Impact of Lymphocyte and Neutrophil Counts on Mortality Risk in Severe Community-Acquired Pneumonia with or without Septic Shock

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Ethics
2.3. Leukocyte Quantification
2.4. Main Outcome Measures
2.5. Other Study Variables
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics (Table 1)
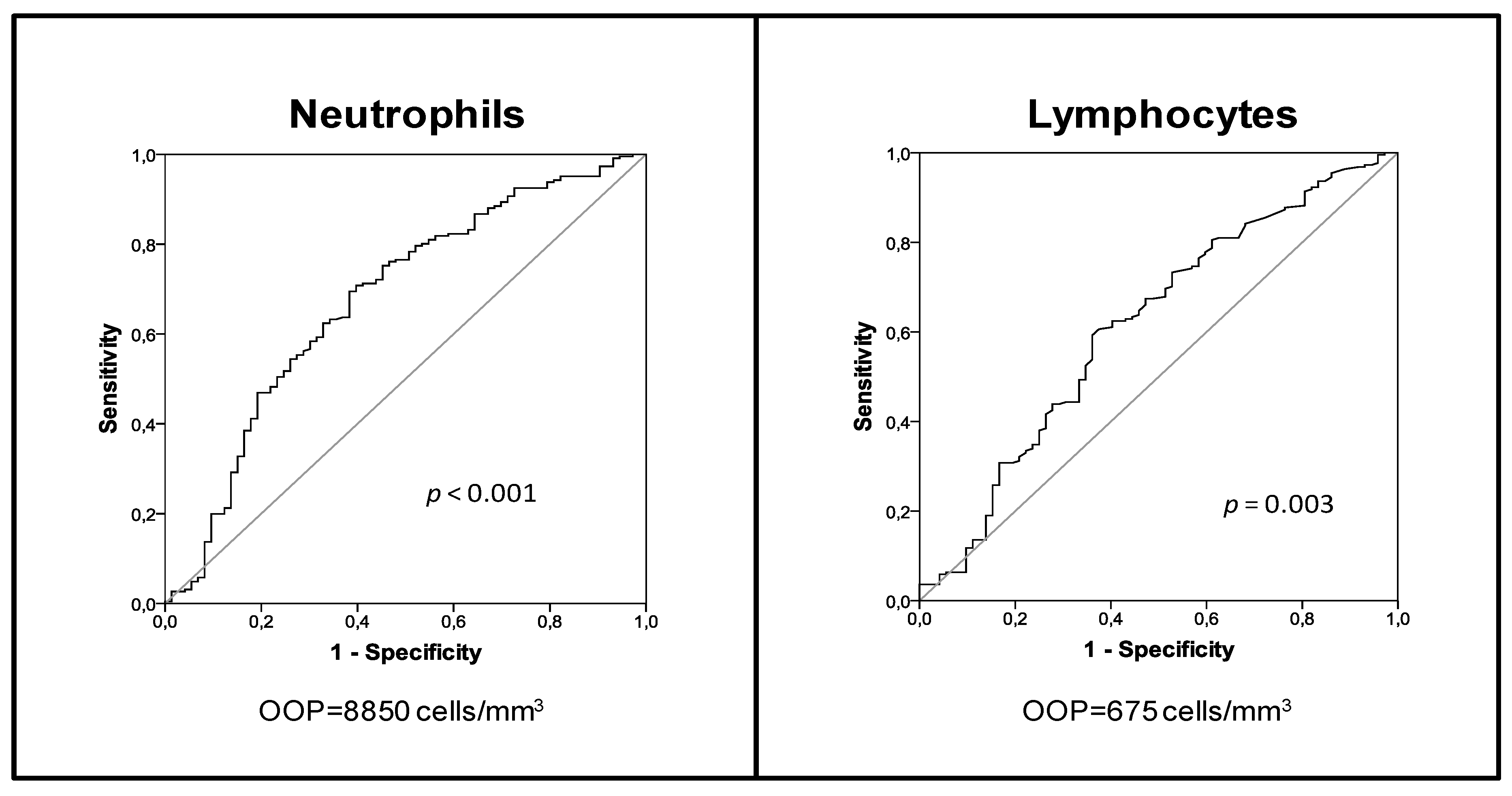
3.2. Analysis of Mortality Risk in the Group of Patients with sCAP and Septic Shock
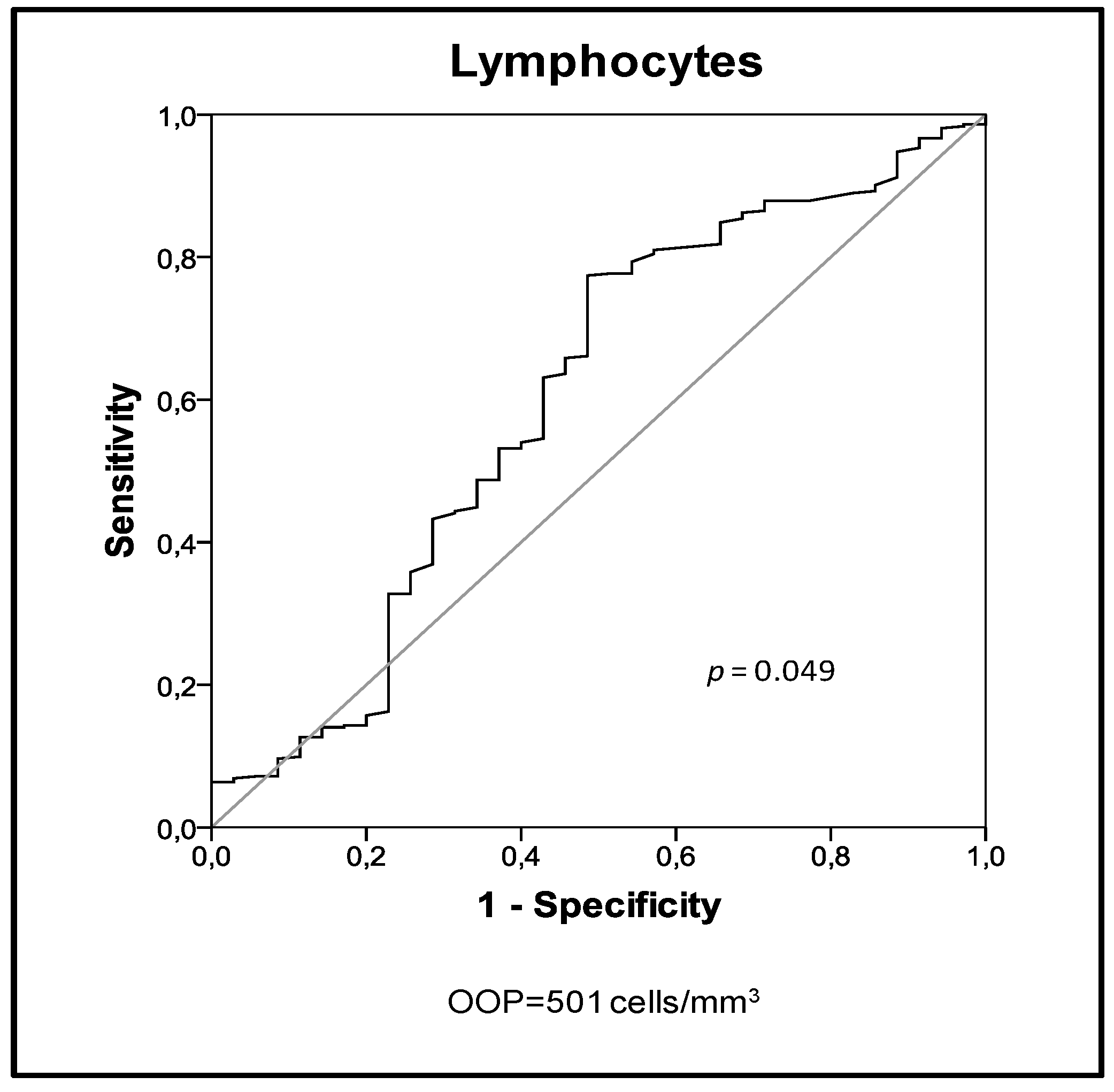
3.3. Analysis of Mortality Risk in the Group of Patients with sCAP and No Septic Shock
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Almirall, J.; Bolíbar, I.; Vidal, J.; Sauca, G.; Coll, P.; Niklasson, B.; Bartolomé, M.; Balanzó, X. Epidemiology of community-acquired pneumonia in adults: A population-based study. Eur. Respir. J. 2000, 15, 757–763. [Google Scholar] [CrossRef]
- Almirall, J.; Güell, E.; Capdevila, J.A.; Campins, L.; Palomera, E.; Martinez, R.; Miró, G.; de la Torre, M.C.; Solsona, M.; Yébenes, J.C. Epidemiology of community-acquired severe sepsis. A population-based study. Med. Clin. 2016, 147, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Pascual, F.E.; Matthay, M.A.; Bacchetti, P.; Wachter, R.M. Assessment of prognosis in patients with community-acquired pneumonia who require mechanical ventilation. Chest 2000, 117, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Fine, M.J.; Smith, M.A.; Carson, C.A.; Mutha, S.S.; Sankey, S.S.; Weissfeld, L.A.; Kapoor, W.N. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA 1996, 275, 134–141. [Google Scholar] [CrossRef]
- Chalfin, D.B.; Trzeciak, S.; Likourezos, A.; Baumann, B.M.; Dellinger, R.P. DELAY-ED study group Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit. Care Med. 2007, 35, 1477–1483. [Google Scholar] [CrossRef]
- Renaud, B.; Brun-Buisson, C.; Santin, A.; Coma, E.; Noyez, C.; Fine, M.J.; Yealy, D.M.; Labarère, J. Outcomes of early, late, and no admission to the intensive care unit for patients hospitalized with community-acquired pneumonia. Acad. Emerg. Med. 2012, 19, 294–303. [Google Scholar] [CrossRef]
