Physiological Criteria Are Useful for the Diagnosis of Idiopathic Pleuroparenchymal Fibroelastosis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Clinical Characteristics and Respiratory Function Data
2.3. The Flat Chest Index
2.4. Diagnostic Sensitivity and Specificity of the Physiological Criteria
2.5. Statistical Analyses
3. Results
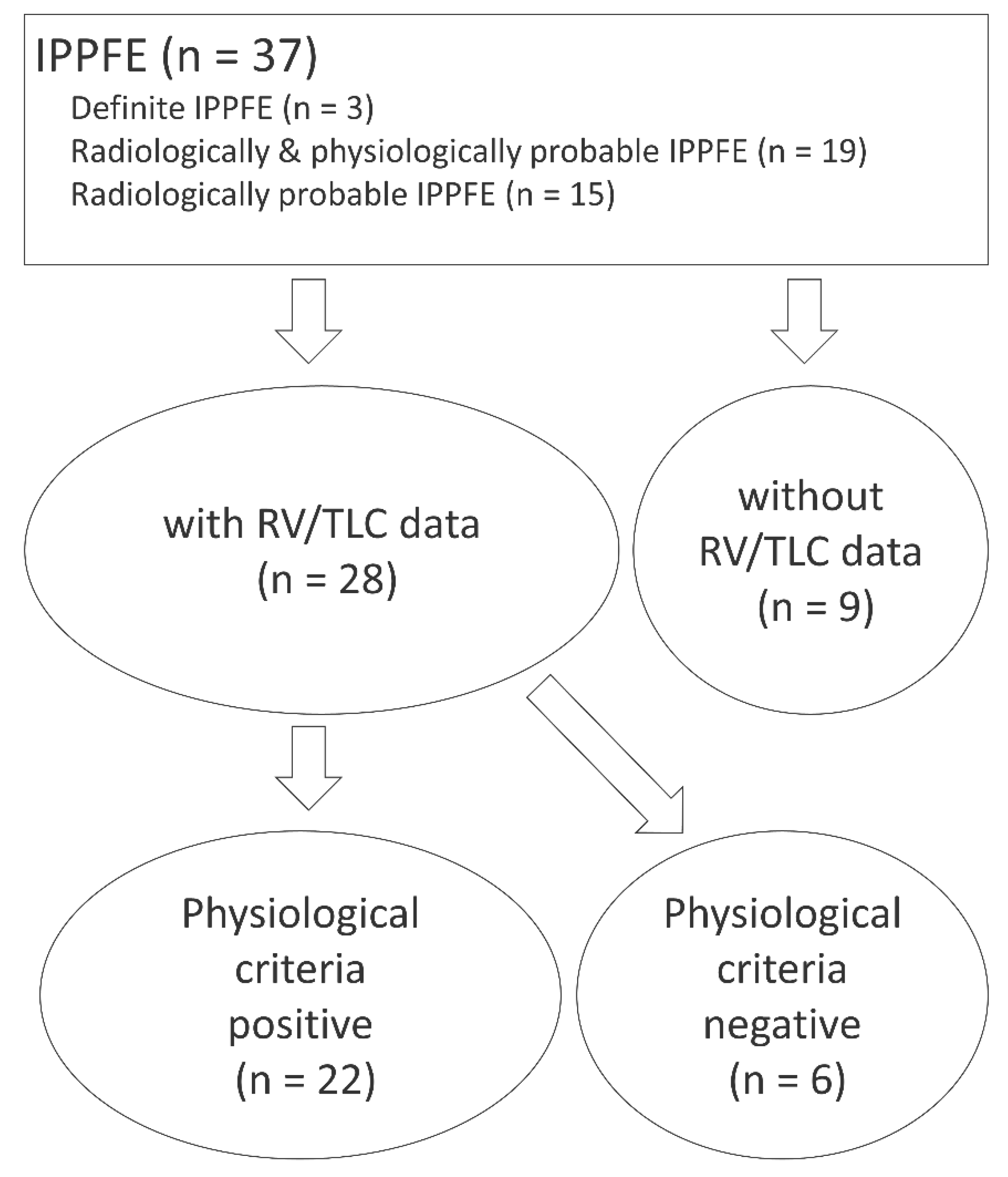
3.1. Study Patients
3.2. Patients’ Characteristics
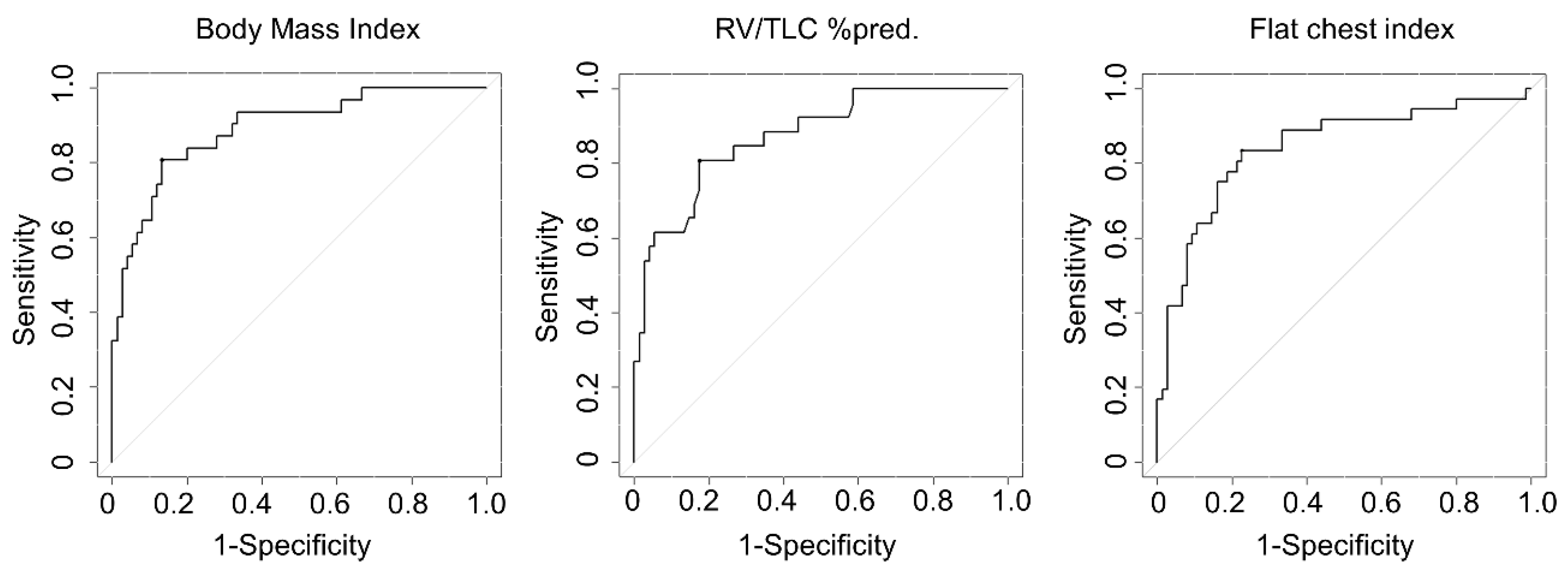
3.3. Diagnostic Sensitivity and Specificity of the Physiological Criteria
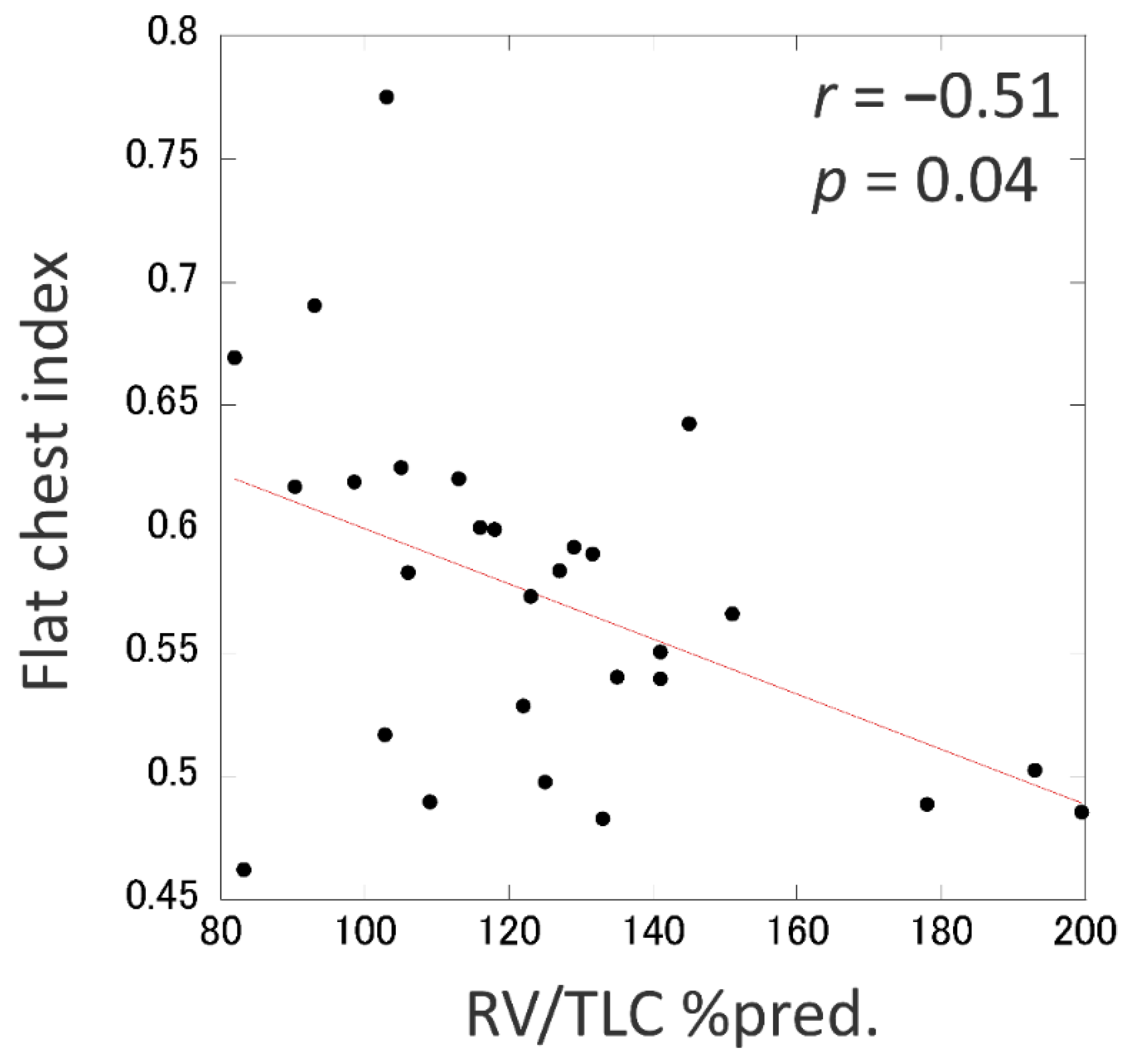
3.4. An Alternative Physiologic Parameter for RV/TLC %pred.
3.5. Clinical Characteristics of IPPFE Patients Who Did Not Meet the Physiological Criteria
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Amitani, R.; Niimi, A.; Kuse, F. Idiopathic pulmonary upper lobe fibrosis. Kokyu 1992, 11, 693–699. [Google Scholar]
- Frankel, S.K.; Cool, C.D.; Lynch, D.A.; Brown, K.K. Idiopathic pleuroparenchymal fibroelastosis: Description of a novel clinicopathologic entity. Chest 2004, 126, 2007–2013. [Google Scholar] [CrossRef]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef]
- Kato, M.; Sasaki, S.; Kurokawa, K.; Nakamura, T.; Yamada, T.; Sasano, H.; Arano, N.; Komura, M.; Ihara, H.; Nagashima, O.; et al. Usual interstitial pneumonia pattern in the lower lung lobes as a prognostic factor in idiopathic pleuroparenchymal fibroelastosis. Respiration 2019, 97, 319–328. [Google Scholar] [CrossRef]
- Shiota, S.; Shimizu, K.; Suzuki, M.; Nakaya, Y.; Sakamoto, K.; Iwase, A.; Aoki, S.; Matsuoka, R.; Shimizu, S.; Nagayama, Y.; et al. Seven cases of marked pulmonary fibrosis in the upper lobe. Nihon Kokyuki Gakkai Zasshi 1999, 37, 87–96. [Google Scholar]
- Watanabe, K.; Nagata, N.; Kitasato, Y.; Wakamatsu, K.; Nabeshima, K.; Harada, T.; Hirota, T.; Shiraishi, M.; Fujita, M. Rapid decrease in forced vital capacity in patients with idiopathic pulmonary upper lobe fibrosis. Respir. Investig. 2012, 50, 88–97. [Google Scholar] [CrossRef]
