Effects of Variability in Blood Pressure, Glucose, and Cholesterol Concentrations, and Body Mass Index on End-Stage Renal Disease in the General Population of Korea

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Measurements and Definitions
2.3. Definition of Variability and Scoring
2.4. Study Outcomes and Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Risk of ESRD According to the Variability for Each Parameter
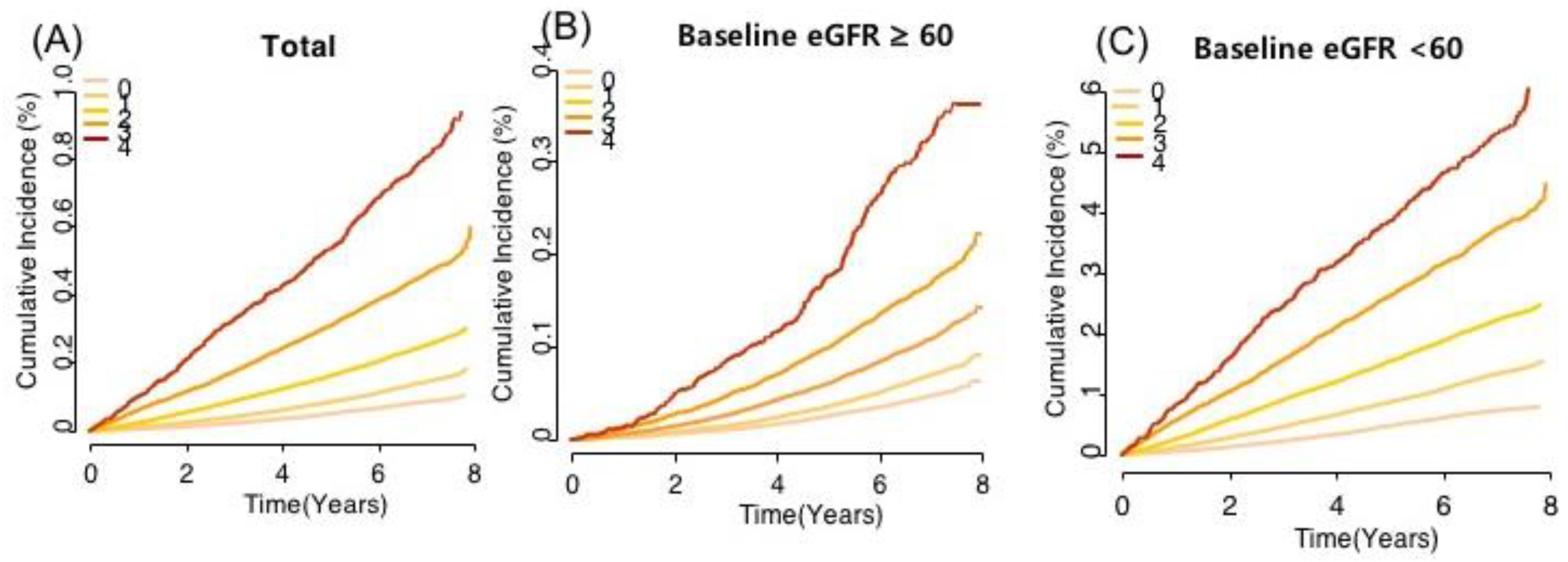
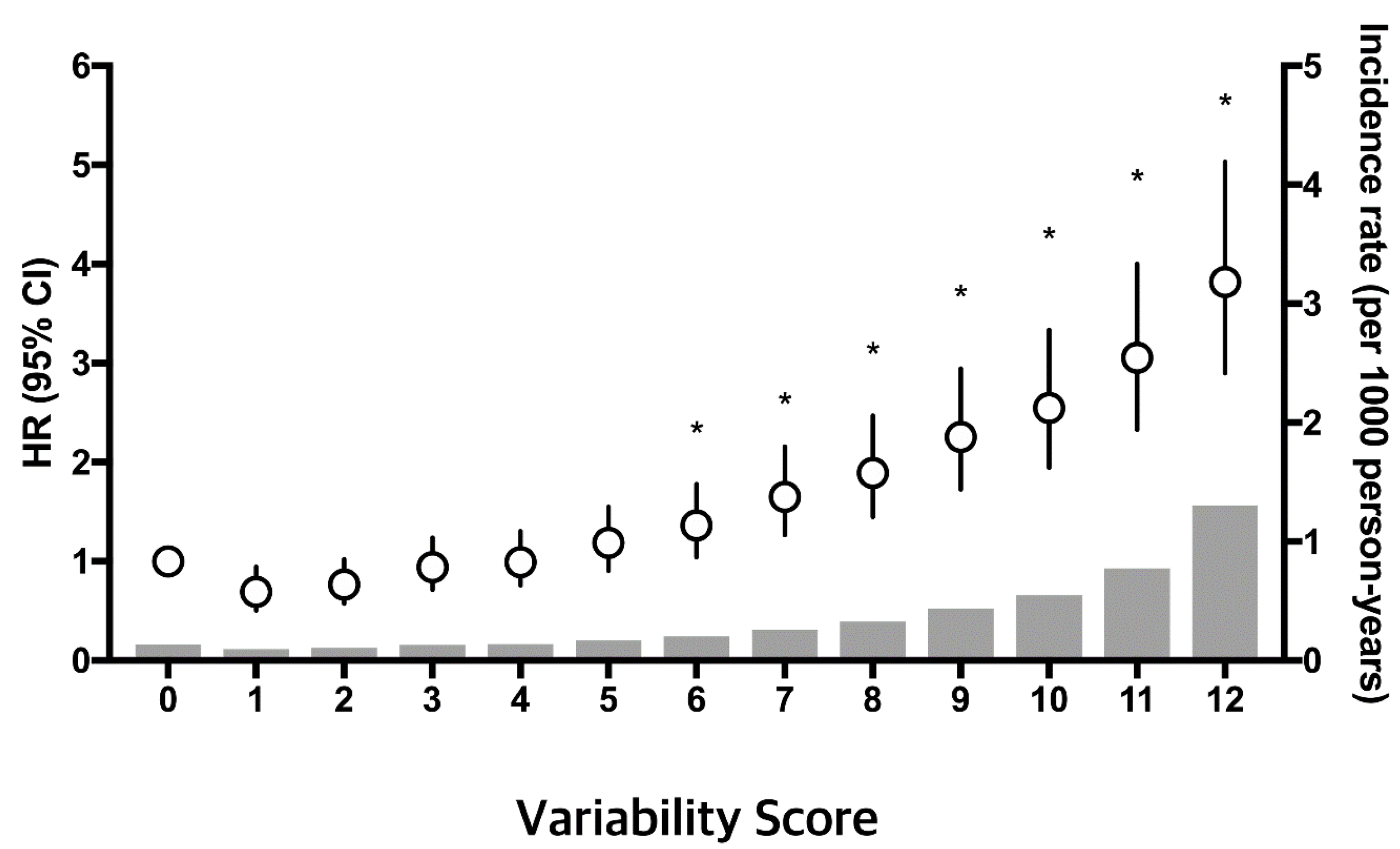
3.3. Risk of ESRD According to the Number of High-Variability Parameters
3.4. Sensitivity Analysis
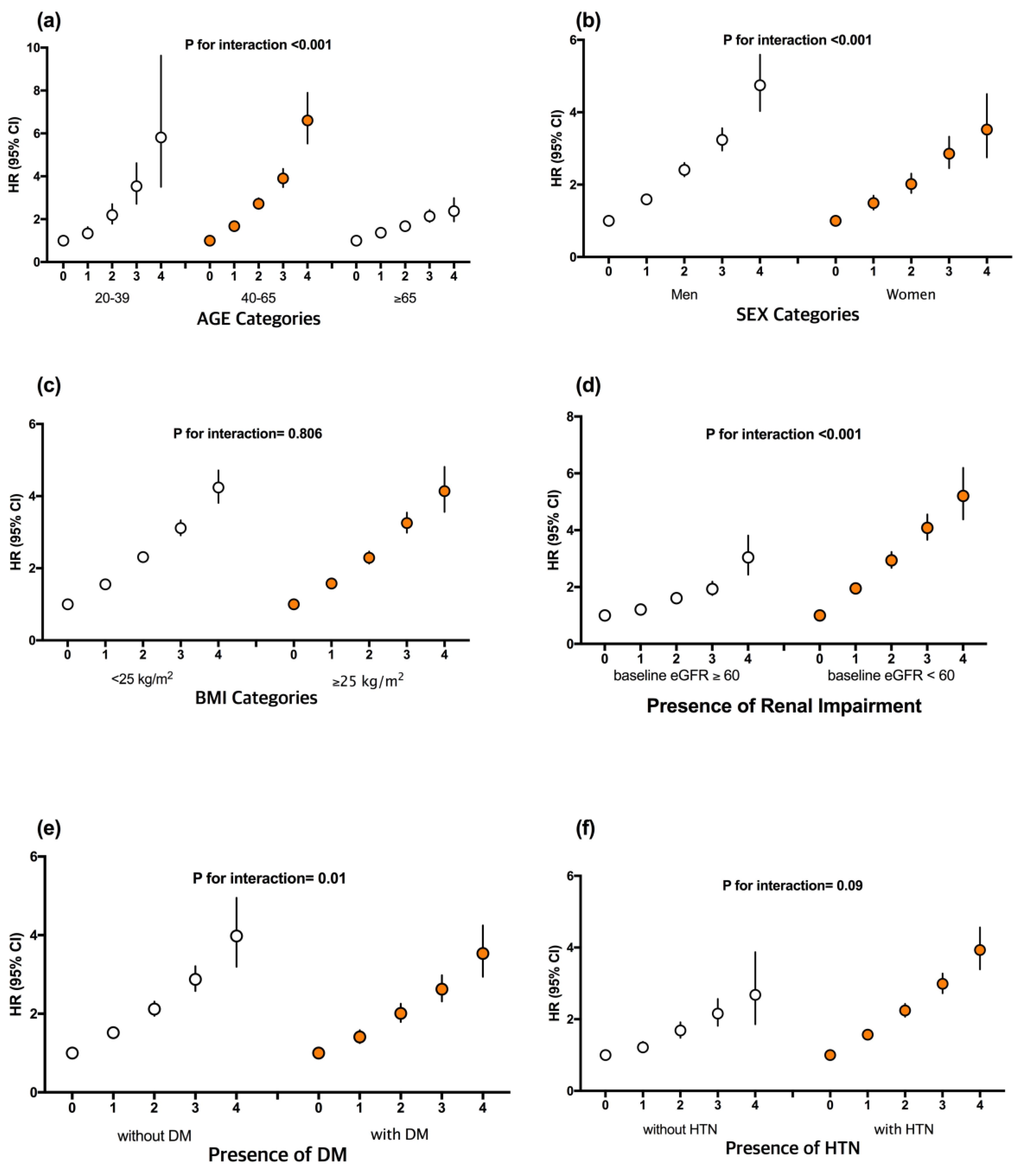
3.5. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nissenson, A.R. Improving Outcomes for ESRD Patients: Shifting the Quality Paradigm. Clin. J. Am. Soc. Nephrol. 2014, 9, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Ng, I.H.Y.; Cheung, K.K.T.; Yau, T.T.L.; Chow, E.; Ozaki, R.; Chan, J.C.N. Evolution of Diabetes Care in Hong Kong: From the Hong Kong Diabetes Register to JADE-PEARL Program to RAMP and PEP Program. Endocrinol. Metab. (Seoul) 2018, 33, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Han, K.; Park, Y.M.; Kwon, H.S.; Kang, G.; Yoon, K.H.; Lee, S.H. Associations of Variability in Blood Pressure, Glucose and Cholesterol Concentrations, and Body Mass Index With Mortality and Cardiovascular Outcomes in the General Population. Circulation 2018, 138, 2627–2637. [Google Scholar] [CrossRef]
- Bangalore, S.; Fayyad, R.; Laskey, R.; DeMicco, D.A.; Messerli, F.H.; Waters, D.D. Body-Weight Fluctuations and Outcomes in Coronary Disease. N. Engl. J. Med. 2017, 376, 1332–1340. [Google Scholar] [CrossRef]
- Gosmanova, E.O.; Mikkelsen, M.K.; Molnar, M.Z.; Lu, J.L.; Yessayan, L.T.; Kalantar-Zadeh, K.; Kovesdy, C.P. Association of systolic blood pressure variability with mortality, coronary heart disease, stroke, and renal disease. J. Am. Coll. Cardiol. 2016, 68, 1375–1386. [Google Scholar] [CrossRef]
- Bangalore, S.; Breazna, A.; DeMicco, D.A.; Wun, C.C.; Messerli, F.H.; TNT Steering Committee and Investigators. Visit-to-visit low-density lipoprotein cholesterol variability and risk of cardiovascular outcomes: Insights from the TNT trial. J. Am. Coll. Cardiol. 2015, 65, 1539–1548. [Google Scholar] [CrossRef]
