Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation



Abstract
:1. Introduction
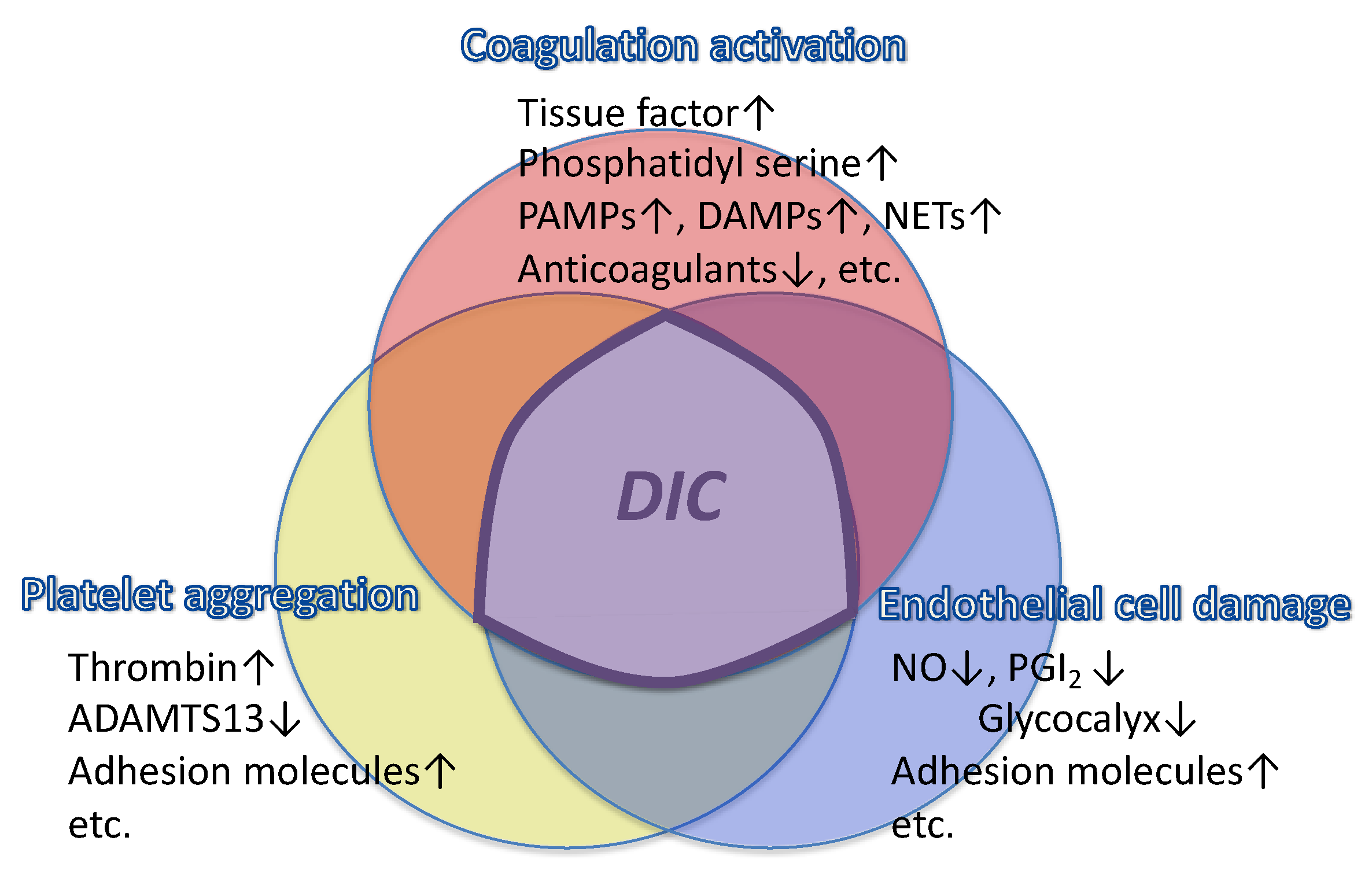
2. Pathophysiology of Sepsis-Induced Coagulopathy and DIC
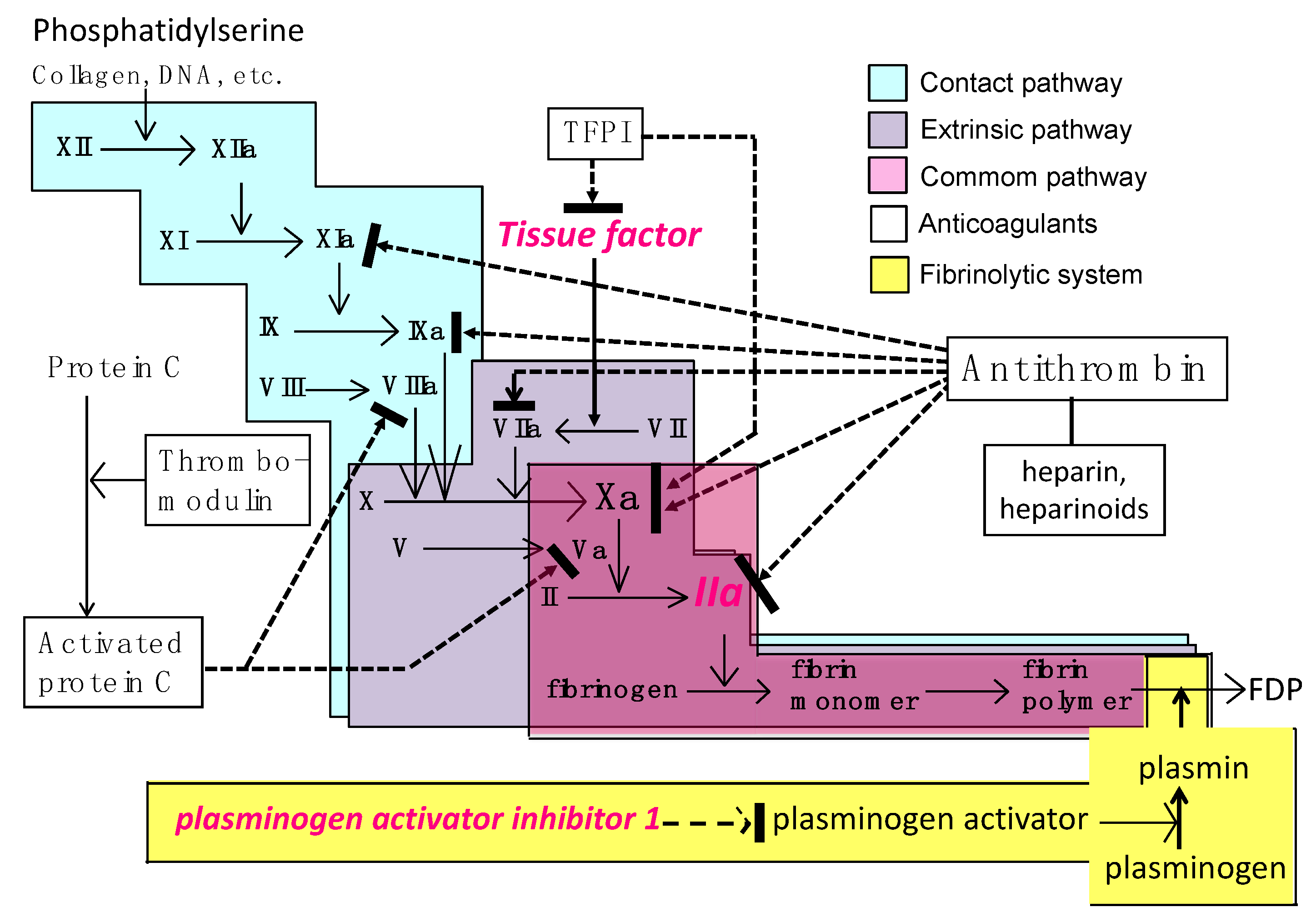
2.1. Activation of the Coagulation Cascade
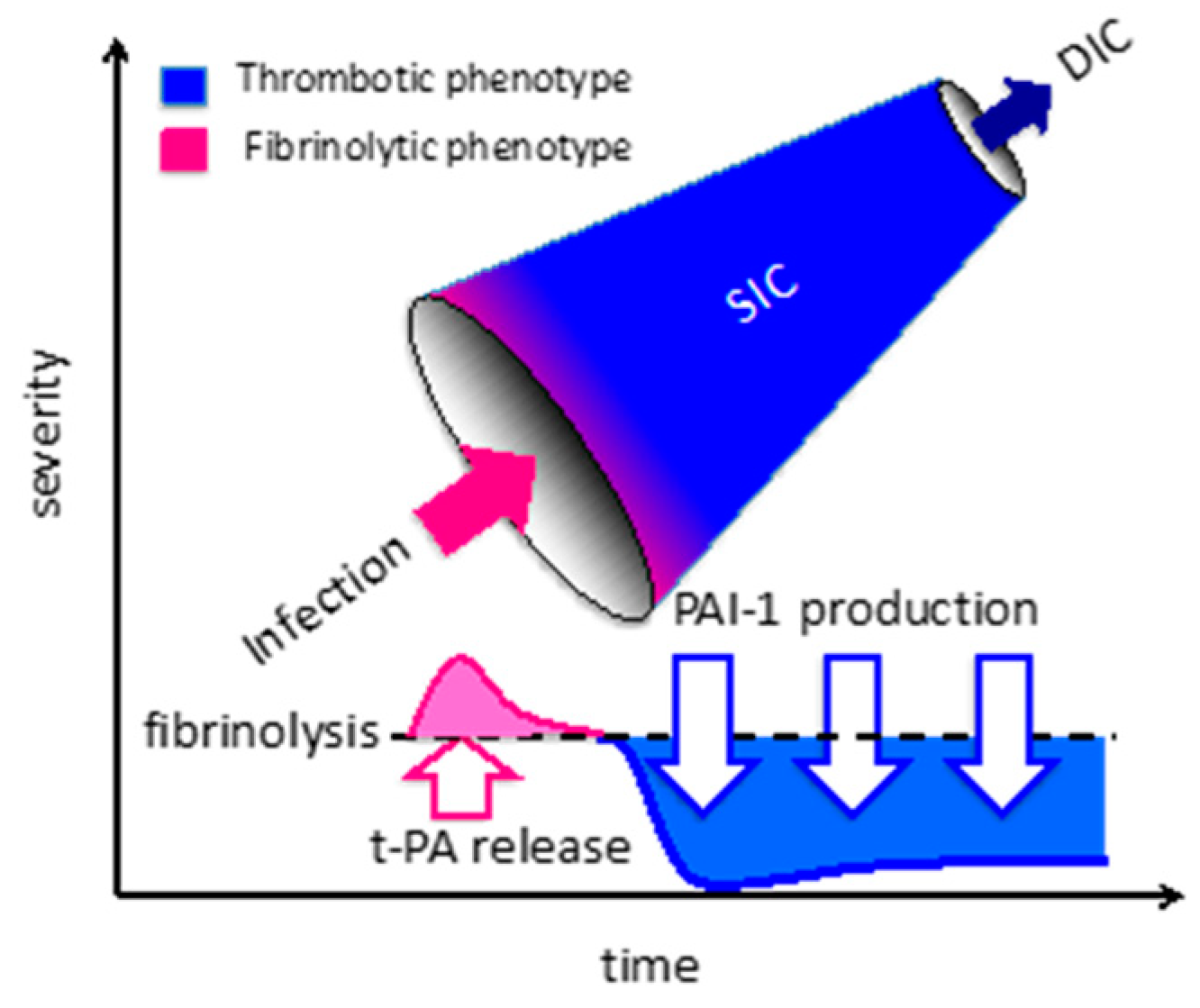
2.2. Fibrinolytic Shutdown
2.3. Endothelial Dysfunction
2.4. Platelet Aggregation
2.5. Impairment of Anticoagulant Systems
3. Diagnosis of Sepsis-Induced Coagulopathy and DIC
3.1. Diagnostic Criteria for Sepsis-Associated DIC
3.2. Diagnostic Criteria for Sepsis-Induced Coagulopathy (SIC)
3.3. Viscoelastic Testing for Sepsis-Associated DIC
3.4. Waveform Analysis of Clot Formation
4. Differential Diagnoses of Sepsis-Induced Coagulopathy and DIC
5. Treatment of Sepsis-Induced Coagulopathy and DIC
5.1. Unfractionnated Heparin and Low-Molecular-Weight Heparin
5.2. Antithrombin
5.3. Recombinant Activated Protein C
5.4. Recombinant Thrombomodulin
5.5. Recombinant Tissue Factor Pathway Inhibitor
6. Summary
Conflicts of Interest
References
- Jackson, S.P.; Darbousset, R.; Schoenwaelder, S.M. Thromboinflammation: Challenges of therapeutically targeting coagulation and other host defense mechanisms. Blood 2019, 133, 906–918. [Google Scholar] [CrossRef]
- van der Poll, T.; Herwald, H. The coagulation system and its function in early immune defense. Thromb. Haemost. 2014, 112, 640–648. [Google Scholar] [CrossRef] [Green Version]
- Levi, M.; van der Poll, T. A short contemporary history of disseminated intravascular coagulation. Semin. Thromb. Hemost. 2014, 40, 874–880. [Google Scholar]
- Taylor, F.B.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef]
- Prentice, C.R. Acquired coagulation disorders. Clin. Haematol. 1985, 14, 413–442. [Google Scholar]
- Warkentin, T.E. Microvascular thrombosis and ischaemic limb losses in critically ill patients. Hamostaseologie 2019, 39, 6–19. [Google Scholar] [CrossRef]
- Ito, T. PAMPs and DAMPs as triggers for DIC. J. Intensive Care 2014, 2, 67. [Google Scholar] [CrossRef]
- Lupu, F.; Keshari, R.S.; Lambris, J.D.; Coggeshall, K.M. Crosstalk between the coagulation and complement systems in sepsis. Thromb. Res. 2014, 133, S28–S31. [Google Scholar] [CrossRef] [Green Version]
- Iba, T.; Miki, T.; Hashiguchi, N.; Tabe, Y.; Nagaoka, I. Is the neutrophil a ‘prima donna’ in the procoagulant process during sepsis? Crit. Care 2014, 18, 230. [Google Scholar] [CrossRef]
- Liaw, P.C.; Ito, T.; Iba, T.; Thachil, J.; Zeerleder, S. DAMP and DIC: The role of extracellular DNA and DNA-binding proteins in the pathogenesis of DIC. Blood Rev. 2016, 30, 257–261. [Google Scholar] [CrossRef]
- Wang, Y.; Luo, L.; Braun, O.Ö.; Westman, J.; Madhi, R.; Herwald, H.; Mörgelin, M.; Thorlacius, H. Neutrophil extracellular trap-microparticle complexes enhance thrombin generation via the intrinsic pathway of coagulation in mice. Sci. Rep. 2018, 8, 4020. [Google Scholar] [CrossRef]
- Østerud, B.; Bjørklid, E. The tissue factor pathway in disseminated intravascular coagulation. Semin. Thromb. Hemost. 2001, 27, 605–617. [Google Scholar]
- Iba, T.; Ogura, H. Role of extracellular vesicles in the development of sepsis-induced coagulopathy. J. Intensive Care 2018, 6, 68. [Google Scholar] [CrossRef]
- Delabranche, X.; Helms, J.; Meziani, F. Immunohaemostasis: A new view on haemostasis during sepsis. Ann. Intensive Care 2017, 7, 117. [Google Scholar] [CrossRef]
- Madoiwa, S. Recent advances in disseminated intravascular coagulation: Endothelial cells and fibrinolysis in sepsis-induced DIC. J. Intensive Care 2015, 3, 8. [Google Scholar] [CrossRef]
