Fast Tac Metabolizers at Risk—It is Time for a C/D Ratio Calculation


Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Tacrolimus Metabolism Rate
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. Patient and Overall Allograft Survival
3.3. Renal Function
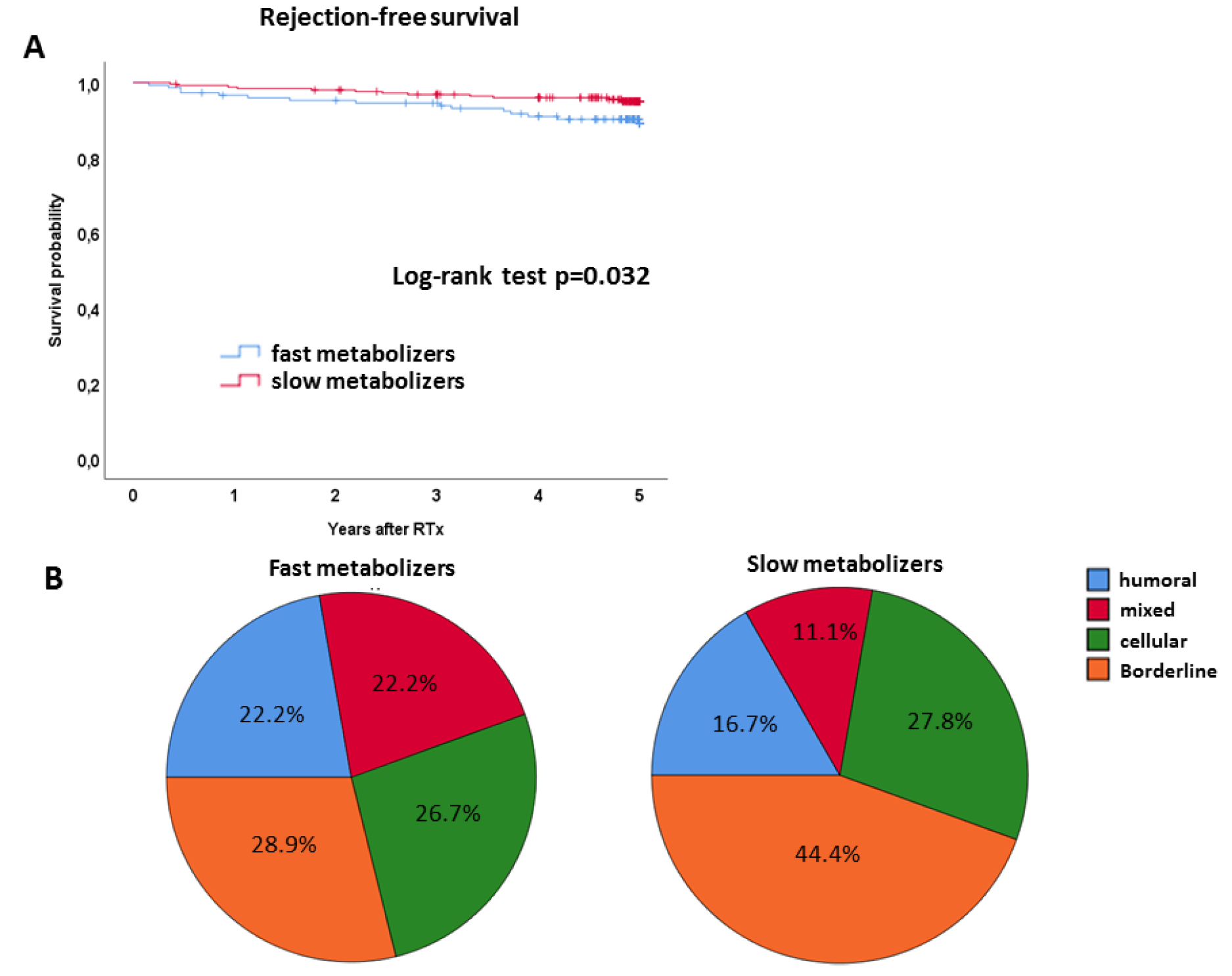
3.4. Rejections
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 9. [CrossRef]
- Schutte-Nutgen, K.; Tholking, G.; Suwelack, B.; Reuter, S. Tacrolimus - Pharmacokinetic Considerations for Clinicians. Curr. Drug. Metab. 2018, 19, 342–350. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Li, J.-L.; Meng, F.-H.; Wang, X.-D.; Liu, T.; Li, J.; Liu, L.-S.; Fu, Q.; Huang, M.; Wang, C.-X. Individualization of tacrolimus dosage basing on cytochrome P450 3A5 polymorphism—a prospective, randomized, controlled study. Clin. Transplant. 2013, 27, E272–E281. [Google Scholar] [CrossRef]
- Boughton, O.; Borgulya, G.; Cecconi, M.; Fredericks, S.; Moreton-Clack, M.; MacPhee, I.A.M. A published pharmacogenetic algorithm was poorly predictive of tacrolimus clearance in an independent cohort of renal transplant recipients. Br. J. Clin. Pharmacol. 2013, 76, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Picard, N.; Bergan, S.; Marquet, P.; van Gelder, T.; Wallemacq, P.; Hesselink, D.A.; Haufroid, V. Pharmacogenetic Biomarkers Predictive of the Pharmacokinetics and Pharmacodynamics of Immunosuppressive Drugs. Ther. Drug Monit. 2016, 38 (Suppl. 1), S57–S69. [Google Scholar] [CrossRef]
- Mourad, M.; Wallemacq, P.; De Meyer, M.; Brandt, D.; van Kerkhove, V.; Malaise, J.; Chaïb Eddour, D.; Lison, D.; Haufroid, V. The influence of genetic polymorphisms of cytochrome P450 3A5 and ABCB1 on starting dose- and weight-standardized tacrolimus trough concentrations after kidney transplantation in relation to renal function. Clin. Chem. Lab. Med. 2006, 44, 1192–1198. [Google Scholar] [CrossRef]
- Pallet, N.; Etienne, I.; Buchler, M.; Bailly, E.; Hurault de Ligny, B.; Choukroun, G.; Colosio, C.; Thierry, A.; Vigneau, C.; Moulin, B.; et al. Long-Term Clinical Impact of Adaptation of Initial Tacrolimus Dosing to CYP3A5 Genotype. Am. J. Transplant. 2016, 16, 2670–2675. [Google Scholar] [CrossRef] [PubMed]
- Thölking, G.; Fortmann, C.; Koch, R.; Gerth, H.U.; Pabst, D.; Pavenstädt, H.; Kabar, I.; Hüsing, A.; Wolters, H.; Reuter, S.; et al. The tacrolimus metabolism rate influences renal function after kidney transplantation. PLoS ONE 2014, 9, e111128, eCollection 2014. [Google Scholar] [CrossRef]
