Impact of COVID-19 Quarantine on Advanced Hemorrhoidal Disease and the Role of Telemedicine in Patient Management

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Approval
2.2. Study Setting, Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Descriptive Data
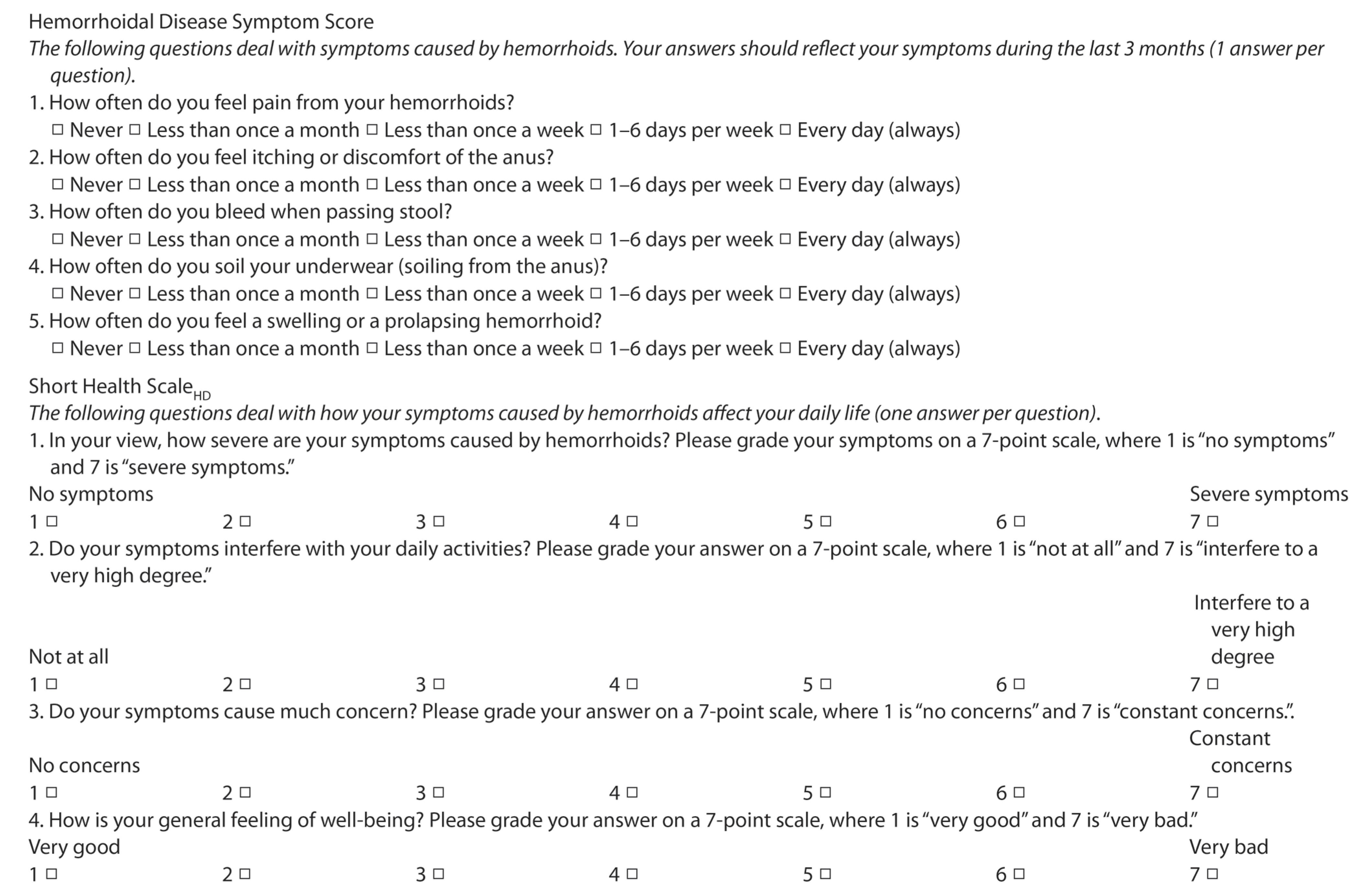
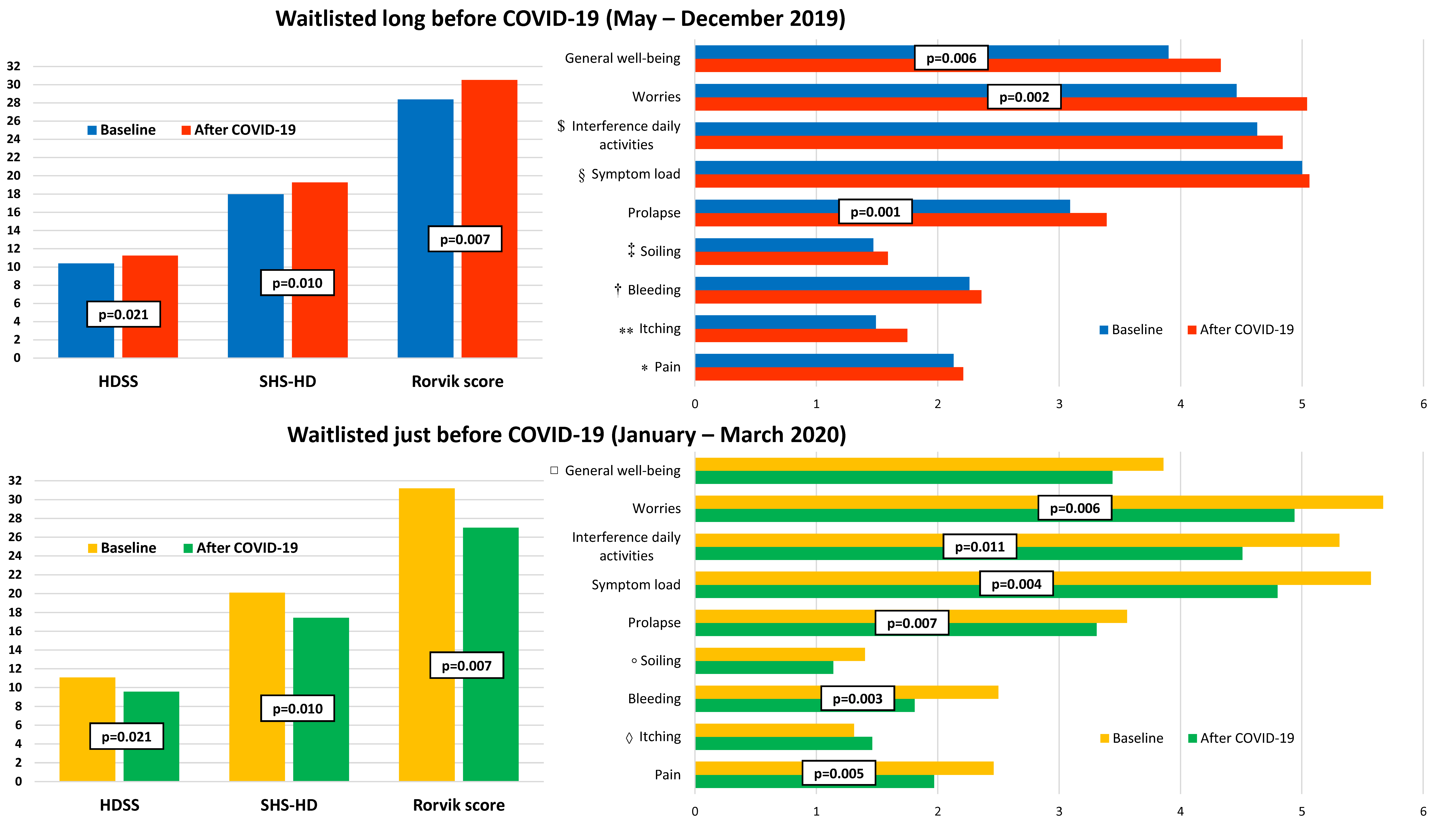
3.2. Hemorrhoidal Disease Symptoms
3.3. Telemedicine and Changes in the Waiting List
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- COVIDSurg Collaborative. Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. Br. J. Surg. 2020. [Google Scholar] [CrossRef]
- Søreide, K.; Hallet, J.; Matthews, J.B.; Schnitzbauer, A.A.; Line, P.D.; Lai, P.B.S.; Otero, J.; Callegaro, D.; Warner, S.G.; Baxter, N.N.; et al. Immediate and long-term impact of the COVID-19 pandemic on delivery of surgical services. Br. J. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Using Telehealth to Expand Access to Essential Health Services during the COVID-19 Pandemic. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/telehealth.html (accessed on 11 September 2020).
- Gençosmanoğlu, R.; Sad, O.; Koç, D.; Inceoğlu, R. Hemorrhoidectomy: Open or closed technique? A prospective, randomized clinical trial. Dis. Colon. Rectum. 2002, 45, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Lohsiriwat, V. Anatomy, Physiology, and Pathophysiology of Haemorrhoids. In Haemorrhoids, 1st ed.; Ratto, C., Parello, A., Litta, F., Eds.; Springer: Cham, Switzerland, 2018; Volume 2, pp. 9–18. [Google Scholar]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italian Ministry of Health. National guidelines on telemedicine. 2012. Available online: www.salute.gov.it/portale/temi/p2_6.jsp?lingua=italiano&id=2515&area=eHealth&menu=vuoto&tab=2 (accessed on 11 September 2020).
