Sirtuin 1: Endocan and Sestrin 2 in Different Biological Samples in Patients with Asthma. Does Severity Make the Difference?





Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Sputum Induction
2.3. Blood Sampling
2.4. Lung Function
2.5. Atopic Status
2.6. Mediator Assays
3. Statistical Analysis
4. Results
5. Discussion
Author Contributions
Conflicts of Interest
References
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef]
- McDowell, P.J.; Heaney, L.G. Different endotypes and phenotypes drive the heterogeneity in severe asthma. Allergy 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, K.F.; Wenzel, S.E.; Brozek, j.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djukanovic, R.; Adcock, I.M.; Anderson, G.; Bel, E.H.; Canonica, G.W.; Cao, H.; Chung, K.F.; Davies, D.E.; Genton, C.; Gibson-Latimer, T.; et al. The Severe Heterogeneous Asthma Research collaboration, Patient-centred (SHARP) ERS Clinical Research Collaboration: A new dawn in asthma research. Eur. Respir. J. 2018, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samitas, K.; Zervas, E.; Gaga, M. T2-low asthma: Current approach to diagnosis and therapy. Curr. Opin. Pulm. Med. 2017, 23, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Colley, T.; Mercado, N.; Kunori, Y.; Brightling, C.; Bhavsar, P.K.; Barnes, P.J.; Ito, K. Defective sirtuin-1 increases IL-4 expression through acetylation of GATA-3 in patients with severe asthma. J. Allergy Clin. Immunol. 2016, 137, 1595–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.; Chen, Q.; Meng, Z.; Sun, L.; Zhu, L.; Liu, J.; Hu, J.; Ni, Z.; Wang, X. Suppression of Sirtuin-1 Increases IL-6 Expression by Activation of the Akt Pathway During Allergic Asthma. Cell Physiol. Biochem. 2017, 43, 1950–1960. [Google Scholar] [CrossRef]
- Ichikawa, T.; Hayashi, R.; Suzuki, K.; Imanishi, S.; Kambara, K.; Okazawa, S.; Inomata, M.; Yamada, T.; Yamazaki, Y.; Koshimizu, Y.; et al. Sirtuin 1 activator SRT1720 suppresses inflammation in an ovalbumin-induced mouse model of asthma. Respirology 2013, 18, 332–339. [Google Scholar] [CrossRef]
- Wang, M.; Xu, Y.; Liu, J.; Ye, J.; Yuan, W.; Jiang, H.; Wang, Z.; Wan, J. Recent Insights into the Biological Functions of Sestrins in Health and Disease. Cell Physiol. Biochem. 2017, 43, 1731–1741. [Google Scholar] [CrossRef]
- Budanov, A.V.; Lee, J.H.; Karin, M. Stressin’ Sestrins take an aging fight. EMBO Mol. Med. 2010, 2, 388–400. [Google Scholar] [CrossRef]
- Lassalle, P.; Molet, S.; Janin, A.; Heyden, J.V.; Tavernier, J.; Fiers, W.; Devos, R.; Tonnel, A.B. ESM-1 is a novel human endothelial cell-specific molecule expressed in lung and regulated by cytokines. J. Biol. Chem. 1996, 271, 20458–20464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Mohsen, A.H.; Allam, E. Relationship between Serum Level of Endocan and Severity of Childhood Asthma. Egypt. J. Immunol. 2018, 25, 135–142. [Google Scholar] [PubMed]
- Global Initiative for Asthma 2016: Updated from Global Strategy for Asthma Management and Prevention. Workshop Report 2016. Available online: www.ginasthma.com (accessed on 9 February 2020).