- Li, T.C.; Yang, C.P.; Tseng, S.T.; Li, C.I.; Liu, C.S.; Lin, W.Y.; Hwang, K.L.; Yang, S.Y.; Chiang, J.H.; Lin, C.C. Visit-to-Visit Variations in Fasting Plasma Glucose and HbA1c Associated With an Increased Risk of Alzheimer Disease: Taiwan Diabetes Study. Diabetes Care 2017, 40, 1210–1217. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.K.; Han, K.; Kim, H.S.; Park, Y.M.; Kwon, H.S.; Yoon, K.H.; Lee, S.H. Cholesterol variability and the risk of mortality, myocardial infarction, and stroke: A nationwide population-based study. Eur. Heart J. 2017, 38, 3560–3566. [Google Scholar] [CrossRef]
- Yang, Y.F.; Li, T.C.; Li, C.I.; Liu, C.S.; Lin, W.Y.; Yang, S.Y.; Chiang, J.H.; Huang, C.C.; Sung, F.C.; Lin, C.C. Visit-to-Visit Glucose Variability Predicts the Development of End-Stage Renal Disease in Type 2 Diabetes: 10-Year Follow-Up of Taiwan Diabetes Study. Medicine (Baltimore) 2015, 94, e1804. [Google Scholar] [CrossRef]
- Shafi, T.; Sozio, S.M.; Bandeen-Roche, K.J.; Ephraim, P.L.; Luly, J.R.; St Peter, W.L.; McDermott, A.; Scialla, J.J.; Crews, D.C.; Tangri, N.; et al. Predialysis systolic BP variability and outcomes in hemodialysis patients. J. Am. Soc. Nephrol. 2014, 25, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Han, K.; Koh, E.S.; Kim, H.S.; Kwon, H.S.; Park, Y.M.; Yoon, K.H.; Lee, S.H. Variability in total cholesterol is associated with the risk of end-stage renal disease: A nationwide population-based study. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1963–1970. [Google Scholar] [CrossRef]
- Nashar, K.; Egan, B.M. Relationship between chronic kidney disease and metabolic syndrome: Current perspectives. Diabetes Metab. Syndr. Obes. 2014, 7, 421–435. [Google Scholar] [CrossRef]
- Lee, Y.H.; Han, K.; Ko, S.H.; Ko, K.S.; Lee, K.U. Data Analytic Process of a Nationwide Population-Based Study Using National Health Information Database Established by National Health Insurance Service. Diabetes Metab. J. 2016, 40, 79–82. [Google Scholar] [CrossRef]
- Yang, H.K.; Han, K.; Kwon, H.S.; Park, Y.M.; Cho, J.H.; Yoon, K.H.; Kang, M.I.; Cha, B.Y.; Lee, S.H. Obesity, metabolic health, and mortality in adults: A nationwide population-based study in Korea. Sci. Rep. 2016, 6, 30329. [Google Scholar] [CrossRef]
- Lamb, E.J.; Tomson, C.R.; Roderick, P.J.; Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry. Estimating kidney function in adults using formulae. Ann. Clin. Biochem. 2005, 42, 321–345. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef]
- Hoshide, S. Clinical implication of visit-to-visit blood pressure variability. Hypertens. Res. 2018, 41, 993–999. [Google Scholar] [CrossRef]
