Characteristics of Individuals with Dry Eye Symptoms without Clinical Diagnosis: Analysis of a Web-Based Survey

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
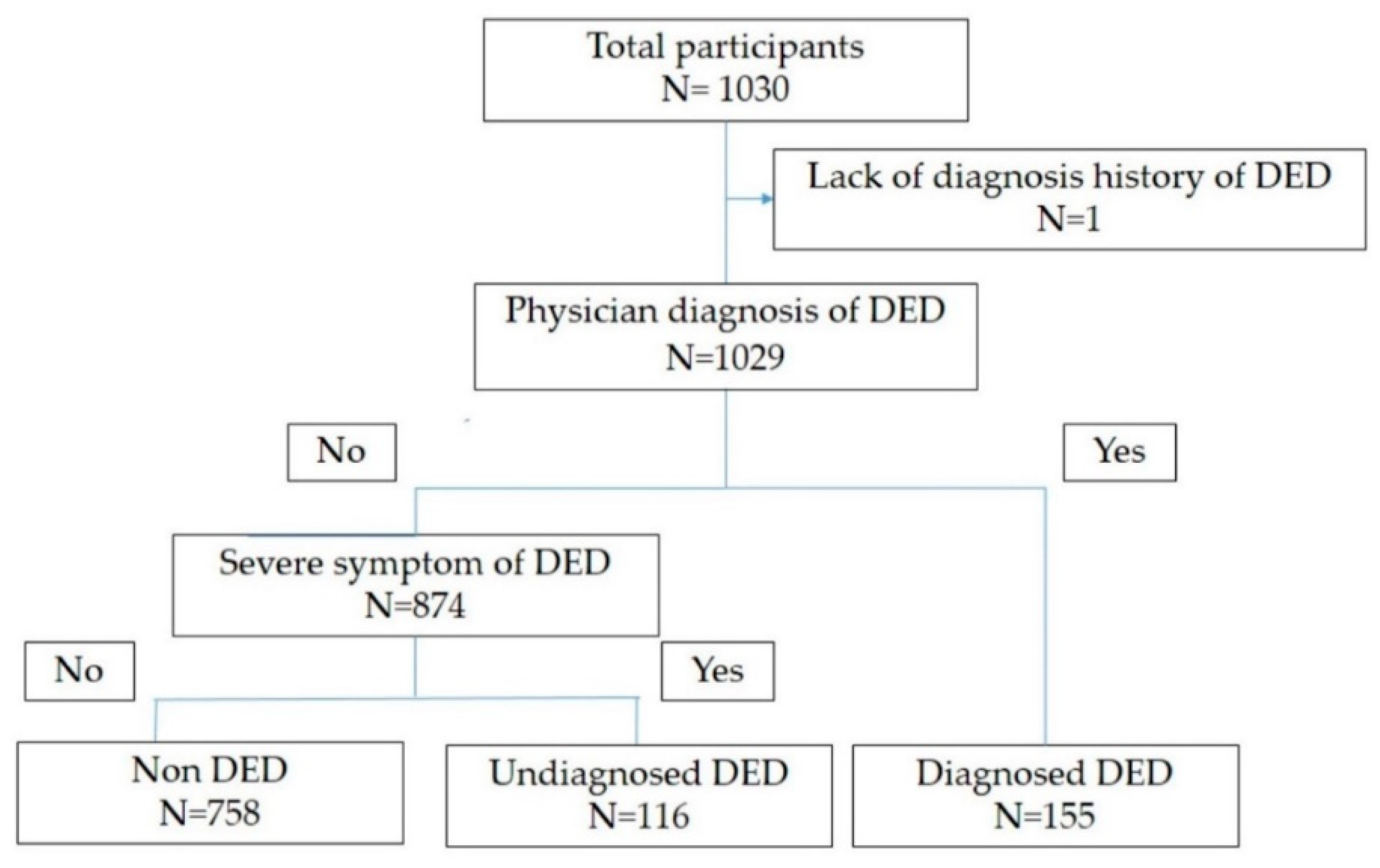
2.1. Study Participants
2.2. Dry Eye Disease Symptoms
2.3. Diagnosis of Dry Eye Disease
2.4. Dry Eye-Related Quality-Of-Life Score
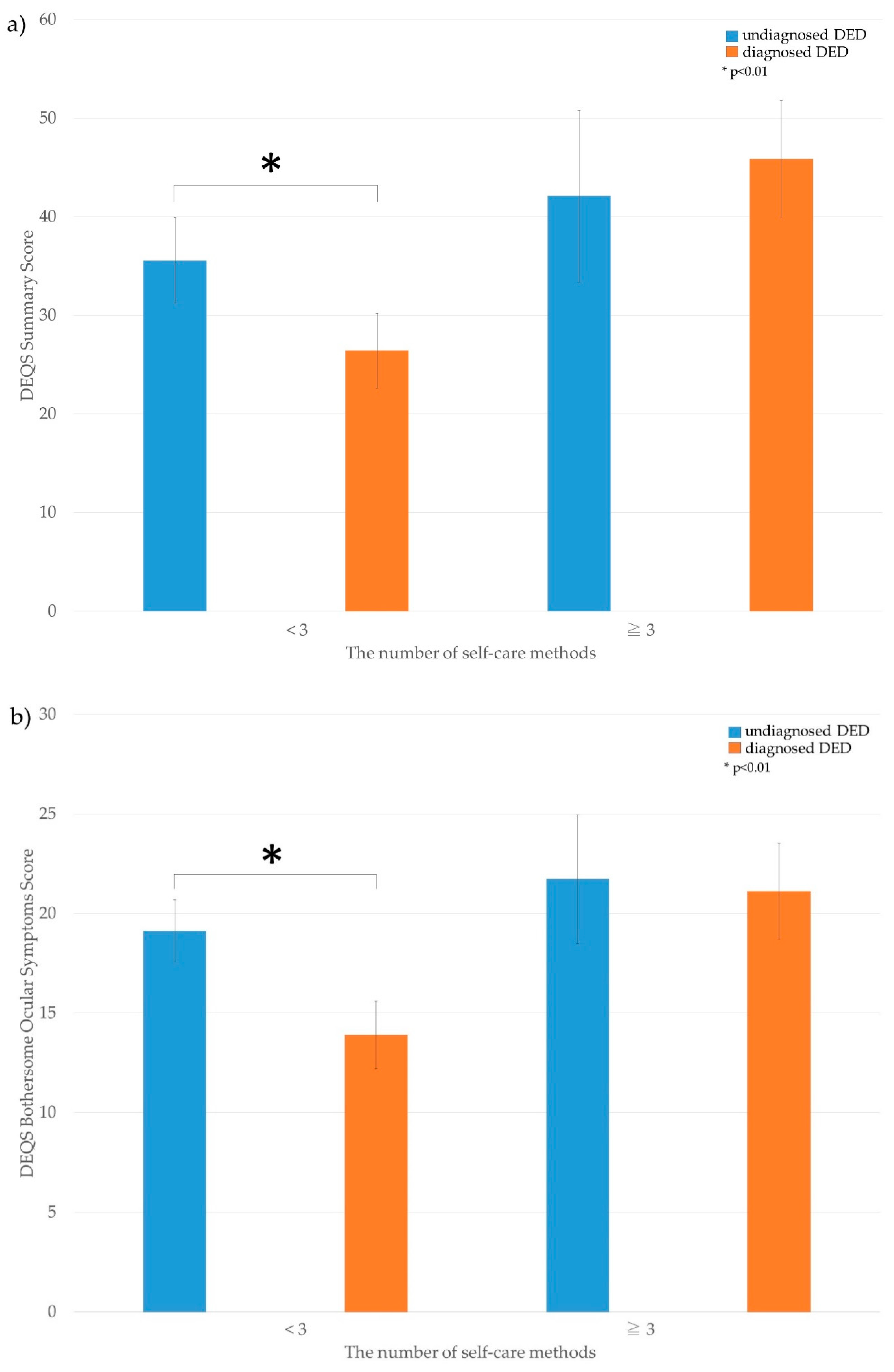
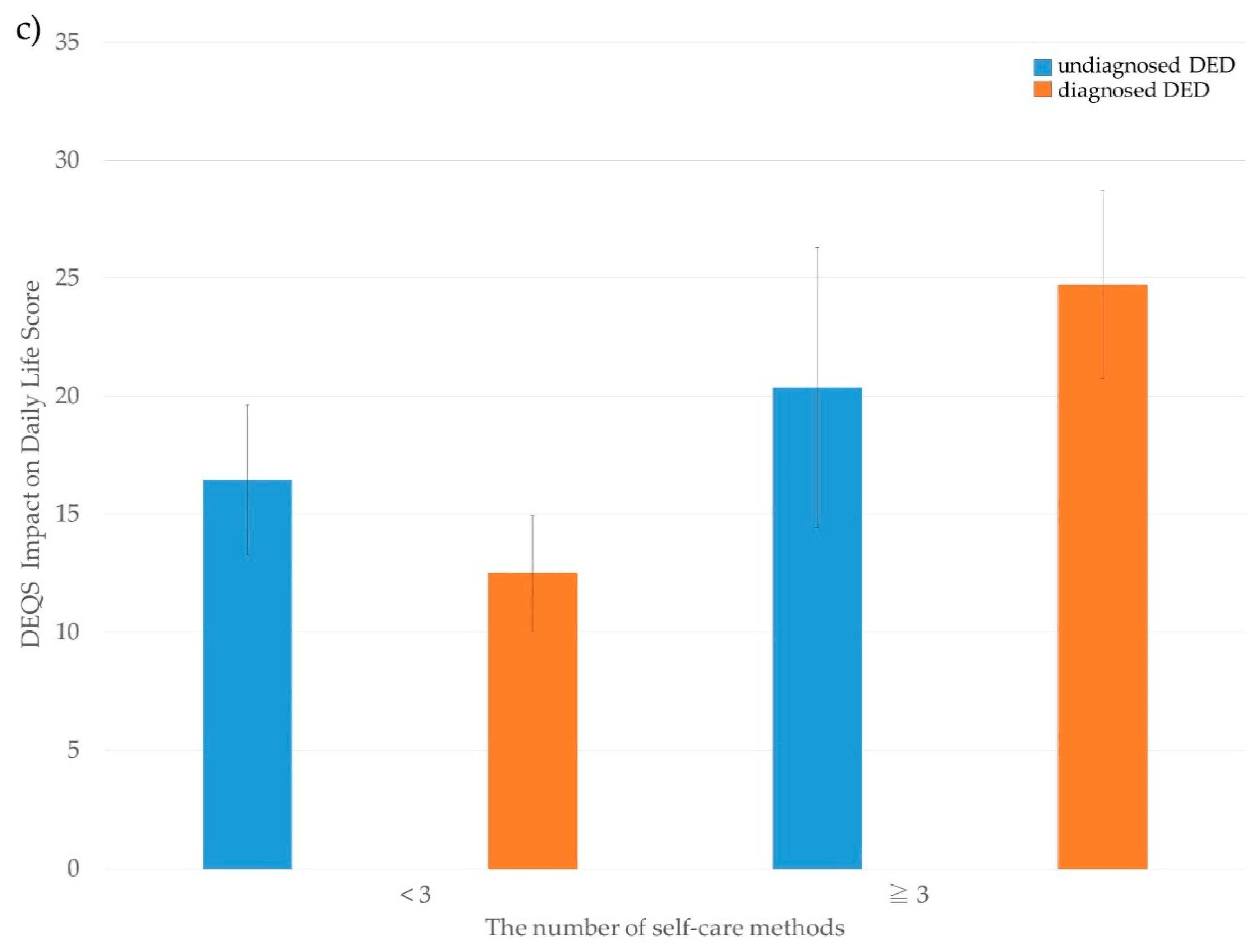
2.5. Self-Care Methods for Dry Eye Disease
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Tsubota, K.; Yokoi, N.; Shimazaki, J.; Watanabe, H.; Dogru, M.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y.; et al. New Perspectives on Dry Eye Definition and Diagnosis: A Consensus Report by the Asia Dry Eye Society. Ocul. Surf. 2017, 15, 65–76. [Google Scholar] [CrossRef]
- Koh, S. Mechanisms of Visual Disturbance in Dry Eye. Cornea 2016, 35, S83–S88. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.; Patel, D.A.; Keith, M.S.; Snedecor, S.J. Economic and Humanistic Burden of Dry Eye Disease in Europe, North America, and Asia: A Systematic Literature Review. Ocul. Surf. 2016, 14, 144–167. [Google Scholar] [CrossRef]
- Matossian, C.; McDonald, M.; Donaldson, K.E.; Nichols, K.K.; MacIver, S.; Gupta, P.K. Dry Eye Disease: Consideration for Women’s Health. J. Womens Health 2019, 28, 502–514. [Google Scholar] [CrossRef] [PubMed]
- Vehof, J.; Sillevis Smitt-Kamminga, N.; Nibourg, S.A.; Hammond, C.J. Sex differences in clinical characteristics of dry eye disease. Ocul. Surf. 2018, 16, 242–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaumberg, D.A.; Uchino, M.; Christen, W.G.; Semba, R.D.; Buring, J.E.; Li, J.Z. Patient reported differences in dry eye disease between men and women: Impact, management, and patient satisfaction. PLoS ONE 2013, 8, e76121. