Persistent Inflammation, Immunosuppression and Catabolism Syndrome (PICS) after Polytrauma: A Rare Syndrome with Major Consequences

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
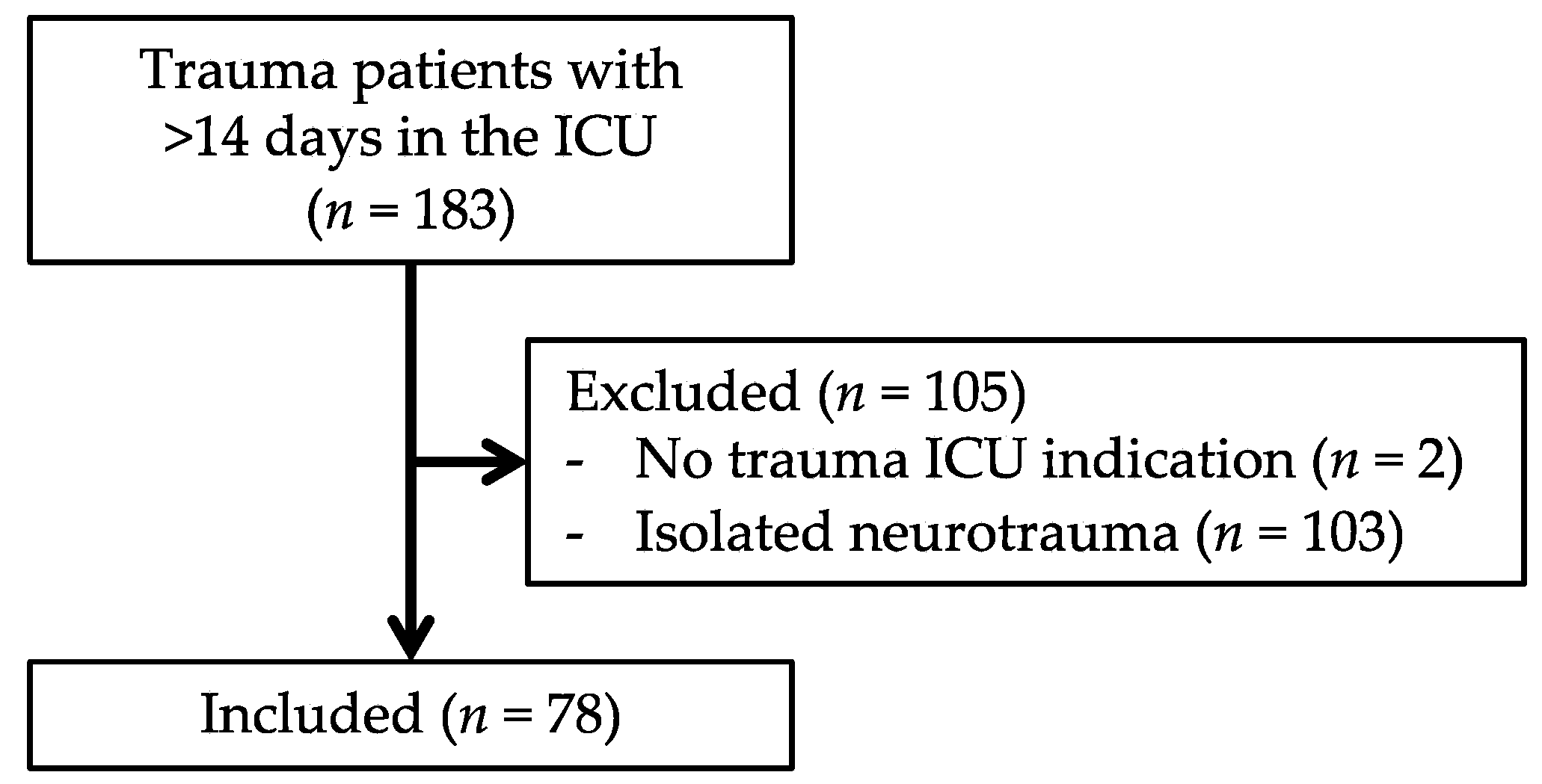
2.2. Patients
2.3. Definitions, Variables and Outcomes
2.4. Statistical Analysis
2.5. Ethics
3. Results
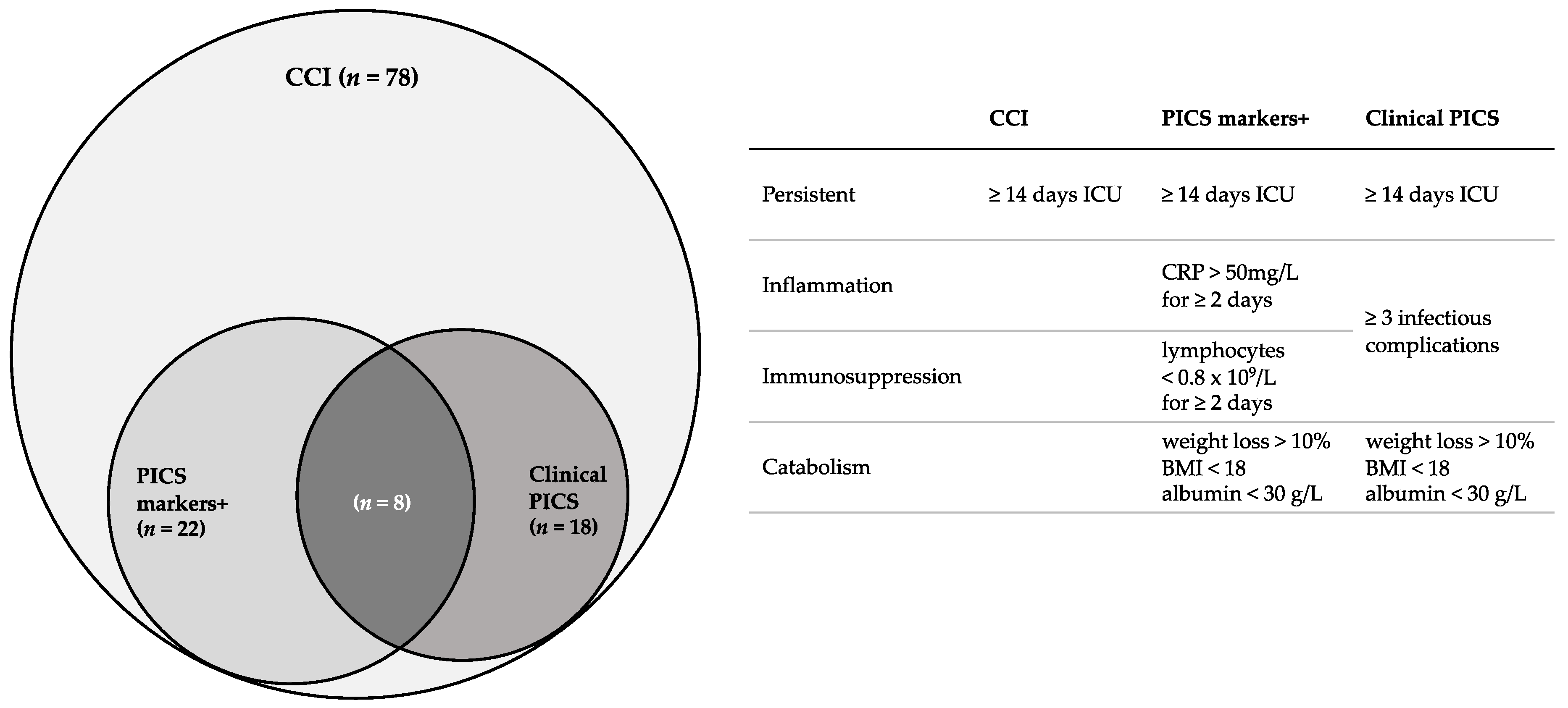
3.1. PICS Incidence
3.2. Clinical PICS Patients vs. Other CCI Patients
3.3. PICS Markers-Positive Group vs. Other CCI Patients
3.4. Testing the Accuracy of PICS Markers
3.4.1. Sensitivity and Specificity
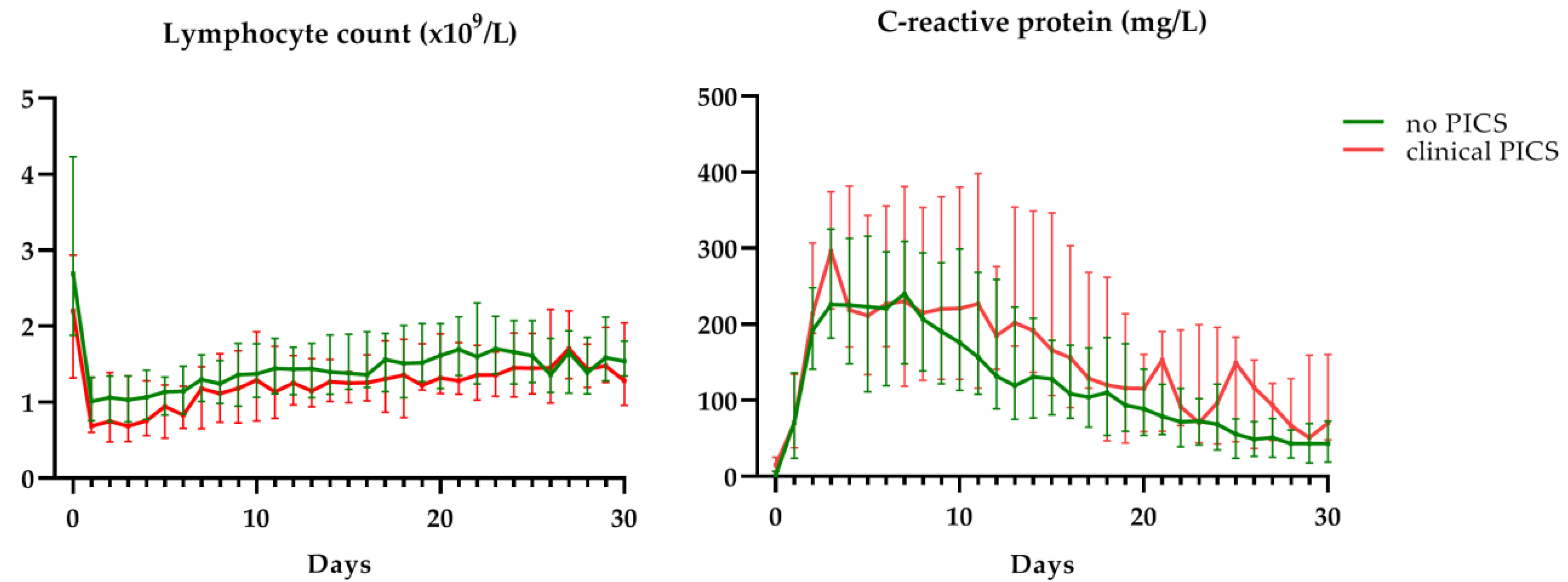
3.4.2. Lymphocytes and CRP
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Jochems, D.; Leenen, L.P.H.; Hietbrink, F.; Houwert, R.M.; van Wessem, K.J.P. Increased reduction in exsanguination rates leaves brain injury as the only major cause of death in blunt trauma. Injury 2018, 49, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- van Wessem, K.J.P.; Leenen, L.P.H. Reduction in Mortality Rates of Postinjury Multiple Organ Dysfunction Syndrome. Shock 2017, 49, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Lyons, T.; Balogh, Z.J.; Evans, J.A.; McDougall, D.; van Wessem, K.J.P.; Lee, K.A. Epidemiology of Traumatic Deaths: Comprehensive Population-Based Assessment. World J. Surg. 2009, 34, 158–163. [Google Scholar]
- Radomski, M.; Zettervall, S.; Schroeder, M.E.; Messing, J.; Dunne, J.; Sarani, B. Critical Care for the Patient With Multiple Trauma. J. Intensive Care Med. 2016, 31, 307–318. [Google Scholar] [CrossRef]
- Gentile, L.F.; Cuenca, A.G.; Vanzant, E.L.; Efron, P.A.; Mckinley, B.; Moore, F.; Moldawer, L.L. Persistent inflammation and immunosuppression: A common sydrome and new horizon for surgical intensive care. J. Trauma Acute Care Surg. 2012, 72, 1491–1501. [Google Scholar] [CrossRef] [Green Version]
- Lansink, K.W.W.; Gunning, A.C.; Leenen, L.P.H. Cause of death and time of death distribution of trauma patients in a Level I trauma centre in the Netherlands. Eur. J. Trauma Emerg. Surg. 2013, 39, 375–383. [Google Scholar] [CrossRef]
- Mira, J.C.; Brakenridge, S.C.; Moldawer, L.L.; Moore, F.A. Persistent Inflammation, Immunosuppression and Catabolism Syndrome (PICS). Crit. Care Clin. 2017, 33, 245–258. [Google Scholar] [CrossRef]
- Mira, J.C.; Cuschieri, J.; Ozrazgat-Baslanti, T.; Wang, Z.; Ghita, G.L.; Loftus, T.J.; Stortz, J.A.; Raymond, S.L.; Lanz, J.D.; Hennessy, L.V.; et al. The epidemiology of chronic critical illness after severe traumatic injury at two level-one trauma centers. Crit. Care Med. 2017, 45, 1989–1996. [Google Scholar] [CrossRef]