- Semeraro, N.; Ammollo, C.T.; Semeraro, F.; Colucci, M. Sepsis, thrombosis and organ dysfunction. Thromb. Res. 2012, 129, 290–295. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Borreguero-León, J.M.; Solé-Violán, J.; Ferreres, J.; Labarta, L.; Díaz, C.; Jiménez, A.; Páramo, J.A. Sustained high plasma plasminogen activator inhibitor-1 levels are associated with severity and mortality in septic patients. Thromb. Res. 2014, 134, 182–186. [Google Scholar] [CrossRef]
- Zeerleder, S.; Schroeder, V.; Hack, C.E.; Kohler, H.P.; Wuillemin, W.A. TAFI and PAI-1 levels in human sepsis. Thromb. Res. 2006, 118, 205–212. [Google Scholar] [CrossRef]
- Mavrommatis, A.C.; Theodoridis, T.; Economou, M.; Kotanidou, A.; El Ali, M.; Christopoulou-Kokkinou, V.; Zakynthinos, S.G. Activation of the fibrinolytic system and utilization of the coagulation inhibitors in sepsis: Comparison with severe sepsis and septic shock. Intensive Care Med. 2001, 27, 1853–1859. [Google Scholar] [CrossRef]
- Hack, C.E. Fibrinolysis in disseminated intravascular coagulation. Semin. Thromb. Hemost. 2001, 27, 633–638. [Google Scholar] [CrossRef]
- Iba, T.; Thachil, J. Clinical significance of measuring plasminogen activator inhibitor-1 in sepsis. J. Intensive Care 2017, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Iba, T.; Levy, J.H. Inflammation and thrombosis: Roles of neutrophils, platelets and endothelial cells and their interactions in thrombus formation during sepsis. J. Thromb. Haemost. 2018, 16, 231–241. [Google Scholar] [CrossRef]
- Erez, O.; Mastrolia, S.A.; Thachil, J. Disseminated intravascular coagulation in pregnancy: Insights in pathophysiology, diagnosis and management. Am. J. Obstet. Gynecol. 2015, 213, 452–463. [Google Scholar] [CrossRef]
- López-Aguirre, Y.; Páramo, J.A. Endothelial cell and hemostatic activation in relation to cytokines in patients with sepsis. Thromb. Res. 1999, 94, 95–101. [Google Scholar] [CrossRef]
- Muth, H.; Maus, U.; Wygrecka, M.; Lohmeyer, J.; Grimminger, F.; Seeger, W.; Günther, A. Pro- and antifibrinolytic properties of human pulmonary microvascular versus artery endothelial cells: Impact of endotoxin and tumor necrosis factor-alpha. Crit. Care Med. 2004, 32, 217–226. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H. Derangement of the endothelial glycocalyx in sepsis. J. Thromb. Haemost. 2019, 17, 283–294. [Google Scholar] [CrossRef]
- Chappell, D.; Hofmann-Kiefer, K.; Jacob, M.; Rehm, M.; Briegel, J.; Welsch, U.; Conzen, P.; Becker, B.F. TNF-α induced shedding of the endothelial glycocalyx is prevented by hydrocortisone and antithrombin. Basic Res. Cardiol. 2008, 104, 78–89. [Google Scholar] [CrossRef]
- Bermejo-Martin, J.F.; Martín-Fernandez, M.; López-Mestanza, C.; Duque, P.; Almansa, R. Shared Features of Endothelial Dysfunction between Sepsis and Its Preceding Risk Factors (Aging and Chronic Disease). J. Clin. Med. 2018, 7. [Google Scholar] [CrossRef]
- Nelson, A.; Berkestedt, I.; Schmidtchen, A.; Ljunggren, L.; Bodelsson, M. Increased levels of glycosaminoglycans during septic shock: Relation to mortality and the antibacterial actions of plasma. Shock 2008, 30, 623–627. [Google Scholar] [CrossRef]
- Kitchens, C.S. Thrombocytopenia and thrombosis in disseminated intravascular coagulation (DIC). Hematol. Am. Soc. Hematol. Educ. Program 2009, 2009, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Lopez, E.; Bermejo, N.; Berna-Erro, A.; Alonso, N.; Salido, G.M.; Redondo, P.C.; Rosado, J.A. Relationship between calcium mobilization and platelet α- and δ-granule secretion. A role for TRPC6 in thrombin-evoked δ-granule exocytosis. Arch. Biochem. Biophys. 2015, 585, 75–81. [Google Scholar] [CrossRef]