- Renaud, B.; Santin, A.; Coma, E.; Camus, N.; Van Pelt, D.; Hayon, J.; Gurgui, M.; Roupie, E.; Hervé, J.; Fine, M.J.; et al. Association between timing of intensive care unit admission and outcomes for emergency department patients with community-acquired pneumonia. Crit. Care Med. 2009, 37, 2867–2874. [Google Scholar] [CrossRef] [PubMed]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. 2), S27–S72. [Google Scholar] [CrossRef]
- Lee, K.-Y. A common immunopathogenesis mechanism for infectious diseases: The protein-homeostasis-system hypothesis. Infect. Chemother. 2015, 47, 12–26. [Google Scholar] [CrossRef] [PubMed]
- Scicluna, B.P.; van Vught, L.A.; Zwinderman, A.H.; Wiewel, M.A.; Davenport, E.E.; Burnham, K.L.; Nürnberg, P.; Schultz, M.J.; Horn, J.; Cremer, O.L.; et al. Classification of patients with sepsis according to blood genomic endotype: A prospective cohort study. Lancet Respir. Med. 2017, 5, 816–826. [Google Scholar] [CrossRef]
- Dela Cruz, C.S.; Wunderink, R.G.; Christiani, D.C.; Cormier, S.A.; Crothers, K.; Doerschuk, C.M.; Evans, S.E.; Goldstein, D.R.; Khatri, P.; Kobzik, L.; et al. Future Research Directions in Pneumonia. NHLBI Working Group Report. Am. J. Respir. Crit. Care Med. 2018, 198, 256–263. [Google Scholar] [CrossRef]
- Bermejo-Martin, J.F.; Almansa, R.; Martin-Fernandez, M.; Menendez, R.; Torres, A. Immunological profiling to assess disease severity and prognosis in community-acquired pneumonia. Lancet Respir. Med. 2017, 5, e35–e36. [Google Scholar] [CrossRef] [Green Version]
- Bermejo-Martín, J.F.; Tamayo, E.; Ruiz, G.; Andaluz-Ojeda, D.; Herrán-Monge, R.; Muriel-Bombín, A.; Fe Muñoz, M.; Heredia-Rodríguez, M.; Citores, R.; Gómez-Herreras, J.; et al. Circulating neutrophil counts and mortality in septic shock. Crit. Care 2014, 18, 407. [Google Scholar] [CrossRef]
- Wyllie, D.H.; Bowler, I.C.J.W.; Peto, T.E.A. Relation between lymphopenia and bacteraemia in UK adults with medical emergencies. J. Clin. Pathol. 2004, 57, 950–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkins, C.A.; Collignon, P.; Adams, D.N.; Bowden, F.J.; Cook, M.C. Profound lymphopenia and bacteraemia. Intern. Med. J. 2006, 36, 385–388. [Google Scholar] [CrossRef]
