Remote Ischemic Preconditioning Neither Improves Survival nor Reduces Myocardial or Kidney Injury in Patients Undergoing Transcatheter Aortic Valve Implantation (TAVI)

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
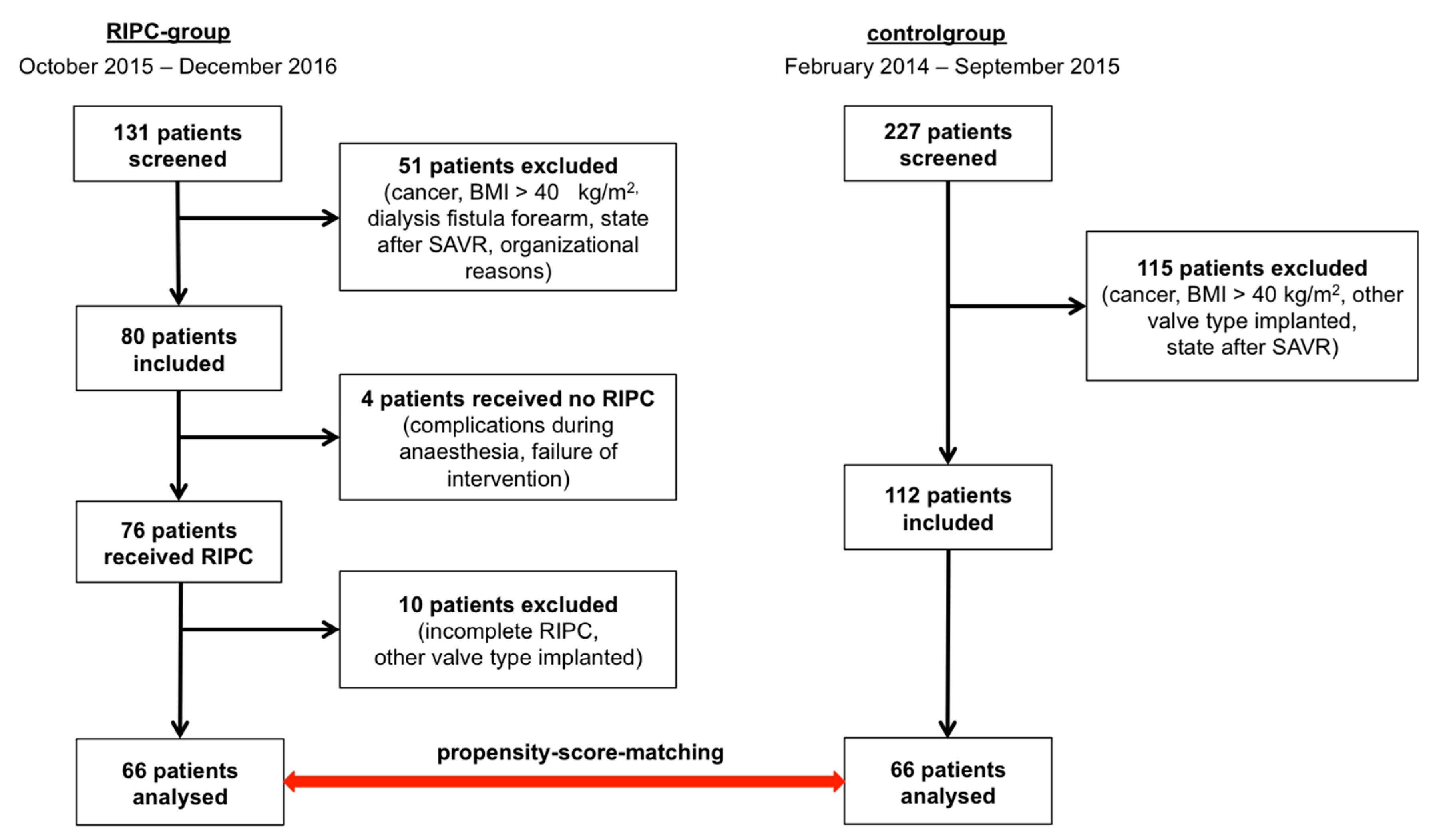
2.1. Study Design and Patient Enrolment
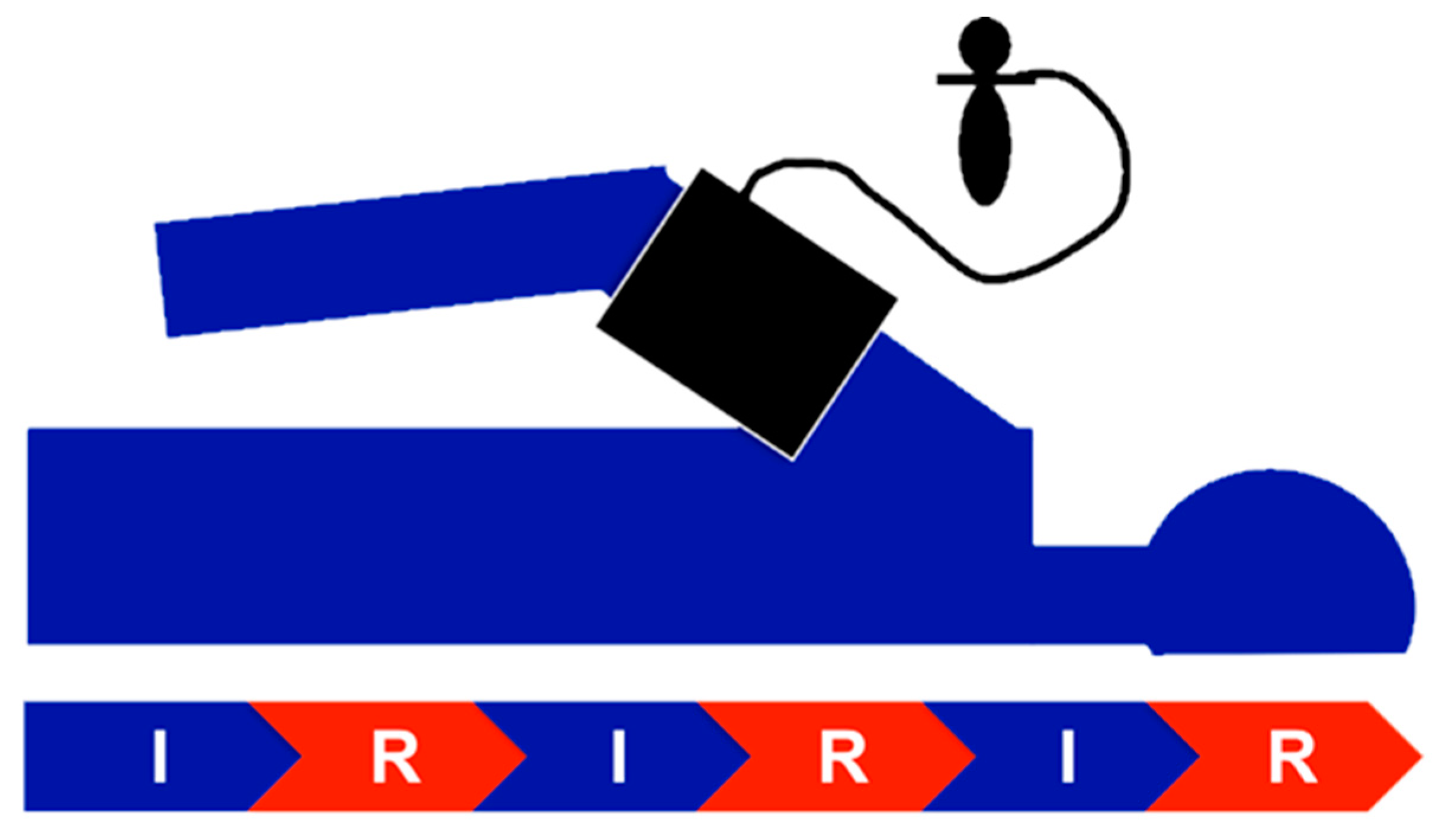
2.2. Procedure—TAVI and RIPC
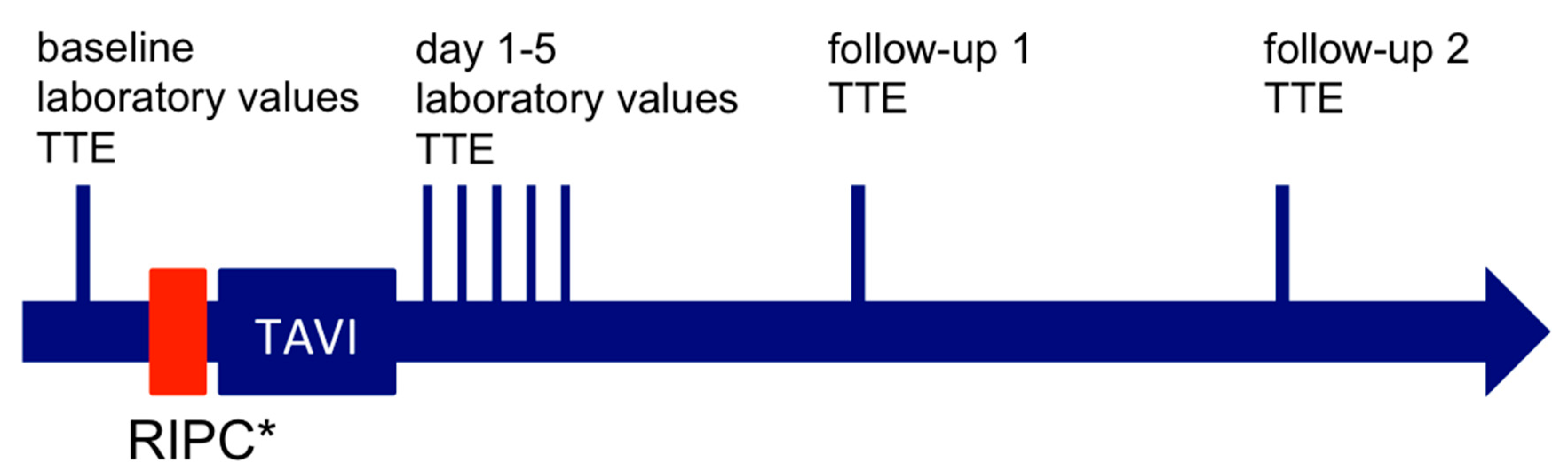
2.3. Blood Sampling and Analysis
2.4. Endpoints
2.5. Statistical Analyses
3. Results
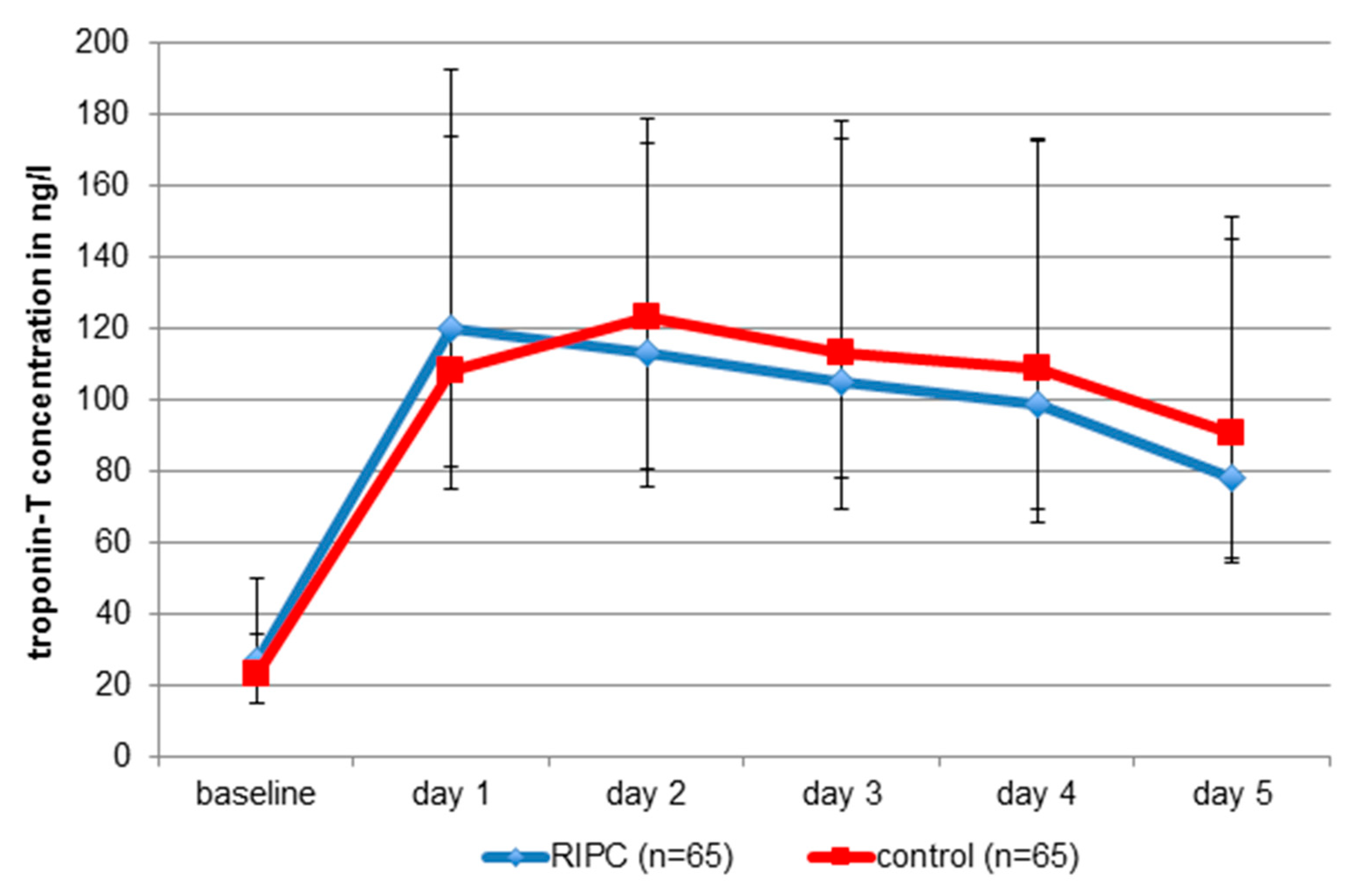
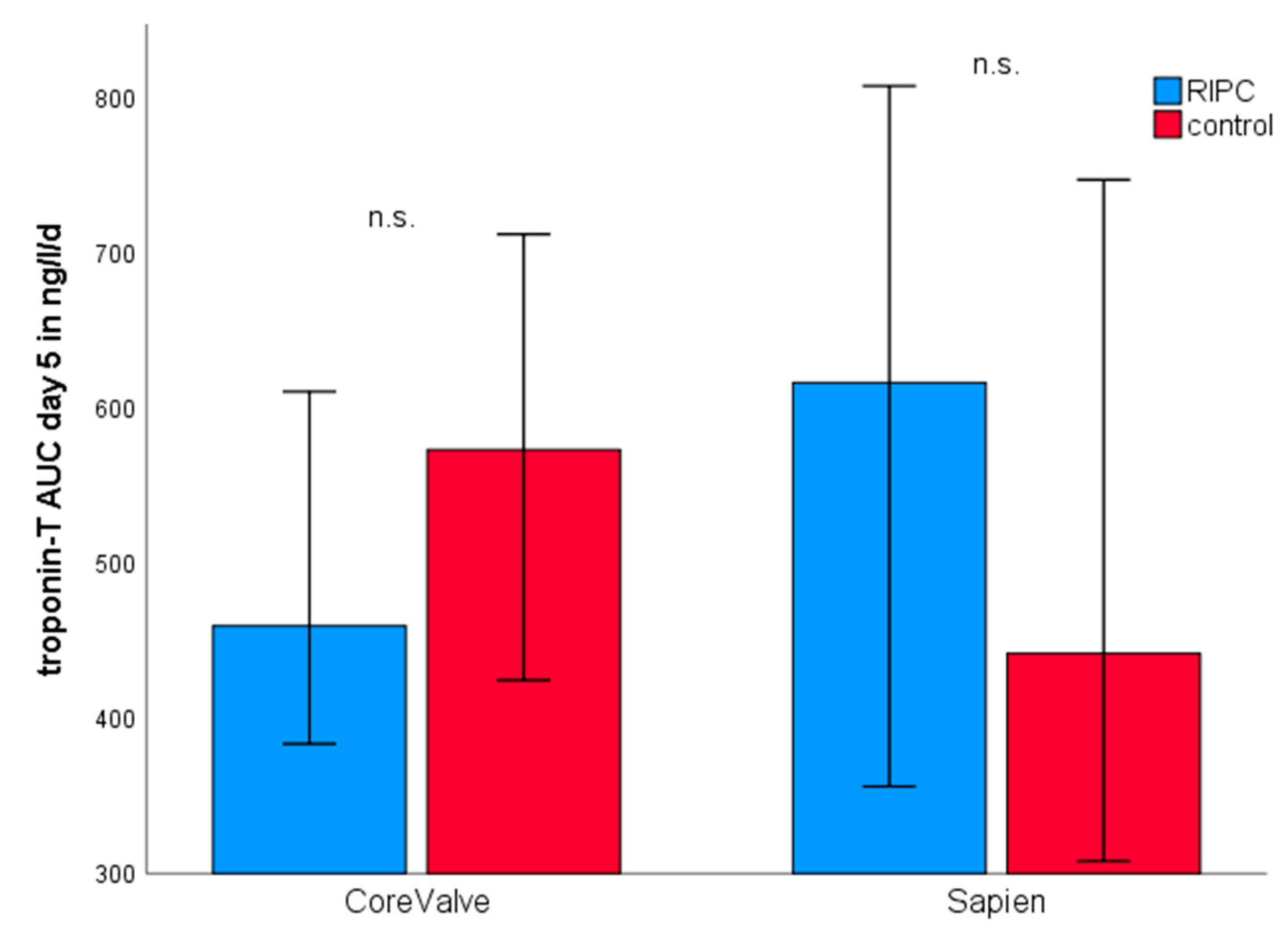
3.1. Myocardial Injury
3.2. Kidney Injury
3.3. Echocardiography
3.4. Mortality
3.5. Complications According to VARC-2
4. Discussion
4.1. Baseline Characteristics
4.2. Type of Bioprosthesis
4.3. Mortality and Myocardial Injury
4.4. Renoprotection by RIPC
4.5. Pharmacological Confounding Factors
4.6. Best Practice of RIPC
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Przyklenk, K.; Darling, C.E.; Dickson, E.W.; Whittaker, P. Cardioprotection ‘outside the box’—the evolving paradigm of remote preconditioning. Basic Res. Cardiol. 2003, 98, 149–157. [Google Scholar] [CrossRef]
- Botker, H.E.; Kharbanda, R.; Schmidt, M.R.; Bottcher, M.; Kaltoft, A.K.; Terkelsen, C.J.; Munk, K.; Andersen, N.H.; Hansen, T.M.; Trautner, S.; et al. Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: A randomised trial. Lancet 2010, 375, 727–734. [Google Scholar] [CrossRef]
- Eitel, I.; Stiermaier, T.; Rommel, K.P.; Fuernau, G.; Sandri, M.; Mangner, N.; Linke, A.; Erbs, S.; Lurz, P.; Boudriot, E.; et al. Cardioprotection by combined intrahospital remote ischaemic perconditioning and postconditioning in ST-elevation myocardial infarction: The randomized LIPSIA CONDITIONING trial. Eur. Heart J. 2015, 36, 3049–3057. [Google Scholar] [CrossRef]
- Sloth, A.D.; Schmidt, M.R.; Munk, K.; Kharbanda, R.K.; Redington, A.N.; Schmidt, M.; Pedersen, L.; Sorensen, H.T.; Botker, H.E.; Investigators, C. Improved long-term clinical outcomes in patients with ST-elevation myocardial infarction undergoing remote ischaemic conditioning as an adjunct to primary percutaneous coronary intervention. Eur. Heart J. 2014, 35, 168–175. [Google Scholar] [CrossRef] [Green Version]