- Rørvik, H.D.; Styr, K.; Ilum, L.; McKinstry, G.L.; Dragesund, T.; Campos, A.H.; Brandstrup, B.; Olaison, G. Hemorrhoidal Disease Symptom Score and Short Health ScaleHD: New Tools to Evaluate Symptoms and Health-Related Quality of Life in Hemorrhoidal Disease. Dis. Colon. Rectum. 2019, 62, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obes. Res. Clin. Pract. 2020, 14, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S. Telemedicine During The COVID-19 in Italy: A Missed Opportunity? Telemed. e-Health 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwell, K.L.; Gilroy, A.S. Incorporating telemedicine as part of COVID-19 outbreak response systems. Am. J. Manag. Care 2020, 26, 147–148. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| n Patients (%) | |
|---|---|
| Sex ratio (M:F) | 59:44 |
| Age (years) | 51.3 (11.9) * |
| Comorbidities | 55 (53.4) |
| Cardiovascular | 35 (34.0) |
| Endocrine | 9 (8.7) |
| Neurological | 6 (5.8) |
| Gastrointestinal | 6 (5.8) |
| Previous cancer | 2 (1.9) |
| Others | 10 (9.7) |
| Disabilities | 2 (1.9) |
| Blindness | 1 (1.0) |
| Paraplegia | 1 (1.0) |
| Antithrombotic therapy | 10 (9.7) |
| Antiplatelet | 9 (8.7) |
| Anticoagulant | 1 (1.0) |
| Recommended surgical procedure | |
| Excisional hemorrhoidectomy | 48 (46.6) |
| Dearterialization and mucopexy | 25 (24.3) |
| Dearterialization | 2 (1.9) |
| Mixed procedure † | 28 (27.2) |
| Baseline vs. After COVID-19 | Delta * | p | ||
|---|---|---|---|---|
| Time in waiting list before COVID-19 | Long time (67) ** | 28.4(7.8) vs. 30.5(9.9) | 2.1(9.0) | <0.001 |
| Short time (36) † | 31.2(8.4) vs. 27.0(9.5) | −4.2(7.8) | ||
| Weight loss | <3 kg (91) | 28.9(8.2) vs. 29.6(9.8) | 0.8(8.4) | 0.020 |
| >3 kg (12) | 33.3(6.2) vs. 26.8(10.6) | −6.5(11.8) | ||
| Starting physical activity | No (95) | 29.1(8.1) vs. 29.8(9.7) | 0.7(8.7) | 0.002 |
| Yes (8) | 32.3(8.5) vs. 22.8(9.8) | −9.5(9.3) | ||
| Voluntary Teleconsultation | No (92) | 29.2(8.0) vs. 28.2(9.8) | −1.0(8.6) | 0.009 |
| Yes (11) | 30.9(8.9) vs. 38.3(5.5) | 7.4(10.0) | ||
| Rørvik Score | Univariate Analysis Odds Ratio (95% CI) | p | Multivariate Analysis Odds Ratio (95% CI) | p |
|---|---|---|---|---|
| Long time in waiting list * | 0.170 (0.067–0.430) | <0.001 | 0.135 (0.048–0.375) | <0.001 |
| Weight loss † | 0.312 (0.079–1.228) | 0.083 | ||
| Starting physical activity | 0.134 (0.016–1.133) | 0.034 | 0.132 (0.014–1.196) | 0.072 |
| Voluntary Teleconsultation | 5.598 (1.146–27.350) | 0.019 | 7.412 (1.268–43.338) | 0.026 |
| Emergency surgery | 2.167 (0.190–24.668) | 0.524 | ||
| Medication § | 2.020 (0.876–4.657) | 0.097 | ||
| Topical medication | 2.148 (0.891–5.177) | 0.086 | ||
| Antithrombotic therapy | 1.670 (0.442–6.310) | 0.446 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campennì, P.; Marra, A.A.; Ferri, L.; Orefice, R.; Parello, A.; Litta, F.; De Simone, V.; Goglia, M.; Ratto, C. Impact of COVID-19 Quarantine on Advanced Hemorrhoidal Disease and the Role of Telemedicine in Patient Management. J. Clin. Med. 2020, 9, 3416. https://doi.org/10.3390/jcm9113416
Campennì P, Marra AA, Ferri L, Orefice R, Parello A, Litta F, De Simone V, Goglia M, Ratto C. Impact of COVID-19 Quarantine on Advanced Hemorrhoidal Disease and the Role of Telemedicine in Patient Management. Journal of Clinical Medicine. 2020; 9(11):3416. https://doi.org/10.3390/jcm9113416
Chicago/Turabian StyleCampennì, Paola, Angelo A. Marra, Lorenzo Ferri, Raffaele Orefice, Angelo Parello, Francesco Litta, Veronica De Simone, Marta Goglia, and Carlo Ratto. 2020. "Impact of COVID-19 Quarantine on Advanced Hemorrhoidal Disease and the Role of Telemedicine in Patient Management" Journal of Clinical Medicine 9, no. 11: 3416. https://doi.org/10.3390/jcm9113416
APA StyleCampennì, P., Marra, A. A., Ferri, L., Orefice, R., Parello, A., Litta, F., De Simone, V., Goglia, M., & Ratto, C. (2020). Impact of COVID-19 Quarantine on Advanced Hemorrhoidal Disease and the Role of Telemedicine in Patient Management. Journal of Clinical Medicine, 9(11), 3416. https://doi.org/10.3390/jcm9113416