- Kips, J.C.; Fahy, J.V.; Hargreave, F.E.; Ind, P.W.; in’t Veen, J.C. Methods for sputum induction and analysis of induced sputum: A method for assessing airway inflammation in asthma. Eur. Respir. J. Suppl. 1998, 26, 9S–12S. [Google Scholar] [PubMed]
- Grootendorst, D.C.; van den Bos, J.W.; Romeijn, J.J.; Veselic-Charvat, M.; Duiverman, E.J.; Vrijlandt, E.J.; Sterk, P.J.; Roldaan, A.C. Induced sputum in adolescents with severe stable asthma. Safety and the relationship of cell counts and eosinophil cationic protein to clinical severity. Eur. Respir. J. 1999, 13, 647–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Thoracic Society. Standardization of Spirometry, 1994 Update. Am. J. Respir. Crit. Care Med. 1995, 152, 1107–1136. [Google Scholar] [CrossRef]
- Yanagisawa, S.; Papaioannou, A.I.; Papaporfyriou, A.; Baker, J.R.; Vuppusetty, C.; Loukides, S.; Barnes, P.J.; Ito, K. Decreased Serum Sirtuin-1 in COPD. Chest 2017, 152, 343–352. [Google Scholar] [CrossRef] [Green Version]
- Kechagia, M.; Michalakakou, K.; Griniouk, K.; Piante, A.; Karagiannidis, N.; Filaditaki, V.; Daniil, Z.; Papassotiriou, I.; Gourgoulianis, K.I. Serum endocan levels in patients with chronic obstructive pulmonary disease: A potential role in the evaluation of susceptibility to exacerbation. Clin. Chem. Lab. Med. 2018, 56, e295–e297. [Google Scholar] [CrossRef]
- Kanazawa, H.; Nomura, S.; Yoshikawa, J. Role of microvascular permeability on physiologic differences in asthma and eosinophilic bronchitis. Am. J. Respir. Crit. Care Med. 2004, 169, 1125–1130. [Google Scholar] [CrossRef]