- Mena, L.; Pintos, S.; Queipo, N.V.; Aizpurua, J.A.; Maestre, G.; Sulbaran, T. A reliable index for the prognostic significance of blood pressure variability. J. Hypertens. 2005, 23, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Fukuda, K.; Kai, H.; Kamouchi, M.; Hata, J.; Ago, T.; Nakane, H.; Imaizumi, T.; Kitazono, T.; FSR Investigators. Day-by-day blood pressure variability and functional outcome after acute ischemic stroke: Fukuoka stroke registry. Stroke 2015, 46, 1832–1839. [Google Scholar] [CrossRef]
- Krinsley, J.S.; Preiser, J.C. Time in blood glucose range 70 to 140 mg/dL >80% is strongly associated with increased survival in non-diabetic critically ill adults. Crit. Care 2015, 19, 179. [Google Scholar] [CrossRef]
- Cardoso, C.R.L.; Leite, N.C.; Moram, C.B.M.; Salles, G.F. Long-term visit-to-visit glycemic variability as predictor of micro- and macrovascular complications in patients with type 2 diabetes: The Rio de Janeiro Type 2 Diabetes Cohort Study. Cardiovasc. Diabetol. 2018, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Chen, C.C.; Chen, F.N.; Li, C.I.; Liu, C.S.; Lin, W.Y.; Yang, S.Y.; Lee, C.C.; Li, T.C. Risks of diabetic nephropathy with variation in hemoglobin A1c and fasting plasma glucose. Am. J. Med. 2013, 126, 1017.e1–1017.e10. [Google Scholar] [CrossRef]
- Jones, S.C.; Saunders, H.J.; Qi, W.; Pollock, C.A. Intermittent high glucose enhances cell growth and collagen synthesis in cultured human tubulointerstitial cells. Diabetologia 1999, 42, 1113–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarafidis, P.A.; Ruilope, L.M.; Loutradis, C.; Gorostidi, M.; de la Sierra, A.; de la Cruz, J.J.; Vinyoles, E.; Divisón-Garrote, J.A.; Segura, J.; Banegas, J.R. Blood pressure variability increases with advancing chronic kidney disease stage: A cross-sectional analysis of 16546 hypertensive patients. J. Hypertens. 2018, 36, 1076–1085. [Google Scholar] [CrossRef] [PubMed]
- Mezue, K.; Goyal, A.; Pressman, G.S.; Horrow, J.C.; Rangaswami, J. Blood Pressure Variability Predicts Adverse Events and Cardiovascular Outcomes in Chronic Kidney Disease: A Post-Hoc Analysis of the SPRINT Trial. Am. J. Hypertens. 2017, 31, 48–52. [Google Scholar] [CrossRef]