- Stortz, J.A.; Murphy, T.J.; Raymond, S.L.; Mira, J.C.; Ungaro, R.; Dirain, M.L.; Nacionales, D.C.; Loftus, T.J.; Wang, Z.; Ozrazgat-Baslanti, T.; et al. Evidence for persistent immune suppression in patients who develop chronic critical illness after sepsis. Shock 2018, 49, 249–258. [Google Scholar] [CrossRef]
- Nelson, J.E.; Cox, C.E.; Hope, A.A.; Carson, S.S. Concise Clinical Review: Chronic Critical Illness. Am. J. Respir. Crit. Care Med. 2010, 182, 1–9. [Google Scholar] [CrossRef]
- Carson, S.S. Definitions and epidemiology of the chronically critically ill. Respir. Care 2012, 57, 848–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, A.K.; Ghita, G.L.; Wang, Z.; Ozrazgat-Baslanti, T.; Raymond, S.L.; Mankowski, R.T.; Brumback, B.A.; Efron, P.A.; Bihorac, A.; Moore, F.A.; et al. The Development of Chronic Critical Illness Determines Physical Function, Quality of Life, and Long-Term Survival Among Early Survivors of Sepsis in Surgical ICUs. Crit. Care Med. 2019, 47, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, M.D.; Moore, F.A. Persistent inflammatory, immunosuppressed, catabolic syndrome (PICS): A new phenotype of multiple organ failure. J. Adv. Nutr. Hum. Metab. 2015, 1, 1–16. [Google Scholar]
- Loftus, T.J.; Moore, F.A.; Moldawer, L.L. ICU-Acquired Weakness, Chronic Critical Illness, and the Persistent Inflammation-Immunosuppression and Catabolism Syndrome. Crit. Care Med. 2017, 45, e1184. [Google Scholar] [CrossRef] [PubMed]
- Rawal, G.; Yadav, S.; Kumar, R. Post-intensive care syndrome: An overview. J. Transl. Intern. Med. 2017, 5, 90–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanzant, E.L.; Lopez, C.M.; Ozrazgat-baslanti, T.; Davis, R.; Cuenca, A.G.; Gentile, L.F.; Dina, C.; Cuenca, A.L.; Bihorac, A.; Leeuwenburgh, C.; et al. Persistent Inflammation, Immunosuppression and Catabolism Syndrome after Severe Blunt Trauma. J. Trauma Acute Care Surg. 2014, 76, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Gennarelli, T.A.; Wodzin, E. AIS 2005: A contemporary injury scale. Injury 2006, 37, 1083–1091. [Google Scholar] [CrossRef]
- ten Berg, M.J.; Huisman, A.; Van den Bemt, P.M.L.A.; Schobben, A.F.A.M.; Egberts, A.C.G.; van Solinge, W.W. Linking laboratory and medication data: New opportunities for pharmacoepidemiological research. Clin. Chem. Lab. Med. 2007, 45, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschmann, C.S.; Seymour, C.W.; Shanka-hari, M.; Annane, D.; Bauer, M. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Baker, S.P.; O’Neill, B.; Haddon, W.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Plate, J.D.J.; Peelen, L.M.; Leenen, L.P.H.; Hietbrink, F. The intermediate care unit as a cost-reducing critical care facility in tertiary referral hospitals: A single-centre observational study. BMJ Open 2019, 9, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Eurostat Hospital Discharges and Length of Stay Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Hospital_discharges_and_length_of_stay_statistics (accessed on 10 August 2019).
- Lansink, K.W.W.; Gunning, A.C.; Spijkers, A.T.E.; Leenen, L.P.H. Evaluation of Trauma Care in a Mature Level I Trauma Center in The Netherlands: Outcomes in a Dutch Mature Level I Trauma. World J. Surg. 2013, 37, 2353–2359. [Google Scholar] [CrossRef]
- Childers, C.P.; Maggard-Gibbons, M. Understanding costs of care in the operating room. JAMA Surg. 2018, 153, e176233. [Google Scholar] [CrossRef] [PubMed]
- Murthy, S.; Wunsch, H. Clinical review: International comparisons in critical care-lessons learned. Crit. Care 2012, 16, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wunsch, H.; Angus, D.C.; Harrison, D.A.; Collange, O.; Fowler, R.; Hoste, E.A.J.; De Keizer, N.F.; Kersten, A.; Linde-Zwirble, W.T.; Sandiumenge, A.; et al. Variation in critical care services across North America and Western Europe. Crit. Care Med. 2008, 36, 2787–2793. [Google Scholar] [CrossRef] [PubMed]
- You, J.W.; Lee, S.J.; Kim, Y.E.; Cho, Y.J.; Jeong, Y.Y.; Kim, H.C.; Lee, J.D.; Kim, J.R.; Hwang, Y.S. Association between weight change and clinical outcomes in critically ill patients. J. Crit. Care 2013, 28, 923–927. [Google Scholar] [CrossRef]
- Bharadwaj, S.; Ginoya, S.; Tandon, P.; Gohel, T.D.; Guirguis, J.; Vallabh, H.; Jevenn, A.; Hanouneh, I. Malnutrition: Laboratory markers vs nutritional assessment. Gastroenterol. Rep. 2016, 4, 272–280. [Google Scholar] [CrossRef] [Green Version]
- Alpers, D.H.; Stenson, W.F.; Taylore, B.E.; Bier, D.M. Manual of nutritional therapeutics. In Manual of Nutrional Therapeutics; LWW: Philadelphia, UK, 2008; pp. 104–105. [Google Scholar]
- Gosling, P.; Dickson, G.R. Serum c-reactive protein in patients with serious trauma. Injury 1992, 23, 483–486. [Google Scholar] [CrossRef]
- Simon, L.; Gauvin, F.; Amre, D.; Saint-Louis, P. Serum Procalcitonin and C-Reactive Protein Levels as Markers of Bacterial Infection: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2014, 39, 206–217. [Google Scholar] [CrossRef] [Green Version]