- Kuypers, D.R.J.; Naesens, M.; de Jonge, H.; Lerut, E.; Verbeke, K.; Vanrenterghem, Y. Tacrolimus dose requirements and CYP3A5 genotype and the development of calcineurin inhibitor-associated nephrotoxicity in renal allograft recipients. Ther. Drug Monit. 2010, 32, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Egeland, E.J.; Robertsen, I.; Hermann, M.; Midtvedt, K.; Størset, E.; Gustavsen, M.T.; Reisæter, A.V.; Klaasen, R.; Bergan, S.; Holdaas, H.; et al. High Tacrolimus Clearance Is a Risk Factor for Acute Rejection in the Early Phase After Renal Transplantation. Transplantation 2017, 101, e273–e279. [Google Scholar] [CrossRef]
- Ohtani, H.; Barter, Z.; Minematsu, T.; Makuuchi, M.; Sawada, Y.; Rostami-Hodjegan, A. Bottom-up modeling and simulation of tacrolimus clearance: prospective investigation of blood cell distribution, sex and CYP3A5 expression as covariates and assessment of study power. Biopharm. Drug Dispos. 2011, 32, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Thölking, G.; Schmidt, C.; Koch, R.; Schuette-Nuetgen, K.; Pabst, D.; Wolters, H.; Kabar, I.; Hüsing, A.; Pavenstädt, H.; Reuter, S.; et al. Influence of tacrolimus metabolism rate on BKV infection after kidney transplantation. Sci. Rep. 2016, 6, 32273. [Google Scholar] [CrossRef]
- Taber, D.J.; Gebregziabher, M.G.; Srinivas, T.R.; Chavin, K.D.; Baliga, P.K.; Egede, L.E. African-American race modifies the influence of tacrolimus concentrations on acute rejection and toxicity in kidney transplant recipients. Pharmacotherapy 2015, 35, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Li, H.; Meng, Y.; Liu, H.; Yang, L.; Xu, T.; Yu, J.; Zhao, N.; Liu, Y. Effect of CYP3A5 polymorphism on the pharmacokinetics of tacrolimus and acute rejection in renal transplant recipients: Experience at a single centre. Int. J. Clin. Pract. Suppl. 2015, 183, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Genvigir, F.D.V.; Salgado, P.C.; Felipe, C.R.; Luo, E.Y.F.; Alves, C.; Cerda, A.; Tedesco-Silva, H.; Medina-Pestana, J.O.; Oliveira, N.; Rodrigues, A.C.; et al. Influence of the CYP3A4/5 genetic score and ABCB1 polymorphisms on tacrolimus exposure and renal function in Brazilian kidney transplant patients. Pharmacogenet. Genomics 2016, 26, 462–472. [Google Scholar] [CrossRef]
- Thölking, G.; Siats, L.; Fortmann, C.; Koch, R.; Hüsing, A.; Cicinnati, V.R.; Gerth, H.U.; Wolters, H.H.; Anthoni, C.; Pavenstädt, H.; et al. Tacrolimus Concentration/Dose Ratio is Associated with Renal Function After Liver Transplantation. Ann. Transplant. 2016, 21, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Cox, D.R. Regression Models and Life-Tables. J. Roy. Statisti. Soc. Ser. B Metho. 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Barraclough, K.A.; Staatz, C.E.; Johnson, D.W.; Lee, K.J.; McWhinney, B.C.; Ungerer, J.P.; Hawley, C.M.; Campbell, S.B.; Leary, D.R.; Isbel, N.M. Kidney transplant outcomes are related to tacrolimus, mycophenolic acid and prednisolone exposure in the first week. Transpl. Int. 2012, 25, 1182–1193. [Google Scholar] [CrossRef]