- Ku, E.; Kopple, J.D.; Johansen, K.L.; McCulloch, C.E.; Go, A.S.; Xie, D.; Lin, F.; Hamm, L.L.; He, J.; Kusek, J.W.; et al. Longitudinal Weight Change During CKD Progression and Its Association With Subsequent Mortality. Am. J. Kidney Dis. 2018, 71, 657–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaman, S.B.; Hossain, N.; Rahman, M. Associations between Body Mass Index and Chronic Kidney Disease in Type 2 Diabetes Mellitus Patients: Findings from the Northeast of Thailand. Diabetes Metab. J. 2018, 42, 330–337. [Google Scholar] [CrossRef]
- Ryu, S.; Chang, Y.; Woo, H.Y.; Kim, S.G.; Kim, D.I.; Kim, W.S.; Suh, B.S.; Choi, N.K.; Lee, J.T. Changes in body weight predict CKD in healthy men. J. Am. Soc. Nephrol. 2008, 19, 1798–1805. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, S.M.; Han, K.D.; Son, J.W.; Lee, S.S.; Oh, S.W.; Lee, W.Y.; Yoo, S.J.; Taskforce Team of the Obesity Fact Sheet of the Korean Society for the Study of Obesity. Change in Weight and Body Mass Index Associated With All-Cause Mortality in Korea: A Nationwide Longitudinal Study. J. Clin. Endocrinol. Metab. 2017, 102, 4041–4050. [Google Scholar] [CrossRef]
- Russo, G.T.; De Cosmo, S.; Viazzi, F.; Pacilli, A.; Ceriello, A.; Genovese, S.; Guida, P.; Giorda, C.; Cucinotta, D.; Pontremoli, R.; et al. Plasma Triglycerides and HDL-C Levels Predict the Development of Diabetic Kidney Disease in Subjects With Type 2 Diabetes: The AMD Annals Initiative. Diabetes Care 2016, 39, 2278–2287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.H.; Chang, D.M.; Lin, K.C.; Hsieh, C.H.; Lee, Y.J. High-density lipoprotein cholesterol and the risk of nephropathy in type 2 diabetic patients. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, F. HDL in CKD-The Devil Is in the Detail. J. Am. Soc. Nephrol. 2018, 29, 1356–1371. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 0 (n = 2,782,077) | 1 (n = 3,209,154) | 2 (n = 1,678,400) | 3 (n = 470,610) | 4 (n = 58,894) | |
|---|---|---|---|---|---|
| Age (years) | 47.0 ± 12.6 | 48.1 ± 13.7 | 49.6 ± 14.6 | 51.3 ± 15.5 | 53.3 ± 16.0 |
| Sex (male) | 1,769,429 (63.6) | 1,868,857 (58.2) | 905,309 (53.9) | 238,342 (50.7) | 28,387 (48.2) |
| FBG (mg/dL) | 95.4 ± 17.0 | 96.7 ± 21.2 | 98.7 ± 25.5 | 101.0 ± 30.0 | 104.0 ± 35.2 |
| TC (mg/dL) | 196.3 ± 33.2 | 195.6 ± 35.8 | 195.2 ± 38.9 | 194.9 ± 42.4 | 193.8 ± 45.5 |
| HDL cholesterol (mg/dL) | 54.7 ± 19.0 | 55.1 ± 19.9 | 55.4 ± 20.6 | 55.6 ± 21.9 | 55.3 ± 21.9 |
| LDL cholesterol (mg/dL) | 116.6 ± 44.5 | 115.1 ± 46.1 | 114.0 ± 47.7 | 112.8 ± 48.8 | 111.3 ± 49.3 |
| Triglyceride (mg/dL) | 110 (75–163) | 110 (76–164) | 112 (77–166) | 114 (79–170) | 117 (80–174) |
