The Predictivity of N-Terminal Pro b-Type Natriuretic Peptide for All-Cause Mortality in Various Follow-Up Periods among Heart Failure Patients



Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Population
2.2. NT-proBNP Assay
2.3. Endpoints of the Study
2.4. Ethical Approval
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics, Clinical Variables, and Outcomes
3.2. Association of Plasma NT-pro-BNP Levels and 12-Month Mortality
3.3. The Independent Predictors of 12-Month Mortality
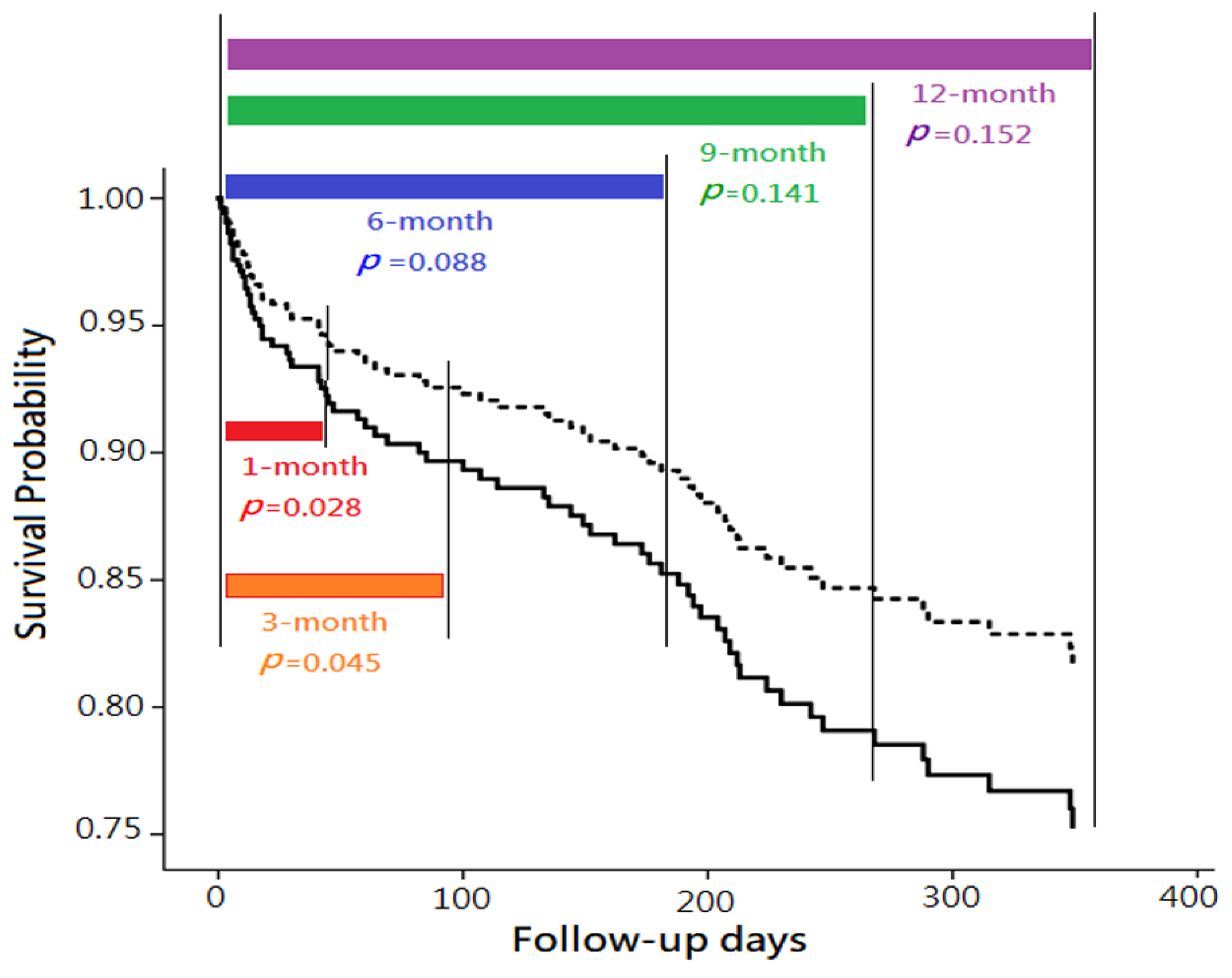
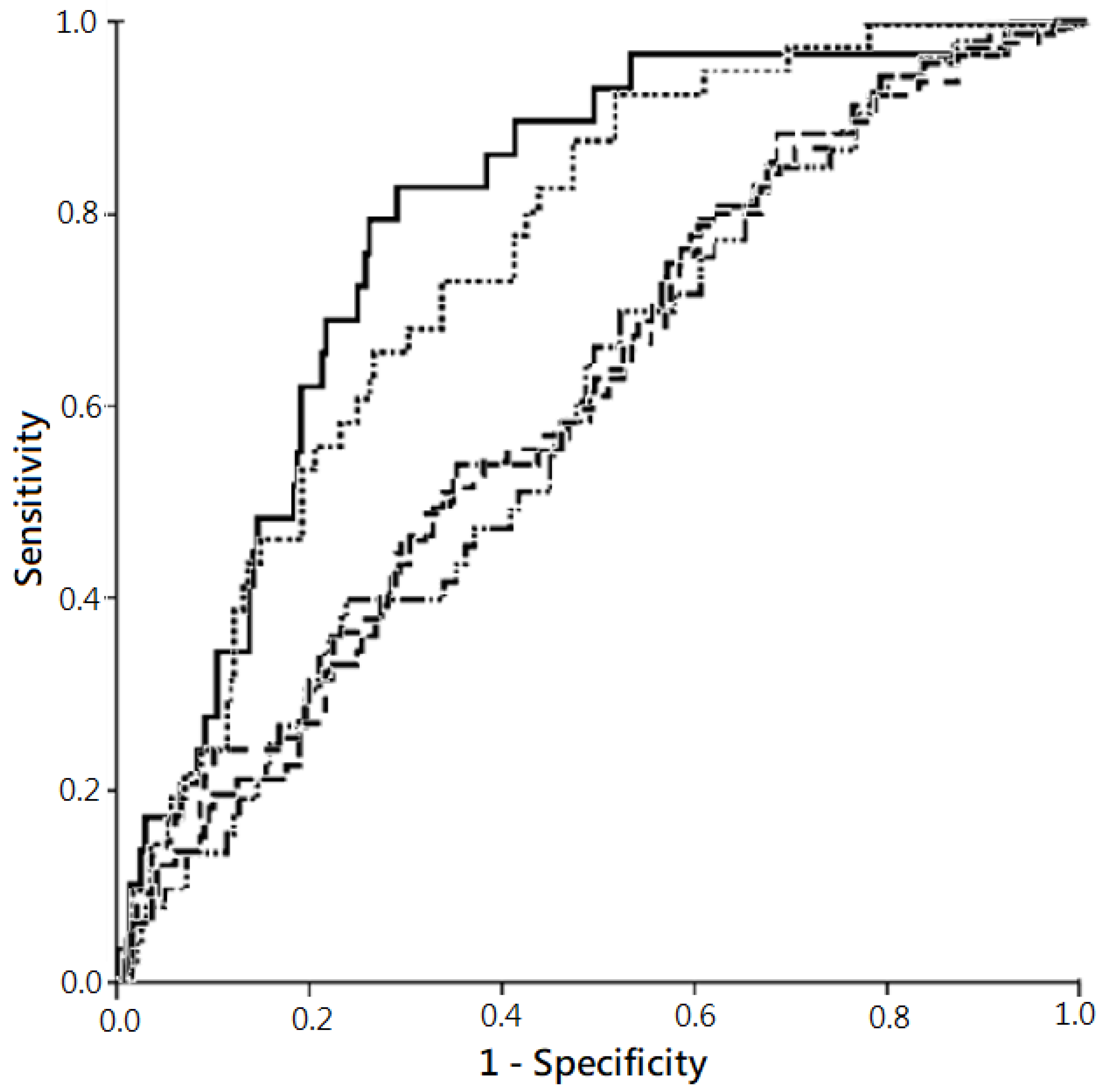
3.4. Predictive Powers of Plasma NT-proBNP Levels on Mortality with Various Follow-Up Periods
4. Discussion
4.1. NT-proBNP and Patient Prognoses
4.2. Other Predictors of Mortality
4.3. Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Chen, J.; Normand, S.L.; Wang, Y.; Krumholz, H.M. National and regional trends in heart failure hospitalization and mortality rates for Medicare beneficiaries, 1998–2008. JAMA 2011, 306, 1669–1678. [Google Scholar] [CrossRef]
- Spinar, J.; Parenica, J.; Vitovec, J.; Widimsky, P.; Linhart, A.; Fedorco, M.; Malek, F.; Cihalik, C.; Spinarova, L.; Miklik, R.; et al. Baseline characteristics and hospital mortality in the Acute Heart Failure Database (AHEAD) Main registry. Crit. Care 2011, 15, R291. [Google Scholar] [CrossRef] [PubMed]
- Bueno, H.; Ross, J.S.; Wang, Y.; Chen, J.; Vidan, M.T.; Normand, S.L.; Curtis, J.P.; Drye, E.E.; Lichtman, J.H.; Keenan, P.S.; et al. Trends in length of stay and short-term outcomes among Medicare patients hospitalized for heart failure, 1993–2006. JAMA 2010, 303, 2141–2147. [Google Scholar] [CrossRef]
- Muntwyler, J.; Abetel, G.; Gruner, C.; Follath, F. One-year mortality among unselected outpatients with heart failure. Eur. Heart J. 2002, 23, 1861–1866. [Google Scholar] [CrossRef] [Green Version]
- Gustafsson, F.; Torp-Pedersen, C.; Brendorp, B.; Seibaek, M.; Burchardt, H.; Kober, L. Long-term survival in patients hospitalized with congestive heart failure: Relation to preserved and reduced left ventricular systolic function. Eur. Heart J. 2003, 24, 863–870. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef]