- Coppinger, J.A.; Cagney, G.; Toomey, S.; Kislinger, T.; Belton, O.; McRedmond, J.P.; Cahill, D.J.; Emili, A.; Fitzgerald, D.J.; Maguire, P.B. Characterization of the proteins released from activated platelets leads to localization of novel platelet proteins in human atherosclerotic lesions. Blood 2004, 103, 2096–2104. [Google Scholar] [CrossRef] [Green Version]
- Opal, S.; Laterre, P.F.; Abraham, E.; Francois, B.; Wittebole, X.; Lowry, S.; Dhainaut, J.F.; Warren, B.; Dugernier, T.; Lopez, A.; et al. Recombinant human platelet-activating factor acetylhydrolase for treatment of severe sepsis: Results of a phase III, multicenter, randomized, double-blind, placebo-controlled, clinical trial. Crit. Care Med. 2004, 32, 332–341. [Google Scholar] [CrossRef]
- Vincent, J.L.; Spapen, H.; Bakker, J.; Webster, N.R.; Curtis, L. Phase II multicenter clinical study of the platelet-activating factor receptor antagonist BB-882 in the treatment of sepsis. Crit. Care Med. 2000, 28, 638–642. [Google Scholar] [CrossRef]
- Ouyang, Y.; Wang, Y.; Liu, B.; Ma, X.; Ding, R. Effects of antiplatelet therapy on the mortality rate of patients with sepsis: A meta-analysis. J. Crit. Care 2019, 50, 162–168. [Google Scholar] [CrossRef]
- Cuccurullo, A.; Greco, E.; Lupia, E.; De Giuli, P.; Bosco, O.; Martin-Conte, E.; Spatola, T.; Turco, E.; Montrucchio, G. Blockade of Thrombopoietin Reduces Organ Damage in Experimental Endotoxemia and Polymicrobial Sepsis. PLoS ONE 2016, 11, e0151088. [Google Scholar] [CrossRef]
- Iba, T.; Gando, S.; Thachil, J. Anticoagulant therapy for sepsis-associated disseminated intravascular coagulation: The view from Japan. J. Thromb. Haemost. 2014, 12, 1010–1019. [Google Scholar] [CrossRef]
- Levy, J.H.; Sniecinski, R.M.; Welsby, I.J.; Levi, M. Antithrombin: Anti-inflammatory properties and clinical applications. Thromb. Haemost. 2016, 115, 712–728. [Google Scholar]
- Roemisch, J.; Gray, E.; Hoffmann, J.N.; Wiedermann, C.J. Antithrombin: A new look at the actions of a serine protease inhibitor. Blood Coagul. Fibrinolysis 2002, 13, 657–670. [Google Scholar] [CrossRef]
- Fourrier, F.; Chopin, C.; Goudemand, J.; Hendrycx, S.; Caron, C.; Rime, A.; Marey, A.; Lestavel, P. Septic shock, multiple organ failure, and disseminated intravascular coagulation. Compared patterns of antithrombin III, protein C, and protein S deficiencies. Chest 1992, 101, 816–823. [Google Scholar] [CrossRef]
- Lauterbach, R.; Pawlik, D.; Radziszewska, R.; Wozniak, J.; Rytlewski, K. Plasma antithrombin III and protein C levels in early recognition of late-onset sepsis in newborns. Eur. J. Pediatr. 2006, 165, 585–589. [Google Scholar] [CrossRef]
- Aibiki, M.; Fukuoka, N.; Umakoshi, K.; Ohtsubo, S.; Kikuchi, S. Serum albumin levels anticipate antithrombin III activities before and after antithrombin III agent in critical patients with disseminated intravascular coagulation. Shock 2007, 27, 139–144. [Google Scholar] [CrossRef]
- Chappell, D.; Brettner, F.; Doerfler, N.; Jacob, M.; Rehm, M.; Bruegger, D.; Conzen, P.; Jacob, B.; Becker, B.F. Protection of glycocalyx decreases platelet adhesion after ischaemia/reperfusion: An animal study. Eur. J. Anaesthesiol. 2014, 31, 474–481. [Google Scholar] [CrossRef]
- Mehta, D.; Ravindran, K.; Kuebler, W.M. Novel regulators of endothelial barrier function. Am. J. Physiol. Lung Cell. Mol. Physiol. 2014, 307, L924–L935. [Google Scholar] [CrossRef]