- Thielmann, M.; Kottenberg, E.; Kleinbongard, P.; Wendt, D.; Gedik, N.; Pasa, S.; Price, V.; Tsagakis, K.; Neuhauser, M.; Peters, J.; et al. Cardioprotective and prognostic effects of remote ischaemic preconditioning in patients undergoing coronary artery bypass surgery: A single-centre randomised, double-blind, controlled trial. Lancet 2013, 382, 597–604. [Google Scholar] [CrossRef]
- Candilio, L.; Malik, A.; Ariti, C.; Barnard, M.; Di Salvo, C.; Lawrence, D.; Hayward, M.; Yap, J.; Roberts, N.; Sheikh, A.; et al. Effect of remote ischaemic preconditioning on clinical outcomes in patients undergoing cardiac bypass surgery: A randomised controlled clinical trial. Heart 2015, 101, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Hausenloy, D.J.; Candilio, L.; Yellon, D.M. Remote Ischemic Preconditioning and Cardiac Surgery. N. Engl. J. Med. 2016, 374, 491–492. [Google Scholar] [CrossRef] [PubMed]
- Meybohm, P.; Bein, B.; Brosteanu, O.; Cremer, J.; Gruenewald, M.; Stoppe, C.; Coburn, M.; Schaelte, G.; Boning, A.; Niemann, B.; et al. A Multicenter Trial of Remote Ischemic Preconditioning for Heart Surgery. N. Engl. J. Med. 2015, 373, 1397–1407. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B. Transcatheter Aortic-Valve Replacement in Low-Risk Patients. Reply. N. Engl. J. Med. 2019, 381, 684–685. [Google Scholar]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [Green Version]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Genereux, P.; Head, S.J.; Van Mieghem, N.M.; Kodali, S.; Kirtane, A.J.; Xu, K.; Smith, C.; Serruys, P.W.; Kappetein, A.P.; Leon, M.B. Clinical outcomes after transcatheter aortic valve replacement using valve academic research consortium definitions: A weighted meta-analysis of 3,519 patients from 16 studies. J. Am. Coll. Cardiol. 2012, 59, 2317–2326. [Google Scholar] [CrossRef] [Green Version]
- Koskinas, K.C.; Stortecky, S.; Franzone, A.; O’Sullivan, C.J.; Praz, F.; Zuk, K.; Raber, L.; Pilgrim, T.; Moschovitis, A.; Fiedler, G.M.; et al. Post-Procedural Troponin Elevation and Clinical Outcomes Following Transcatheter Aortic Valve Implantation. J. Am. Heart Assoc. 