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Mizuno, Y.; Shigeyasu, C. Impact of dry eye on work productivity. Clin. Outcomes Res. Ceor. 2012, 4, 307–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeo, S.; Tong, L. Coping with dry eyes: A qualitative approach. BMC Ophthalmol. 2018, 18, 8. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, N.; Georgiev, G.A. Tear Film-Oriented Diagnosis and Tear Film-Oriented Therapy for Dry Eye Based on Tear Film Dynamics. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES13–DES22. [Google Scholar] [CrossRef] [PubMed]
- Uchino, M.; Nishiwaki, Y.; Michikawa, T.; Shirakawa, K.; Kuwahara, E.; Yamada, M.; Dogru, M.; Schaumberg, D.A.; Kawakita, T.; Takebayashi, T.; et al. Prevalence and risk factors of dry eye disease in Japan: Koumi study. Ophthalmology 2011, 118, 2361–2367. [Google Scholar] [CrossRef]
- Uchino, M.; Kawashima, M.; Uchino, Y.; Suzuki, N.; Mitamura, H.; Mizuno, M.; Hori, Y.; Yokoi, N.; Tsubota, K. The evaluation of dry eye mobile apps for screening of dry eye disease and educational tear event in Japan. Ocul. Surf. 2018, 16, 430–435. [Google Scholar] [CrossRef]
- Schaumberg, D.A.; Sullivan, D.A.; Buring, J.E.; Dana, M.R. Prevalence of dry eye syndrome among US women. Am. J. Ophthalmol. 2003, 136, 318–326. [Google Scholar] [CrossRef]
- Sakane, Y.; Yamaguchi, M.; Yokoi, N.; Uchino, M.; Dogru, M.; Oishi, T.; Ohashi, Y.; Ohashi, Y. Development and validation of the Dry Eye-Related Quality-of-Life Score questionnaire. JAMA Ophthalmol. 2013, 131, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-Del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. TFOS DEWS II Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, N.; Bron, A.J.; Georgiev, G.A. The precorneal tear film as a fluid shell: The effect of blinking and saccades on tear film distribution and dynamics. Ocul. Surf. 2014, 12, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Shen, G.; Qi, Q.; Ma, X. Effect of Moisture Chamber Spectacles on Tear Functions in Dry Eye Disease. Optom. Vis. Sci. 