Accuracy of Customized Prefabricated Screw-Type Immediate Provisional Restorations after Single-Implant Placement



Abstract
:1. Introduction
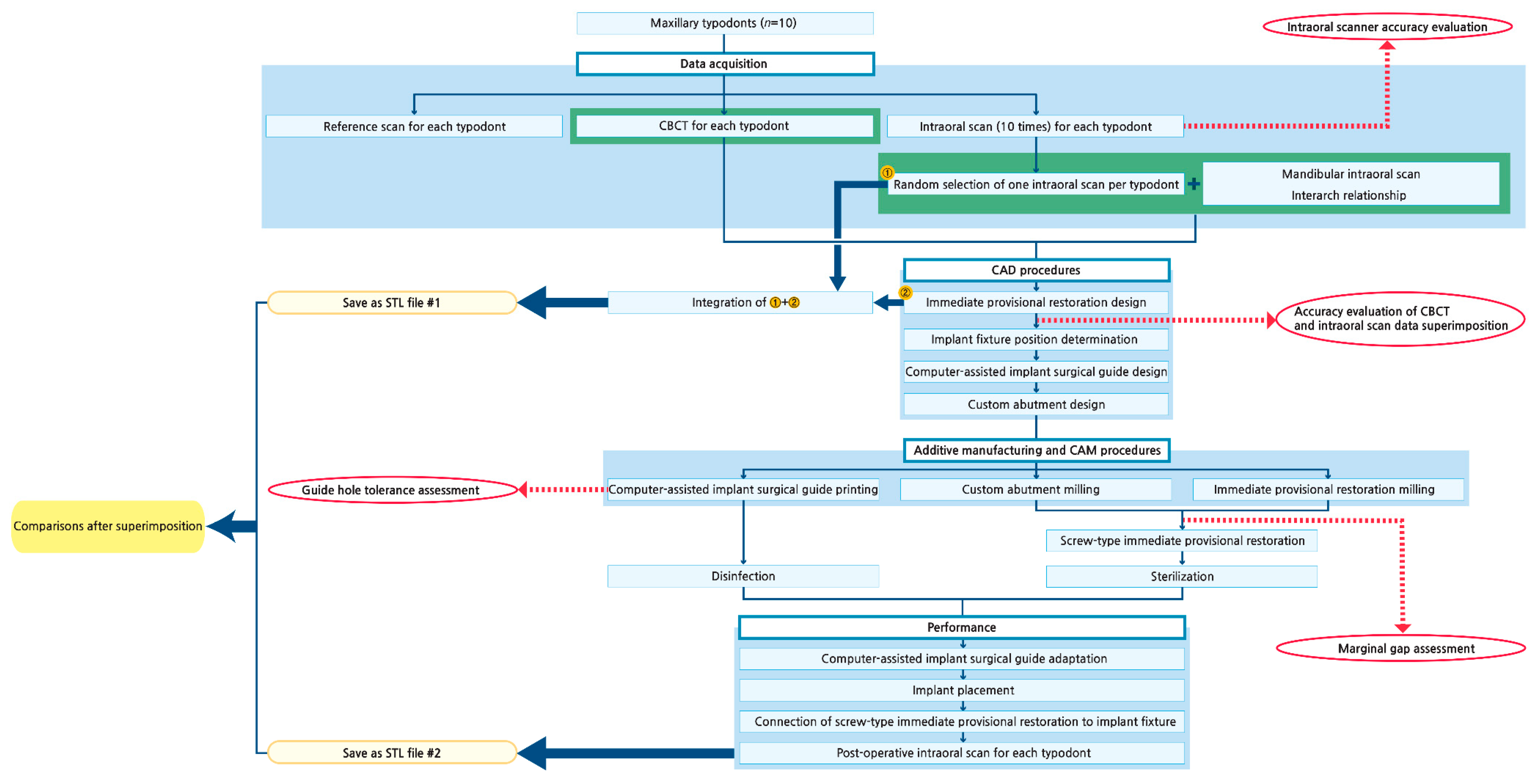
2. Experimental Section
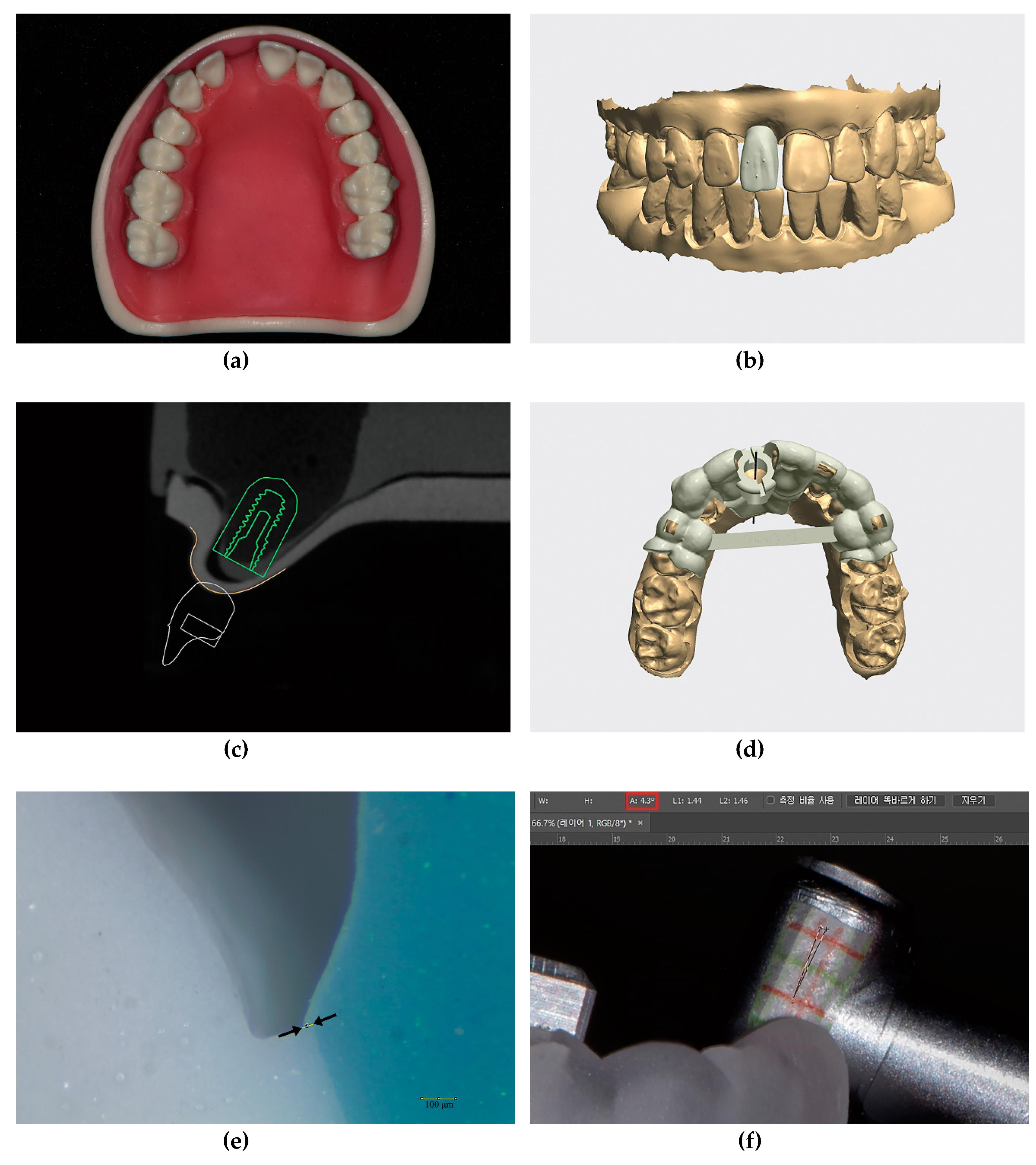
2.1. Modification of Dental Models
2.2. Evaluation of Intraoral Scanner Accuracy (Trueness and Precision)
2.3. Acquisition of Intraoral Scan Data
2.4. Acquisition of CBCT Data
2.5. CAD Procedures
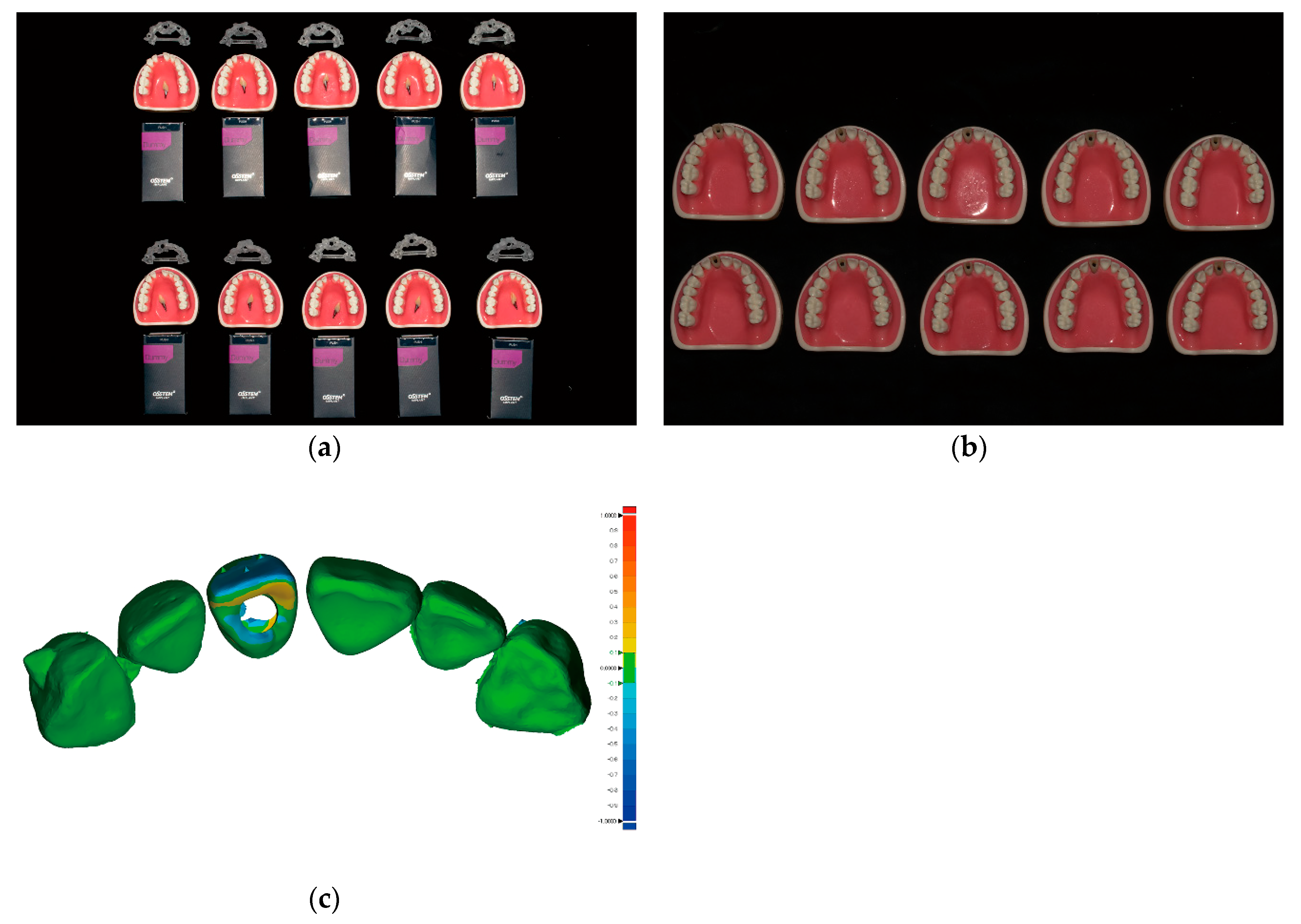
2.6. Additive Manufacturing (3D Printing) and CAM Procedures
2.7. Evaluation of the Marginal Adaptation of the Provisional Restorations
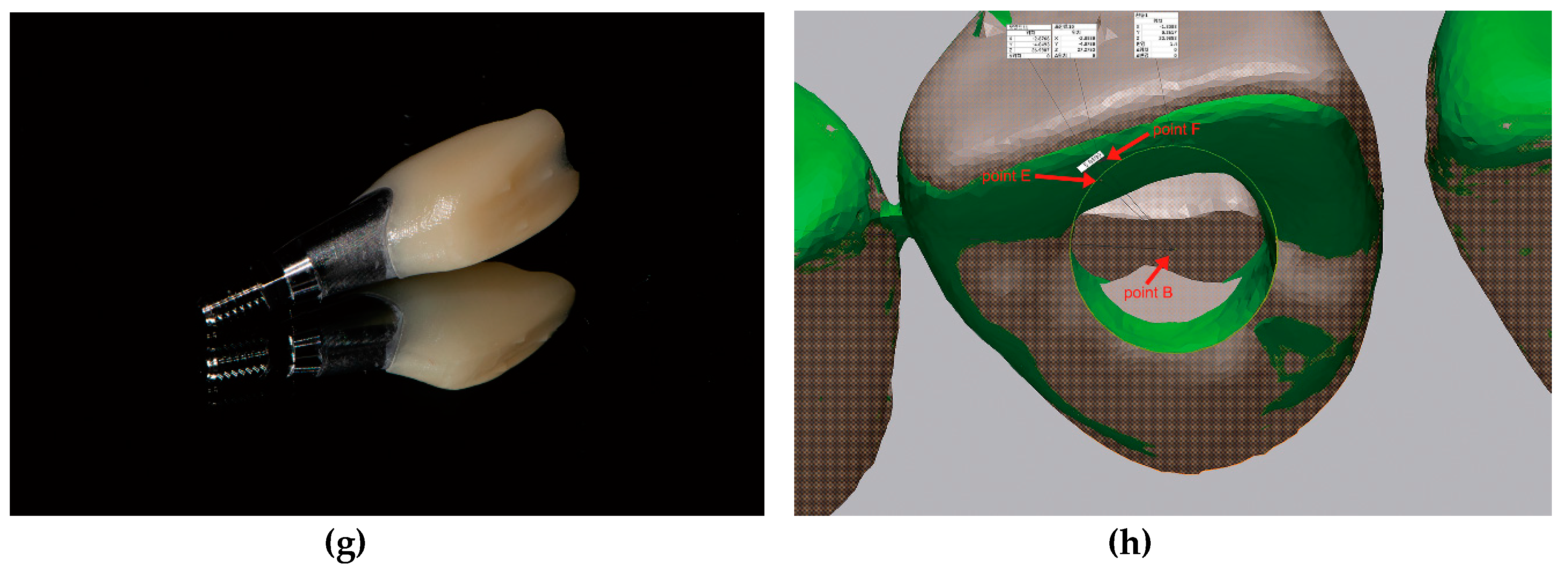
2.8. Evaluation of the Guide Hole Tolerance of the Surgical Guides
2.9. Preparation of Prefabricated Screw-Type Immediate Provisional Restorations
2.10. Surgical and Prosthodontic Procedures: Implant Placement and Screw-Type Immediate Provisional Restoration Connection
2.11. 3D Analysis of the Provisional Restoration Position
2.12. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MOD#1 | MOD#2 | MOD#3 | MOD#4 | MOD#5 | MOD#6 | MOD#7 | MOD#8 | MOD#9 | MOD#10 | Overall Mean ± SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 133.7 | 147.3 | 161.4 | 107.1 | 154.7 | 149.8 | 143.7 | 120.1 | 189.6 | 181.7 | ||
| 138.0 | 137.6 | 153.4 | 117.0 | 158.6 | 163.3 | 135.8 | 112.3 | 179.1 | 171.9 | ||
| 159.7 | 241.8 | 176.1 | 117.3 | 166.7 | 149.3 | 135.3 | 114.3 | 181.1 | 188.8 | ||
| 134.4 | 145.8 | 160.9 | 126.6 | 149.6 | 158.6 | 139.2 | 104.1 | 205.6 | 184.6 | ||
| 135.9 | 136.2 | 137.8 | 171.2 | 157.8 | 149.0 | 142.2 | 119.5 | 189.7 | 196.0 | ||
| 140.7 | 147.5 | 151.8 | 125.4 | 166.5 | 147.3 | 142.0 | 113.3 | 181.6 | 191.9 | ||
| 168.7 | 165.0 | 161.6 | 128.8 | 162.2 | 160.0 | 127.2 | 104.8 | 176.7 | 177.1 | ||
| 137.8 | 181.2 | 156.7 | 116.7 | 162.9 | 150.8 | 147.9 | 124.4 | 179.5 | 175.4 | ||
| 138.4 | 147.1 | 155.3 | 139.7 | 255.0 | 195.4 | 150.0 | 118.6 | 192.6 | 168.9 | ||
| 141.3 | 146.6 | 152.7 | 123.1 | 192.0 | 149.6 | 133.5 | 115.7 | 188.1 | 171.4 | ||
| Mean | 142.9 | 159.6 | 156.8 | 127.3 | 172.6 | 157.3 | 139.7 | 114.7 | 186.4 | 180.8 | 153.8 ± 23.0 |
| MOD#1 | MOD#2 | MOD#3 | MOD#4 | MOD#5 | MOD#6 | MOD#7 | MOD#8 | MOD#9 | MOD#10 | Overall Mean ± SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 29.9 | 92.3 | 46.7 | 42.5 | 83.2 | 63.7 | 37.9 | 109.6 | 101.1 | 68.9 | ||
| 115.8 | 327.6 | 146.2 | 32.9 | 86.6 | 61.0 | 85.7 | 35.2 | 52.2 | 31.7 | ||
| 59.0 | 117.1 | 34.8 | 50.0 | 37.0 | 58.8 | 61.2 | 61.7 | 135.9 | 108.3 | ||
| 50.5 | 138.0 | 38.7 | 131.5 | 40.7 | 75.3 | 83.6 | 36.5 | 82.3 | 31.1 | ||
| 63.2 | 158.0 | 70.2 | 58.6 | 73.2 | 50.0 | 38.9 | 40.7 | 58.5 | 37.4 | ||
| 119.4 | 180.3 | 124.0 | 61.3 | 55.7 | 69.4 | 48.5 | 68.8 | 52.4 | 33.7 | ||