- Fuke, S.; Betsuyaku, T.; Oizumi, S.; Saito, Y.; Hiroshi, N.; Etsuro, Y.; Nishimura, M. A case of idiopathic pulmonary upper lobe fibrosis complicated by invasive pulmonary Aspergillosis. Nihon Kokyuki Gakkai Zasshi 1982, 20, 203–209. [Google Scholar]
- Morimoto, A.; Mochizuki, Y.; Nakahara, Y.; Kawamura, T.; Sakaki, S.; Kobashi, Y. A case of idiopathic pulmonary upper lobe fibrosis. Nihon Kokyuki Gakkai Zasshi 2011, 48, 944–949. [Google Scholar]
- Nagashima, O.; Matsuno, K.; Tominaga, S.; Takahashi, K. Esophageal diverticulum with idiopathic pulmonary upper lobe fibrosis. Intern. Med. 2013, 52, 159. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, Y.; Yoshimura, K.; Enomoto, Y.; Yasui, H.; Hozumi, H.; Karayama, M.; Furuhashi, K.; Enomoto, N.; Fujisawa, T.; Nakamura, Y.; et al. Distinct profile and prognostic impact of body composition changes in idiopathic pulmonary fibrosis and idiopathic pleuroparenchymal fibroelastosis. Sci. Rep. 2018, 8, 14074. [Google Scholar] [CrossRef]
- Ishii, H.; Watanabe, K.; Kushima, H.; Baba, T.; Watanabe, S.; Yamada, Y.; Arai, T.; Tsushima, K.; Kondoh, Y.; Nakamura, Y.; et al. Pleuroparenchymal fibroelastosis diagnosed by multidisciplinary discussions in Japan. Respir. Med. 2018, 141, 190–197. [Google Scholar] [CrossRef]
- Ishii, H.; Kinoshita, Y.; Kushima, H.; Nagata, N.; Watanabe, K. The similarities and differences between pleuroparenchymal fibroelastosis and idiopathic pulmonary fibrosis. Chronic Respir. Dis. 2019, 16, 147997311986794. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Ishii, H.; Kiyomi, F.; Terasaki, Y.; Hebisawa, A.; Kawabata, Y.; Johkoh, T.; Sakai, F.; Kondoh, Y.; Inoue, Y.; et al. Criteria for the diagnosis of idiopathic pleuroparenchymal fibroelastosis: A proposal. Respir. Investig. 2019, 57, 312–320. [Google Scholar] [CrossRef]
- Camus, P.; von der Thüsen, J.H.; Hansell, D.M.; Colby, T.V. Pleuroparenchymal fibroelastosis: One more walk on the wild side of drugs? Eur. Respir. J. 2014, 44, 289–296. [Google Scholar] [CrossRef] [Green Version]