- Chappell, D.; Jacob, M.; Hofmann-Kiefer, K.; Rehm, M.; Welsch, U.; Conzen, P. Antithrombin reduces shedding of the endothelial glycocalyx following ischaemia/reperfusion. Antithrombin reduces shedding of the endothelial glycocalyx following ischaemia/reperfusion. Cardiovasc. Res. 2009, 83, 388–396. [Google Scholar] [CrossRef]
- Griffin, J.H.; Zlokovic, B.V.; Mosnier, L.O. Activated protein C: Biased for translation. Blood 2015, 125, 2898–2907. [Google Scholar] [CrossRef]
- Choi, Q.; Hong, K.H.; Kim, J.E.; Kim, H.K. Changes in plasma levels of natural anticoagulants in disseminated intravascular coagulation: High prognostic value of antithrombin and protein C in patients with underlying sepsis or severe infection. Ann. Lab. Med. 2014, 34, 85–91. [Google Scholar] [CrossRef]
- Griffin, J.H.; Zlokovic, B.V.; Mosnier, L.O. Protein C anticoagulant and cytoprotective pathways. Int. J. Hematol. 2012, 95, 333–345. [Google Scholar] [CrossRef] [Green Version]
- Kawamoto, E.; Nago, N.; Okamoto, T.; Gaowa, A.; Masui-Ito, A.; Sakakura, Y.; Akama, Y.; Soe, Z.Y.; Prajuabjinda, O.; Darkwah, S.; et al. Anti-adhesive effects of human soluble thrombomodulin and its domains. Biochem. Biophys. Res. Commun. 2019, 511, 312–317. [Google Scholar] [CrossRef]
- Reinhart, K.; Bayer, O.; Brunkhorst, F.; Meisner, M. Markers of endothelial damage in organ dysfunction and sepsis. Crit. Care Med. 2002, 30, S302–S312. [Google Scholar] [CrossRef]
- Wada, H.; Thachil, J.; Di Nisio, M.; Kurosawa, S.; Gando, S.; Toh, C.H. Harmonized guidance for disseminated intravascular coagulation from the International Society on Thrombosis and Haemostasis and the current status of anticoagulant therapy in Japan: A rebuttal. J. Thromb. Haemost. 2013, 11, 2078–2079. [Google Scholar] [CrossRef]
- Cauchie, P.; Cauchie, C.H.; Boudjeltia, K.Z.; Carlier, E.; Deschepper, N.; Govaerts, D.; Migaud-Fressart, M.; Woodhams, B.; Brohée, D. Diagnosis and prognosis of overt disseminated intravascular coagulation in a general hospital—Meaning of the ISTH score system, fibrin monomers, and lipoprotein-C-reactive protein complex formation. Am. J. Hematol. 2006, 81, 414–419. [Google Scholar] [CrossRef]
- Umemura, Y.; Yamakawa, K.; Hayakawa, M.; Hamasaki, T.; Fujimi, S. Screening itself for disseminated intravascular coagulation may reduce mortality in sepsis: A nationwide multicenter registry in Japan. Thromb. Res. 2018, 161, 60–66. [Google Scholar] [CrossRef]
- Gando, S.; Saitoh, D.; Ogura, H.; Mayumi, T.; Koseki, K.; Ikeda, T.; Ishikura, H.; Iba, T.; Ueyama, M.; Eguchi, Y.; et al. Natural history of disseminated intravascular coagulation diagnosed based on the newly established diagnostic criteria for critically ill patients: Results of a multicenter, prospective survey. Crit. Care. Med. 2008, 36, 145–150. [Google Scholar] [CrossRef]
- Yamakawa, K.; Umemura, Y.; Murao, S.; Hayakawa, M.; Fujimi, S. Optimal Timing and Early Intervention with Anticoagulant Therapy for Sepsis-Induced Disseminated Intravascular Coagulation. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619835055. [Google Scholar] [CrossRef]
- Hunt, B.J. Bleeding and coagulopathies in critical care. N. Engl. J. Med. 2014, 370, 2147–2159. [Google Scholar] [CrossRef]
- Gando, S.; Saitoh, D.; Ogura, H.; Mayumi, T.; Koseki, K.; Ikeda, T.; Ishikura, H.; Iba, T.; Ueyama, M.; Eguchi, Y.; et al. Disseminated intravascular coagulation (DIC) diagnosed based on the Japanese Association for Acute Medicine criteria is a dependent continuum to overt DIC in patients with sepsis. Thromb. Res. 2009, 123, 715–718. [Google Scholar] [CrossRef]