| 46.9 | 250.2 | 70.3 | 35.0 | 59.6 | 55.6 | 42.3 | 39.9 | 91.2 | 38.8 | ||
| 59.7 | 179.9 | 76.1 | 98.8 | 169.8 | 118.5 | 121.8 | 117.7 | 38.7 | 79.7 | ||
| 59.0 | 144.9 | 28.9 | 51.3 | 125.1 | 52.8 | 65.7 | 123.5 | 108.4 | 46.5 | ||
| 127.9 | 239.6 | 93.6 | 30.7 | 32.5 | 53.0 | 85.1 | 106.3 | 46.1 | 55.9 | ||
| 57.9 | 39.0 | 71.1 | 46.2 | 52.3 | 61.5 | 56.9 | 56.3 | 74.4 | 37.5 | ||
| 49.2 | 45.5 | 40.6 | 139.1 | 57.5 | 88.4 | 89.9 | 120.4 | 40.0 | 75.6 | ||
| 71.2 | 117.1 | 38.1 | 56.0 | 25.3 | 47.9 | 30.0 | 87.6 | 44.5 | 84.4 | ||
| 143.3 | 137.4 | 97.1 | 81.9 | 30.2 | 40.6 | 41.9 | 41.7 | 52.1 | 41.0 | ||
| 45.5 | 143.9 | 35.4 | 42.2 | 28.4 | 43.2 | 45.4 | 108.3 | 32.1 | 37.4 | ||
| 55.8 | 125.1 | 46.1 | 104.0 | 105.6 | 68.4 | 106.5 | 31.0 | 82.0 | 20.5 | ||
| 57.5 | 96.5 | 37.0 | 50.3 | 50.2 | 85.0 | 61.5 | 35.1 | 49.6 | 27.0 | ||
| 65.3 | 209.0 | 166.0 | 41.6 | 59.0 | 32.4 | 38.2 | 49.4 | 133.6 | 94.6 | ||
| 76.7 | 175.4 | 98.3 | 139.1 | 67.2 | 41.8 | 23.8 | 26.6 | 50.0 | 33.1 | ||
| 53.2 | 103.8 | 86.2 | 54.4 | 36.8 | 22.8 | 90.2 | 31.1 | 36.3 | 55.3 | ||
| 41.2 | 63.2 | 33.6 | 62.3 | 32.6 | 31.2 | 50.4 | 57.5 | 24.7 | 26.1 | ||
| 72.0 | 66.2 | 72.3 | 30.5 | 36.4 | 26.9 | 105.2 | 42.0 | 49.9 | 28.3 | ||
| 65.6 | 104.4 | 75.2 | 102.1 | 101.3 | 102.4 | 23.8 | 112.8 | 49.3 | 64.2 | ||
| 51.1 | 115.2 | 148.0 | 47.4 | 47.4 | 42.3 | 33.7 | 110.2 | 118.5 | 37.3 | ||
| 31.2 | 47.2 | 48.3 | 94.5 | 23.9 | 29.5 | 34.5 | 69.4 | 76.0 | 103.9 | ||
| 28.1 | 98.5 | 96.4 | 25.3 | 49.7 | 34.9 | 52.7 | 35.9 | 93.8 | 107.9 | ||
| 91.0 | 127.4 | 140.8 | 101.4 | 41.1 | 53.6 | 25.9 | 26.8 | 113.6 | 77.9 | ||
| 33.5 | 139.1 | 93.1 | 52.6 | 39.9 | 44.4 | 77.3 | 89.1 | 81.1 | 63.3 | ||
| 28.5 | 117.9 | 91.2 | 57.1 | 186.9 | 131.9 | 46.9 | 59.8 | 131.8 | 37.1 | ||
| 25.8 | 88.2 | 45.4 | 24.9 | 122.9 | 21.7 | 24.1 | 53.5 | 30.3 | 55.3 | ||
| 39.7 | 62.7 | 52.9 | 107.8 | 55.0 | 50.0 | 91.6 | 34.9 | 27.1 | 28.4 | ||
| 106.6 | 92.3 | 106.2 | 217.9 | 38.9 | 66.3 | 49.9 | 74.7 | 37.0 | 47.5 | ||
| 27.8 | 87.1 | 52.9 | 158.9 | 40.8 | 59.7 | 105.0 | 34.8 | 23.0 | 55.9 | ||
| 35.9 | 69.8 | 57.3 | 50.9 | 186.5 | 151.5 | 24.1 | 135.5 | 68.4 | 97.8 | ||
| 37.8 | 52.3 | 42.3 | 98.2 | 118.7 | 28.4 | 35.4 | 130.0 | 60.5 | 67.0 | ||
| 72.8 | 42.3 | 58.1 | 122.9 | 29.5 | 33.7 | 30.1 | 46.4 | 26.5 | 54.6 | ||
| 32.6 | 44.9 | 30.8 | 75.9 | 25.8 | 30.1 | 46.7 | 54.1 | 45.4 | 69.8 | ||
| 30.3 | 34.6 | 31.1 | 54.5 | 116.2 | 102.8 | 100.8 | 105.8 | 59.1 | 115.7 | ||
| 27.5 | 36.3 | 62.3 | 29.0 | 53.3 | 48.1 | 55.8 | 100.1 | 79.1 | 75.6 | ||
| 100.3 | 24.1 | 58.2 | 58.7 | 21.1 | 31.1 | 65.9 | 96.2 | 48.2 | 26.5 | ||
| 91.5 | 42.0 | 53.5 | 164.1 | 121.0 | 78.2 | 71.7 | 52.9 | 52.4 | 49.1 | ||
| 79.4 | 44.7 | 123.4 | 106.4 | 67.4 | 69.0 | 31.5 | 65.2 | 77.4 | 23.0 | ||