- Bouamar, R.; Shuker, N.; Hesselink, D.A.; Weimar, W.; Ekberg, H.; Kaplan, B.; Bernasconi, C.; van Gelder, T. Tacrolimus predose concentrations do not predict the risk of acute rejection after renal transplantation: A pooled analysis from three randomized-controlled clinical trials(†). Am. J. Transplant. 2013, 13, 1253–1261. [Google Scholar] [CrossRef]
- Farrugia, D.; Cheshire, J.; Begaj, I.; Khosla, S.; Ray, D.; Sharif, A. Death within the first year after kidney transplantation--an observational cohort study. Transpl. Int. 2014, 27, 262–270. [Google Scholar] [CrossRef]
- Hart, A.; Smith, J.M.; Skeans, M.A.; Gustafson, S.K.; Wilk, A.R.; Robinson, A.; Wainright, J.L.; Haynes, C.R.; Snyder, J.J.; Kasiske, B.L.; et al. OPTN/SRTR 2016 Annual Data Report: Kidney. Am. J. Transplant. 2018, 18 Suppl 1, 18–113. [Google Scholar] [CrossRef]
- Thölking, G.; Schuette-Nuetgen, K.; Vogl, T.; Dobrindt, U.; Kahl, B.C.; Brand, M.; Pavenstädt, H.; Suwelack, B.; Koch, R.; Reuter, S. Male kidney allograft recipients at risk for urinary tract infection? PLoS ONE 2017, 12, e0188262. [Google Scholar]
- Kinnunen, S.; Karhapää, P.; Juutilainen, A.; Finne, P.; Helanterä, I. Secular Trends in Infection-Related Mortality after Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2018, 13, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Abeling, T.; Scheffner, I.; Karch, A.; Broecker, V.; Koch, A.; Haller, H.; Schwarz, A.; Gwinner, W. Risk factors for death in kidney transplant patients: Analysis from a large protocol biopsy registry. Nephrol. Dial. Transplant. 2018, 13, 755–762. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Slow Metabolizers (n = 253) | Fast Metabolizers (n = 148) | p-Value | |
|---|---|---|---|
| Tac mean trough level at 3 months (ng/mL) | 8.6 ± 2.8 | 7.1 ± 2.7 | <0.001 a |
| Tac daily dose at 3 months (mg/day) | 4.9 ± 2.3 | 10.3 ± 4.3 | <0.001 a |
| Age (years, mean ± SD) | 53.0 ± 13.4 | 50.2 ± 13.8 | 0.051 a |
| Male sex, n (%) | 156 (61.7) | 80 (54.1) | 0.142 c |
| BMI (kg/m2, mean ± SD) | 25.2 ± 4.0 | 25.2 ± 4.1 | 0.944 a |
| Pre-existing recipient hypertension, n (%) | 239 (94.5) | 139 (94.6) | 1.000 c |
| Pre-existing recipient diabetes, n (%) | 33 (13.0) | 16 (10.9) | 0.636 c |