2016, 93, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Geerling, G.; Tauber, J.; Baudouin, C.; Goto, E.; Matsumoto, Y.; O’Brien, T.; Rolando, M.; Tsubota, K.; Nichols, K.K. The international workshop on meibomian gland dysfunction: Report of the subcommittee on management and treatment of meibomian gland dysfunction. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2050–2064. [Google Scholar] [CrossRef]
- Ayaki, M.; Kawashima, M.; Negishi, K.; Tsubota, K. High prevalence of sleep and mood disorders in dry eye patients: Survey of 1000 eye clinic visitors. Neuropsychiatr. Dis. Treat. 2015, 11, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Sano, K.; Kawashima, M.; Takechi, S.; Mimura, M.; Tsubota, K. Exercise program improved subjective dry eye symptoms for office workers. Clin. Ophthalmol. 2018, 12, 307–311. [Google Scholar] [CrossRef]
- Sano, K.; Kawashima, M.; Ikeura, K.; Arita, R.; Tsubota, K. Abdominal breathing increases tear secretion in healthy women. Ocul. Surf. 2015, 13, 82–87. [Google Scholar] [CrossRef]
- Sung, J.; Wang, M.T.M.; Lee, S.H.; Cheung, I.M.Y.; Ismail, S.; Sherwin, T.; Craig, J.P. Randomized double-masked trial of eyelid cleansing treatments for blepharitis. Ocul. Surf. 2018, 16, 77–83. [Google Scholar] [CrossRef]
- Uchino, M.; Uchino, Y.; Dogru, M.; Kawashima, M.; Yokoi, N.; Komuro, A.; Sonomura, Y.; Kato, H.; Kinoshita, S.; Schaumberg, D.A.; et al. Dry eye disease and work productivity loss in visual display users: The Osaka study. Am. J. Ophthalmol. 2014, 157, 294–300. [Google Scholar] [CrossRef]
- Uchino, M.; Schaumberg, D.A.; Dogru, M.; Uchino, Y.; Fukagawa, K.; Shimmura, S.; Satoh, T.; Takebayashi, T.; Tsubota, K. Prevalence of dry eye disease among Japanese visual display terminal users. Ophthalmology 2008, 115, 1982–1988. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II Epidemiology Report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef]