- Santonocito, C.; De Loecker, I.; Donadello, K.; Moussa, M.D.; Markowicz, S.; Gullo, A.; Vincent, J.L. C-reactive protein kinetics after major surgery. Anesth. Analg. 2014, 119, 624–629. [Google Scholar] [CrossRef]
- Sabino, H.; Moreira, P.; Mealha, R.; Fernandes, A.; Coelho, L.; Almeida, E.; Póvoa, P. C-reactive protein as a marker of infection in critically ill patients. Clin. Microbiol. Infect. 2005, 11, 101–108. [Google Scholar]
- Huber-Lang, M.; Lambris, J.D.; Ward, P.A. Innate immune responses to trauma. Nat. Immunol. 2018, 19, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, D.S.; Monaghan, S.F.; Cioffi, W.G.; Machan, J.T.; Thakkar, R.K.; Ayala, A. Failure to normalize lymphopenia following trauma is associated with increased mortality, independent of the leukocytosis pattern. Crit. Care 2012, 16, R12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hesselink, L.; Spijkerman, R.; Van Wessem, K.J.P.; Koenderman, L.; Leenen, L.P.H.; Huber-lang, M.; Hietbrink, F. Neutrophil heterogeneity and its role in infectious complications after severe trauma. World J. Emerg. Surg. 2019, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Spijkerman, R.; Hesselink, L.; Hellebrekers, P.; Vrisekoop, N.; Hietbrink, F.; Leenen, L.P.H.; Koenderman, L. Automated flow cytometry enables high performance point-of-care analysis of leukocyte phenotypes. J. Immunol. Methods 2019, 474, 112646. [Google Scholar] [CrossRef]
- Pape, H.C. Effects of changing strategies of fracture fixation on immunologic changes and systemic complications after multiple trauma: Damage control orthopedic surgery. J. Orthop. Res. 2008, 26, 1478–1484. [Google Scholar] [CrossRef]
- Lamb, C.M.; Macgoey, P.; Navarro, A.P.; Brooks, A.J. Damage control surgery in the era of damage control resuscitation. Br. J. Anaesth. 2014, 113, 242–249. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, D.; Jacobs, D.; Kudsk, K.; Moore, F.; Oswanski, M.; Poole, G.; Sacks, G.; Scherer, L., 3rd; Sinclair, K.; EAST Practice Management Guidelines Work Group. Practice management guidelines for nutritional support of the trauma patient. J. Trauma Acute Care Surg. 2004, 57, 660–679. [Google Scholar] [CrossRef] [Green Version]
- de Smet, A.; Kluytmans, J.; Cooper, B.S.; Mascini, E.M.; Van Der Werf, T.S.; Van Der Hoeven, J.G.; Pickkers, P.; Bernards, A.T.; Kuijper, E.J.; Hall, M.A.L.; et al. Decontamination of the Digestive Tract and Oropharynx in ICU Patients. N. Engl. J. Med. 2009, 360, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Oostdijk, E.A.N.; Kesecioglu, J.; Schultz, M.J.; Visser, C.E.; De Jonge, E.; Van Essen, E.H.R.; Bernards, A.T.; Purmer, I.; Brimicombe, R.; Bergmans, D.; et al. Effects of decontamination of the oropharynx and intestinal tract on antibiotic resistance in icus a randomized clinical trial. JAMA J. Am. Med. Assoc. 2014, 312, 1429–1437. [Google Scholar] [CrossRef] [Green Version]