2016, 5, e002430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, H.B.; Larose, E.; de la Paz Ricapito, M.; Le Ven, F.; Nombela-Franco, L.; Urena, M.; Allende, R.; Amat-Santos, I.; Dahou, A.; Capoulade, R.; et al. Myocardial injury following transcatheter aortic valve implantation: Insights from delayed-enhancement cardiovascular magnetic resonance. EuroIntervention 2015, 11, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahlert, P.; Hildebrandt, H.A.; Patsalis, P.C.; Al-Rashid, F.; Janosi, R.A.; Nensa, F.; Schlosser, T.W.; Schlamann, M.; Wendt, D.; Thielmann, M.; et al. No protection of heart, kidneys and brain by remote ischemic preconditioning before transfemoral transcatheter aortic valve implantation: Interim-analysis of a randomized single-blinded, placebo-controlled, single-center trial. Int. J. Cardiol. 2017, 231, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Baumgartner, H. Updated 2017 European and American guidelines for prosthesis type and implantation mode in severe aortic stenosis. Heart 2018, 104, 710–713. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Genereux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. EuroIntervention 2012, 8, 782–795. [Google Scholar] [CrossRef] [Green Version]
- Rodes-Cabau, J.; Gutierrez, M.; Bagur, R.; De Larochelliere, R.; Doyle, D.; Cote, M.; Villeneuve, J.; Bertrand, O.F.; Larose, E.; Manazzoni, J.; et al. Incidence, predictive factors, and prognostic value of myocardial injury following uncomplicated transcatheter aortic valve implantation. J. Am. Coll. Cardiol. 2011, 57, 1988–1999. [Google Scholar] [CrossRef] [Green Version]
- Ho, D.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 28. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]
- Walther, T.; Hamm, C.W.; Schuler, G.; Berkowitsch, A.; Kotting, J.; Mangner, N.; Mudra, H.; Beckmann, A.; Cremer, J.; Welz, A.; et al. Perioperative Results and Complications in 15,964 Transcatheter Aortic Valve Replacements: Prospective Data from the GARY Registry. J. Am. Coll. Cardiol. 2015, 65, 2173–2180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noorani, A.; Bapat, V. Differences in Outcomes and Indications between Sapien and CoreValve Transcatheter Aortic Valve Implantation Prostheses. Interv. Cardiol. 2014, 9, 121–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chorianopoulos, E.; Krumsdorf, U.; Geis, N.; Pleger, S.T.; Giannitsis, E.; Katus, H.A.; Bekeredjian, R. Preserved prognostic value of preinterventional troponin T levels despite successful TAVI in patients with severe aortic stenosis. Clin. Res. Cardiol. 2014, 103, 65–72. [Google Scholar] [CrossRef]