- Clerico, A.; Giannoni, A.; Vittorini, S.; Passino, C. Thirty years of the heart as an endocrine organ: Physiological role and clinical utility of cardiac natriuretic hormones. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H12–H20. [Google Scholar] [CrossRef]
- Semenov, A.G.; Seferian, K.R.; Tamm, N.N.; Artem’eva, M.M.; Postnikov, A.B.; Bereznikova, A.V.; Kara, A.N.; Medvedeva, N.A.; Katrukha, A.G. Human pro-B-type natriuretic peptide is processed in the circulation in a rat model. Clin. Chem. 2011, 57, 883–890. [Google Scholar] [CrossRef]
- Richards, A.M. N-Terminal B-type Natriuretic Peptide in Heart Failure. Heart Fail. Clin. 2018, 14, 27–39. [Google Scholar] [CrossRef]
- Anjan, V.Y.; Loftus, T.M.; Burke, M.A.; Akhter, N.; Fonarow, G.C.; Gheorghiade, M.; Shah, S.J. Prevalence, clinical phenotype, and outcomes associated with normal B-type natriuretic peptide levels in heart failure with preserved ejection fraction. Am. J. Cardiol. 2012, 110, 870–876. [Google Scholar] [CrossRef]
- Troughton, R.W.; Prior, D.L.; Pereira, J.J.; Martin, M.; Fogarty, A.; Morehead, A.; Yandle, T.G.; Richards, A.M.; Starling, R.C.; Young, J.B.; et al. Plasma B-type natriuretic peptide levels in systolic heart failure: Importance of left ventricular diastolic function and right ventricular systolic function. J. Am. Coll. Cardiol. 2004, 43, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Yasue, H.; Yoshimura, M.; Sumida, H.; Kikuta, K.; Kugiyama, K.; Jougasaki, M.; Ogawa, H.; Okumura, K.; Mukoyama, M.; Nakao, K. Localization and mechanism of secretion of B-type natriuretic peptide in comparison with those of A-type natriuretic peptide in normal subjects and patients with heart failure. Circulation 1994, 90, 195–203. [Google Scholar] [CrossRef]
- Januzzi, J.L.; van Kimmenade, R.; Lainchbury, J.; Bayes-Genis, A.; Ordonez-Llanos, J.; Santalo-Bel, M.; Pinto, Y.M.; Richards, M. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: An international pooled analysis of 1256 patients: The International Collaborative of, N.T-proBNP Study. Eur. Heart J. 2006, 27, 330–337. [Google Scholar] [CrossRef]
- Sokhanvar, S.; Shekhi, M.; Mazlomzadeh, S.; Golmohammadi, Z. The Relationship between Serum, N.T– Pro-BNP Levels and Prognosis in Patients with Systolic Heart Failure. J. Cardiovasc. Thor. Res. 2011, 3, 57–61. [Google Scholar]