- Rodriguez-Fernandez, A.; Andaluz-Ojeda, D.; Almansa, R.; Justel, M.; Eiros, J.M.; Ortiz de Lejarazu, R. Eosinophil as a protective cell in S. aureus ventilator-associated pneumonia. Mediators Inflamm. 2013, 2013, 152943. [Google Scholar] [CrossRef] [PubMed]
- Curbelo, J.; Luquero Bueno, S.; Galván-Román, J.M.; Ortega-Gómez, M.; Rajas, O.; Fernández-Jiménez, G.; Vega-Piris, L.; Rodríguez-Salvanes, F.; Arnalich, B.; Díaz, A.; et al. Inflammation biomarkers in blood as mortality predictors in community-acquired pneumonia admitted patients: Importance of comparison with neutrophil count percentage or neutrophil-lymphocyte ratio. PLoS ONE 2017, 12, e0173947. [Google Scholar] [CrossRef]
- Marrie, T.J.; Wu, L. Factors influencing in-hospital mortality in community-acquired pneumonia: A prospective study of patients not initially admitted to the ICU. Chest 2005, 127, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Martin, J.F.; Cilloniz, C.; Mendez, R.; Almansa, R.; Gabarrus, A.; Ceccato, A.; Torres, A.; Menendez, R. NEUMONAC Group. Lymphopenic Community Acquired Pneumonia (L-CAP), an Immunological Phenotype Associated with Higher Risk of Mortality. EBioMedicine 2017, 24, 231–236. [Google Scholar] [CrossRef]
- de Jager, C.P.C.; van Wijk, P.T.L.; Mathoera, R.B.; de Jongh-Leuvenink, J.; van der Poll, T.; Wever, P.C. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit. Care 2010, 14, R192. [Google Scholar] [CrossRef]
- de Jager, C.P.C.; Wever, P.C.; Gemen, E.F.A.; Kusters, R.; van Gageldonk-Lafeber, A.B.; van der Poll, T.; Laheij, R.J.F. The neutrophil-lymphocyte count ratio in patients with community-acquired pneumonia. PLoS ONE 2012, 7, e46561. [Google Scholar] [CrossRef] [PubMed]
- Akilli, N.B.; Yortanlı, M.; Mutlu, H.; Günaydın, Y.K.; Koylu, R.; Akca, H.S.; Akinci, E.; Dundar, Z.D.; Cander, B. Prognostic importance of neutrophil-lymphocyte ratio in critically ill patients: Short- and long-term outcomes. Am. J. Emerg. Med. 2014, 32, 1476–1480. [Google Scholar] [CrossRef]