- Domanski, M.J.; Mahaffey, K.; Hasselblad, V.; Brener, S.J.; Smith, P.K.; Hillis, G.; Engoren, M.; Alexander, J.H.; Levy, J.H.; Chaitman, B.R.; et al. Association of myocardial enzyme elevation and survival following coronary artery bypass graft surgery. JAMA 2011, 305, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Eigel, P.; van Ingen, G.; Wagenpfeil, S. Predictive value of perioperative cardiac troponin I for adverse outcome in coronary artery bypass surgery. Eur. J. Cardiothorac. Surg. 2001, 20, 544–549. [Google Scholar] [CrossRef] [Green Version]
- Kathiresan, S.; Servoss, S.J.; Newell, J.B.; Trani, D.; MacGillivray, T.E.; Lewandrowski, K.; Lee-Lewandrowski, E.; Januzzi, J.L., Jr. Cardiac troponin T elevation after coronary artery bypass grafting is associated with increased one-year mortality. Am. J. Cardiol. 2004, 94, 879–881. [Google Scholar] [CrossRef]
- Carrabba, N.; Valenti, R.; Migliorini, A.; Vergara, R.; Parodi, G.; Antoniucci, D. Prognostic value of myocardial injury following transcatheter aortic valve implantation. Am. J. Cardiol. 2013, 111, 1475–1481. [Google Scholar] [CrossRef]
- Zahn, R.; Werner, N.; Gerckens, U.; Linke, A.; Sievert, H.; Kahlert, P.; Hambrecht, R.; Sack, S.; Abdel-Wahab, M.; Hoffmann, E.; et al. Five-year follow-up after transcatheter aortic valve implantation for symptomatic aortic stenosis. Heart 2017, 103, 1970–1976. [Google Scholar] [CrossRef]
- Hausenloy, D.J.; Candilio, L.; Evans, R.; Ariti, C.; Jenkins, D.P.; Kolvekar, S.; Knight, R.; Kunst, G.; Laing, C.; Nicholas, J.; et al. Remote Ischemic Preconditioning and Outcomes of Cardiac Surgery. N. Engl. J. Med. 2015, 373, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Heusch, G.; Gersh, B.J. ERICCA and RIPHeart: Two nails in the coffin for cardioprotection by remote ischemic conditioning? Probably not! Eur. Heart J. 2016, 37, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Callaghan, C.J.; Lim, E.; Ali, A.A.; Nouraei, S.A.; Akthar, A.M.; Boyle, J.R.; Varty, K.; Kharbanda, R.K.; Dutka, D.P.; et