- Gardner, R.S.; Chong, K.S.; Morton, J.J.; McDonagh, T.A. N-terminal brain natriuretic peptide, but not anemia, is a powerful predictor of mortality in advanced heart failure. J. Card. Fail. 2005, 11, S47–S53. [Google Scholar] [CrossRef] [PubMed]
- Andersson, S.E.; Edvinsson, M.L.; Bjork, J.; Edvinsson, L. High NT-proBNP is a strong predictor of outcome in elderly heart failure patients. Am. J. Geriatr. Cardiol. 2008, 17, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Noveanu, M.; Breidthardt, T.; Potocki, M.; Reichlin, T.; Twerenbold, R.; Uthoff, H.; Socrates, T.; Arenja, N.; Reiter, M.; Meissner, J.; et al. Direct comparison of serial B-type natriuretic peptide and, N.T-proBNP levels for prediction of short- and long-term outcome in acute decompensated heart failure. Crit. Care 2011, 15, R1. [Google Scholar] [CrossRef]
- Wu, A.H. Serial testing of B-type natriuretic peptide and NTpro-BNP for monitoring therapy of heart failure: The role of biologic variation in the interpretation of results. Am. Heart J. 2006, 152, 828–834. [Google Scholar] [CrossRef]
- Zile, M.R.; Claggett, B.L.; Prescott, M.F.; McMurray, J.J.V.; Packer, M.; Rouleau, J.L.; Swedberg, K.; Desai, A.S.; Gong, J.; Shi, V.C.; et al. Prognostic Implications of Changes in N-Terminal Pro-B-Type Natriuretic Peptide in Patients with Heart Failure. J. Am. Coll. Cardiol. 2016, 68, 2425–2436. [Google Scholar] [CrossRef]
- O’Hanlon, R.; O’Shea, P.; Ledwidge, M.; O’Loughlin, C.; Lange, S.; Conlon, C.; Phelan, D.; Cunningham, S.; McDonald, K. The biologic variability of B-type natriuretic peptide and N-terminal pro-B-type natriuretic peptide in stable heart failure patients. J. Card. Fail. 2007, 13, 50–55. [Google Scholar] [CrossRef]
- Cortes, R.; Rivera, M.; Salvador, A.; Bertomeu, V.; de Burgos, F.G.; Rosello-Lleti, E.; Portoles, M.; Paya, R.; Martinez-Dolz, L.; Climent, V. Variability of NT-proBNP plasma and urine levels in patients with stable heart failure: A 2-year follow-up study. Heart 2007, 93, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.T.; Tseng, Y.T.; Chu, T.W.; Chen, J.; Lai, M.Y.; Tang, W.R.; Shiao, C.C. N-terminal pro b-type natriuretic peptide (NT-pro-BNP) -based score can predict in-hospital mortality in patients with heart failure. Sci. Rep. 2016, 6, 29590. [Google Scholar] [CrossRef] [PubMed]