| eGFR (mL/min/1.73 m2) | 86.5 ± 42.6 | 87.0 ± 40.1 | 87.2 ± 39.2 | 87.1 ± 39.3 | 86.7 ± 39.0 |
| eGFR < 60 mL/min/1.73m2 | 167,159 (6.0) | 201,998(6.3) | 121,175 (7.2) | 40,717 (8.7) | 6287 (10.7) |
| Proteinuria (yes) a | 49,727 (1.8) | 68,587(2.1) | 43,510 (2.6) | 15,293 (3.3) | 2442 (4.2) |
| Systolic BP (mmHg) | 122.5 ± 13.0 | 122.4 ± 14.6 | 122.6 ± 15.9 | 122.8 ± 17.3 | 123.0 ± 18.8 |
| Diastolic BP (mmHg) | 76.6 ± 9.3 | 76.4 ± 9.8 | 76.3 ± 10.2 | 76.2 ± 10.7 | 76.1 ± 11.3 |
| BMI (kg/m2) | 23.7 ± 3.0 | 23.8 ± 3.1 | 23.8 ± 3.3 | 23.8 ± 3.4 | 23.7 ± 3.5 |
| Waist circumferences (cm) | 80.5 ± 8.7 | 80.5 ± 8.9 | 80.7 ± 9.1 | 80.9 ± 9.2 | 81.0 ± 9.4 |
| Variability | |||||
| VIM of FBG (%) | 7.1 ± 3.1 | 9.9 ± 5.7 | 12.5 ± 6.6 | 15.4 ± 6.6 | 18.6 ± 5.4 |
| VIM of TC (%) | 13. 8 ± 5.7 | 18.7 ± 10.7 | 24.7 ± 13.0 | 30.9 ± 13.2 | 36.6 ± 11.5 |
| VIM of systolic BP (%) | 6.9 ± 2.9 | 9.3 ± 4. 9 | 11.4 ± 5.5 | 13.6 ± 5.4 | 16.4 ± 4.0 |
| VIM of diastolic BP (%) | 5.85 ± 3.0 | 6.6 ± 3.6 | 7.4 ± 3.9 | 8.3 ± 4.1 | 9.4 ± 4.1 |
| VIM of BMI (%) | 0.5 ± 0.2 | 0.7 ± 0.5 | 1.0 ± 0.6 | 1.2 ± 0.7 | 1.5 ± 0.7 |
| Current smoker (yes) | 724,804 (26.1) | 815,211 (25.4) | 406,455 (24.2) | 108,387 (23.0) | 12,866 (21.9) |
| Heavy alcohol drinker (yes) | 218,920 (7.9) | 244,023 (7.6) | 123,648 (7.4) | 34,132 (7.3) | 4116 (7.0) |
| Regular Exercise | 570,589 (20.5) | 635,744 (19.8) | 318,960 (19.0) | 84,638 (18.0) | 9902 (16.8) |
| Income (lower 25%) | 396,775 (14.3) | 527,799 (16.5) | 307,135 (18.3) | 91,791 (19.5) | 12,024 (20.4) |
| Diabetes mellitus | 138,223 (5.0) | 261,325 (8.1) | 205,021 (12.2) | 82,009 (17.4) | 14,272 (24.2) |
| Hypertension | 594,422 (21.4) | 835,561 (26.0) | 525,243 (31.3) | 173,001 (36.8) | 25,115 (42.6) |
| Dyslipidemia | 314,731 (11.3) | 502,007 (15.6) | 343,067 (20.4) | 117,774 (25.0) | 17,128 (29.1) |
| No ESRD (n = 8,185,535) | ESRD (n = 13,600) | |
|---|---|---|
| Age (years) | 48.2 ± 13.7 | 60.9 ± 13.0 |
| Sex (male) | 4,800,955 (58.7) | 9369 (68.9) |
| FBG (mg/dL) | 96.9 ± 21.6 | 118.8 ± 50.9 |
| TC (mg/dL) | 195.7 ± 36.1 | 192.6 ± 44.9 |
| HDL cholesterol (mg/dL) | 55.1 ± 19.9 | 50.2 ± 23.8 |
| LDL cholesterol (mg/dL) | 115.2 ± 46.1 | 111.4 ± 48.2 |
| Triglyceride (mg/dL) | 111 (76–165) | 136 (96–199) |
| eGFR (mL/min/1.73 m2) | 86.9 ± 40.7 | 54.7 ± 34.9 |
| eGFR <60mL/min/1.73m2 | 529,140 (6.5) | 8196 (60.3) |
| Proteinuria a | 173,792 (2.1) | 5767 (42.4) |
| Systolic BP (mmHg) | 122.5 ± 14.5 | 132.3 ± 17.8 |