- Harada, T.; Yoshida, Y.; Kitasato, Y.; Tsuruta, N.; Wakamatsu, K.; Hirota, T.; Tanaka, M.; Tashiro, N.; Ishii, H.; Shiraishi, M.; et al. The thoracic cage becomes flattened in the progression of pleuroparenchymal fibroelastosis. Eur. Respir. Rev. 2014, 23, 263–266. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, Y.; Nagata, N.; Tsuruta, N.; Kitasato, Y.; Wakamatsu, K.; Yoshimi, M.; Ishii, H.; Hirota, T.; Hamada, N.; Fujita, M.; et al. Heterogeneous clinical features in patients with pulmonary fibrosis showing histology of pleuroparenchymal fibroelastosis. Respir. Investig. 2016, 54, 162–169. [Google Scholar] [CrossRef]
- Watanabe, K. Pleuroparenchymal fibroelastosis: Its clinical characteristics. Curr. Respir. Med. Rev. 2013, 9, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, S.; Waseda, Y.; Takato, H.; Matsunuma, R.; Johkoh, T.; Egashira, R.; Kawabata, Y.; Ikeda, H.; Yasui, M.; Fujimura, M.; et al. Pleuroparenchymal fibroelastosis: Distinct pulmonary physiological features in nine patients. Respir. Investig. 2015, 53, 149–155. [Google Scholar] [CrossRef]
- Oda, T.; Ogura, T.; Kitamura, H.; Hagiwara, E.; Baba, T.; Enomoto, Y.; Iwasawa, T.; Okudela, K.; Takemura, T.; Sakai, F.; et al. Distinct characteristics of pleuroparenchymal fibroelastosis with usual interstitial pneumonia compared with idiopathic pulmonary fibrosis. Chest 2014, 146, 1248–1255. [Google Scholar] [CrossRef]
- Enomoto, Y.; Nakamura, Y.; Satake, Y.; Sumikawa, H.; Johkoh, T.; Colby, T.V.; Yasui, H.; Hozumi, H.; Karayama, M.; Suzuki, Y.; et al. Clinical diagnosis of idiopathic pleuroparenchymal fibroelastosis: A retrospective multicenter study. Respir. Med. 2017, 133, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, H.; Nei, T.; Abe, S.; Saito, Y.; Kokuho, N.; Atsumi, K.; Fujita, K.; Saito, T.; Tanaka, T.; Gemma, A.; et al. Body mass index and arterial blood oxygenation as prognostic factors in patients with idiopathic pleuroparenchymal fibroelastosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2017, 34, 35–40. [Google Scholar]