- Iba, T.; Nisio, M.D.; Levy, J.H.; Kitamura, N.; Thachil, J. New criteria for sepsis-induced coagulopathy (SIC) following the revised sepsis definition: A retrospective analysis of a nationwide survey. BMJ Open 2017, 7, e017046. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Iba, T.; Arakawa, M.; Di Nisio, M.; Gando, S.; Anan, H.; Sato, K.; Ueki, Y.; Levy, J.H.; Thachil, J. Newly Proposed Sepsis-Induced Coagulopathy Precedes International Society on Thrombosis and Haemostasis Overt-Disseminated Intravascular Coagulation and Predicts High Mortality. J. Intensive Care Med. 2018. [Google Scholar] [CrossRef]
- Shen, L.; Tabaie, S.; Ivascu, N. Viscoelastic testing inside and beyond the operating room. J. Thorac. Dis. 2017, 9, S299–S308. [Google Scholar] [CrossRef] [Green Version]
- Drumheller, B.C.; Stein, D.M.; Moore, L.J.; Rizoli, S.B.; Cohen, M.J. Thromboelastography and Rotational Thromboelastometry for the Surgical Intensivist: A Narrative Review. J. Trauma Acute Care Surg. 2019. [Google Scholar] [CrossRef]
- Koami, H.; Sakamoto, Y.; Ohta, M.; Goto, A.; Narumi, S.; Imahase, H.; Yahata, M.; Miike, T.; Iwamura, T.; Yamada, K.C.; et al. Can rotational thromboelastometry predict septic disseminated intravascular coagulation? Blood Coagul. Fibrinolysis 2015, 26, 778–783. [Google Scholar] [CrossRef]
- Prakash, S.; Verghese, S.; Roxby, D.; Dixon, D.; Bihari, S.; Bersten, A. Changes in fibrinolysis and severity of organ failure in sepsis: A prospective observational study using point-of-care test—ROTEM. J. Crit. Care 2015, 30, 264–270. [Google Scholar] [CrossRef]
- Favaloro, E.J. Laboratory testing in disseminated intravascular coagulation. Semin. Thromb. Hemost. 2010, 36, 458–467. [Google Scholar] [CrossRef]
- Toh, C.H.; Giles, A.R. Waveform analysis of clotting test optical profiles in the diagnosis and management of disseminated intravascular coagulation (DIC). Clin. Lab. Haematol. 2002, 24, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Samis, J.A.; Stewart, K.A.; Toh, C.H.; Day, A.; Downey, C.; Nesheim, M.E. Temporal changes in factors associated with neutrophil elastase and coagulation in intensive care patients with a biphasic waveform and disseminated intravascular coagulation. J. Thromb. Haemost. 2004, 2, 1535–1544. [Google Scholar] [CrossRef]
- Saha, M.; McDaniel, J.K.; Zheng, X.L. Thrombotic thrombocytopenic purpura: Pathogenesis, diagnosis and potential novel therapeutics. J. Thromb. Haemost. 2017, 15, 1889–1900. [Google Scholar] [CrossRef]
- Jokiranta, T.S. HUS and atypical HUS. Blood 2017, 129, 2847–2856. [Google Scholar] [CrossRef] [Green Version]
- Noris, M.; Mescia, F.; Remuzzi, G. STEC-HUS, atypical HUS and TTP are all diseases of complement activation. Nat. Rev. Nephrol. 2012, 8, 622–633. [Google Scholar] [CrossRef]
- Abildgaard, U.; Heimdal, K. Pathogenesis of the syndrome of hemolysis, elevated liver enzymes, and low platelet count (HELLP): A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 166, 117–123. [Google Scholar] [CrossRef]
- Warkentin, T.E. Heparin-induced thrombocytopenia in critically ill patients. Semin. Thromb. Hemost. 2015, 41, 49–60. [Google Scholar] [CrossRef]
- Warkentin, T.E. Clinical picture of heparin-induced thrombocytopenia (HIT) and its differentiation from non-HIT thrombocytopenia. Thromb. Haemost. 2016, 116, 813–822. [Google Scholar] [CrossRef]