| 28.6 | 46.1 | 33.6 | 97.5 | 127.2 | 94.8 | 161.5 | 155.6 | 78.7 | 50.7 | ||
| 30.4 | 45.4 | 59.9 | 55.2 | 67.0 | 56.2 | 81.7 | 161.3 | 56.3 | 30.6 | ||
| 22.8 | 35.2 | 71.8 | 59.1 | 52.3 | 143.3 | 39.1 | 26.0 | 173.4 | 34.5 | ||
| Mean | 58.6 | 105.5 | 70.8 | 75.6 | 68.4 | 61.2 | 60.5 | 72.4 | 67.6 | 54.8 | 69.5 ± 14.3 |
| MOD#1 | MOD#2 | MOD#3 | MOD#4 | MOD#5 | MOD#6 | MOD#7 | MOD#8 | MOD#9 | MOD#10 | Overall Mean ± SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Labial | 84.1 | 102.6 | 54.6 | 81.4 | 62.5 | 74.6 | 142.2 | 86.1 | 111.4 | 66.1 | |
| Mesial | 88.6 | 80.3 | 99.5 | 32.0 | 66.6 | 151.9 | 135.3 | 92.8 | 71.6 | 87.1 | |
| Distal | 32.3 | 88.6 | 70.4 | 85.6 | 106.9 | 78.0 | 102.1 | 63.1 | 67.6 | 112.9 | |
| Palatal | 43.9 | 70.4 | 156.0 | 53.5 | 83.6 | 119.5 | 93.3 | 131.9 | 95.2 | 87.2 | |
| Mean | 62.2 | 85.5 | 95.1 | 63.1 | 79.9 | 106 | 118.2 | 93.5 | 86.5 | 88.3 | 87.8 ± 17.2 |
| MOD#1 | MOD#2 | MOD#3 | MOD#4 | MOD#5 | MOD#6 | MOD#7 | MOD#8 | MOD#9 | MOD#10 | Mean ± SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tolerance | 4.3 | 3.1 | 4.2 | 4.7 | 5.0 | 5.5 | 3.0 | 3.6 | 5.6 | 4.3 | 4.3 ± 0.9 |
References
- Ludlow, M.; Renne, W. Digital workflow in implant dentistry. Curr. Oral Health Rep. 2017, 4, 131–135. [Google Scholar] [CrossRef]
- Van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Barazanchi, A.; Li, K.C.; Al-Amleh, B.; Lyons, K.; Waddell, J.N. Additive technology: Update on current materials and applications in dentistry. J. Prosthodont. 2017, 26, 156–163. [Google Scholar] [CrossRef]
- Block, M.S. Dental implants: The last 100 years. J. Oral Maxillofac. Surg. 2018, 76, 11–26. [Google Scholar] [CrossRef]
- Patel, N. Integrating three-dimensional digital technologies for comprehensive implant dentistry. J. Am. Dent. Assoc. 2010, 141, 20s–24s. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Mehl, A.; Mormann, W.H.; Reich, S. Intraoral scanning systems—A current overview. Int. J. Comput. Dent. 2015, 18, 101–129. [Google Scholar]
- Joda, T.; Gallucci, G.O. The virtual patient in dental medicine. Clin. Oral Implants Res. 2015, 26, 725–726. [Google Scholar] [CrossRef]
- Joda, T.; Wolfart, S.; Reich, S.; Zitzmann, N.U. Virtual dental patient: How long until it’s here? Curr. Oral Health Rep. 2018, 5, 116–120. [Google Scholar] [CrossRef]
- Mangano, F.; Shibli, J.A.; Fortin, T. Digital dentistry: New materials and techniques. Int. J. Dent. 2016, 2016, 5261247. [Google Scholar] [CrossRef] [PubMed]
- Scarfe, W.C.; Farman, A.G. What is cone-beam CT and how does it work? Dent. Clin. North Am. 2008, 52, 707–730. [Google Scholar] [CrossRef]
- Wesemann, C.; Muallah, J.; Mah, J.; Bumann, A. Accuracy and efficiency of full-arch digitalization and 3d printing: A comparison between desktop model scanners, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing. Quintessence Int. 2017, 48, 41–50. [Google Scholar]