- Rosenthal, M.D.; Moore, F.A. Persistent Inflammation, Immunosuppression, and Catabolism: Evolution of Multiple Organ Dysfunction. Surg. Infect. 2016, 17, 167–172. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Entire Cohort (n = 78) | No PICS (n = 60) | Clinical PICS (n = 18) | p-Value |
|---|---|---|---|---|
| Gender, male (%) | 63 (80.8%) | 48 (80.0%) | 15 (83.3%) | 0.999 |
| Age | 49 (32–65) | 46 (28–62) | 57 (45–68) | 0.086 |
| Injury severity score | 34 (26–42) | 34 (27–41) | 29 (22–48) | 0.548 |
| Injury mechanism | 0.261 | |||
| Traffic accident | 51 (65.4%) | 39 (65.0%) | 12 (66.7%) | |
| Fall from height | 18 (23.1%) | 15 (25.0%) | 3 (16.7%) | |
| Crush injury | 4 (5.1%) | 2 (3.3%) | 2 (11.1%) | |
| Other | 5 (6.4%) | 4 (6.9%) | 1 (5.6%) | |
| Massive transfusion protocol | 32 (41.0%) | 20 (33.3%) | 12 (66.7%) | 0.015 |
| Hospital days | 43 (35–63) | 40 (31–52) | 83 (41–106) | <0.001 |
| ICU days | 20 (16–29) | 19 (16–26) | 30 (19–37) | 0.006 |
| Tracheostomy | 45 (57.7%) | 33 (55.0%) | 12 (66.7%) | 0.427 |
| Mechanical ventilation days | 20 (15–27) | 17 (14–26) | 20 (27–38) | 0.001 |
| Continuous veno-venous hemofiltration | 5 (6.4%) | 2 (3.3%) | 3 (16.7%) | 0.078 |
| Infectious complications | 57 (73.1%) | 39 (65.0%) | 18 (100%) | 0.002 |
| Per patient | 1 (0–2) | 1 (0–1) | 3 (3–3) | <0.001 |
| Sepsis * | 23 (29.5%) | 10 (16.7%) | 13 (72.2%) | <0.001 |
| Type of infections | ||||
| Pneumonia | 40 (51.3%) | 28 (46.7%) | 12 (66.7%) | 0.185 |
| Surgical site infection | 14 (17.9%) | 6 (10.0%) | 8 (44.4%) | 0.002 |
| Blood stream infection | 15 (19.8%) | 6 (10.0%) | 9 (50.0%) | 0.001 |
| Infected OSM | 7 (9.0%) | 1 (1.7%) | 6 (33.3%) | <0.001 |
| UTI | 5 (6.4%) | 4 (6.7%) | 1 (5.6%) | 0.999 |
| Abscess | 4 (5.1%) | 2 (3.3%) | 2 (11.1%) | 0.226 |
| Other | 12 (15.4%) | 5 (8.3%) | 7 (38.9%) | 0.005 |
| Multi-drug resistant organisms | 0.000 | |||
| MRSA | 1 (1.3%) | 0 (0%) | 1 (5.6%) | |
| ESBL | 5 (6.4%) | 3 (5.0%) | 2 (11.1%) | |
| MDR-GNB | 5 (6.4%) | 1 (1.7%) | 4 (22.2%) | |
| Multi-drug resistant Pseudomonas | 2 (2.6%) | 0 (0%) | 2 (11.1%) | |
| Multi-drug resistant Acinobacter | 2 (2.6%) | 1 (1.7%) | 1 (5.6%) | |
| Infectious readmissions | 20 (25.6%) | 8 (13.3%) | 12 (66.7%) | <0.001 |