- Warkentin, T.E.; Makris, M.; Jay, R.M.; Kelton, J.G. A spontaneous prothrombotic disorder resembling heparin-induced thrombocytopenia. Am. J. Med. 2008, 121, 632–636. [Google Scholar] [CrossRef]
- Poudel, D.R.; Ghimire, S.; Dhital, R.; Forman, D.; Warkentin, T.E. Spontaneous HIT syndrome post-knee replacement surgery with delayed recovery of thrombocytopenia: A case report and literature review. Platelets 2017, 28, 614–620. [Google Scholar] [CrossRef]
- Martel, N.; Lee, J.; Wells, P.S. Risk for heparin-induced thrombocytopenia with unfractionated and low-molecular-weight heparin thromboprophylaxis: A meta-analysis. Blood 2005, 106, 2710–2715. [Google Scholar] [CrossRef]
- Warkentin, T.E.; Greinacher, A.; Gruel, Y.; Aster, R.H.; Chong, B.H. Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Laboratory testing for heparin-induced thrombocytopenia: A conceptual framework and implications for diagnosis. J. Thromb. Haemost. 2011, 9, 2498–2500. [Google Scholar] [CrossRef]
- Greinacher, A.; Selleng, K.; Warkentin, T.E. Autoimmune heparin-induced thrombocytopenia. J. Thromb. Haemost. 2017, 15, 2099–2114. [Google Scholar] [CrossRef] [Green Version]
- Warkentin, T.E. Ischemic limb gangrene with pulses. N. Engl. J. Med. 2015, 373, 642–655. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Wada, H.; Thachil, J.; Warkentin, T.E.; Levi, M. Differential diagnoses for sepsis-induced disseminated intravascular coagulation: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2019, 17, 415–419. [Google Scholar] [CrossRef]
- Levi, M.; de Jonge, E.; van der Poll, T.; ten Cate, H. Advances in the understanding of the pathogenetic pathways of disseminated intravascular coagulation result in more insight in the clinical picture and better management strategies. Semin. Thromb. Hemost. 2001, 27, 569–575. [Google Scholar] [CrossRef]
- Umemura, Y.; Yamakawa, K.; Ogura, H.; Yuhara, H.; Fujimi, S. Efficacy and safety of anticoagulant therapy in three specific populations with sepsis: A meta-analysis of randomized controlled trials. J. Thromb. Haemost. 2016, 14, 518–530. [Google Scholar] [CrossRef]
- Fan, Y.; Jiang, M.; Gong, D.; Zou, C. Efficacy and safety of low-molecular-weight heparin inpatients with sepsis: A meta-analysis of randomized controlled trials. Sci. Rep. 2016, 6, 25984. [Google Scholar] [CrossRef]
- Yasunaga, K.; Ogawa, N.; Mori, K.; Aoki, N.; Matsuda, T.; Nakagawa, M. Evaluation of clinical effect of danaparoid sodium (KB-101) on disseminated intravascular coagulation (DIC): Double blind comparative study. Jpn. Pharmacol. Ther. 1995, 23, 2815–2834. [Google Scholar]
- Nishida, O.; Ogura, H.; Egi, M.; Hayashi, Y.; Iba, T.; Imaizumi, H.; Inoue, S.; Kakihana, Y.; Kotani, J.; Kushimoto, S.; et al. The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2016 (J-SSCG 2016). Acute Med. Surg. 2018, 5, 3–89. [Google Scholar] [CrossRef]
- Arishima, T.; Ito, T.; Yasuda, T.; Yashima, N.; Furubeppu, H.; Kamikokuryo, C.; Futatsuki, T.; Madokoro, Y.; Miyamoto, S.; Eguchi, T.; et al. Circulating activated protein C levels are not increased in septic patients treated with recombinant human soluble thrombomodulin. Thromb. J. 2018, 16, 24. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Warren, B.L.; Eid, A.; Singer, P.; Pillay, S.S.; Carl, P.; Novak, I.; Chalupa, P.; Atherstone, A.; Pénzes, I.; Kübler, A.; et al. Caring for the critically ill patient. Hig-dose antithrombin III in severe sepsis, a randomized controlled trial. JAMA 2001, 286, 1869–1978. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Antithrombin concentrate use in disseminated intravascular coagulation of sepsis: Meta-analyses revisited. J. Thromb. Haemost. 2018, 16, 455–457. [Google Scholar] [CrossRef]