al. Remote ischemic preconditioning reduces myocardial and renal injury after elective abdominal aortic aneurysm repair: A randomized controlled trial. Circulation 2007, 116, I98–I105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausenloy, D.J.; Mwamure, P.K.; Venugopal, V.; Harris, J.; Barnard, M.; Grundy, E.; Ashley, E.; Vichare, S.; Di Salvo, C.; Kolvekar, S.; et al. Effect of remote ischaemic preconditioning on myocardial injury in patients undergoing coronary artery bypass graft surgery: A randomised controlled trial. Lancet 2007, 370, 575–579. [Google Scholar] [CrossRef]
- Kharbanda, R.K.; Mortensen, U.M.; White, P.A.; Kristiansen, S.B.; Schmidt, M.R.; Hoschtitzky, J.A.; Vogel, M.; Sorensen, K.; Redington, A.N.; MacAllister, R. Transient limb ischemia induces remote ischemic preconditioning in vivo. Circulation 2002, 106, 2881–2883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murry, C.E.; Jennings, R.B.; Reimer, K.A. Preconditioning with ischemia: A delay of lethal cell injury in ischemic myocardium. Circulation 1986, 74, 1124–1136. [Google Scholar] [CrossRef] [Green Version]
- Przyklenk, K.; Bauer, B.; Ovize, M.; Kloner, R.A.; Whittaker, P. Regional ischemic ‘preconditioning’ protects remote virgin myocardium from subsequent sustained coronary occlusion. Circulation 1993, 87, 893–899. [Google Scholar] [CrossRef] [Green Version]
- Botker, H.E.; Lassen, T.R.; Jespersen, N.R. Clinical translation of myocardial conditioning. Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H1225–H1252. [Google Scholar] [CrossRef]
- Vinten-Johansen, J.; Shi, W. Perconditioning and postconditioning: Current knowledge, knowledge gaps, barriers to adoption, and future directions. J. Cardiovasc. Pharm. 2011, 16, 260–266. [Google Scholar] [CrossRef]
- Zhu, S.B.; Liu, Y.; Zhu, Y.; Yin, G.L.; Wang, R.P.; Zhang, Y.; Zhu, J.; Jiang, W. Remote preconditioning, perconditioning, and postconditioning: A comparative study of their cardio-protective properties in rat models. Clinics (Sao Paulo) 2013, 68, 263–268. [Google Scholar] [CrossRef]