- Prontera, C.; Zucchelli, G.C.; Vittorini, S.; Storti, S.; Emdin, M.; Clerico, A. Comparison between analytical performances of polyclonal and monoclonal electrochemiluminescence immunoassays for NT-proBNP. Clin. Chim. Acta 2009, 400, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Clerico, A.; Fontana, M.; Zyw, L.; Passino, C.; Emdin, M. Comparison of the diagnostic accuracy of brain natriuretic peptide (BNP) and the N-terminal part of the propeptide of BNP immunoassays in chronic and acute heart failure: A systematic review. Clin. Chem. 2007, 53, 813–822. [Google Scholar] [CrossRef] [PubMed]
- Hunt, P.J.; Richards, A.M.; Nicholls, M.G.; Yandle, T.G.; Doughty, R.N.; Espiner, E.A. Immunoreactive amino-terminal pro-brain natriuretic peptide (NT-PROBNP): A new marker of cardiac impairment. Clin. Endocrinol. (Oxf) 1997, 47, 287–296. [Google Scholar] [CrossRef]
- Hunt, P.J.; Yandle, T.G.; Nicholls, M.G.; Richards, A.M.; Espiner, E.A. The amino-terminal portion of pro-brain natriuretic peptide (Pro-BNP) circulates in human plasma. Biochem. Biophys. Res. Commun. 1995, 214, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Schou, M.; Gustafsson, F.; Kjaer, A.; Hildebrandt, P.R. Long-term clinical variation of NT-proBNP in stable chronic heart failure patients. Eur. Heart J. 2007, 28, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Gegenhuber, A.; Mueller, T.; Dieplinger, B.; Poelz, W.; Pacher, R.; Haltmayer, M. B-type natriuretic peptide and amino terminal proBNP predict one-year mortality in short of breath patients independently of the baseline diagnosis of acute destabilized heart failure. Clin. Chim. Acta 2006, 370, 174–179. [Google Scholar] [CrossRef]
- Lassus, J.P.; Siirila-Waris, K.; Nieminen, M.S.; Tolonen, J.; Tarvasmaki, T.; Peuhkurinen, K.; Melin, J.; Pulkki, K.; Harjola, V.P.; group F-As. Long-term survival after hospitalization for acute heart failure—Differences in prognosis of acutely decompensated chronic and new-onset acute heart failure. Int. J. Cardiol. 2013, 168, 458–462. [Google Scholar] [CrossRef]
- Richards, A.M. Variability of NT-proBNP levels in heart failure: Implications for clinical application. Heart 2007, 93, 899–900. [Google Scholar] [CrossRef]
- Flather, M.D.; Yusuf, S.; Køber, L.; Pfeffer, M.; Hall, A.; Murray, G.; Torp-Pedersen, C.; Ball, S.; Pogue, J.; Moyé, L.; et al. Long-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: A systematic overview of data from individual patients. Lancet 2000, 355, 1575–1581. [Google Scholar] [CrossRef]