- Cataudella, E.; Giraffa, C.M.; Di Marca, S.; Pulvirenti, A.; Alaimo, S.; Pisano, M.; Terranova, V.; Corriere, T.; Ronsisvalle, M.L.; Di Quattro, R.; et al. Neutrophil-To-Lymphocyte Ratio: An Emerging Marker Predicting Prognosis in Elderly Adults with Community-Acquired Pneumonia. J. Am. Geriatr. Soc. 2017, 65, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.-L.; Ramsay, G.; et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Zimmerman, J.E.; Wagner, D.P.; Draper, E.A.; Lawrence, D.E. APACHE-acute physiology and chronic health evaluation: A physiologically based classification system. Crit. Care Med. 1981, 9, 591–597. [Google Scholar] [CrossRef]
- Almansa, R.; Ortega, A.; Ávila-Alonso, A.; Heredia-Rodríguez, M.; Martín, S.; Benavides, D.; Martín-Fernandez, M.; Rico, L.; Aldecoa, C.; Rico, J.; et al. Quantification of Immune Dysregulation by Next-generation Polymerase Chain Reaction to Improve Sepsis Diagnosis in Surgical Patients. Ann. Surg. 2019, 269, 545–553. [Google Scholar] [CrossRef]
- Lim, E.-M.; Cembrowski, G.; Cembrowski, M.; Clarke, G. Race-specific WBC and neutrophil count reference intervals. Int. J. Lab. Hematol. 2010, 32, 590–597. [Google Scholar] [CrossRef]
- Lee, K.-Y. Pneumonia, Acute Respiratory Distress Syndrome, and Early Immune-Modulator Therapy. Int. J. Mol. Sci. 2017, 18, 388. [Google Scholar] [CrossRef] [PubMed]
- Alfageme, I.; Aspa, J.; Bello, S.; Blanquer, J.; Blanquer, R.; Borderías, L.; Bravo, C.; de Celis, R.; de Gracia, X.; Dorca, J.; et al. Normativas para el diagnóstico y el tratamiento de la neumonía adquirida en la comunidad. Sociedad Española de Neumología y Cirugía Torácica (SEPAR). Arch. Bronconeumol. 2005, 41, 272–289. [Google Scholar]
- Rello, J.; Rodriguez, A.; Lisboa, T.; Gallego, M.; Lujan, M.; Wunderink, R. PIRO score for community-acquired pneumonia: A new prediction rule for assessment of severity in intensive care unit patients with community-acquired pneumonia. Crit. Care Med. 2009, 37, 456–462. [Google Scholar] [CrossRef]
- Bourquard, A.; Pablo-Trinidad, A.; Butterworth, I.; Sánchez-Ferro, Á.; Cerrato, C.; Humala, K.; Fabra Urdiola, M.; Del Rio, C.; Valles, B.; Tucker-Schwartz, J.M.; et al. Non-invasive detection of severe neutropenia in chemotherapy patients by optical imaging of nailfold microcirculation. Sci. Rep. 2018, 8, 5301. [Google Scholar] [CrossRef]