- Vecsei, B.; Joos-Kovacs, G.; Borbely, J.; Hermann, P. Comparison of the accuracy of direct and indirect three-dimensional digitizing processes for CAD/CAM systems—An in vitro study. J. Prosthodontics Res. 2017, 61, 177–184. [Google Scholar] [CrossRef]
- Kirschneck, C.; Kamuf, B.; Putsch, C.; Chhatwani, S.; Bizhang, M.; Danesh, G. Conformity, reliability and validity of digital dental models created by clinical intraoral scanning and extraoral plaster model digitization workflows. Comput. Biol. Med. 2018, 100, 114–122. [Google Scholar] [CrossRef]
- Sancho-Puchades, M.; Fehmer, V.; Hammerle, C.; Sailer, I. Advanced smile diagnostics using CAD/CAM mock-ups. Int. J. Esthet. Dent. 2015, 10, 374–391. [Google Scholar]
- Mangano, C.; Luongo, F.; Migliario, M.; Mortellaro, C.; Mangano, F.G. Combining intraoral scans, cone beam computed tomography and face scans: The virtual patient. J. Craniofac. Surg. 2018, 29, 2241–2246. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Neugebauer, J.; Stachulla, G.; Ritter, L.; Dreiseidler, T.; Mischkowski, R.A.; Keeve, E.; Zoller, J.E. Computer-aided manufacturing technologies for guided implant placement. Expert Rev. Med. Devices 2010, 7, 113–129. [Google Scholar] [CrossRef]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Siadat, H.; Alikhasi, M.; Beyabanaki, E. Interim prosthesis options for dental implants. J. Prosthodont. 2017, 26, 331–338. [Google Scholar] [CrossRef]
- Kan, J.Y.K.; Rungcharassaeng, K.; Deflorian, M.; Weinstein, T.; Wang, H.L.; Testori, T. Immediate implant placement and provisionalization of maxillary anterior single implants. Periodontol. 2000 2018, 77, 197–212. [Google Scholar] [CrossRef]
- Ganeles, J.; Wismeijer, D. Early and immediately restored and loaded dental implants for single-tooth and partial-arch applications. Int. J. Oral Maxillofac. Implants 2004, 19, 92–102. [Google Scholar]
- Kupeyan, H.K.; May, K.B. Implant and provisional crown placement: A one stage protocol. Implant Dent. 1998, 7, 213–219. [Google Scholar] [CrossRef]
- Wohrle, P.S. Single-tooth replacement in the aesthetic zone with immediate provisionalization: Fourteen consecutive case reports. Pract. Periodontics Aesthet. Dent. 1998, 10, 1107–1114. [Google Scholar]
- Touati, B.; Guez, G. Immediate implantation with provisionalization: From literature to clinical implications. Pract. Proced Aesthet Dent 2002, 14, 699–707. [Google Scholar]
- Kan, J.Y.; Rungcharassaeng, K.; Lozada, J. Immediate placement and provisionalization of maxillary anterior single implants: 1-year prospective study. Int. J. Oral Maxillofac. Implants 2003, 18, 31–39. [Google Scholar]
