Patients with Inflammatory Bowel Disease Are Not at Increased Risk of COVID-19: A Large Multinational Cohort Study


 ,
,  ,
,  ,
,  , ,
, ,  , , add
Show full author list
, , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Study Population
4. Outcome Measures
5. Statistical Analyses
6. Results
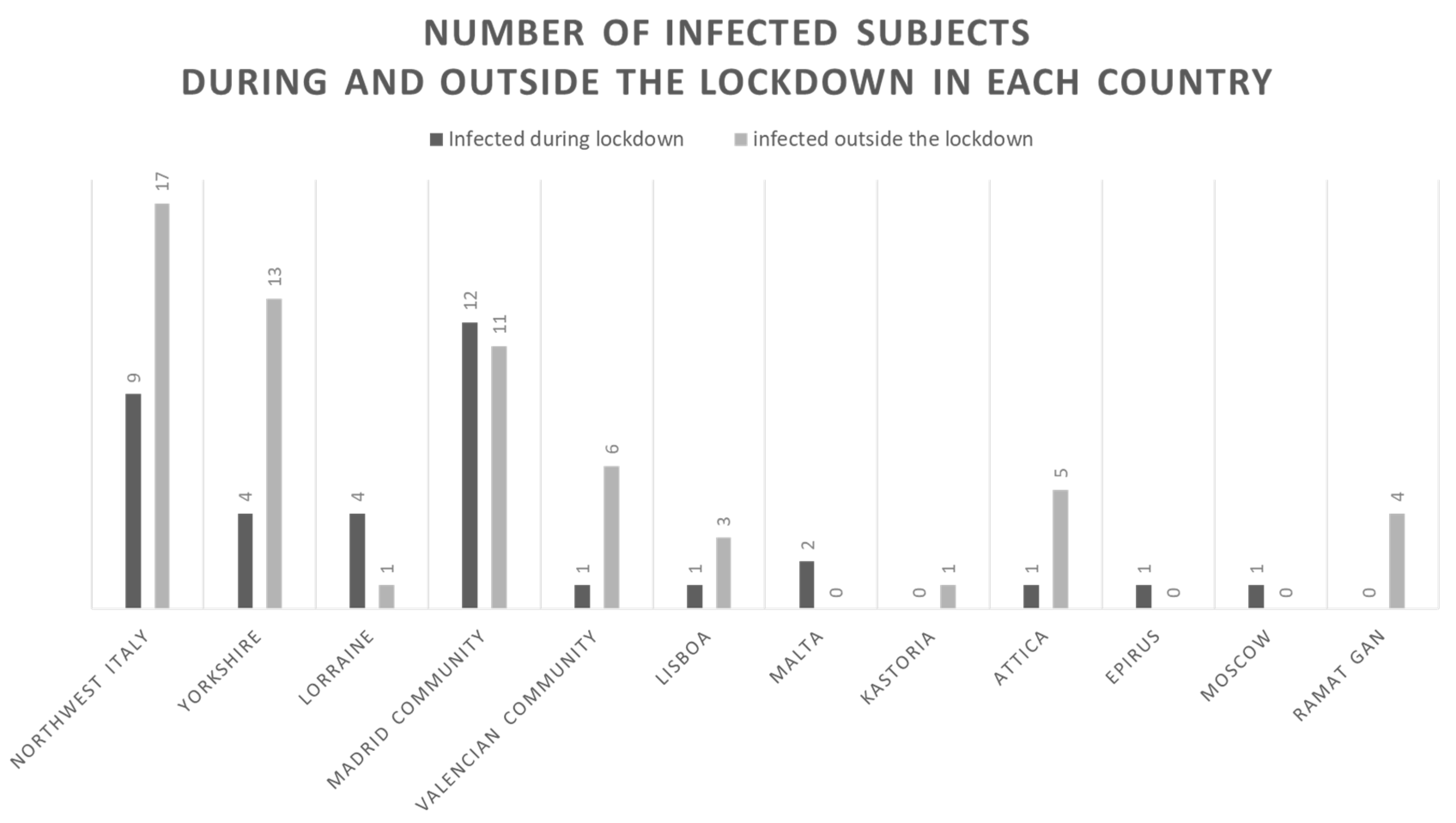