| Per patient | 0 (0–0) | 0 (0–0) | 1 (0–3) | <0.001 |
| Total infectious complications during or after hospitalization per patient | 1 (0–3) | 1 (0–2) | 6 (3–7) | <0.001 |
| Surgical procedures during hospitalization | 62 (79.5%) | 44 (73.3%) | 18 (100%) | 0.016 |
| Per patient | 3 (1–6) | 2 (0–5) | 8 (3–13) | <0.001 |
| Surgical procedures after discharge | 27 (34.6%) | 16 (22.4%) | 11 (61.1%) | 0.011 |
| Per patient | 2 (0–2) | 0 (0–1) | 3 (0–5) | 0.006 |
| Total surgical procedures during or after hospitalization per patient | 3 (1–7) | 3 (1–5) | 13 (2–22) | 0.003 |
| Discharge | 0.931 | |||
| Other hospital | 8 (10.3%) | 7 (11.7%) | 1 (5.6%) | |
| Nursing home | 11 (14.1%) | 9 (15.0%) | 2 (11.1%) | |
| Rehabilitation facility | 27 (34.6%) | 19 (31.7%) | 8 (44.4%) | |
| Home (+/− additional care) | 27 (34.6%) | 21 (25.0%) | 6 (33.3%) | |
| Total mortality | 13 (16.6%) | 10 (16.6%) | 3 (16.7%) | 1.000 |
| In hospital | 5 (6.4%) | 4 (6.7%) | 1 (5.6%) | 1.000 |
| <3 years | 8 (10.3%) | 6 (10.0%) | 2 (11.1%) | 1.000 |
| Characteristics | Entire Cohort (n = 78) | No PICS Markers (n = 56) | PICS Markers (n = 22) | p-Value |
|---|---|---|---|---|
| Gender, male (%) | 63 (80.8%) | 45 (80.4%) | 18 (81.8%) | 0.999 |
| Age | 49 (32–65) | 49 (33–66) | 40 (27–63) | 0.512 |
| Injury severity score | 34 (26–42) | 34 (29–43) | 29 (20–42) | 0.147 |
| Injury mechanism | 0.702 | |||
| Traffic accident | 51 (65.4%) | 36 (64.2%) | 15 (68.2%) | |
| Fall from height | 18 (23.1%) | 14 (25%) | 4 (18.2%) | |
| Crush injury | 4 (5.1%) | 3 (5.4%) | 1 (4.6%) | |
| Other | 5 (6.4%) | 3 (5.4%) | 2 (9.1%) | |
| Massive transfusion protocol | 32 (41.0%) | 21 (37.5%) | 11 (50.0%) | 0.322 |
| Hospital days | 43 (35–63) | 42 (34–60) | 50 (35–93) | 0.281 |
| ICU days | 20 (16–29) | 19 (16–25) | 27 (23–36) | <0.001 |
| Tracheostomy | 45 (57.7%) | 31 (55.4%) | 14 (63.6%) | 0.613 |
| Mechanical ventilation days | 20 (15–27) | 17 (14–26) | 27 (22–37) | 0.000 |
| Continuous veno-venous hemofiltration | 5 (6.4%) | 0 (0%) | 5 (22.7%) | 0.001 |
| Infectious complications | 57 (73.1%) | 37 (66%) | 20 (90%) | 0.045 |
| Per patient | 1 (0–2) | 1 (0–2) | 2 (1–3) | 0.008 |
| Sepsis * | 23 (29.5%) | 12 (21.4%) | 11 (50%) | 0.025 |
| Type of infections | ||||
| Pneumonia | 40 (51.3%) | 24 (42.9%) | 16 (72.7%) | 0.024 |
| Surgical site infection | 14 (17.9%) | 11 (9.6%) | 3 (13.6%) | 0.746 |
| Blood stream infection | 15 (19.8%) | 8 (14.3%) | 7 (31.8%) | 0.110 |
| Infected OSM | 7 (9.0%) | 3 (5.4%) | 4 (18.2%) | 0.094 |