- Gustafsson, F.; Torp-Pedersen, C.; Seibaek, M.; Burchardt, H.; Kober, L. Effect of age on short and long-term mortality in patients admitted to hospital with congestive heart failure. Eur. Heart J. 2004, 25, 1711–1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jong, P.; Vowinckel, E.; Liu, P.P.; Gong, Y.; Tu, J.V. Prognosis and determinants of survival in patients newly hospitalized for heart failure: A population-based study. Arch. Intern. Med. 2002, 162, 1689–1694. [Google Scholar] [CrossRef]
- Hunt, S.A.; Abraham, W.T.; Chin, M.H.; Feldman, A.M.; Francis, G.S.; Ganiats, T.G.; Jessup, M.; Konstam, M.A.; Mancini, D.M.; Michl, K.; et al. Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung Transplantation. J. Am. Coll. Cardiol. 2009, 53, e1–e90. [Google Scholar] [PubMed]
- Bloom, H.L.; Shukrullah, I.; Cuellar, J.R.; Lloyd, M.S.; Dudley, S.C.; Zafari, A.M. Long-term survival after successful inhospital cardiac arrest resuscitation. Am. Heart J. 2007, 153, 831–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tariq, S.; Aronow, W.S. Use of Inotropic Agents in Treatment of Systolic Heart Failure. Int. J. Mol. Sci. 2015, 16, 29060–29068. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Wright, L.; Negishi, T.; Negishi, K.; Liu, J.; Marwick, T.H. Research to Practice: Assessment of Left Ventricular Global Longitudinal Strain for Surveillance of Cancer Chemotherapeutic-Related Cardiac Dysfunction. JACC Cardiovasc. Imaging 2018, 11, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Park, J.J.; Park, J.B.; Park, J.H.; Cho, G.Y. Global Longitudinal Strain to Predict Mortality in Patients with Acute Heart Failure. J. Am. Coll. Cardiol. 2018, 71, 1947–1957. [Google Scholar] [CrossRef]
- Velazquez, E.J.; Morrow, D.A.; DeVore, A.D.; Duffy, C.I.; Ambrosy, A.P.; McCague, K.; Rocha, R.; Braunwald, E.; Investigators P-H. Angiotensin-Neprilysin Inhibition in Acute Decompensated Heart Failure. N. Engl. J. Med. 2019, 380, 539–548. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Survivor (n = 197) | Non-Survivor (n = 72) | p-Value | |
|---|---|---|---|
| Age, years | 72.1 ± 13.9 74.0 (75.0) | 80.9 ± 10.6 83.0 (55.0) | <0.001 |