| Diastolic BP (mmHg) | 76.4 ± 9.8 | 79.5 ± 11.0 |
| BMI (kg/m2) | 23.7 ± 3.1 | 24.1 ± 3.2 |
| Waist circumferences (cm) | 80.6 ± 8.9 | 84.2 ± 8.9 |
| Variability | ||
| VIM of FBG (%) | 9.9 ± 5.8 | 12.2 ± 8.0 |
| VIM of TC (%) | 19.1 ± 11.3 | 26.3 ± 15. 8 |
| VIM of systolic BP (%) | 9.2 ± 5.0 | 10.9 ± 6.0 |
| VIM of diastolic BP (%) | 6.6 ± 3.6 | 7.7 ± 4.3 |
| VIM of BMI (%) | 0.73 ± 0.51 | 0.86 ± 0.62 |
| Current smoker (yes) | 2,064,667 (25.2) | 3056 (22.5) |
| Heavy alcohol drinker (yes) | 624,100 (7.6) | 739 (5.4) |
| Regular Exercise | 1,617,018 (19.8) | 2815 (20.7) |
| Income (lower 25%) | 1,332,692 (16.3) | 2832 (20.8) |
| Diabetes mellitus | 694,862 (8.5) | 5988 (44.0) |
| Hypertension | 2,142,688 (26.2) | 10,654 (78.3) |
| Dyslipidemia | 1,289,041 (15.8) | 5666 (41.7) |
| Events (n) | Follow-Up Duration (Person-Year) | Incidence Rate (per 1000 Person-Years) | Model 1 | Model 2 | Model 3 | |
|---|---|---|---|---|---|---|
| Glucose variability (VIM of FBG) | ||||||
| Q1 | 2771 | 14,077,785 | 0.20 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Q2 | 2702 | 14,204,338 | 0.19 | 1.02 (0.96,1.07) | 1.01 (0.96,1.06) | 1.01 (0.96,1.06) |
| Q3 | 3090 | 14,240,501 | 0.22 | 1.16 (1.11,1.23) | 1.13 (1.07,1.19) | 1.16 (1.11,1.22) |
| Q4 | 5037 | 14,201,590 | 0.35 | 1.73 (1.65,1.81) | 1.46 (1.40,1.53) | 1.47 (1.40,1.54) |
| p for trend | <0.0001 | <0.0001 | <0.0001 | |||
| Cholesterol variability (VIM of TC) | ||||||
| Q1 | 2091 | 14,144,226 | 0.15 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Q2 | 2276 | 14,264,721 | 0.16 | 1.12 (1.05,1.19) | 1.11 (1.04,1.17) | 1.06 (1.00,1.13) |
| Q3 | 2923 | 14,240,930 | 0.21 | 1.39 (1.31,1.47) | 1.35 (1.27,1.43) | 1.31 (1.23,1.38) |
| Q4 | 6310 | 14,074,337 | 0.45 | 2.52 (2.40,2.65) | 2.27 (2.16,2.39) | 2.08 (1.97,2.18) |
| p for trend | <0.0001 | <0.0001 | <0.0001 | |||
| Blood pressure variability (VIM of systolic BP) | ||||||
| Q1 | 2794 | 14,348,779 | 0.19 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Q2 | 2591 | 14,032,640 | 0.18 | 1.02 (0.97,1.08) | 1.04 (0.98,1.10) | 0.98 (0.93,1.04) |
| Q3 | 3165 | 14,160,292 | 0.22 | 1.13 (1.07,1.19) | 1.12 (1.07,1.18) | 1.08 (1.03,1.14) |
| Q4 | 5050 | 14,182,504 | 0.36 | 1.53 (1.46,1.61) | 1.52 (1.45,1.59) | 1.46 (1.39,1.53) |
| p for trend | <0.0001 | <0.0001 | <0.0001 | |||
| BMI variability (VIM of BMI) | ||||||
| Q1 | 2909 | 14,166,998 | 0.21 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Q2 | 2753 | 14,261,067 | 0.19 | 1.00 (0.94,1.05) | 0.99 (0.94,1.04) | 0.98 (0.93,1.04) |