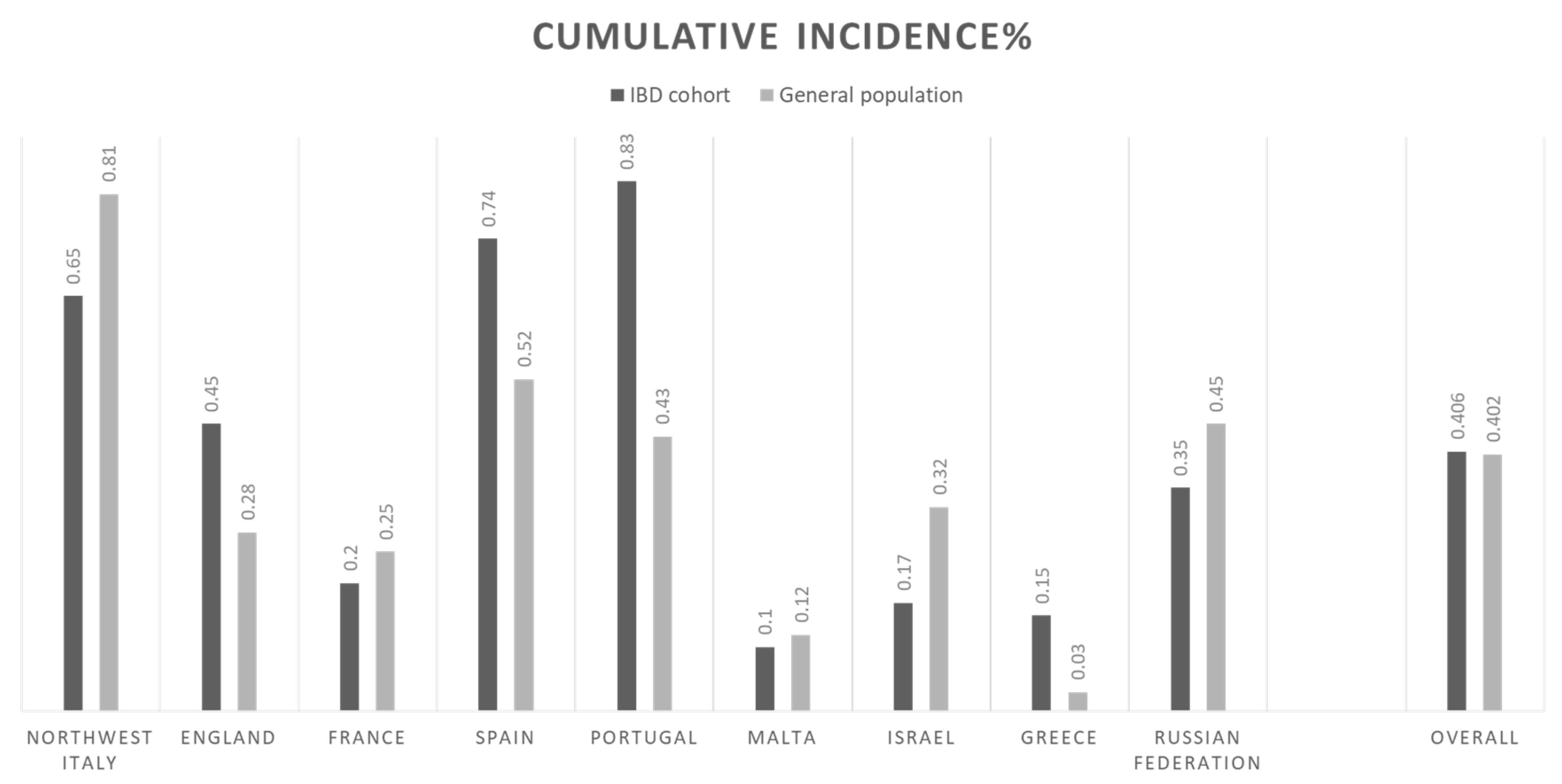
7. The Impact of National Lockdowns on SARS-CoV-2 Infection
8. COVID-19 Outcomes
9. Special Situations
10. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- John Hopkins University Coronavirus Resource Center. Coronavirus Covid-19 Global Cases. Available online: https://coronavirus.jhu.edu/map.html (accessed on 25 October 2020).