- Japanese Ministry of Health, Labour and Welfare. Average Income per Household and per Household Member by Age Group of Householder. Available online: https://www.mhlw.go.jp/english/database/db-hh/1-3.html (accessed on 17 May 2019).
- Parihar, J.K.; Jain, V.K.; Chaturvedi, P.; Kaushik, J.; Jain, G.; Parihar, A.K. Computer and visual display terminals (VDT) vision syndrome (CVDTS). Med. J. Armed Forces India 2016, 72, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Tachibana, H.; Izumi, T.; Honda, S.; Takemoto, T.I. The prevalence and pattern of insomnia in Japanese industrial workers: Relationship between psychosocial stress and type of insomnia. Psychiatry Clin. Neurosci. 1998, 52, 397–402. [Google Scholar] [CrossRef] [Green Version]
- Uchino, M.; Yokoi, N.; Uchino, Y.; Dogru, M.; Kawashima, M.; Komuro, A.; Sonomura, Y.; Kato, H.; Kinoshita, S.; Schaumberg, D.A.; et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: The Osaka study. Am. J. Ophthalmol. 2013, 156, 759–766. [Google Scholar] [CrossRef]
- Tsubota, K.; Nakamori, K. Dry eyes and video display terminals. N. Engl. J. Med. 1993, 328, 584. [Google Scholar] [CrossRef]
- Uchino, M.; Kawashima, M.; Uchino, Y.; Tsubota, K.; Yokoi, N. Association between tear film break up time and blink interval in visual display terminal users. Int. J. Ophthalmol. 2018, 11, 1691–1697. [Google Scholar] [CrossRef]
- Xue, A.L.; Downie, L.E.; Ormonde, S.E.; Craig, J.P. A comparison of the self-reported dry eye practices of New Zealand optometrists and ophthalmologists. Ophthalmic Physiol. Opt. 2017, 37, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Downie, L.E.; Rumney, N.; Gad, A.; Keller, P.R.; Purslow, C.; Vingrys, A.J. Comparing self-reported optometric dry eye clinical practices in Australia and the United Kingdom: Is there scope for practice improvement? Ophthalmic Physiol. Opt. 2016, 36, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, Y.A.; Camp, A.; Feuer, W.; Karp, C.L.; Wellik, S.; Galor, A. Compliance and Subjective Patient Responses to Eyelid Hygiene. Eye Contact Lens 2017, 43, 213–217. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristic | Men | Women | p Value |