- Cooper, L.F.; Reside, G.J.; Raes, F.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M.; De Bruyn, H. Immediate provisionalization of dental implants placed in healed alveolar ridges and extraction sockets: A 5-year prospective evaluation. Int. J. Oral Maxillofac. Implants 2014, 29, 709–717. [Google Scholar] [CrossRef]
- Cochran, D.L.; Morton, D.; Weber, H.P. Consensus statements and recommended clinical procedures regarding loading protocols for endosseous dental implants. Int. J. Oral Maxillofac. Implants 2004, 19, 109–113. [Google Scholar]
- Feine, J.; Abou-Ayash, S.; Al Mardini, M.; de Santana, R.B.; Bjelke-Holtermann, T.; Bornstein, M.M.; Braegger, U.; Cao, O.; Cordaro, L.; Eycken, D. Group 3 ITI consensus report: Patient-reported outcome measures associated with implant dentistry. Clin. Oral Implants Res. 2018, 29, 270–275. [Google Scholar] [CrossRef]
- Zuiderveld, E.G.; Meijer, H.J.A.; den Hartog, L.; Vissink, A.; Raghoebar, G.M. Effect of connective tissue grafting on peri-implant tissue in single immediate implant sites: A rct. J. Clin. Periodontol. 2018, 45, 253–264. [Google Scholar] [CrossRef]
- Oh, K.C.; Jeon, C.; Park, J.M.; Shim, J.S. Digital workflow to provide an immediate interim restoration after single-implant placement by using a surgical guide and a matrix-positioning device. J. Prosthet. Dent. 2019, 121, 17–21. [Google Scholar] [CrossRef]
- Hui, E.; Chow, J.; Li, D.; Liu, J.; Wat, P.; Law, H. Immediate provisional for single-tooth implant replacement with branemark system: Preliminary report. Clin. Implant Dent. Relat. Res. 2001, 3, 79–86. [Google Scholar] [CrossRef]
- Raico Gallardo, Y.N.; da Silva-Olivio, I.R.T.; Mukai, E.; Morimoto, S.; Sesma, N.; Cordaro, L. Accuracy comparison of guided surgery for dental implants according to the tissue of support: A systematic review and meta-analysis. Clin. Oral Implants Res. 2017, 28, 602–612. [Google Scholar] [CrossRef]
- Nickenig, H.J.; Wichmann, M.; Hamel, J.; Schlegel, K.A.; Eitner, S. Evaluation of the difference in accuracy between implant placement by virtual planning data and surgical guide templates versus the conventional free-hand method—A combined in vivo–in vitro technique using cone-beam CT (Part II). J. Craniomaxillofac. Surg. 2010, 38, 488–493. [Google Scholar] [CrossRef]
- D’Haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontol. 2000 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Van Assche, N.; van Steenberghe, D.; Guerrero, M.E.; Hirsch, E.; Schutyser, F.; Quirynen, M.; Jacobs, R. Accuracy of implant placement based on pre-surgical planning of three-dimensional cone-beam images: A pilot study. J. Clin. Periodontol. 2007, 34, 816–821. [Google Scholar] [CrossRef]