| Gender, female | 104 (52.8%) | 41 (56.9%) | 0.545 |
| Current smoker | 55 (27.9%) | 11 (15.3%) | 0.033 |
| Body mass index, kg/m2 | 24.0 ± 5.3 23.4 (27.0) | 22.5 ± 4.6 22.1 (28.3) | 0.006 |
| Charlson comorbidity index | 6.5 ± 2.5 | 8.8 ± 2.6 | <0.001 |
| Comorbidity | |||
| Chronic lung disease | 44 (22.3%) | 13 (18.1%) | 0.447 |
| Diabetes mellitus | 80 (40.6%) | 35 (48.6%) | 0.240 |
| Chronic kidney disease | 70 (35.5%) | 47 (65.3%) | <0.001 |
| Cerebral vascular accident | 21 (10.7%) | 13 (18.1%) | 0.106 |
| Malignancy | 7 (3.6%) | 7 (9.7%) | 0.044 |
| Heart-specific comorbidity | 0.776 | ||
| Hypertension | 12 (6.1%) | 4 (5.6%) | |
| Ischemic heart disease | 90 (45.7%) | 36 (50.0%) | |
| Rheumatic heart disease | 4 (2.0%) | 2 (2.8%) | |
| Valvular heart disease | 74 (37.6%) | 27 (37.5%) | |
| Dilated cardiomyopathy | 17 (8.6%) | 3 (4.2%) | |
| Medication | |||
| ACEI/ARB | 119 (60.4%) | 27 (37.5%) | 0.001 |
| Beta-blocker | 82 (41.6%) | 14 (19.4%) | 0.001 |
| Ald. blocker | 62 (31.5%) | 12 (16.7%) | 0.016 |
| Loop-diuretic | 129 (65.5%) | 35 (48.6%) | 0.012 |
| Digoxin | 34 (17.3%) | 6 (8.3%) | 0.069 |
| Vital sign at initial hospitalization | |||
| Body temperature, °C | 36. 5 ± 0.8 36.3 (5.8) | 36.4 ± 0.8 36.3 (4.4) | 0.736 |
| Heart rate, bpm | 95.7 ± 23.4 95.0 (120.0) | 97.7 ± 24.8 98.3 (100.0) | 0.474 |
| Respiratory rate, breath per min | 22.9 ± 5.3 21.0 (39.0) | 22.9 ± 5.6 22.0 (30.0) | 0.843 |
| Systolic blood pressure, mmHg | 138.9 ± 31.1 137.0 (172.0) | 138.5 ± 32.3 138.0 (148.0) | 0.592 |
| Diastolic blood pressure, mmHg | 82.9 ± 18.4 82.0 (111.0) | 76.5 ± 15.6 78.0 (76.0) | 0.187 |
| NYHA Fc | <0.001 | ||
| II | 53 (26.9%) | 15 (20.8%) | |
| III | 110 (55.8%) | 28 (38.9%) | |
| IV | 34 (17.3%) | 29 (40.3%) | |
| Laboratory tests at initial hospitalization | |||
| White blood cell, ×109/L | 9.9 ± 4.4 8.7 (24.8) | 10.6 ± 6.1 9.2 (36.3) | 0.762 |
| Hemoglobin, g/dL | 11.9 ± 2.4 | 10.6 ± 2.4 | <0.001 |
| Neutrophil, % | 72.7 ± 12.07 73.8 (60.9) | 78.5 ± 13.7 80.3 (64.7) | 0.009 |
| Sodium, mmol/L | 138.4 ± 5.6 139.0 (39.0) | 136.1 ± 6.6 137.0 (30.0) | 0.007 |
| Potassium, mEq/L | 4.0 ± 0.8 3.9 (5.1) | 4.2 ± 1.0 4.0 (4.5) | 0.374 |
| eGFR, ml/min/1.73m2 | 57.8 ± 33.2 54.9 (169.9) | 44.9 ± 35.5 37.6 (216.0) | 0.002 |
| Glutamate oxaloacetate transaminase, U/> | 55.0 ± 119.9 29.0 (1349.0) | 35.7 ± 26.0 28.0 (126.0) | 0.603 |