| Diagnosis of ESRD, n (%) | 0.411 c | ||
| Hypertension | 20 (7.9) | 11 (7.4) | |
| Diabetes | 11 (4.3) | 1 (0.7) | |
| Polycystic kidney disease | 36 (14.2) | 26 (17.6) | |
| Obstructive Nephropathy | 20 (7.9) | 14 (9.5) | |
| Glomerulonephritis | 103 (40.7) | 53 (35.8) | |
| FSGS | 6 (2.4) | 5 (3.4) | |
| Interstitial nephritis | 4 (1.6) | 2 (1.4) | |
| Vasculitis | 5 (2.0) | 2 (1.4) | |
| Other | 45 (17.8) | 34 (23.0) | |
| Time on dialysis (months, median (IQR)) | 60.5 (25.5, 90.3) | 52.5 (24.9, 87.1) | 0.323 b |
| ≥ 1 prior kidney transplant, n (%) | 39 (15.4) | 19 (12.8) | 0.557 c |
| Living donor transplantation | 58 (22.9) | 44 (29.7) | 0.4 c |
| Number HLA mismatch, n (%) | 1.000 c | ||
| 0–3 | 169 (67.1) | 98 (66.7) | |
| 4–6 | 83 (32.9) | 49 (33.3) | |
| Current PRA, n (%) | 1.000 c | ||
| 0–20% | 248 (98.0) | 145 (98.0) | |
| > 20% | 5 (2.0) | 3 (2.0) | |
| Induction, n (%) | 0.163 c | ||
| Basiliximab | 233 (92.1) | 130 (87.8) | |
| Thymoglobulin | 20 (7.9) | 18 (12.2) | |
| Cold ischaemia time (hours, mean ± SD) | 8.7 ± 4.9 | 8.2 ± 5.4 | 0.419 a |
| Warm ischaemia time (min, mean ± SD) | 31.8 ± 6.9 | 32.2 ± 8.0 | 0.684 a |
| Donor age (years, mean ± SD) | 53.4 ± 16.6 | 54.7 (13.7) | 0.394 a |
| Donor male sex, n (%) | 121 (47.8) | 63 (42.6) | 0.350 c |
| Parameters | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Fast metabolizers vs. slow metabolizers (ref.) | 2.209 (1.034–4.719) | 0.041 | 5.749 (1.556–21.242) | 0.004 |
| Age (years) | 1.057 (1.023–1.093) | 0.001 | - | 0.081 |
| Recipient sex Male vs. female (ref.) | 1.631 (0.714–3.727) | 0.246 | - | 0.262 |
| Recipient BMI (kg/m2) | 0.942 (0.852–1.042) | 0.248 | - | 0.213 |
| Pre-existing recipient hypertension yes vs. no (ref.) | 1.512 (0.205–11.142) | 0.685 | - | 0.635 |
| Pre-existing recipient diabetes yes vs. no (ref.) | 2.206 (0.890–5.468) | 0.087 | - | 0.691 |
| Cause of ESRD | - | 0.852 | - | 0.738 |
| Time on dialysis (months) | 1.002 (0.993–1.011) | 0.714 | - | 0.553 |
| Prior kidney transplantation ≥1 vs. 0 (ref.) | 1.379 (0.522–3.641) | 0.517 | - | 0.707 |
| Donor type Postmortal vs. living donor (ref.) | 2.832 (0.853–9.405) | 0.089 | - | 0.936 |
| Number HLA mismatch 4–6 vs. 0–3 | 2.335 (1.097–4.968) | 0.028 | - | 0.053 |
| Current PRA >20% vs. 0–20% | 1.951 (0.265–14.387) | 0.512 | - | 0.709 |
| Cold ischemia time (hours) | 1.042 (0.972–1.118) | 0.245 | - | 0.668 |
| Donor age (years) | 1.043 (1.014–1.074) | 0.004 | - | 0.540 |
| Donor sex Male vs. female (ref.) | 0.928 (0.434–1.982) | 0.847 | - | 0.266 |
| NODAT yes vs. no (ref.) | 2.983 (1.396–6.373) | 0.005 | 5.150 (1.550–17.110) | 0.005 |