|---|---|---|---|
| n (%) | n (%) | ||
| 729 (70.8) | 301 (29.2) | ||
| Age (year), mean ± SD | 49.6 ± 0.4 | 40.1 ± 0.6 | <0.001 a |
| DEQS | |||
| Summary score, mean ± SD | 17.9 ± 0.7 | 24.6 ± 1.2 | <0.001 a |
| Bothersome ocular symptoms, mean ± SD | 9.0 ± 0.3 | 13.1 ± 0.5 | 0.002 a |
| Impact of daily life, mean ± SD | 8.9 ± 0.4 | 11.4 ± 0.7 | <0.001 a |
| Marital status: married n (%) | 502 (68.9) | 111 (36.9) | <0.001 b |
| Offspring status: does have any children n (%) | 436 (59.8) | 86 (28.6) | <0.001 b |
| Annual household income n (%) | <0.001b | ||
| <$40,000 per year | 94 (12.9) | 87 (28.9) | |
| $40,000–$59,999 per year | 145 (19.9) | 51 (16.9) | |
| ≥$60,000 per year | 430 (59.0) | 116 (38.5) | |
| VDT hours during work (hrs), mean ± SD | 6.6 ± 0.1 | 7.1 ± 0.2 | 0.02 a |
| CL use, n (%) | 121 (16.6) | 145 (48.2) | <0.001 b |
| History of smoking, n (%) | 202 (27.7) | 47 (15.6) | <0.001 b |
| The number of self-care methods mean + SD | 1.6 (0.0) | 1.8 (0.1) | 0.02 a |
| Demographic Characteristic | Non DED | Undiagnosed DED | Diagnosed DED | p Value ** |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| 758 (73.7) | 116 (11.3) | 155 (15.1) | ||
| Age (year), mean ± SD | 47.8 ± 0.4 | 41.8 ± 0.9 | 45.7 ± 0.9 | 0.002 a |
| Women, n (%) | 175 (23.1) | 54 (46.6) | 72 (46.5) | 0.99 b |
| DEQS | ||||
| Summary score, mean ± SD | 14.6 ± 0.5 | 37.3 ± 2.0 | 32.2 ± 1.8 | 0.06 a |
| Bothersome ocular symptoms, mean ± SD | 7.6 ± 0.2 | 19.8 ± 0.7 | 16.0 ± 0.7 | <0.001 a |
| Impact of daily life, mean ± SD | 7.0 ± 0.3 | 17.5 ± 1.4 | 16.2 ± 1.1 | 0.47 a |
| Marital status: married, n (%) | 463 (61.1) | 62 (53.4) | 88 (56.8) | 0.59 b |