- Reddy, T.L.; Tominaga, M.; Hansell, D.M.; von der Thüsen, J.H.; Rassl, D.; Parfrey, H.; Guy, S.; Twentyman, O.; Rice, A.; Maher, T.M.; et al. Pleuroparenchymal fibroelastosis: A spectrum of histopathological and imaging phenotypes. Eur. Respir. J. 2012, 40, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Watanabe, K.; Ishii, H.; Kushima, H.; Fujita, M.; Nabeshima, K. Proliferation of elastic fibres in idiopathic pulmonary fibrosis: A whole-slide image analysis and comparison with pleuroparenchymal fibroelastosis. Histopathology 2017, 71, 934–942. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Ishii, H.; Kushima, H.; Johkoh, T.; Yabuuchi, H.; Fujita, M.; Nabeshima, K.; Watanabe, K. Remodeling of the pulmonary artery in idiopathic pleuroparenchymal fibroelastosis. Sci. Rep. 2020, 10, 306. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Watanabe, K.; Ishii, H.; Kushima, H.; Fujita, M.; Nabeshima, K. Significant increases in the density and number of lymphatic vessels in pleuroparenchymal fibroelastosis. Histopathology 2018, 73, 417–427. [Google Scholar] [CrossRef]
- Sekine, A.; Satoh, H.; Iwasawa, T.; Matsui, K.; Ikeya, E.; Ikeda, S.; Yamakawa, H.; Okuda, R.; Kitamura, H.; Shinohara, T.; et al. Unilateral Upper Lung Field Pulmonary Fibrosis Radiologically Consistent with Pleuroparenchymal Fibroelastosis after Thoracotomy: A New Disease Entity Related to Thoracotomy. Respiration 2017, 94, 431–441. [Google Scholar] [CrossRef]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.-F.; Flaherty, K.R.; Lasky, J.a.; et al. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef]
- Bendstrup, E.; Hilberg, O.; Hyldgaard, C. Idiopathic pulmonary fibrosis: Diagnosis and treatment. International consensus statement. Am. J. Respir. Crit. Care Med. 2000, 161, 646–664. [Google Scholar] [CrossRef] [Green Version]