- Younes, F.; Cosyn, J.; De Bruyckere, T.; Cleymaet, R.; Bouckaert, E.; Eghbali, A. A randomized controlled study on the accuracy of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients. J. Clin. Periodontol. 2018, 45, 721–732. [Google Scholar] [CrossRef]
- Vermeulen, J. The accuracy of implant placement by experienced surgeons: Guided vs freehand approach in a simulated plastic model. Int. J. Oral Maxillofac. Implants 2017, 32, 617–624. [Google Scholar] [CrossRef]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef]
- Rehmann, P.; Sichwardt, V.; Wostmann, B. Intraoral scanning systems: Need for maintenance. Int. J. Prosthodontics 2017, 30, 27–29. [Google Scholar] [CrossRef]
- Huang, Z.; Zhang, L.; Zhu, J.; Zhang, X. Clinical marginal and internal fit of metal ceramic crowns fabricated with a selective laser melting technology. J. Prosthet. Dent. 2015, 113, 623–627. [Google Scholar] [CrossRef]
- Reich, S.; Wichmann, M.; Nkenke, E.; Proeschel, P. Clinical fit of all-ceramic three-unit fixed partial dentures, generated with three different CAD/CAM systems. Eur. J. Oral Sci. 2005, 113, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.C.; Park, J.M.; Shim, J.S.; Kim, J.H.; Kim, J.E.; Kim, J.H. Assessment of metal sleeve-free 3d-printed implant surgical guides. Dent. Mater. 2019, 35, 468–476. [Google Scholar] [CrossRef]
- Muller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the trios pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar] [PubMed]
- Jeong, I.D.; Lee, J.J.; Jeon, J.H.; Kim, J.H.; Kim, H.Y.; Kim, W.C. Accuracy of complete-arch model using an intraoral video scanner: An in vitro study. J. Prosthet. Dent. 2016, 115, 755–759. [Google Scholar] [CrossRef]
- Fokas, G.; Vaughn, V.M.; Scarfe, W.C.; Bornstein, M.M. Accuracy of linear measurements on CBCT images related to presurgical implant treatment planning: A systematic review. Clin. Oral Implants Res. 2018, 29, 393–415. [Google Scholar] [CrossRef]
- Abduo, J.; Lyons, K.; Bennamoun, M. Trends in computer-aided manufacturing in prosthodontics: A review of the available streams. Int. J. Dent. 2014, 2014, 783948. [Google Scholar] [CrossRef]
- Kim, S.Y.; Shin, Y.S.; Jung, H.D.; Hwang, C.J.; Baik, H.S.; Cha, J.Y. Precision and trueness of dental models manufactured with different 3-dimensional printing techniques. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 144–153. [Google Scholar] [CrossRef]
- McLean, J.W.; von Fraunhofer, J.A. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Kelvin Khng, K.Y.; Ettinger, R.L.; Armstrong, S.R.; Lindquist, T.; Gratton, D.G.; Qian, F. In vitro evaluation of the marginal integrity of CAD/CAM interim crowns. J. Prosthet. Dent. 2016, 115, 617–623. [Google Scholar] [CrossRef]
- Van Assche, N.; Quirynen, M. Tolerance within a surgical guide. Clin. Oral Implants Res. 2010, 21, 455–458. [Google Scholar] [CrossRef]