- Yatabe, T.; Inoue, S.; Sakamoto, S.; Sumi, Y.; Nishida, O.; Hayashida, K.; Hara, Y.; Fukuda, T.; Matsushima, A.; Matsuda, A.; et al. The anticoagulant treatment for sepsis induced disseminated intravascular coagulation; network meta-analysis. Thromb. Res. 2018, 171, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, J.N.; Wiedermann, C.J.; Juers, M.; Ostermann, H.; Kienast, J.; Briegel, J.; Strauss, R.; Warren, B.L.; Opal, S.M. Benefit/risk profile of high-dose antithrombin in patients with severe sepsis treated with and without concomitant heparin. Thromb. Haemost. 2006, 95, 850–856. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Hirota, T.; Hiki, M.; Sato, K.; Murakami, T.; Nagaoka, I. Protection of the endothelial glycocalyx by antithrombin in an endotoxin-induced rat model of sepsis. Thromb. Res. 2018, 171, 1–6. [Google Scholar] [CrossRef]
- Bernard, G.R.; Vincent, J.L.; Laterre, P.F.; LaRosa, S.P.; Dhainaut, J.F.; Lopez-Rodriguez, A.; Steingrub, J.S.; Garber, G.E.; Helterbrand, J.D.; Ely, E.W.; et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N. Engl. J. Med. 2001, 344, 699–709. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Thompson, B.T.; Barie, P.S.; Dhainaut, J.F.; Douglas, I.S.; Finfer, S.; Gårdlund, B.; Marshall, J.C.; Rhodes, A.; Artigas, A.; et al. Drotrecogin alfa (activated) in adults with septic shock. N. Engl. J. Med. 2012, 366, 2055–2064. [Google Scholar] [CrossRef]
- de Pont, A.C.; Bakhtiari, K.; Hutten, B.A.; de Jonge, E.; Vroom, M.B.; Meijers, J.C.; Büller, H.R.; Levi, M. Recombinant human activated protein C resets thrombin generation in patients with severe sepsis—A case control study. Crit. Care 2005, 9, R490–R497. [Google Scholar] [CrossRef]
- Thachil, J.; Toh, C.H.; Levi, M.; Watson, H.G. The withdrawal of Activated Protein C from the use in patients with severe sepsis and DIC [Amendment to the BCSH guideline on disseminated intravascular coagulation]. Br. J. Haematol. 2012, 157, 493–494. [Google Scholar] [CrossRef]
- Kerschen, E.J.; Fernandez, J.A.; Cooley, B.C.; Yang, X.V.; Sood, R.; Mosnier, L.O.; Castellino, F.J.; Mackman, N.; Griffin, J.H.; Weiler, H. Endotoxemia and sepsis mortality reduction by non-anticoagulantactivated protein C. J. Exp. Med. 2007, 204, 2439–2448. [Google Scholar] [CrossRef]
- Saito, H.; Maruyama, I.; Shimazaki, S.; Yamamoto, Y.; Aikawa, N.; Ohno, R.; Hirayama, A.; Matsuda, T.; Asakura, H.; Nakashima, M.; et al. Efficacy and safety of recombinant human soluble thrombomodulin (ART-123) in disseminated intravascular coagulation: Results of a phase III, randomized, double-blind clinical trial. J. Thromb. Haemost. 2007, 5, 31–41. [Google Scholar] [CrossRef]
- Aikawa, N.; Shimazaki, S.; Yamamoto, Y.; Saito, H.; Maruyama, I.; Ohno, R.; Hirayama, A.; Aoki, Y.; Aoki, N. Thrombomodulin alfa in the treatment of infectious patients complicated by disseminated intravascular coagulation: Subanalysis from the phase 3 trial. Shock 2011, 35, 349–354. [Google Scholar] [CrossRef]
- Vincent, J.L.; Ramesh, M.K.; Ernest, D.; LaRosa, S.P.; Pachl, J.; Aikawa, N.; Hoste, E.; Levy, H.; Hirman, J.; Levi, M.; et al. A randomized, double-blind, placebo-controlled, Phase 2b study to evaluate the safety and efficacy of recombinant human soluble thrombomodulin, ART-123, in patients with sepsis and suspected disseminated intravascular coagulation. Crit. Care Med. 2013, 41, 2069–2079. [Google Scholar] [CrossRef]