- Clay, R.D.; Iyer, V.N.; Reddy, D.R.; Siontis, B.; Scanlon, P.D. The “Complex Restrictive” Pulmonary Function Pattern: Clinical and Radiologic Analysis of a Common but Previously Undescribed Restrictive Pattern. Chest 2017, 152, 1258–1265. [Google Scholar] [CrossRef]
- Suzuki, Y.; Fujisawa, T.; Sumikawa, H.; Tanaka, T.; Sugimoto, C.; Masato, K.; Hozumi, H.; Karayama, M.; Furuhashi, K.; Enomoto, N.; et al. Disease course and prognosis of pleuroparenchymal fibroelastosis compared with idiopathic pulmonary fibrosis. Respir. Med. 2020, 106078. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | IPPFE (n = 37) | IPF (n = 89) | p-Value |
|---|---|---|---|
| Clinical data | |||
| Age, years | 69.6 ± 14.7 | 74.4 ± 7.23 | 0.016 |
| Gender, male/female | 21/16 | 73/16 | 0.006 |
| Brinkman Index | 208 ± 331 | 744 ± 757 | <0.001 |
| BMI, kg/m2 | 17.9 ± 3.17 | 22.8 ± 2.98 | <0.001 |
| Flat chest index | 0.57 ± 0.07 | 0.65 ± 0.05 | <0.001 |
| Serum KL-6, U/mL | 574 ± 345 | 1100 ± 798 | <0.001 |
| Respiratory function parameters | |||
| FVC, %pred. | 66.6 ± 23.2 | 87.4 ± 17.2 | <0.001 |
| FEV1/FVC, % | 90.6 ± 9.82 | 80.0 ± 8.36 | <0.001 |
| FRC, %pred. | 78.2 ± 18.2 | 70.8 ± 18.0 | 0.072 |
| RV, %pred. | 86.9 ± 27.5 | 64.0 ± 19.7 | <0.001 |
| TLC, %pred. | 73.9 ± 14.6 | 76.3 ± 14.3 | 0.453 |
| RV/TLC, %pred. | 124 ± 29.5 | 86.3 ± 19.2 | <0.001 |
| DLco, %pred. | 103 ± 49.8 | 74.6 ± 37.2 | 0.005 |
| Present Study | Watanabe et al [13] | |||||||
|---|---|---|---|---|---|---|---|---|
| Cut-Off | Sensitivity | Specificity | AUC | Cut-Off | Sensitivity | Specificity | AUC | |
| BMI, kg/m2 | 20 | 75.0% | 88.0% | 0.875 | 20 | 78.1% | 82.5% | 0.881 |
| RV/TLC, %pred. | 115 | 64.3% | 93.3% | 0.878 | 115 | 75.6% | 88.7% | 0.908 |
| Flat chest index | 0.58 | 61.5% | 92.0% | 0.837 | NA | NA | NA | NA |
| BMI + RV/TLC | 78.6% | 88.0% | 87.8% | 83.5% | ||||
| BMI + flat chest index | 82.1% | 89.3% | NA | NA | ||||
| Factor | IPPFE with Physiologically Positive (n = 22) | IPPFE with Physiologically Negative (n = 6) | p-Value |
|---|---|---|---|
| Clinical data | |||
| Age, years | 72.0 (67.5–75.7) | 66.0 (63.7–77.2) | 0.736 |