| CMV DNAaemia yes vs. no (ref.) | 0.832 (0.352–1.968) | 0.676 | - | 0.629 |
| Acute rejection within 1 year yes vs. no (ref.) | 1.610 (0.680–3.807) | 0.279 | - | 0.947 |
| eGFR at month 3 (mL/min/1.73m2) | 0.979 (0.960–0.998) | 0.028 | - | 0.999 |
| eGFR at month 12 (mL/min/1.73m2) | 0.968 (0.937–1.000) | 0.047 | - | 0.166 |
| Parameters | Univariable | p-Value | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Fast metabolizers vs. slow metabolizers (ref.) | 1.772 (1.006–3.121) | 0.047 | 2.715 (1.231–5.989) | 0.012 |
| Age (years) | 1.056 (1.030–1.082) | <0.001 | - | 0.673 |
| Recipient sex Male vs. female (ref.) | 0.957 (0.539–1.698) | 0.880 | - | 0.354 |
| Recipient BMI (kg/m2) | 1.018 (0.949–1.092) | 0.619 | - | 0.715 |
| Pre-existing recipient hypertension yes vs. no (ref.) | 2.797 (0.386–20.272) | 0.309 | - | 0.401 |
| Pre-existing recipient diabetes yes vs. no (ref.) | 2.044 (1.018–4.102) | 0.044 | - | 0.827 |
| Cause of ESRD | - | 0.717 | - | 0.942 |
| Time on dialysis (months) | 0.999 (0.992–1.007) | 0.833 | - | 0.376 |
| Prior kidney transplantation ≥1 vs. 0 (ref.) | 0.702 (0.278–1.772) | 0.454 | - | 0.331 |
| Donor type Postmortem vs. living donor (ref.) | 3.121 (1.236–7.879) | 0.016 | - | 0.774 |
| Number HLA mismatch 4–6 vs. 0–3 | 1.814 (1.028–3.201) | 0.040 | - | 0.504 |
| Current PRA >20% vs. 0–20% | 1.073 (0.148–7.780) | 0.944 | - | 0.709 |
| Cold ischemia time (hours) | 1.060 (1.006–1.116) | 0.028 | - | 0.427 |
| Donor age (years) | 1.052 (1.029–1.075) | <0.001 | - | 0.485 |
| Donor sex Male vs. female (ref.) | 0.567 (0.311–1.034) | 0.064 | - | 0.140 |
| NODAT yes vs. no (ref.) | 3.163 (1.787–5.596) | <0.001 | 3.203 (1.451–7.072) | 0.003 |
| CMV DNAaemia yes vs. no (ref.) | 1.331 (0.737–2.404) | 0.344 | - | 0.443 |
| Acute rejection within one year yes vs. no (ref.) | 1.909 (1.024–3.558) | 0.042 | - | 0.943 |
| eGFR at month 3 (mL/min/1.73m2) | 0.958 (0.941–0.976) | <0.001 | - | 0.851 |
| eGFR at month 12 (mL/min/1.73m2) | 0.941 (0.916–0.967) | <0.001 | 0.943 (0.915–0.971) | <0.001 |
| Slow Metabolizers (n = 12) | Fast Metabolizers (n = 15) | |
|---|---|---|
| Cardiovascular | 4 (33.3) | 6 (40) |
| Infection | 5 (41.7) | 4 (26.7) |
| Tumor disease | 2 (16.7) | - |
| Unknown | 1 (8.3%) | 5 (33.3) |
| (a) | ||||
| Variable | B | 95% CI | p | |
| Metabolizer type | ||||
| Fast vs. slow (at month 12) | −3.54 | −8.57 to 1.49 | 0.167 | |
| Fast vs slow (time-trends) | −1.07 | −2.10 to −0.05 | 0.040 | |
| R_Sex | ||||
| Male vs. female (at month 12) | −16.21 | −1.26 to −11.61 | <0.001 | |