- Boruchowicz, A.; Duclos, B.; Soulé, J.C.; Lerebours, E.; Lémann, M.; Belaïche, J.; Colombel, J.F.; Cosnes, J.; Gendre, J.P.; Carbonnel, F. Intravenous cyclosporine in attacks of ulcerative colitis. Dig. Dis. Sci. 1996, 41, 2471–2476. [Google Scholar] [CrossRef]
- Panaccione, R.; Löfberg, R.; Rutgeerts, P.; Sandborn, W.J.; Schreiber, S.; Berg, S.; Maa, J.-F.; Petersson, J.; Robinson, A.M.; Colombel, J.-F. Efficacy and Safety of Adalimumab by Disease Duration: Analysis of Pooled Data From Crohn’s Disease Studies. J. Crohn’s Colitis 2019, 13, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide Incidence and Prevalence of Inflammatory Bowel Disease in the 21st Century: A Systematic Review of Population-Based Studies. Lancet 2018, 390, 2769–2778. [Google Scholar] [CrossRef]
- Kirchgesner, J.; Lemaitre, M.; Carrat, F.; Zureik, M.; Carbonnel, F.; Dray-Spira, R. Risk of Serious and Opportunistic Infections Associated With Treatment of Inflammatory Bowel Diseases. Gastroenterology 2018, 155, 337–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.; Lee, J.K.; Mitra, A.R.; Teriaky, A.; Choudhary, D.; Nguyen, T.M.; Casteele, N.V.; Khanna, R.; Panaccione, R.; Feagan, B.G.; et al. Systematic review with meta-analysis: Efficacy and safety of oral Janus kinase inhibitors for inflammatory bowel disease. Aliment. Pharmacol. Ther. 2019, 50, 5–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allocca, M.; Fiorino, G.; Zallot, C.; Furfaro, F.; Gilardi, D.; Radice, S.; Danese, S.; Peyrin-Biroulet, L. Incidence and Patterns of COVID-19 Among Inflammatory Bowel Disease Patients From the Nancy and Milan Cohorts. Clin. Gastroenterol. Hepatol. 2020, 18, 2134–2135. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.; Fatima, R.; Haghbin, H.; Lee-Smith, W.; Nawras, A. The Incidence and Outcomes of COVID-19 in IBD Patients: A Rapid Review and Meta-analysis. Inflamm. Bowel Dis. 2020, 26, e132–e133. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.; Fatima, R.; Assaly, R. Elevated interleukin-6 and severe COVID-19: A meta-analysis. J. Med. Virol. 2020, 92, 2283–2285. [Google Scholar] [CrossRef] [PubMed]
- Bezzio, C.; Manes, G.; Bini, F.; Pellegrini, L.; Saibeni, S. Infliximab for Severe Ulcerative Colitis and Subsequent Sars-Cov-2 Pneumonia: A Stone for Two Birds. Gut 2020. [Google Scholar] [CrossRef] [PubMed]
- Mazza, S.; Sorce, A.; Peyvandi, F.; Vecchi, M.; Caprioli, F. A fatal case of COVID-19 pneumonia occurring in a patient with severe acute ulcerative colitis. Gut 2020, 69, 1148–1149. [Google Scholar] [CrossRef] [PubMed]
- Allocca, M.; Guidelli, G.M.; Borroni, R.G.; Selmi, C.; Narcisi, A.; Danese, S.; Fiorino, G. Clinical course of COVID-19 in 41 patients with immune-mediated inflammatory diseases: Experience from humanitas center, Milan. Pharmacol. Res. 2020, 160, 105061. [Google Scholar] [CrossRef] [PubMed]
- Brenner, E.J.; Ungaro, R.C.; Gearry, R.B.; Kaplan, G.G.; Kissous-Hunt, M.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Ruemmele, F.M.; et al. Corticosteroids, But Not TNF Antagonists, Are Associated with Adverse COVID-19 Outcomes in Patients with Inflammatory Bowel Diseases: Results From an International Registry. Gastroenterology 2020, 159, 481–491. [Google Scholar] [CrossRef] [PubMed]