| UTI | 5 (6.4%) | 4 (7.1%) | 1 (4.5%) | 0.999 |
| Abscess | 4 (5.1%) | 1 (1.8%) | 3 (13.6%) | 0.066 |
| Other | 12 (15.4%) | 7 (12.5%) | 5 (22.7%) | 0.303 |
| Multi-drug resistant organisms | 0.233 | |||
| MRSA | 1 (1.3%) | 1 (1.8%) | 0 (0%) | |
| ESBL | 5 (6.4%) | 3 (5.4%) | 1 (4.5%) | |
| MDR-GNB | 5 (6.4%) | 2 (3.6%) | 1 (4.5%) | |
| Multi-drug resistant Pseudomonas | 2 (2.6%) | 1 (1.8%) | 1 (4.5%) | |
| Multi-drug resistant Acinobacter | 2 (2.6%) | 1 (1.8%) | 1 (4.5%) | |
| Infectious readmissions | 20 (25.6%) | 13 (23.2%) | 7 (31.8%) | 0.565 |
| Per patient | 0 (0–0.25) | 0 (0–0) | 0 (0–1) | 0.246 |
| Total infectious complications during or after hospitalization per patient | 1 (0–3) | 1 (0–2) | 2 (1–5) | 0.018 |
| Surgical procedures during hospitalization | 62 (79.5%) | 46 (82.1%) | 16 (72.7%) | 0.365 |
| Per patient | 3 (1–6) | 3 (1–5) | 3 (0–9) | 0.720 |
| Surgical procedures after discharge | 27 (34.6%) | 20 (35.7%) | 7 (31.8%) | 0.797 |
| Per patient | 2 (0–2) | 0 (0–1) | 0 (0–2) | 0.937 |
| Total surgical procedures during or after hospitalization per patient | 3 (1–7) | 3 (1–7) | 3 (0–14) | 0.980 |
| Discharge | 0.488 | |||
| Other hospital | 8 (10.3%) | 5 (8.9%) | 3 (13.6%) | |
| Nursing home | 11 (14.1%) | 9 (16.1%) | 2 (9.1%) | |
| Rehabilitation facility | 27 (34.6%) | 20 (35.7%) | 7 (31.8%) | |
| Home (+/− additional care) | 27 (34.6%) | 20 (35.7%) | 7 (31.8%) | |
| Totally mortality | 13 (16.6%) | 8 (14.3%) | 5 (22.7%) | 0.500 |
| In hospital | 5 (6.4%) | 2 (3.6%) | 3 (13.6%) | 0.133 |
| <3 years | 8 (10.3%) | 6 (10.7%) | 2 (9.1%) | 1.000 |
| Total Cohort (n = 78) | Clinical PICS (n = 18) | Other CCI Patients (n = 60) | |
|---|---|---|---|
| PICS markers (n = 22) | n = 8 | n = 14 | Positive predictive value = 36% |
| No PICS markers (n = 56) | n = 10 | n = 46 | Negative predictive value = 82% |
| Sensitivity = 44% | Specificity = 77% |
| Characteristics | Normal Lymphocyte Count (n = 9) | Lymphocytopenia (n = 9) | p-Value |
|---|---|---|---|
| Hospital days | 58 (40–128) | 92 (71–110) | 0.401 |
| ICU days | 19 (16–25) | 27 (23–36) | 0.001 |
| Tracheostomy | 4 (44.4%) | 8 (88.9%) | 0.131 |
| Mechanical ventilation days | 21 (16–27) | 35 (31–60) | 0.001 |
| Continuous veno-venous hemofiltration | 0 (0%) | 3 (33.3%) | 0.206 |
| Infectious complications during hospitalization | 9 (100%) | 9 (100%) | 0.999 |
| Per patient | 3 (3–3) | 3 (3–4) | 0.090 |
| Multi-drug resistant organisms | 0.217 | ||
| MRSA | 1 (11.1%) | 0 (0%) | |
| ESBL | 2 (22.2%) | 0 (0%) | |
| MDR-GNB | 1 (11.1%) | 3 (33.3%) | |