| Male vs. female (time-trends) | 0.49 | −0.49 to 1.47 | 0.325 | |
| PreHypertension | ||||
| No vs. yes (at month 12) | 0.78 | −9.63 to 11.19 | 0.883 | |
| No vs. yes (time-trends) | 1.26 | −0.79 to 0.20 | 0.240 | |
| PreDiabetes | ||||
| No vs. yes (at month 12) | 4.52 | −3.04 to 12.08 | 0.241 | |
| No vs. yes (time-trends) | 0.91 | −0.68 to 2.51 | 0.262 | |
| Cause of ESRD | ||||
| Cause of ESRD (at month 12) | - | - | 0.010 * | |
| Diabetes vs. Hypertension (at month 12) | 3.72 | −15.38 to 22.82 | 0.703 | |
| Polycystic kidney disease vs. Hypertension (at month 12) | 8.30 | −1.90 to 18.50 | 0.111 | |
| Obstructive Nephropahty vs. Hypertension (at month 12) | 16.20 | 4.91 to 27.48 | 0.005 | |
| Glomerulonephritis vs. Hypertension (at month 12) | 5.82 | −3.12 to 14.76 | 0.202 | |
| FSGS vs. Hypertension (at month 12) | 7.14 | −10.58 to 24.85 | 0.429 | |
| Interstitial nephritis vs. Hypertension (at month 12) | 11.40 | −8.85 to 31.65 | 0.269 | |
| Vasculitis vs. Hypertension (at month 12) | 2.51 | −16.28 to 21.32 | 0.792 | |
| Other vs. Hypertension (at month 12) | 16.81 | 7.14 to 26.48 | 0.001 | |
| Cause of ESRD (time-trends) | - | - | 0.998 * | |
| PriorTx | ||||
| No vs. yes (at month 12) | −8.67 | −15.48 to −1.86 | 0.013 | |
| No vs. yes (time-trends) | 0.25 | −1.13 to 1.63 | 0.719 | |
| DonorType | ||||
| Postmortal vs. Living (at month 12) | −11.15 | −16.40 to −5.90 | <0.001 | |
| Postmortal vs. Living ( time-trends) | 0.47 | −0.60 to 1.55 | 0.387 | |
| HLA Mismatch | ||||
| 0–3 vs. 4–6 (at month 12) | 5.45 | 0.37 to 10.53 | 0.035 | |
| 0–3 vs. 4–6 (time-trends) | −0.21 | −1.25 to 0.83 | 0.696 | |
| CurrentPRA | ||||
| 0–20 vs. >20 (at month 12) | −14.81 | −32.19 to 2.57 | 0.095 | |
| 0–20 vs. >20 (time-trends) | −0.80 | −4.15 to 2.54 | 0.638 | |
| D_Sex | ||||
| Male vs. female (at month 12) | 4.31 | −0.47 to 9.09 | 0.077 | |
| Male vs. female (time-trends) | −0.36 | −1.32 to 0.62 | 0.470 | |
| NODAT | ||||
| No vs. yes (at month 12) | 6.50 | 1.31 to 11.69 | 0.014 | |
| No vs. yes (time-trends) | 0.52 | −0.56 to 1.60 | 0.342 | |
| CMV DNAaemia | ||||
| No vs. yes (at month 12) | 4.46 | −0.74 to 9.66 | 0.093 | |
| No vs. yes (time-trends) | −0.26 | −1.32 to 0.80 | 0.629 | |
| Acute rejection 1 year post RTx | ||||
| No vs. yes (at month 12) | 16.23 | 10.34 to 22.13 | <0.001 | |
| No vs. yes (time-trends) | 0.09 | −1.18 to 1.35 | 0.893 | |
| R-Age (years) | ||||
| R-Age (at month 12) | −0.47 | −0.63 to −0.32 | <0.001 | |
| R-Age (time-trends) | −0.004 | −0.013 to 0.005 | 0.415 | |
| R-BMI | ||||
| R-BMI (at month 12) | −1.12 | −1.67 to −0.57 | <0.001 | |