- Vincent, J.L.; Francois, B.; Zabolotskikh, I.; Daga, M.K.; Lascarrou, J.B.; Kirov, M.Y.; Pettilä, V.; Wittebole, X.; Meziani, F.; Mercier, E. Effect of a Recombinant Human Soluble Thrombomodulin on Mortality in Patients With Sepsis-Associated Coagulopathy: The SCARLET Randomized Clinical Trial. JAMA 2019. [Google Scholar] [CrossRef]
- Yamakawa, K.; Murao, S.; Aihara, M. Recombinant Human Soluble Thrombomodulin in Sepsis-Induced Coagulopathy: An Updated Systematic Review and Meta-Analysis. Thromb. Haemost. 2019, 119, 56–65. [Google Scholar] [CrossRef]
- Lwaleed, B.A.; Bass, P.S. Tissue factor pathway inhibitor: Structure, biology and involvement in disease. J. Pathol. 2006, 208, 327–339. [Google Scholar] [CrossRef]
- Abraham, E.; Reinhart, K.; Opal, S.; Demeyer, I.; Doig, C.; Rodriguez, A.L.; Beale, R.; Svoboda, P.; Laterre, P.F.; Simon, S.; et al. Efficacy and safety of tifacogin (recombinant tissue factor pathway inhibitor) in severe sepsis: A randomized controlled trial. JAMA 2003, 290, 238–247. [Google Scholar] [CrossRef]
- Wunderink, R.G.; Laterre, P.F.; Francois, B.; Perrotin, D.; Artigas, A.; Vidal, L.O.; Lobo, S.M.; Juan, J.S.; Hwang, S.C.; Dugernier, T.; et al. Recombinant tissue factor pathway inhibitor in severe community-acquired pneumonia: A randomized trial. Am. J. Respir. Crit. Care Med. 2011, 183, 1561–1568. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ISTH overt DIC | SIC | ||
|---|---|---|---|
| Item | Score | Range | Range |
| Platelet count (×109/L) | 2 | <50 | <100 |
| 1 | ≥50, <100 | ≥100, <150 | |
| FDP/D-dimer | 3 | Strong increase | - |
| 2 | Moderate increase | - | |
| Prothrombin Time (PT ratio) | 2 | ≥6 sec | (>1.4) |
| 1 | ≥3 sec, <6 sec | (>1.2, ≤1.4) | |
| Fibrinogen (g/mL) | 1 | <100 | − |
| SOFA score | 2 | - | ≥2 |
| 1 | - | 1 | |
| Total score for DIC or SIC | ≥5 | ≥4 |
| Agent | Recommendation | Rationale | |
|---|---|---|---|
| Unfractionated heparin, low-molecular-weight heparin | None, except for deep vein thrombosis prevention | Efficacy for venous thromboembolic prophylaxis is expected, but insufficient supportive data for DIC treatment. | |
| Antithrombin | If it is available | Optional choice | Although phase III study (KyberSept) did not find efficacy in sepsis (but did show increased bleeding), meta-analysis of DIC patient subset showed beneficial effect in survival [85]. |
| If it is not available | None | - | |
| Recombinant thrombomodulin | If it is available | Optional choice | Although phase III study (SCARLET) did not show efficacy in sepsis with coagulopathy, meta-analysis found trend toward improved survival [86]. |
| If it is not available | None | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iba, T.; Levy, J.H.; Raj, A.; Warkentin, T.E. Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. J. Clin. Med. 2019, 8, 728. https://doi.org/10.3390/jcm8050728
Iba T, Levy JH, Raj A, Warkentin TE. Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. Journal of Clinical Medicine. 2019; 8(5):728. https://doi.org/10.3390/jcm8050728
Chicago/Turabian StyleIba, Toshiaki, Jerrold H. Levy, Aditya Raj, and Theodore E. Warkentin. 2019. "Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation" Journal of Clinical Medicine 8, no. 5: 728. https://doi.org/10.3390/jcm8050728
APA StyleIba, T., Levy, J. H., Raj, A., & Warkentin, T. E. (2019). Advance in the Management of Sepsis-Induced Coagulopathy and Disseminated Intravascular Coagulation. Journal of Clinical Medicine, 8(5), 728. https://doi.org/10.3390/jcm8050728