| Sugar (non-fasting), mg/dL | 179.3 ± 114.7 146.0 (1005.0) | 174.3 ± 94.3 148.2 (678.0) | 0.819 |
| NT-proBNP, ng/L | 10,275.2 ± 11,591.6 5,977.0 (82,590.0) | 14,966.8 ± 12,724.6 10,116.5 (48,195.0) | 0.001 |
| White blood cell, ×109/L | 9.9 ± 4.4 8.7 (24.8) | 10.6 ± 6.1 9.2 (36.3) | 0.762 |
| Hemoglobin, g/dL | 11.9 ± 2.4 | 10.6 ± 2.4 | <0.001 |
| Electrocardiogram-AF | 60 (30.5%) | 27 (37.5%) | 0.274 |
| LVEF, % | 48.2 ± 16.8 49.0 (78.0) | 50.8 ± 17.6 51.5 (73.0) | 0.391 |
| Types of HF | 0.494 | ||
| HFpEF (LVEF ≧50%) | 98 (49.7%) | 41(56.9%) | |
| HFmrEF (LVEF 40-49%) | 31 (15.7%) | 8 (11.1%) | |
| HFrEF (LVEF <40%) | 68 (34.5%) | 23 (31.9%) | |
| Left ventricular hypertrophy | 71 (36.0%) | 37 (51.4%) | 0.023 |
| Dilated left atrium | 118 (59.9%) | 36 (50%) | 0.146 |
| Dilated left ventricle | 78 (39.6%) | 22 (30.6%) | 0.174 |
| Pulmonary hypertension | 59 (29.9%) | 21 (29.2%) | 0.901 |
| Infection during hospitalization | 87 (44.2%) | 51 (70.8%) | <0.001 |
| Outcomes | |||
| ICU admission | 95 (48.2%) | 44 (61.1%) | 0.061 |
| Length of ICU stay, days | 2.56 ± 4.58 | 5.08 ± 7.53 | 0.001 |
| Mechanical ventilator | 28 (14.2%) | 21 (29.2%) | 0.005 |
| Length of ventilator, days | 10.27 ± 10.33 | 9.29 ± 13.01 | 0.779 |
| Use of NIPPV | 14 (7.1%) | 14 (19.4%) | 0.003 |
| Length of NIPPV, days | 4.21 ± 4.21 | 4.86 ± 4.90 | 0.713 |
| Administration of vasopressor | 15 (7.6%) | 18 (25.0%) | <0.001 |
| Underwent CPR | 4 (2.0%) | 9 (12.5%) | <0.001 |
| B | aHR (95% CI) | p-Value | |
|---|---|---|---|
| Age | 0.07 | 1.07 (1.04–1.10) | <0.001 |
| Charlson comorbidity index | 0.20 | 1.22 (1.10–1.34) | <0.001 |
| With ACEI/ARB | |||
| No | Reference | ||
| Yes | −0.89 | 0.411 (0.25–0.68) | <0.001 |
| Administration of vasopressor | |||
| No | Reference | ||
| Yes | 1.23 | 3.43 (1.76–6.71) | <0.001 |
| Underwent CPR | |||
| No | Reference | ||
| Yes | 1.52 | 4.59 (1.86–11.31) | <0.001 |
| 1-month Mortality 1 | 3-month Mortality 2 | 6-month Mortality 3 | 9-month Mortality 4 | 12-month Mortality 5 | |
|---|---|---|---|---|---|
| Crude HR (95% CI) | |||||
| PlasmaNT-pro BNP level (≧ 11,755 ng/L) | 3.32 (1.59–6.59) ** | 2.76 (1.49–5.09) ** | 2.12 (1.24–3.64) ** | 1.90 (1.18–3.08) ** | 1.88 (1.18–2.99) ** |
| aHR (95% CI) | |||||