| R-BMI (time-trends) | −0.008 | −0.027 to 0.011 | 0.405 | |
| Time on Dialysis (month) | ||||
| Time on Dialysis (at month 12) | −0.05 | −0.11 to 0.01 | 0.112 | |
| Time on Dialysis (time-trends) | −0.012 | −0.008 to 0.006 | 0.743 | |
| CIT (hours) | ||||
| CIT (at month 12) | −0.43 | −0.86 to 0.004 | 0.052 | |
| CIT (time-trends) | −0.014 | −0.064 to 0.034 | 0.565 | |
| D_Age (years) | ||||
| D-Age (at month 12) | −0.65 | −0.78 to −0.52 | <0.001 | |
| D-Age (time-trends) | −0.006 | −0.015 to 0.002 | 0.152 | |
| (b) | ||||
| Variable | Estimate | 95% CI | p | |
| At month 12 | ||||
| Metabolizer type: fast vs. slow | −2.48 | −6.47 to 1.51 | 0.222 | |
| D_Age (years) | −0.60 | −0.71 to −0.48 | <0.001 | |
| R_Sex: male vs. female | −12.27 | −15.75 to −8.79 | <0.001 | |
| Donor type: postmortem vs. living | −10.03 | −13.94 to −6.12 | <0.001 | |
| R_BMI (kg/m2) | −0.58 | −1.03 to −0.14 | 0.010 | |
| PreHypertension: no vs. yes | N/S: 0.051 | |||
| PreDiabetes: no vs. yes | N/S: 0.914 | |||
Cause of ESRD
| 10.79 4.72 11.34 2.83 5.16 2.23 −0.31 11.26 | −2.08 to 23.65 −2.57 to 12.02 3.11 to 19.56 −3.53 to 9.19 −6.98 to 17.31 −14.60 to 19.06 −13.54 to 12.93 4.30 to 18.22 | 0.010 * 0.100 0.204 0.007 0.382 0.404 0.794 0.964 0.002 | |
| PriorTx: no vs yes | N/S: 0.225 | |||
| HLAMismatch: 0–3 vs. 4–6 | N/S: 0.713 | |||
| CurrentPRA: 0–20 vs. >20 | N/S: 0.272 | |||
| D_Sex: male vs. female | N/S: 0.107 | |||
| NODAT: no vs. yes | N/S: 0.995 | |||
| CMV DNAaemia: no vs. yes | N/S: 0.417 | |||
| Acute rejection 1 year post RTx: no vs. yes | 14.00 | 9.64 to 18.36 | <0.001 | |
| R_Age (years) | N/S: 0.495 | |||
| Time Dialysis (months) | N/S: 0.112 | |||
| CIT (hours) | N/S: 0.771 | |||
| Time trends | ||||
| Metabolizer type: fast vs. slow | −1.07 | −2.05 to −0.09 | 0.032 | |
| D_Age (years) | N/S: 0.121 | |||
| R_Sex: male vs. female | N/S: 0.240 | |||
| Donor Type: postmortem vs. living | N/S: 0.666 | |||
| R_BMI (kg/m2) | N/S: 0.810 | |||
| PreHypertension: no vs. yes | N/S: 0.366 | |||
| PreDiabetes: no vs. yes | N/S: 0.354 | |||
| Cause of ESRD | N/S: 0.997 * | |||
| PriorTx: no vs. yes | N/S: 0.635 | |||
| HLAMismatch: 0–3 vs. 4–6 | N/S: 0.299 | |||
| CurrentPRA: 0–20 vs. >20 | N/S: 0.708 | |||
| D_Sex: male vs. female | N/S: 0.293 | |||
| NODAT: no vs. yes | N/S: 0.368 | |||
| CMV DNAaemia: no vs. yes | N/S: 0.519 | |||
| Acute rejection1 year post RTx: no vs. yes | N/S: 0.913 | |||
| R_Age (years) | N/S: 0.332 | |||
| Time Dialysis (months) | N/S: 0.840 | |||
| CIT (hours) | N/S: 0.400 | |||
| Parameters | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Fast metabolizers vs. slow metabolizers (ref.) | 1.536 (1.034–2.282) | 0.035 | 1.622 (1.085–2.424) | 0.020 |