- Pfortmueller, C.A.; Meisel, C.; Fux, M.; Schefold, J.C. Assessment of immune organ dysfunction in critical illness: Utility of innate immune response markers. Intensive Care Med. Exp. 2017, 5, 49. [Google Scholar] [CrossRef] [PubMed]
- Mare, T.A.; Treacher, D.F.; Shankar-Hari, M.; Beale, R.; Lewis, S.M.; Chambers, D.J.; Brown, K.A. The diagnostic and prognostic significance of monitoring blood levels of immature neutrophils in patients with systemic inflammation. Crit. Care 2015, 19, 57. [Google Scholar] [CrossRef] [PubMed]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M. Sepsis Definitions Task Force Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No Septic Shock (n = 406) | Septic Shock (n = 304) | p Value | ||
|---|---|---|---|---|
| Characteristics | Age (years, median (IQR)) | 60 (30) | 63 (26) | n.s. |
| Male (%, (n)) | 67.0 (272) | 72.4 (220) | n.s. | |
| Comorbidities, (% (n)) | Chronic cardiovascular disease | 22.7 (92) | 18.1 (55) | n.s. |
| Chronic respiratory disease | 33.7 (137) | 37.8 (115) | n.s. | |
| Chronic renal failure | 4.2 (17) | 6.6 (20) | n.s. | |
| Diabetes mellitus | 27.1 (110) | 22.7 (69) | n.s. | |
| Time course and outcome | Mechanical ventilation (% (n)) | 30.8 (125) | 34.5 (105) | n.s. |
| APACHE II (median (IQR)) | 15.86 (7) | 18.00 (11) | <0.001 | |
| ICU mortality (% (n)) | 9.4 (38) | 25.3 (77) | <0.001 | |
| Microbiology, (% (n)) | Gram+ | 33.8 (136) | 57.9 (175) | <0.001 |
| Gram- | 21.2 (85) | 17.5 (53) | n.s. | |
| Fungi | 7.0 (28) | 4.3 (13) | n.s. | |
| Virus | 14.7 (59) | 7.0 (21) | 0.001 | |
| Polymicrobial | 9.5 (38) | 7.3 (22) | n.s. | |
| Measurements at diagnosis, (median (IQR)) | White blood cells (cells/mm3) | 11,990 (12,745) | 11,215 (18,315) | n.s. |
| Lymphocytes (cells/mm3) | 859 (895) | 716 (880) | 0.009 | |
| Neutrophils (cells/mm3) | 11,360 (10,180) | 11,900 (14,350) | n.s. | |
| OR | CI 95% | p | ||
|---|---|---|---|---|
| Age | 1.02 | 1.00 | 1.04 | 0.121 |
| APACHE-II | 1.07 | 1.03 | 1.12 | 0.001 |
| Gram–bacteria | 2.41 | 1.97 | 6.45 | <0.001 |
| Polymicrobial infection | 0.22 | 0.05 | 0.99 | 0.049 |
| Neutrophils < 8850 cells/mm3 | 3.57 | 1.97 | 6.45 | <0.001 |
| OR | CI 95% | p | ||
|---|---|---|---|---|
| Age | 1.01 | 0.99 | 1.03 | 0.217 |
| APACHE-II | 1.08 | 1.03 | 1.12 | <0.001 |