- Kim, T.K.; Min, J.J.; Cho, Y.J.; Hausenloy, D.J.; Ahn, H.; Kim, K.H.; Hwang, H.Y.; Hong, D.M.; Jeon, Y. Effects of delayed remote ischemic preconditioning on peri-operative myocardial injury in patients undergoing cardiac surgery - A randomized controlled trial. Int. J. Cardiol. 2017, 227, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Przyklenk, K. Reduction of myocardial infarct size with ischemic “conditioning”: Physiologic and technical considerations. Anesth. Analg. 2013, 117, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, J.; Pryds, K.; Salman, R.; Lofgren, B.; Kristiansen, S.B.; Botker, H.E. The remote ischemic preconditioning algorithm: Effect of number of cycles, cycle duration and effector organ mass on efficacy of protection. Basic Res. Cardiol. 2016, 111, 10. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, R.M.; Mohamed el, H.A.; Ashraf, M.; Maithili, S.; Nabil, F.; Rami, R.; Mohamed, T.I. Effect of remote ischemic preconditioning on serum troponin T level following elective percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2013, 82, E647–E653. [Google Scholar] [CrossRef]
- Austin, P.C. Comparing paired vs. non-paired statistical methods of analyses when making inferences about absolute risk reductions in propensity-score matched samples. Stat. Med. 2011, 30, 1292–1301. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RIPC-Group (n = 66) | Control-Group (n = 66) | p-Value | |
|---|---|---|---|
| Age (years) | 82.2 (4.4) | 82.2 (5.6) | 0.960 |
| Gender | |||
| female | 32 (48.5) | 31 (47.0) | 1.000 |
| male | 34 (51.5) | 35 (53.0) | |
| BMI (kg/m2) | 28.2 (25.5–31.2) | 27.6 (23.8–30.9) | 0.171 |
| Body-height (m) | 1.77 (0.09) | 1.65 (0.09) | 0.727 |
| Body-weight (kg) | 80 (69–89) | 75 (65–86) | 0.137 |
| LV-EF (%) | 55 (48–60) | 55 (45–60) | 0.568 |
| Aortic stenosis | |||
| Vmax (cm/sec) | 403.6 (94.3) (n = 53) | 417.6 (79.4) (n = 59) | 0.572 |
| dpmax (mmHg) | 72.0 (48.0–85.0) (n = 63) | 67.0 (53.5–88.5) (n = 62) | 0.907 |
| dpmean (mmHg) | 40.0 (28.0–51.0) (n = 63) | 40.0 (31.3–53.8) (n = 60) | 0.728 |
| CAD (stenosis > 50%) | 33 (50) | 30 (46) | 0.701 |
| PCI/CABG prior TAVI | 26 (39) | 24 (36) | 0.860 |
| Diabetes mellitus | 26 (39) | 27 (41) | 1.000 |
| insulin dependent | 11 (17) | 11 (17) | 1.000 |
| Prior medication | |||
| ACE-Inhibitor/AT1-Blocker | 50 (76) | 42 (64) | 0.215 |
| ß-Blocker | 54 (82) | 50 (76) | 0.541 |