| Q3 | 3319 | 14,223,477 | 0.23 | 1.21 (1.15,1.27) | 1.20 (1.14,1.26) | 1.20 (1.14,1.26) |
| Q4 | 4619 | 14,072,671 | 0.33 | 1.65 (1.57,1.72) | 1.58 (1.51,1.66) | 1.56 (1.49,1.64) |
| p for trend | <0.0001 | <0.0001 | <0.0001 | |||
| Events (n) | Follow-Up Duration (Person-Years) | Incidence Rate (Per 1000 Person-Years) | Model 1 | Model 2 | Model 3 | ||
|---|---|---|---|---|---|---|---|
| VIM | |||||||
| 0 | 2336 | 19,352,484 | 0.12 | 1 (ref.) | 1 (ref.) | 1 (ref.) | |
| 1 | 4540 | 22,215,048 | 0.20 | 1.57 (1.49,1.65) | 1.48 (1.41,1.56) | 1.54 (1.47,1.62) | |
| 2 | 4157 | 11,550,224 | 0.36 | 2.48 (2.36,2.61) | 2.21 (2.10,2.32) | 2.25 (2.14,2.37) | |
| 3 | 2106 | 3,210,226 | 0.66 | 4.02 (3.79,4.27) | 3.36 (3.16,3.57) | 3.17 (2.99,3.37) | |
| 4 | 461 | 396,231 | 1.16 | 6.33 (5.73,7.00) | 4.93 (4.45,5.45) | 4.12 (3.72,4.57) | |
| p for trend | <0.0001 | <0.0001 | <0.0001 | ||||
| CV | |||||||
| 0 | 1884 | 19,622,314 | 0.10 | 1 (ref.) | 1 (ref.) | 1 (ref.) | |
| 1 | 4120 | 21,937,268 | 0.19 | 1.74 (1.65,1.84) | 1.57 (1.49,1.66) | 1.65 (1.56,1.74) | |
| 2 | 4335 | 11,471,033 | 0.38 | 3.03 (2.87,3.20) | 2.46 (2.32,2.60) | 2.50 (2.37,2.65) | |
| 3 | 2629 | 3,271,586 | 0.80 | 5.54 (5.22,5.88) | 4.03 (3.78,4.28) | 3.74 (3.51,3.98) | |
| 4 | 632 | 422,013 | 1.50 | 8.91 (8.13,9.76) | 5.85 (5.33,6.42) | 4.95 (4.51,5.44) | |
| p for trend | <0.0001 | <0.0001 | <0.0001 | ||||
| ARV | |||||||
| 0 | 1698 | 19,749,696 | 0.09 | 1 (ref.) | 1 (ref.) | 1 (ref.) | |
| 1 | 3884 | 21,390,895 | 0.18 | 1.75 (1.66,1.86) | 1.57 (1.48,1.66) | 1.66 (1.57,1.76) | |
| 2 | 4503 | 11,527,893 | 0.39 | 3.14 (2.97,3.33) | 2.50 (2.36,2.65) | 2.57 (2.42,2.72) | |
| 3 | 2757 | 3,546,361 | 0.78 | 5.32 (5.00,5.66) | 3.78 (3.54,4.02) | 3.56 (3.34,3.80) | |
| 4 | 758 | 509,369 | 1.49 | 8.97 (8.22,9.78) | 5.69 (5.21,6.22) | 4.82 (4.41,5.28) | |
| p for trend | <0.0001 | <0.0001 | <0.0001 | ||||
| Events (n) | Follow-Up Duration (Person-Years) | Incidence Rate (Per 1000 Person-Years) | Model 1 | Model 2 | Model 3 | |
|---|---|---|---|---|---|---|
| VIM | ||||||
| 0 | 517 | 13,581,340 | 0.04 | 1 (ref.) | 1(ref.) | 1 (ref.) |
| 1 | 667 | 14,105,586 | 0.05 | 1.22 (1.09,1.37) | 1.22 (1.09,1.37) | 1.24 (1.10,1.39) |
| 2 | 393 | 6,511,970 | 0.06 | 1.48 (1.30,1.69) | 1.47 (1.29,1.68) | 1.50 (1.32,1.72) |
| 3 | 166 | 1,584,979 | 0.10 | 2.40 (2.01,2.86) | 2.38 (1.99,2.84) | 2.40 (2.01,2.87) |