| Offspring status: no children, n (%) | 400 (52.8) | 55 (47.4) | 67 (43.2) | 0.49 b |
| Annual household income, n (%) | 0.82 b | |||
| <$40,000/year | 127 (16.8) | 26 (22.4) | 28 (18.1) | |
| $40,000–$59,999/year | 143 (18.9) | 23 (55.0) | 30 (19.4) | |
| ≥$60,000/year | 414 (54.6) | 57 (49.1) | 75 (48.4) | |
| VDT hours during work (hours), mean ± SD | 6.6 ± 0.1 | 7.7 ± 0.2 | 7.2 ± 0.2 | 0.08 a |
| CL use, n (%) | 164 (21.6) | 41 (35.3) | 61 (39.4) | 0.50 b |
| History of smoking, n (%) | 186 (24.5) | 22 (19.0) | 41 (26.5) | 0.14 b |
| Demographic Characteristic | Undiagnosed DED | Diagnosed DED | ||||
|---|---|---|---|---|---|---|
| Univariate Logistic Analysis (Compared to Non-DED) | Multivariate Logistic Analysis (Compared to Non-DED) | p Value | Univariate Logistic Analysis (Compared to Non-DED) | Multivariate Logistic Analysis (Compared to Non-DED) | p Value | |
| Age (every one year) | ||||||
| OR (95% CI) | 0.95 (0.93–0.97) | 0.97 (0.95–0.99) | 0.01 | 0.98 (0.97–1.00) | 1.01 (0.99–1.03) | 0.38 |
| Gender (men vs. women) | ||||||
| OR (95% CI) | 2.91 (1.94–4.34) | 2.12 (1.28–3.50) | 0.003 | 2.89 (2.02–4.14) | 2.45 (1.58–3.80) | <0.001 |
| Offspring status: does have any children | ||||||
| OR (95% CI) | 0.81 (0.55–1.20) | 0.68 (0.48–0.97) | 0.83 (0.55–1.26) | 0.39 | ||
| Annual household income (every $20,000) | ||||||
| OR (95% CI) | 0.90 (0.81–0.99) | 0.96 (0.87–1.05) | 0.38 | 1.00 (0.92–1.08) | ||
| VDT hours during work (every one hour) | ||||||
| OR (95% CI) | 1.15 (1.07–1.23) | 1.12 (1.04–1.21) | 0.004 | 1.08 (1.01–1.15) | 1.06 (0.99–1.14) | 0.07 |
| CL use (never vs. ever) | ||||||
| OR (95% CI) | 2.01 (1.29–3.12) | 1.28 (0.78–2.11) | 0.33 | 2.35 (1.63–3.39) | 1.66 (1.08–2.54) | 0.02 |
| Self-Care Methods | Undiagnosed DED | Diagnosed DED | p Value |
|---|---|---|---|
| The number of methods, mean + SD | 1.9 ± 0.1 | 2.0 ± 0.1 | 0.37 a |
| The number of methods, n (%) | 0.50 b | ||