| MRA | 6 (9) | 6 (9) | 1.000 |
| Statins | 53 (80) | 53 (80) | 1.000 |
| Anti-platelets | 56 (85) | 54 (82) | 0.842 |
| Heart rhythm | |||
| Atrial flutter/fibrillation | 29 (44) | 26 (39) | 0.720 |
| AV-Block (I-III) | 14 (21) | 9 (14) | 0.359 |
| branch block | 25 (38) | 17 (26) | 0.200 |
| permanent pacemaker | 12 (18) | 12 (18) | 1.000 |
| Euro-II-Score | 4.6 (2.9–7.6) | 4.0 (2.7–7.2) | 0.728 |
| Valvetyp | |||
| Medtronic CoreValve | 44 (67) | 44 (67) | 1.000 |
| Edwards Sapien XT/3 | 22 (33) | 22 (33) | |
| Prothesis size | 29 (26–29) | 26 (26–29) | 0.871 |
| 23 mm | 4 (6) | 2 (3) | |
| 26 mm | 29 (44) | 32 (49) | |
| 29 mm | 31 (47) | 29 (44) | |
| 31 mm | 2 (3) | 3 (5) | |
| n-dilations | 2 (1–2) | 2 (1–2) | 1.000 |
| 1 | 18 (27) | 16 (24) | |
| 2 | 40 (61) | 43 (65) | |
| 3 | 6 (9) | 7 (11) | |
| 4 | 2 (3) | 0 (0) | |
| n-pacing runs | 2 (2–3) | 2 (2–3) | 0.986 |
| 1 | 40 (61) | 35 (53) | |
| 2 | 18 (27) | 25 (38) | |
| 3 | 6 (9) | 6 (9) | |
| 4 | 2 (3) | 0 (0) | |
| Procedure duration (min) | 54 (41–71) | 52 (42–-65) | 0.293 |
| Contrast medium (ml) | 130 (120–150) | 130 (100–153) | 0.227 |
| Blood analysis prior TAVI | |||
| hsTnT (ng/l) | 27.0 (14.8–34.3) | 23.0 (15.0–51.2) | 0.319 |
| Creatinine (µmol/l) | 101 (79–134) | 98 (81–116) | 0.674 |
| GFR (ml/min/KO) | 54 (18) | 56 (17) | 0.473 |
| Urea (mmol/l) | 7.1 (5.6–10.8) | 7.1 (5.6–9.6) | 0.573 |
| Leukocyts (Gpt/l) | 7.1 (6.2–8.2) | 7.0 (6.2–8.0) | 0.928 |
| CRP (mg/l) | 3.5 (1.2–7.2) | 3.1 (1.5–7.1) | 0.682 |
| PCT (µg/l) | 0.05 (0.05–0.08) (n = 46) | 0.05 (0.05–0.07) (n = 45) | 0.554 |
| Interleukin-6 (pg/mL) | 5.8 (4.0–8.3) (n = 48) | 6.6 (4.5–9.4) (n = 34) | 0.803 |
| NTproBNP (ng/l) | 2082 (1463–3372) (n = 50) | 1948 (1205–4287) (n = 37) | 0.679 |
| RIPC-Group (n = 66) | control-Group (n = 66) | p-Value | |
|---|---|---|---|
| Death (from any cause) | 7 (11) | 9 (14) | 0.559 |
| Stroke/TIA | 2 (3) | 0 (0) | 0.500 |
| disabling | 2 (3) | 0 (0) | 0.500 |
| non-disabling | 0 (0) | 0 (0) | 1.000 |
| ppMI | 0 (0) | 0 (0) | 1.000 |
| Valve-embolisation | 3 (5) | 0 (0) | 0.250 |
| Conversion to surgery | 2 (3) | 0 (0) | 0.500 |
| Vascular complications | 6 (9) | 4 (6) | 0.727 |
| Major-bleeding complications | 5 (8) | 8 (12) | 0.581 |
| New arrhythmia | |||