- Koop, R.; Vercruyssen, M.; Vermeulen, K.; Quirynen, M. Tolerance within the sleeve inserts of different surgical guides for guided implant surgery. Clin. Oral Implants Res. 2013, 24, 630–634. [Google Scholar] [CrossRef]
- Munker, T.; van de Vijfeijken, S.; Mulder, C.S.; Vespasiano, V.; Becking, A.G.; Kleverlaan, C.J.; Becking, A.G.; Dubois, L.; Karssemakers, L.H.E.; Milstein, D.M.J. Effects of sterilization on the mechanical properties of poly (methyl methacrylate) based personalized medical devices. J. Mech. Behav. Biomed. Mater. 2018, 81, 168–172. [Google Scholar] [CrossRef]




| MOD#1 | MOD#2 | MOD#3 | MOD#4 | MOD#5 | MOD#6 | MOD#7 | MOD#8 | MOD#9 | MOD#10 | Mean ± SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Angular deviation (°) | −5.89 | −0.05 | −9.07 | −11.87 | 5.71 | −12.49 | −1.17 | 17.90 | 3.03 | 2.24 | 6.94 ± 5.78 (Absolute values) |
| RMS (µm) | 60.8 | 53.4 | 111.7 | 99.5 | 87.3 | 80.7 | 104.8 | 103.1 | 91.1 | 65.3 | 85.8 ± 20.2 |
| Procedures | Factors That May Contribute to Error Reduction | Efforts to Reduce Errors | Methods to Confirm That Potential Sources of Error Had Been Minimized | |
|---|---|---|---|---|
| Data acquisition | Intraoral scanning | Calibration procedures | Calibrated the intraoral scanner before obtaining the data | By assessing the accuracy (trueness and precision) of the intraoral scanner |
| Scanning strategy | Unified scanning strategy | |||
| CBCT | Calibration procedures | Calibrated the CBCT scanner before obtaining the data | ||
| Voxel size | Applied voxel size of 0.2 mm3 | |||
| Data processing | Superimposition (CBCT and intraoral scan data) | Careful selection of three pairwise points | Referred to the color maps within the software | By confirming that the color maps were mostly within the range of ± 200 µm |
| Data production | Computer-assisted implant surgical guides | Selection of additive manufacturing principles | Used a polyjet 3D printer | |
| Custom abutments and immediate provisional restorations | Selection of milling machine | Used a five-axis milling machine for the fabrication of provisional restorations | ||
| Proper adaptation between the two | Used a computer numerical control automatic lathe for the fabrication of custom abutments | By evaluating the marginal gap | ||
| Appropriate amount of cement use | Used a minimal amount of dental cement | |||
| Selection of proper support position | Determined the appropriate support attachment position for provisional restorations | |||
| Pre-operative preparation | Sterilization/Disinfection | Selection of appropriate sterilization/disinfection methods | Sterilized with ethylene oxide gas for the screw-type immediate provisional restorations | |