| Plasma NT-proBNP level (≧11,755 ng/L) | 2.37 (1.10–5.11) * | 1.98 (1.02–3.86) * | 1.63 (0.93–2.86) | 1.44 (0.89–2/35) | 1.41 (0.88–2.26) |
| Age | 1.05 (1.01–1.10) * | 1.06 (1.03–1.10) *** | 1.05 (1.02–1.09) ** | 1.07 (1.04–1.10) *** | 1.07 (1.04–1.10) *** |
| Administration of vasopressor | 3.59 (1.34–9.67) * | 5.35 (2.30–12.43) *** | 3.65 (1.75–7.61) ** | 374 (1906–7.39) *** | 3.43 (1.76–6.71) *** |
| Underwent CPR | 5.93 (1.99–17.64) ** | 4.04 (1.31–12.47) * | 5.62 (2.16–14.64) *** | 4.70 (1.90–11.65) ** | 4.59 (1.86–11.31) *** |
| With ACEI/ARB | 0.23 (0.08–0.61) ** | 0.27 (0.13–0.58) ** | 0.42 (0.23–0.76) ** | 0.43 (0.26–0.73) *** | 0.411 (0.25–0.68) *** |
| With loop-diuretic | 0.37 (0.15–0.90) * | — | — | — | — |
| With beta-blocker | — | 0.13 (0.30–0.53) ** | 0.33 (0.15–0.75) ** | — | — |
| With ICU admission | — | 0.36 (0.14–0.90) * | — | — | — |
| With mechanical ventilator | — | 3.46 (1.19–10.11) * | — | — | — |
| With CPAP | — | 3.70 (1.43–9.63) ** | — | — | — |
| Charlson comorbidity index | — | — | 1.18 (1.05–1.32) ** | 1.21 (1.09–1.34) *** | 1.22 (1.10–1.34) *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, M.-Y.; Kan, W.-C.; Huang, Y.-T.; Chen, J.; Shiao, C.-C. The Predictivity of N-Terminal Pro b-Type Natriuretic Peptide for All-Cause Mortality in Various Follow-Up Periods among Heart Failure Patients. J. Clin. Med. 2019, 8, 357. https://doi.org/10.3390/jcm8030357
Lai M-Y, Kan W-C, Huang Y-T, Chen J, Shiao C-C. The Predictivity of N-Terminal Pro b-Type Natriuretic Peptide for All-Cause Mortality in Various Follow-Up Periods among Heart Failure Patients. Journal of Clinical Medicine. 2019; 8(3):357. https://doi.org/10.3390/jcm8030357
Chicago/Turabian StyleLai, Min-Yu, Wei-Chih Kan, Ya-Ting Huang, John Chen, and Chih-Chung Shiao. 2019. "The Predictivity of N-Terminal Pro b-Type Natriuretic Peptide for All-Cause Mortality in Various Follow-Up Periods among Heart Failure Patients" Journal of Clinical Medicine 8, no. 3: 357. https://doi.org/10.3390/jcm8030357
APA StyleLai, M. -Y., Kan, W. -C., Huang, Y. -T., Chen, J., & Shiao, C. -C. (2019). The Predictivity of N-Terminal Pro b-Type Natriuretic Peptide for All-Cause Mortality in Various Follow-Up Periods among Heart Failure Patients. Journal of Clinical Medicine, 8(3), 357. https://doi.org/10.3390/jcm8030357