- Hoshino, M.; Takahashi, M.; Aoike, N. Expression of vascular endothelial growth factor, basic fibroblast growth factor, and angiogenin immunoreactivity in asthmatic airways and its relationship to angiogenesis. J. Allergy Clin. Immunol. 2001, 107, 295–301. [Google Scholar] [CrossRef]
- Ma, K.; Lu, N.; Zou, F.; Meng, F.Z. Sirtuins as novel targets in the pathogenesis of airway inflammation in bronchial asthma. Eur. J. Pharmacol. 2019, 865, 172670. [Google Scholar] [CrossRef]
- Legutko, A.; Marichal, T.; Fievez, L.; Bedoret, D.; Mayer, A.; de Vries, H.; Klotz, L.; Drion, P.V.; Heirman, C.; Cataldo, D.; et al. Sirtuin 1 promotes Th2 responses and airway allergy by repressing peroxisome proliferator-activated receptor-gamma activity in dendritic cells. J. Immunol. 2011, 187, 4517–4529. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.R.; Lee, K.S.; Park, S.J.; Min, K.H.; Choe, Y.H.; Moon, H.; Yoo, W.H.; Chae, H.J.; Han, M.K.; Lee, Y.C. Involvement of sirtuin 1 in airway inflammation and hyperresponsiveness of allergic airway disease. J. Allergy Clin. Immunol. 2010, 125, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Chen, C.; Hu, X.; Du, X.; Zhai, H.; Fang, Y.; Ye, X.; Yang, W.; Sun, S. Sestrin2 is involved in asthma: A case-control study. Allergy Asthma Clin. Immunol. 2019, 15, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wempe, F.; De-Zolt, S.; Koli, K.; Bangsow, T.; Parajuli, N.; Dumitrascu, R.; Sterner-Kock, A.; Weissmann, N.; Keski-Oja, J.; von Melchner, H. Inactivation of sestrin 2 induces TGF-beta signaling and partially rescues pulmonary emphysema in a mouse model of COPD. Dis. Model. Mech. 2010, 3, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Heidler, J.; Fysikopoulos, A.; Wempe, F.; Seimetz, M.; Bangsow, T.; Tomasovic, A.; Veit, F.; Scheibe, S.; Pichl, A.; Weisel, F.; et al. Sestrin-2, a repressor of PDGFR beta signalling, promotes cigarette-smoke-induced pulmonary emphysema in mice and is upregulated in individuals with COPD. Dis. Model. Mech. 2013, 6, 1378–1387. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All n = 60 | Mild to Moderate Asthma n = 25 | Severe Asthma n = 35 | p-Value* |
|---|---|---|---|---|
| Age | 54 ± 13 | 56 ± 14 | 54 ± 13 | 0.876 |
| Gender F/M | 44/16 | 18/7 | 26/9 | 0.466 |
| Atopy | 24 | 11 | 13 | 0.186 |
| Smoking | 12 | 5 | 4 | ND |
| BMI kg/m2 | 27 ± 5 | 26 ± 4 | 27 ± 6 | 0.435 |
| FEV1 % | 83 ± 23 | 92 ± 21 | 77 ± 22 | 0.011 |
| FEV1/FVC | 73 ± 13 | 75 ± 9 | 71 ± 15 | 0.136 |
| Neutrophils %IS | 16(3,29) | 9(2,25) | 19(3,38) | 0.021 |
| Eosinophils % IS | 1(0,6) | 1(0,2) | 3(2,7) | 0.031 |
| Treatment | 60 | 25 | 35 | ND |
| ICS | 35 | 0 | 35 | |
| High doses ICS ^ | ||||
| LABA | 56 | 23 | 33 | |
| LAMA | 13 | 0 | 13 | |
| LTRAs | 17 | 7 | 10 | |
| Omalizumab | 5 | 0 | 5 | |
| Mepolizumab | 6 | 0 | 6 | |
| Oral Cs ^^ | 8 | 0 | 8 |
| Variables | Mild to Moderate Asthma | Severe Asthma | p-Value |
|---|---|---|---|
| Endocan | |||
| Serum pg/mL | 15 (11, 29) | 21 (10, 34) | 0.315 |
| Sputum supernatant pg/mL | 28 (25, 35) | 29 (24, 34) | 0.976 |
| Sestrin | |||
| Serum pg/mL | 2645 (927, 3928) | 1745 (1090, 3496) | 0.519 |
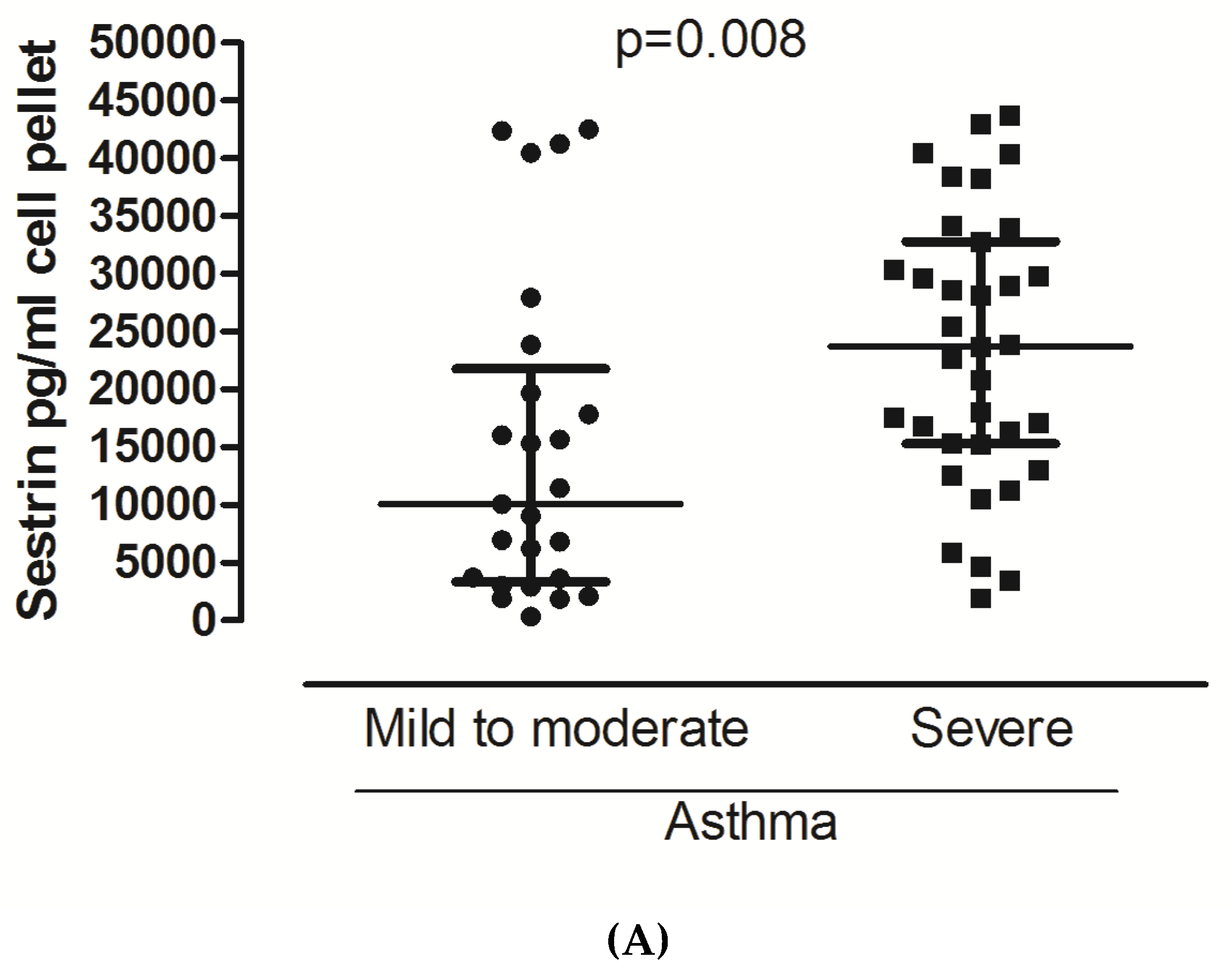
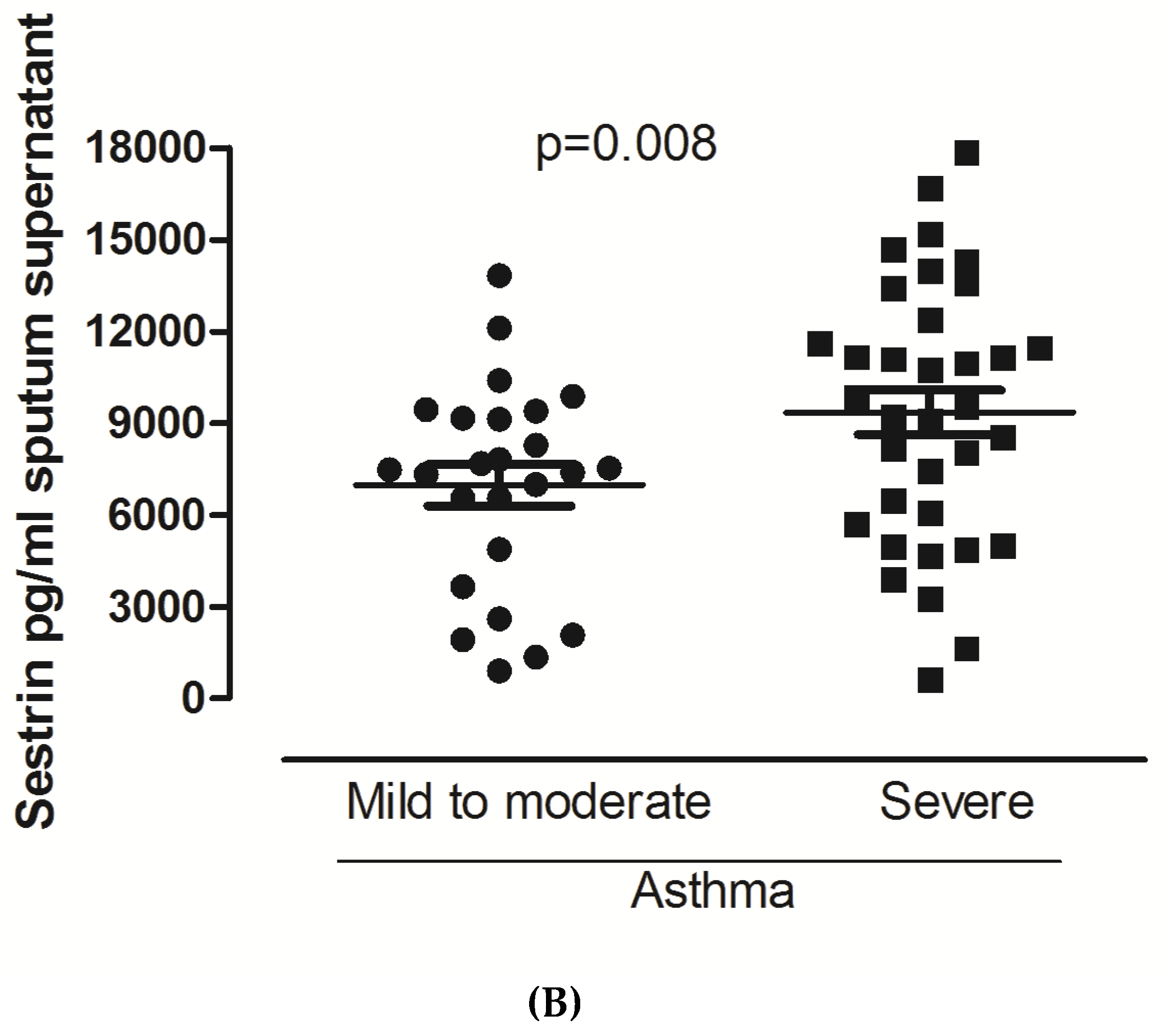
| Sputum supernatant pg/mL | 7476 (4265, 9273) | 9524 (5696, 12,373) | 0.029 |