| 0 | 14 (12.1) | 15 (9.8) | |
| 1 | 35 (30.2) | 52 (34.0) | |
| 2 | 36 (31.0) | 37 (24.2) | |
| ≥3 | 31 (26.7) | 49 (32.0) | |
| Use of over-the-counter eye drops, n (%) | 80 (69.0) | 107 (69.9) | 0.86 b |
| Increase in blinking | 35 (30.2) | 38 (24.8) | 0.33 b |
| Use protection glasses from dryness | 6 (5.2) | 12 (7.8) | 0.39 b |
| Use of a warm compress | 24 (20.7) | 36 (23.5) | 0.58 b |
| Sleeping longer | 42 (36.2) | 71 (46.4) | 0.09 b |
| Exercise | 4 (3.4) | 12 (7.8) | 0.13 b |
| Use of oral supplements | 13 (11.2) | 13 (8.5) | 0.46 b |
| Deep, relaxing breathing | 7 (6.0) | 13 (8.5) | 0.45 b |
| Eyelid hygiene using eye shampoo | 2 (1.7) | 0 (0.0) | 0.10 b |
| Others | 3 (2.6) | 6 (3.9) | 0.55 b |
| Not doing anything | 14 (12.1) | 15 (9.8) | 0.55 b |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamanishi, R.; Uchino, M.; Kawashima, M.; Uchino, Y.; Yokoi, N.; Tsubota, K. Characteristics of Individuals with Dry Eye Symptoms without Clinical Diagnosis: Analysis of a Web-Based Survey. J. Clin. Med. 2019, 8, 721. https://doi.org/10.3390/jcm8050721
Yamanishi R, Uchino M, Kawashima M, Uchino Y, Yokoi N, Tsubota K. Characteristics of Individuals with Dry Eye Symptoms without Clinical Diagnosis: Analysis of a Web-Based Survey. Journal of Clinical Medicine. 2019; 8(5):721. https://doi.org/10.3390/jcm8050721
Chicago/Turabian StyleYamanishi, Ryutaro, Miki Uchino, Motoko Kawashima, Yuichi Uchino, Norihiko Yokoi, and Kazuo Tsubota. 2019. "Characteristics of Individuals with Dry Eye Symptoms without Clinical Diagnosis: Analysis of a Web-Based Survey" Journal of Clinical Medicine 8, no. 5: 721. https://doi.org/10.3390/jcm8050721
APA StyleYamanishi, R., Uchino, M., Kawashima, M., Uchino, Y., Yokoi, N., & Tsubota, K. (2019). Characteristics of Individuals with Dry Eye Symptoms without Clinical Diagnosis: Analysis of a Web-Based Survey. Journal of Clinical Medicine, 8(5), 721. https://doi.org/10.3390/jcm8050721