| Age (years) | 0.996 (0.981–1.010) | 0.547 | - | 0.615 |
| Recipient sex Male vs. female (ref.) | 1.432 (0.943–2.176) | 0.092 | - | 0.122 |
| Recipient BMI (kg/m2) | 1.057 (1.007–1.110) | 0.026 | 1.073 (1.021–1.128) | 0.006 |
| Pre-existing recipient hypertension yes vs. no (ref.) | 1.379 (0.507–3.751) | 0.529 | - | 0.695 |
| Pre-existing recipient diabetes yes vs. no (ref.) | 1.032 (0.564–1.887) | 0.919 | - | 0.716 |
| Cause of ESRD | - | 0.999 | - | 0.998 |
| Time on dialysis (months) | 1.000 (0.996–1.005) | 0.862 | - | 0.746 |
| Prior kidney transplantation ≥1 vs. 0 (ref.) | 1.632 (0.999–2.665) | 0.051 | 1.850 (1.109–3.087) | 0.027 |
| Donor type Postmortem vs. living donor (ref.) | 0.765 (0.498–1.174) | 0.220 | - | 0.249 |
| Number HLA mismatch 4–6 vs. 0–3 | 1.043 (0.683–1.593) | 0.845 | - | 0.905 |
| Current PRA >20% vs. 0–20% | 1.033 (0.255–4.189) | 0.964 | - | 0.830 |
| Cold ischaemia time (hours) | 0.986 (0.948–1.026) | 0.489 | - | 0.620 |
| Donor age (years) | 1.002 (0.989–1.014) | 0.788 | - | 0.846 |
| Donor sex Male vs. female (ref.) | 0.936 (0.629–1.391) | 0.742 | - | 0.632 |
| Slow Metabolizers (n = 253) | Fast Metabolizers (n = 148) | p-Value | |
|---|---|---|---|
| Type of acute rejection | 0.084 | ||
| No rejection | 199 (78.7) | 103 (69.6) | |
| Humoral | 9 (3.6) | 10 (6.8) | |
| Mixed | 6 (2.4) | 10 (6.8) | |
| Cellular | 15 (5.9) | 12 (8.1) | |
| Borderline | 24 (9.5) | 13 (8.8) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schütte-Nütgen, K.; Thölking, G.; Steinke, J.; Pavenstädt, H.; Schmidt, R.; Suwelack, B.; Reuter, S. Fast Tac Metabolizers at Risk—It is Time for a C/D Ratio Calculation. J. Clin. Med. 2019, 8, 587. https://doi.org/10.3390/jcm8050587
Schütte-Nütgen K, Thölking G, Steinke J, Pavenstädt H, Schmidt R, Suwelack B, Reuter S. Fast Tac Metabolizers at Risk—It is Time for a C/D Ratio Calculation. Journal of Clinical Medicine. 2019; 8(5):587. https://doi.org/10.3390/jcm8050587
Chicago/Turabian StyleSchütte-Nütgen, Katharina, Gerold Thölking, Julia Steinke, Hermann Pavenstädt, René Schmidt, Barbara Suwelack, and Stefan Reuter. 2019. "Fast Tac Metabolizers at Risk—It is Time for a C/D Ratio Calculation" Journal of Clinical Medicine 8, no. 5: 587. https://doi.org/10.3390/jcm8050587
APA StyleSchütte-Nütgen, K., Thölking, G., Steinke, J., Pavenstädt, H., Schmidt, R., Suwelack, B., & Reuter, S. (2019). Fast Tac Metabolizers at Risk—It is Time for a C/D Ratio Calculation. Journal of Clinical Medicine, 8(5), 587. https://doi.org/10.3390/jcm8050587