- Caruso, D.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Polidori, T.; Rucci, C.; Guido, G.; Bracci, B.; De Dominicis, C.; Laghi, A. Chest CT Features of COVID-19 in Rome, Italy. Radiology 2020, 296, E79–E85. [Google Scholar] [CrossRef] [PubMed]
- Bezzio, C.; Saibeni, S.; Variola, A.; Allocca, M.; Massari, A.; Gerardi, V.; Casini, V.; Ricci, C.; Zingone, F.; Amato, A.; et al. Outcomes of COVID-19 in 79 patients with IBD in Italy: An IG-IBD study. Gut 2020, 69, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.T.; Feuerstein, J.D.; Wang, A.Y.; Cohen, R.D. AGA Clinical Practice Update on Management of Inflammatory Bowel Disease During the COVID-19 Pandemic: Expert Commentary. Gastroenterology 2020, 159, 350–357. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age at diagnosis of COVID-19 | 42 (28.7–54.2) |
| Age > 65 years | 9 (9.0) |
| Males | 50 (52) |
| Countries | |
| Northwest Italy (Italy) | 26 (27) |
| Yorkshire (England) | 17 (18) |
| Lorraine (France) | 5 (5.0) |
| Madrid (Spain) | 23 (24) |
| Valencia (Spain) | 7 (7.0) |
| Lisboa (Portugal) | 5 (5.0) |
| Malta (Malta) | 2 (2.0) |
| Ramat Gan (Israel) | 4 (4.0) |
| Kastoria (Greece) | 1 (1.0) |
| Athens (Greece) | 5 (5.0) |
| Epirus (Greece) | 1 (1.0) |
| Moscow (Russian federation) | 1 (1.0) |
| IBD diagnosis | |
| Ulcerative colitis | 43 (44) |
| Crohn’s disease | 53 (55) |
| Unclassified IBD | 1 (1.0) |
| Clinical activity * | 27 (28) |
| Medications | |
| Corticosteroids | 8 (8.0) |
| Any immunosuppressants | 24 (25) |
| Azathioprine | 16 (67) |
| Methotrexate | 7 (29) |
| Tacrolimus | 1 (4.0) |
| Monoclonal Antibodies | 51 (53) |
| Tumor necrosis factor inhibitor | 38 (74) |
| Interleukin-12/23 blocker | 10 (20) |
| Vedolizumab | 3 (6.0) |
| Janus Kinase Inhibitor | 1 (1.0) |
| Filgotinib | 1 (1.0) |
| Combo therapy | 18 (19) |
| Azathioprine + Tumor necrosis factor inhibitor | 8 (44) |
| Methotrexate + Tumor necrosis factor inhibitor | 3 (17) |
| Methotrexate + Interleukin-12/23 blocker | 3 (17) |
| Corticosteroids + Tacrolimus + Tumor necrosis factor inhibitor | 1 (5.0) |
| Corticosteroids + Tumor necrosis factor inhibitor | 2 (11) |
| Corticosteroids + Tumor necrosis factor inhibitor | 1 (5.0) |
| Clinical trial participants | 4 (4.0) |
| Exposure risk | |
| High-risk work ** | 18 (22) |
| Working contact | 42 (48) |
| Contact with confirmed or suspected COVID patients | 44 (56) |
| No strict adherence to prevention measures | 27 (28) |
| In- and out-patient visits (within 14 days from COVID infection) | 22 (23) |
| Smoking | 8 (8.0) |
| Comorbidities | 33 (34) |
| Hypertension | 13 (13) |
| Chronic lung diseases | 3 (3.0) |
| Diabetes mellitus | 5 (5.0) |
| Obesity | 5 (5.0) |
| Connective tissue diseases | 6 (6.0) |
| Malignancy § | 2 (2.0) |
| Chronic liver disease | 4 (4.0) |
| Stroke | 1 (1.0) |
| Myocardial ischemia | 2 (2.0) |
| Renal transplantation | 1 (1.0) |
| Other | 3 (3.0) |
| Pregnancy | 2 (2.0) |