| Cell pellet pg/mL | 10,084 (3349, 21,784) | 23,748 (15,280, 32,742) | 0.008 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsilogianni, Z.; Baker, J.R.; Papaporfyriou, A.; Papaioannou, A.I.; Papathanasiou, E.; Koulouris, N.G.; Daly, L.; Ito, K.; Hillas, G.; Papiris, S.; et al. Sirtuin 1: Endocan and Sestrin 2 in Different Biological Samples in Patients with Asthma. Does Severity Make the Difference? J. Clin. Med. 2020, 9, 473. https://doi.org/10.3390/jcm9020473
Tsilogianni Z, Baker JR, Papaporfyriou A, Papaioannou AI, Papathanasiou E, Koulouris NG, Daly L, Ito K, Hillas G, Papiris S, et al. Sirtuin 1: Endocan and Sestrin 2 in Different Biological Samples in Patients with Asthma. Does Severity Make the Difference? Journal of Clinical Medicine. 2020; 9(2):473. https://doi.org/10.3390/jcm9020473
Chicago/Turabian StyleTsilogianni, Zoe, Jonathan R Baker, Anastasia Papaporfyriou, Andrianna I Papaioannou, Evgenia Papathanasiou, Nikolaos G Koulouris, Leah Daly, Kazuhiro Ito, Georgios Hillas, Spyridon Papiris, and et al. 2020. "Sirtuin 1: Endocan and Sestrin 2 in Different Biological Samples in Patients with Asthma. Does Severity Make the Difference?" Journal of Clinical Medicine 9, no. 2: 473. https://doi.org/10.3390/jcm9020473
APA StyleTsilogianni, Z., Baker, J. R., Papaporfyriou, A., Papaioannou, A. I., Papathanasiou, E., Koulouris, N. G., Daly, L., Ito, K., Hillas, G., Papiris, S., Bakakos, P., & Loukides, S. (2020). Sirtuin 1: Endocan and Sestrin 2 in Different Biological Samples in Patients with Asthma. Does Severity Make the Difference? Journal of Clinical Medicine, 9(2), 473. https://doi.org/10.3390/jcm9020473