| Disinfected with 0.12% chlorhexidine digluconate solution for the surgical guides | ||||
| Performance | Placement of the implant surgical guides | Adaptation onto the typodonts | Created windows on the guide in the planning stage | By inspecting the adaptation via windows and absence of guide movement |
| Guide hole tolerance | Used a polyjet 3D printer | By evaluating the guide hole tolerance | ||
| Surgical procedures | Angle at which the fixture driver is viewed | Tried to view the fixture driver from a vertical perspective | ||
| Bony imitation structure of the typodonts | Conducted a pilot study to gauge differences between typodont structures and real bone in clinical settings | |||
| Prosthodontic procedures | Amount of torque applied | Provided consistent torque throughout the study with the torque gauge | By confirming the values on the torque gauge | |
| Improper seating of the screw-type provisional restorations into the fixtures due to the tight interproximal contacts | Designed the restoration to be free of contacts with adjacent teeth | By confirming the absence of interproximal contacts after connecting the prosthesis | ||
| Post-operative intraoral scanning | Calibration procedures | Calibrated the scanner before its use | Not applicable: had been confirmed during the pre-operative evaluation stage | |
| Scanning strategy | Applied the same scanning protocols as in the pre-operative scanning | |||
| Final verification | Superimposition | Regions of interest | Regions of interest were restricted to the tooth portion | |
| Overall consideration | Inter-operator variability | All scans and surgical/prosthodontic procedures performed by a single experienced clinician | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, K.C.; Kim, J.-H.; Woo, C.-W.; Moon, H.S. Accuracy of Customized Prefabricated Screw-Type Immediate Provisional Restorations after Single-Implant Placement. J. Clin. Med. 2019, 8, 490. https://doi.org/10.3390/jcm8040490
Oh KC, Kim J-H, Woo C-W, Moon HS. Accuracy of Customized Prefabricated Screw-Type Immediate Provisional Restorations after Single-Implant Placement. Journal of Clinical Medicine. 2019; 8(4):490. https://doi.org/10.3390/jcm8040490
Chicago/Turabian StyleOh, Kyung Chul, Jee-Hwan Kim, Chang-Woo Woo, and Hong Seok Moon. 2019. "Accuracy of Customized Prefabricated Screw-Type Immediate Provisional Restorations after Single-Implant Placement" Journal of Clinical Medicine 8, no. 4: 490. https://doi.org/10.3390/jcm8040490
APA StyleOh, K. C., Kim, J. -H., Woo, C. -W., & Moon, H. S. (2019). Accuracy of Customized Prefabricated Screw-Type Immediate Provisional Restorations after Single-Implant Placement. Journal of Clinical Medicine, 8(4), 490. https://doi.org/10.3390/jcm8040490