| Positive rhino-pharyngeal swabs | 64 (66) |
| COVID-related symptoms | 87 (90) |
| Gastro-intestinal symptoms | 30 (31) |
| COVID-related pneumonia | 21 (22) |
| Discontinuation of IBD therapy | 46 (47) |
| Hospitalization | 23 (24) |
| Intensive Care Unit | 4 (4.0) |
| Death | 1 (1.0) |
| Risk of Pneumonia | Risk of Hospitalization | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| Parameters | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p |
| Age > 65 years | 9.60 (2.15–42.74) | 0.003 | 6.76 (1.10–41.46) | 0.038 | 4.86 (1.18–19.97) | 0.028 | 5.13 (1.10–23.86) | 0.036 |
| Any comorbidity | 4.46 (1.61–12.37) | 0.004 | - | - | 2.75 (1.05–7.20) | 0.039 | - | - |
| Charlson’s Comorbidity Index (per unit increase) | 1.47 (1.06–2.04) | 0.02 | - | - | 1.40 (1.021.91) | 0.03 | - | - |
| Monoclonal Antibodies | 0.17 (0.05–0.53) | 0.002 | 0.15 (0.04–0.54) | 0.003 | 0.32 (0.12–0.86) | 0.024 | 0.31 (0.10–0.90) | 0.031 |
| Diagnosis of UC § | 3.17 (1.14–8.79) | 0.02 | - | - | 1.90 (0.74–4.91) | 0.18 | - | - |
| Male gender | 2.85 (1.00–8.16) | 0.05 | - | - | 2.08 (0.79–5.52) | 0.13 | - | - |
| Corticosteroids | 2.33 (0.51–0.69) | 0.27 | - | - | 6.57 (1.43–30.11) | 0.015 | 7.69 (1.48–0.05) | 0.015 |
| Immunomodulators | 0.92 (0.29–2.85) | 0.88 | - | - | 1.09 (0.37–3.20) | 0.86 | - | - |
| Combination therapy | 0.38 (0.08–1.84) | 0.23 | - | - | 0.90 (0.26–3.07) | 0.87 | - | - |
| Smoking habit | 0,42 (0.04–3.55) | 0.42 | - | - | 0.32 (0.03–2.74) | 0.30 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allocca, M.; Chaparro, M.; Gonzalez, H.A.; Bosca-Watts, M.M.; Palmela, C.; D’Amico, F.; Zacharopoulou, E.; Kopylov, U.; Ellul, P.; Bamias, G.; et al. Patients with Inflammatory Bowel Disease Are Not at Increased Risk of COVID-19: A Large Multinational Cohort Study. J. Clin. Med. 2020, 9, 3533. https://doi.org/10.3390/jcm9113533
Allocca M, Chaparro M, Gonzalez HA, Bosca-Watts MM, Palmela C, D’Amico F, Zacharopoulou E, Kopylov U, Ellul P, Bamias G, et al. Patients with Inflammatory Bowel Disease Are Not at Increased Risk of COVID-19: A Large Multinational Cohort Study. Journal of Clinical Medicine. 2020; 9(11):3533. https://doi.org/10.3390/jcm9113533
Chicago/Turabian StyleAllocca, Mariangela, María Chaparro, Haidee Aleman Gonzalez, Marta Maia Bosca-Watts, Carolina Palmela, Ferdinando D’Amico, Eirini Zacharopoulou, Uri Kopylov, Pierre Ellul, Giorgos Bamias, and et al. 2020. "Patients with Inflammatory Bowel Disease Are Not at Increased Risk of COVID-19: A Large Multinational Cohort Study" Journal of Clinical Medicine 9, no. 11: 3533. https://doi.org/10.3390/jcm9113533
APA StyleAllocca, M., Chaparro, M., Gonzalez, H. A., Bosca-Watts, M. M., Palmela, C., D’Amico, F., Zacharopoulou, E., Kopylov, U., Ellul, P., Bamias, G., Ntelis, V., Lahat, A., Mantzaris, G. J., Papaconstantinou, I., Katsanos, K., Uspenskaya, Y., Christodoulou, D., Ben Horin, S., Peyrin-Biroulet, L., ... Fiorino, G. (2020). Patients with Inflammatory Bowel Disease Are Not at Increased Risk of COVID-19: A Large Multinational Cohort Study. Journal of Clinical Medicine, 9(11), 3533. https://doi.org/10.3390/jcm9113533