; Strachan, F.E.; Newby, D.E.; Mills, N.L. Long-Term Outcomes in Patients With Type 2 Myocardial Infarction and Myocardial Injury. Circulation 2018, 137, 1236–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; Whit, H.D. Infarction EG on behalf of the JES of C (ESC)/American C of C (ACC)/American HA (AHA)/World HF (WHF) TF for the UD of M (2018) Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M. Avoiding the Imminent Plague of Troponinitis. J. Am. Coll. Cardiol. 2014, 63, 1449–1450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Qu, X.; Gao, Z.; Zheng, G.; Wang, Y.; Chen, X.; Li, H.; Huang, W.; Zhou, H. Soluble ST2 in Patients with Nonvalvular Atrial Fibrillation and Prediction of Heart Failure. Int. Heart J. 2018, 59, 58–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heijman, J.; Guichard, J.-B.; Dobrev, D.; Nattel, S. Translational Challenges in Atrial Fibrillation. Circ. Res. 2018, 122, 752–773. [Google Scholar] [CrossRef] [PubMed]
- Nortamo, S.; Ukkola, O.; Lepojärvi, S.; Kenttä, T.; Kiviniemi, A.; Junttila, J.; Huikuri, H.; Perkiömäki, J. Association of sST2 and hs-CRP levels with new-onset atrial fibrillation in coronary artery disease. Int. J. Cardiol. 2017, 248, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Okar, S.; Kaypakli, O.; Şahin, D.Y.; Koç, M. Fibrosis Marker Soluble ST2 Predicts Atrial Fibrillation Recurrence after Cryoballoon Catheter Ablation of Nonvalvular Paroxysmal Atrial Fibrillation. Korean Circ. J. 2018, 48, 920. [Google Scholar] [CrossRef] [Green Version]
- Coglianese, E.E.; Larson, M.G.; Vasan, R.S.; Ho, J.E.; Ghorbani, A.; McCabe, E.L.; Cheng, S.; Fradley, M.G.; Kretschman, D.; Gao, W.; et al. Distribution and Clinical Correlates of the Interleukin Receptor Family Member Soluble ST2 in the Framingham Heart Study. Clin. Chem. 2012, 58, 1673–1681. [Google Scholar] [CrossRef] [Green Version]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aleksova, A.; Paldino, A.; Beltrami, A.P.; Padoan, L.; Iacoviello, M.; Sinagra, G.; Emdin, M.; Maisel, A.S. Cardiac Biomarkers in the Emergency Department: The Role of Soluble ST2 (sST2) in Acute Heart Failure and Acute Coronary Syndrome—There is Meat on the Bone. J. Clin. Med. 2019, 8, 270. https://doi.org/10.3390/jcm8020270
Aleksova A, Paldino A, Beltrami AP, Padoan L, Iacoviello M, Sinagra G, Emdin M, Maisel AS. Cardiac Biomarkers in the Emergency Department: The Role of Soluble ST2 (sST2) in Acute Heart Failure and Acute Coronary Syndrome—There is Meat on the Bone. Journal of Clinical Medicine. 2019; 8(2):270. https://doi.org/10.3390/jcm8020270
Chicago/Turabian StyleAleksova, Aneta, Alessia Paldino, Antonio Paolo Beltrami, Laura Padoan, Massimo Iacoviello, Gianfranco Sinagra, Michele Emdin, and Alan S. Maisel. 2019. "Cardiac Biomarkers in the Emergency Department: The Role of Soluble ST2 (sST2) in Acute Heart Failure and Acute Coronary Syndrome—There is Meat on the Bone" Journal of Clinical Medicine 8, no. 2: 270. https://doi.org/10.3390/jcm8020270
APA StyleAleksova, A., Paldino, A., Beltrami, A. P., Padoan, L., Iacoviello, M., Sinagra, G., Emdin, M., & Maisel, A. S. (2019). Cardiac Biomarkers in the Emergency Department: The Role of Soluble ST2 (sST2) in Acute Heart Failure and Acute Coronary Syndrome—There is Meat on the Bone. Journal of Clinical Medicine, 8(2), 270. https://doi.org/10.3390/jcm8020270