| Gram–bacteria | 2.04 | 0.91 | 4.56 | 0.083 |
| Polymicrobial infection | 0.31 | 0.07 | 1.36 | 0.119 |
| Lymphocytes < 675 cells/mm3 | 2.32 | 1.30 | 4.15 | 0.005 |
| OR | CI 95% | p | ||
|---|---|---|---|---|
| Age | 1.02 | 0.99 | 1.04 | 0.278 |
| Chronic obstructive pulmonary disease | 1.53 | 0.69 | 3.36 | 0.294 |
| APACHE-II | 1.09 | 1.03 | 1.15 | 0.003 |
| Mechanical ventilation | 1.49 | 0.68 | 3.29 | 0.318 |
| Gram–bacteria | 1.70 | 0.72 | 4.00 | 0.224 |
| Polymicrobial infection | 2.90 | 0.93 | 8.99 | 0.066 |
| Lymphocytes < 501 cells/mm3 | 3.76 | 1.74 | 8.14 | 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Güell, E.; Martín-Fernandez, M.; De la Torre, M.C.; Palomera, E.; Serra, M.; Martinez, R.; Solsona, M.; Miró, G.; Vallès, J.; Fernández, S.; et al. Impact of Lymphocyte and Neutrophil Counts on Mortality Risk in Severe Community-Acquired Pneumonia with or without Septic Shock. J. Clin. Med. 2019, 8, 754. https://doi.org/10.3390/jcm8050754
Güell E, Martín-Fernandez M, De la Torre MC, Palomera E, Serra M, Martinez R, Solsona M, Miró G, Vallès J, Fernández S, et al. Impact of Lymphocyte and Neutrophil Counts on Mortality Risk in Severe Community-Acquired Pneumonia with or without Septic Shock. Journal of Clinical Medicine. 2019; 8(5):754. https://doi.org/10.3390/jcm8050754
Chicago/Turabian StyleGüell, Estel, Marta Martín-Fernandez, Mari C. De la Torre, Elisabet Palomera, Mateu Serra, Rafael Martinez, Manel Solsona, Gloria Miró, Jordi Vallès, Samuel Fernández, and et al. 2019. "Impact of Lymphocyte and Neutrophil Counts on Mortality Risk in Severe Community-Acquired Pneumonia with or without Septic Shock" Journal of Clinical Medicine 8, no. 5: 754. https://doi.org/10.3390/jcm8050754
APA StyleGüell, E., Martín-Fernandez, M., De la Torre, M. C., Palomera, E., Serra, M., Martinez, R., Solsona, M., Miró, G., Vallès, J., Fernández, S., Cortés, E., Ferrer, V., Morales, M., Yébenes, J. C., Almirall, J., & Bermejo-Martin, J. F. (2019). Impact of Lymphocyte and Neutrophil Counts on Mortality Risk in Severe Community-Acquired Pneumonia with or without Septic Shock. Journal of Clinical Medicine, 8(5), 754. https://doi.org/10.3390/jcm8050754