| Atrial flutter/fibrillation | 6 (9) | 5 (8) | 1.000 |
| AV-Block I-III | 19 (29) | 16 (24) | 0.711 |
| Branch block | 20 (30) | 20 (30) | 1.000 |
| New pacemaker | 23 (34) | 20 (30) | 0.690 |
| RIPC-Group (n = 66) | Control-Group (n = 66) | p-Value | |
|---|---|---|---|
| Creatinine-peak (µmol/L) | 99 (77–127) | 97 (80–119) | 0.684 |
| Creatinine AUC d5 (µmol/L/d) | 442 (351–552) | 434 (356–528) | 0.752 |
| GFR decrease | 31 (47) | 31 (47) | 1.000 |
| AKIN | 1 (1.5) | 4 (6) | 0.250 |
| 1 | 1 (1.5) | 2 (3) | |
| 2 | 0 (0) | 0 (0) | |
| 3 | 0 (0) | 2 (3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flechsig, M.; Ruf, T.F.; Troeger, W.; Wiedemann, S.; Quick, S.; Ibrahim, K.; Pfluecke, C.; Youssef, A.; Sveric, K.M.; Winzer, R.; et al. Remote Ischemic Preconditioning Neither Improves Survival nor Reduces Myocardial or Kidney Injury in Patients Undergoing Transcatheter Aortic Valve Implantation (TAVI). J. Clin. Med. 2020, 9, 160. https://doi.org/10.3390/jcm9010160
Flechsig M, Ruf TF, Troeger W, Wiedemann S, Quick S, Ibrahim K, Pfluecke C, Youssef A, Sveric KM, Winzer R, et al. Remote Ischemic Preconditioning Neither Improves Survival nor Reduces Myocardial or Kidney Injury in Patients Undergoing Transcatheter Aortic Valve Implantation (TAVI). Journal of Clinical Medicine. 2020; 9(1):160. https://doi.org/10.3390/jcm9010160
Chicago/Turabian StyleFlechsig, Mandy, Tobias F. Ruf, Willi Troeger, Stephan Wiedemann, Silvio Quick, Karim Ibrahim, Christian Pfluecke, Akram Youssef, Krunoslav M. Sveric, Robert Winzer, and et al. 2020. "Remote Ischemic Preconditioning Neither Improves Survival nor Reduces Myocardial or Kidney Injury in Patients Undergoing Transcatheter Aortic Valve Implantation (TAVI)" Journal of Clinical Medicine 9, no. 1: 160. https://doi.org/10.3390/jcm9010160
APA StyleFlechsig, M., Ruf, T. F., Troeger, W., Wiedemann, S., Quick, S., Ibrahim, K., Pfluecke, C., Youssef, A., Sveric, K. M., Winzer, R., Heinzel, F. R., Linke, A., Strasser, R. H., Zhang, K., & Heidrich, F. M. (2020). Remote Ischemic Preconditioning Neither Improves Survival nor Reduces Myocardial or Kidney Injury in Patients Undergoing Transcatheter Aortic Valve Implantation (TAVI). Journal of Clinical Medicine, 9(1), 160. https://doi.org/10.3390/jcm9010160