| Multi-drug resistant Pseudomonas | 0 (0%) | 2 (22.2%) | |
| Multi-drug resistant Acinobacter | 0 (0%) | 1 (11.1%) | |
| Sepsis * | 7 (77.8%) | 6 (66.7%) | 0.999 |
| Infectious readmissions | 5 (55.6%) | 7 (77.8%) | 0.620 |
| Per patient | 1 (0–1) | 2 (1–5) | 0.050 |
| Total infectious complications during or after hospitalization per patient | 3 (3–4) | 6 (4–8) | 0.020 |
| Surgical procedures during hospitalization | 9 (100%) | 9 (100%) | 0.999 |
| Per patient | 4 (2–10) | 9 (6–15) | 0.156 |
| Surgical procedures after discharge | 4 (44.4%) | 7 (77.8%) | 0.335 |
| Per patient | 0 (0–3) | 5 (1–15) | 0.037 |
| Total surgical procedures during or after hospitalization per patient | 7 (2–12) | 17 (8–24) | 0.051 |
| Discharge | 0.091 | ||
| Other hospital | 1 (11.1%) | 1 (11.1%) | |
| Nursing home | 1 (11.1%) | 1 (11.1%) | |
| Rehabilitation facility | 2 (22.2%) | 6 (66.7%) | |
| Home (+/− additional care) | 5 (55.6%) | 1 (11.1%) | |
| Totally mortality | 0 (0%) | 2 (22.2%) | 0.471 |
| In hospital | 0 (0%) | 1 (11.1%) | 0.999 |
| <3 years | 0 (0%) | 1 (11.1%) | 0.999 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hesselink, L.; Hoepelman, R.J.; Spijkerman, R.; de Groot, M.C.H.; van Wessem, K.J.P.; Koenderman, L.; Leenen, L.P.H.; Hietbrink, F. Persistent Inflammation, Immunosuppression and Catabolism Syndrome (PICS) after Polytrauma: A Rare Syndrome with Major Consequences. J. Clin. Med. 2020, 9, 191. https://doi.org/10.3390/jcm9010191
Hesselink L, Hoepelman RJ, Spijkerman R, de Groot MCH, van Wessem KJP, Koenderman L, Leenen LPH, Hietbrink F. Persistent Inflammation, Immunosuppression and Catabolism Syndrome (PICS) after Polytrauma: A Rare Syndrome with Major Consequences. Journal of Clinical Medicine. 2020; 9(1):191. https://doi.org/10.3390/jcm9010191
Chicago/Turabian StyleHesselink, Lillian, Ruben J. Hoepelman, Roy Spijkerman, Mark C. H. de Groot, Karlijn J. P. van Wessem, Leo Koenderman, Luke P. H. Leenen, and Falco Hietbrink. 2020. "Persistent Inflammation, Immunosuppression and Catabolism Syndrome (PICS) after Polytrauma: A Rare Syndrome with Major Consequences" Journal of Clinical Medicine 9, no. 1: 191. https://doi.org/10.3390/jcm9010191
APA StyleHesselink, L., Hoepelman, R. J., Spijkerman, R., de Groot, M. C. H., van Wessem, K. J. P., Koenderman, L., Leenen, L. P. H., & Hietbrink, F. (2020). Persistent Inflammation, Immunosuppression and Catabolism Syndrome (PICS) after Polytrauma: A Rare Syndrome with Major Consequences. Journal of Clinical Medicine, 9(1), 191. https://doi.org/10.3390/jcm9010191