| 4 | 25 | 168,698 | 0.15 | 3.15 (2.11,4.72) | 3.09 (2.07,4.63) | 2.98 (1.99,4.46) |
| p for trend | <0.0001 | <0.0001 | <0.0001 | |||
| CV | ||||||
| 0 | 542 | 14,500,895 | 0.04 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| 1 | 662 | 13,925,803 | 0.05 | 1.22 (1.09,1.36) | 1.21 (1.08,1.36) | 1.23 (1.10,1.38) |
| 2 | 378 | 6,023,625 | 0.06 | 1.48 (1.30,1.70) | 1.47 (1.29,1.68) | 1.50 (1.31,1.71) |
| 3 | 159 | 1,368,232 | 0.12 | 2.45 (2.05,2.93) | 2.41 (2.02,2.88) | 2.45 (2.05,2.93) |
| 4 | 27 | 134,019 | 0.20 | 3.69 (2.50,5.44) | 3.59 (2.43,5.29) | 3.42 (2.32,5.05) |
| p for trend | <0.0001 | <0.0001 | <0.0001 | |||
| ARV | ||||||
| 0 | 548 | 15,328,355 | 0.04 | 1 (ref.) | 1(ref.) | 1 (ref.) |
| 1 | 652 | 13,587,492 | 0.05 | 1.20 (1.07,1.35) | 1.21 (1.08,1.36) | 1.23 (1.10,1.38) |
| 2 | 425 | 5,648,100 | 0.08 | 1.65 (1.45,1.88) | 1.68 (1.48,1.91) | 1.72 (1.51,1.95) |
| 3 | 117 | 1,264,835 | 0.09 | 1.74 (1.42,2.13) | 1.78 (1.45,2.18) | 1.80 (1.47,2.21) |
| 4 | 26 | 123,791 | 0.21 | 3.34 (2.25,4.95) | 3.42 (2.30,5.08) | 3.32 (2.23,4.93) |
| p for trend | <0.0001 | <0.0001 | <0.0001 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.K.; Han, K.; Kim, H.-S.; Park, Y.-M.; Kwon, H.-S.; Yoon, K.-H.; Lee, S.-H. Effects of Variability in Blood Pressure, Glucose, and Cholesterol Concentrations, and Body Mass Index on End-Stage Renal Disease in the General Population of Korea. J. Clin. Med. 2019, 8, 755. https://doi.org/10.3390/jcm8050755
Kim MK, Han K, Kim H-S, Park Y-M, Kwon H-S, Yoon K-H, Lee S-H. Effects of Variability in Blood Pressure, Glucose, and Cholesterol Concentrations, and Body Mass Index on End-Stage Renal Disease in the General Population of Korea. Journal of Clinical Medicine. 2019; 8(5):755. https://doi.org/10.3390/jcm8050755
Chicago/Turabian StyleKim, Mee Kyoung, Kyungdo Han, Hun-Sung Kim, Yong-Moon Park, Hyuk-Sang Kwon, Kun-Ho Yoon, and Seung-Hwan Lee. 2019. "Effects of Variability in Blood Pressure, Glucose, and Cholesterol Concentrations, and Body Mass Index on End-Stage Renal Disease in the General Population of Korea" Journal of Clinical Medicine 8, no. 5: 755. https://doi.org/10.3390/jcm8050755
APA StyleKim, M. K., Han, K., Kim, H. -S., Park, Y. -M., Kwon, H. -S., Yoon, K. -H., & Lee, S. -H. (2019). Effects of Variability in Blood Pressure, Glucose, and Cholesterol Concentrations, and Body Mass Index on End-Stage Renal Disease in the General Population of Korea. Journal of Clinical Medicine, 8(5), 755. https://doi.org/10.3390/jcm8050755