| Gender, male/female | 11/11 | 5/1 | 0.196 |
| Brinkman Index | 0 (0–550) | 180 (40.0–650) | 0.273 |
| BMI, kg/m2 | 17.4 (14.9–18.8) | 21.7 (21.2–21.9) | <0.001 |
| Flat chest index | 0.55 (0.50–0.59) | 0.65 (0.62–0.69) | 0.002 |
| Serum KL-6, U/mL | 634 (290–798) | 442 (394–573) | 0.933 |
| Respiratory function parameters | |||
| FVC, %pred. | 58.4 (46.8–72.8) | 91.8 (84.1–96.2) | 0.008 |
| FEV1/FVC, % | 94.4 (86.5–100) | 87.8 (84.0–90.6) | 0.084 |
| FRC, %pred. | 76.4 (68.0–90.0) | 81.6 (58.2–92.1) | 0.867 |
| RV, %pred. | 88.8 (69.8–94.4) | 81.4 (62.1–84.3) | 0.373 |
| TLC, %pred. | 69.0 (63.8–81.2) | 78.8 (71.0–89.2) | 0.314 |
| RV/TLC, %pred. | 128 (116–141) | 98.0 (90.9–104) | 0.002 |
| DLco, %pred. | 95.0 (80.6–119) | 98.6 (87.2–114) | 0.768 |
| CT findings, n (%) | |||
| Lower lobe UIP | 3 (13.6) | 3 (50) | 0.091 |
| Lower lobe ILD (including UIP) | 11 (50) | 5 (83.3) | 0.196 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, T.; Kinoshita, Y.; Ueda, Y.; Sasaki, T.; Kushima, H.; Ishii, H. Physiological Criteria Are Useful for the Diagnosis of Idiopathic Pleuroparenchymal Fibroelastosis. J. Clin. Med. 2020, 9, 3761. https://doi.org/10.3390/jcm9113761
Ikeda T, Kinoshita Y, Ueda Y, Sasaki T, Kushima H, Ishii H. Physiological Criteria Are Useful for the Diagnosis of Idiopathic Pleuroparenchymal Fibroelastosis. Journal of Clinical Medicine. 2020; 9(11):3761. https://doi.org/10.3390/jcm9113761
Chicago/Turabian StyleIkeda, Takato, Yoshiaki Kinoshita, Yusuke Ueda, Tomoya Sasaki, Hisako Kushima, and Hiroshi Ishii. 2020. "Physiological Criteria Are Useful for the Diagnosis of Idiopathic Pleuroparenchymal Fibroelastosis" Journal of Clinical Medicine 9, no. 11: 3761. https://doi.org/10.3390/jcm9113761
APA StyleIkeda, T., Kinoshita, Y., Ueda, Y., Sasaki, T., Kushima, H., & Ishii, H. (2020). Physiological Criteria Are Useful for the Diagnosis of Idiopathic Pleuroparenchymal Fibroelastosis. Journal of Clinical Medicine, 9(11), 3761. https://doi.org/10.3390/jcm9113761