Antibiofilm and Immune Response of Engineered Bioactive Nanoparticles for Endodontic Disinfection

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Phase-1: Characterization of Post-Disinfection Biofilm Model
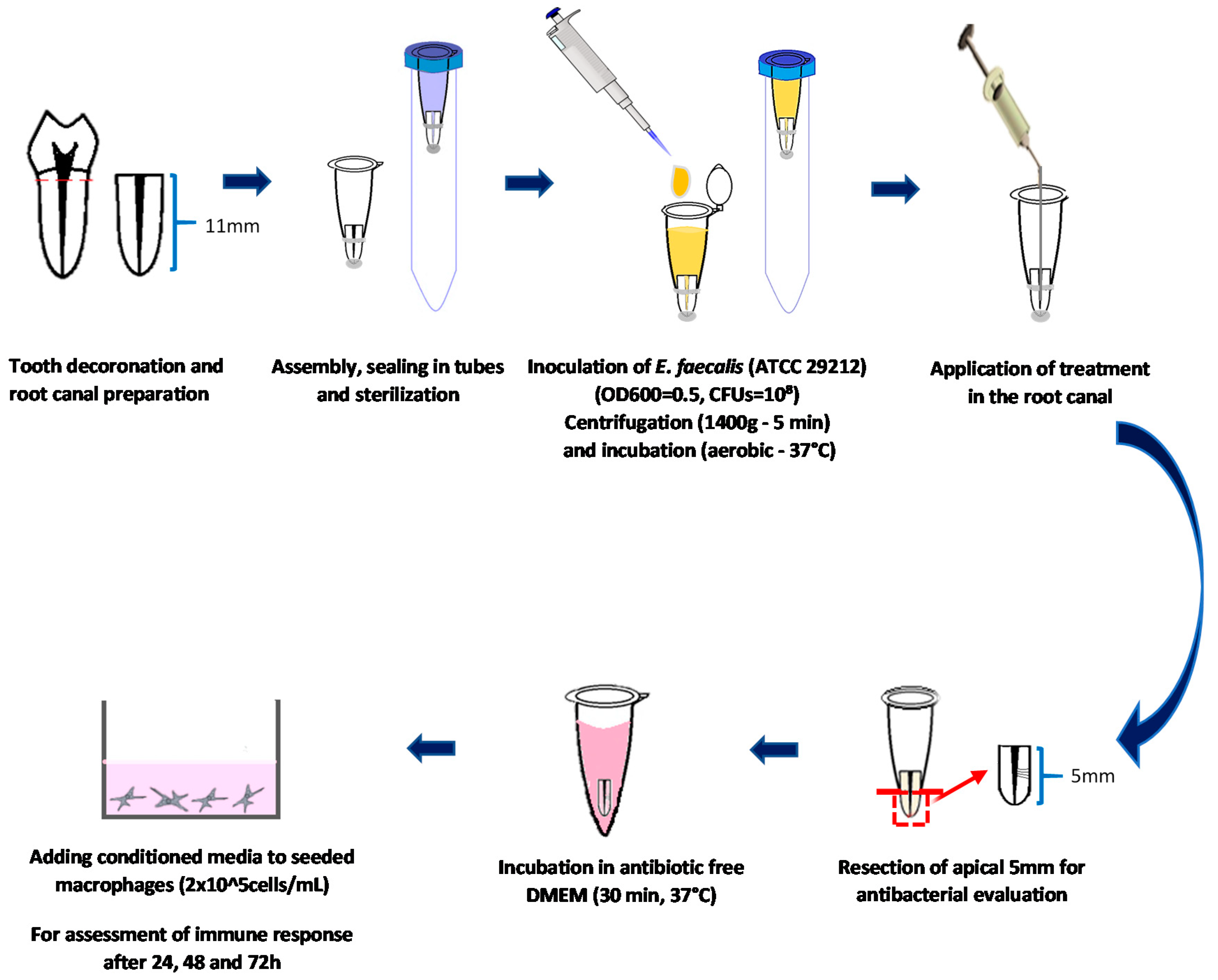
2.1.1. Teeth Selection and Preparation
2.1.2. Mono-Species Biofilm Formation
2.1.3. Disinfection Procedures
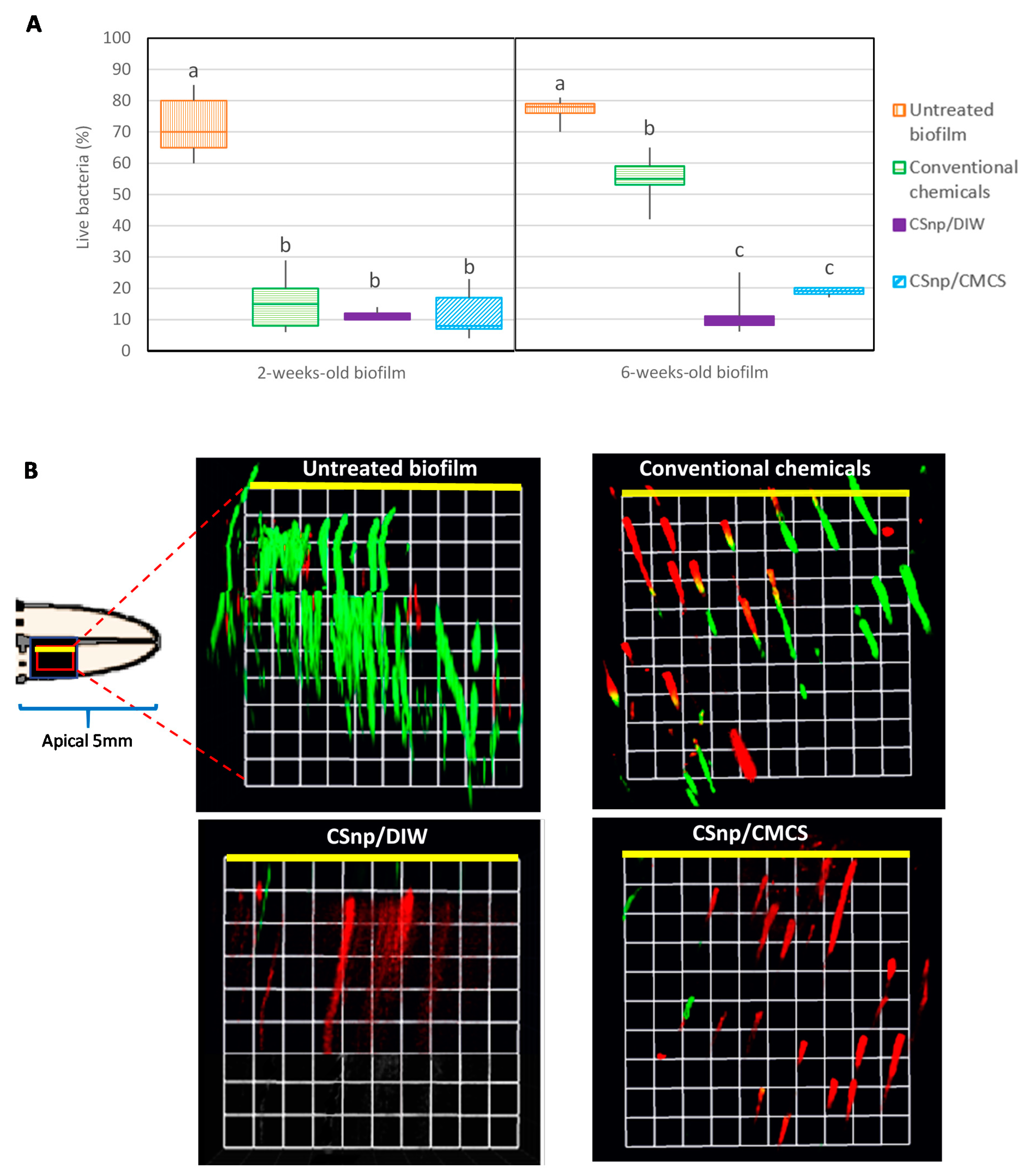
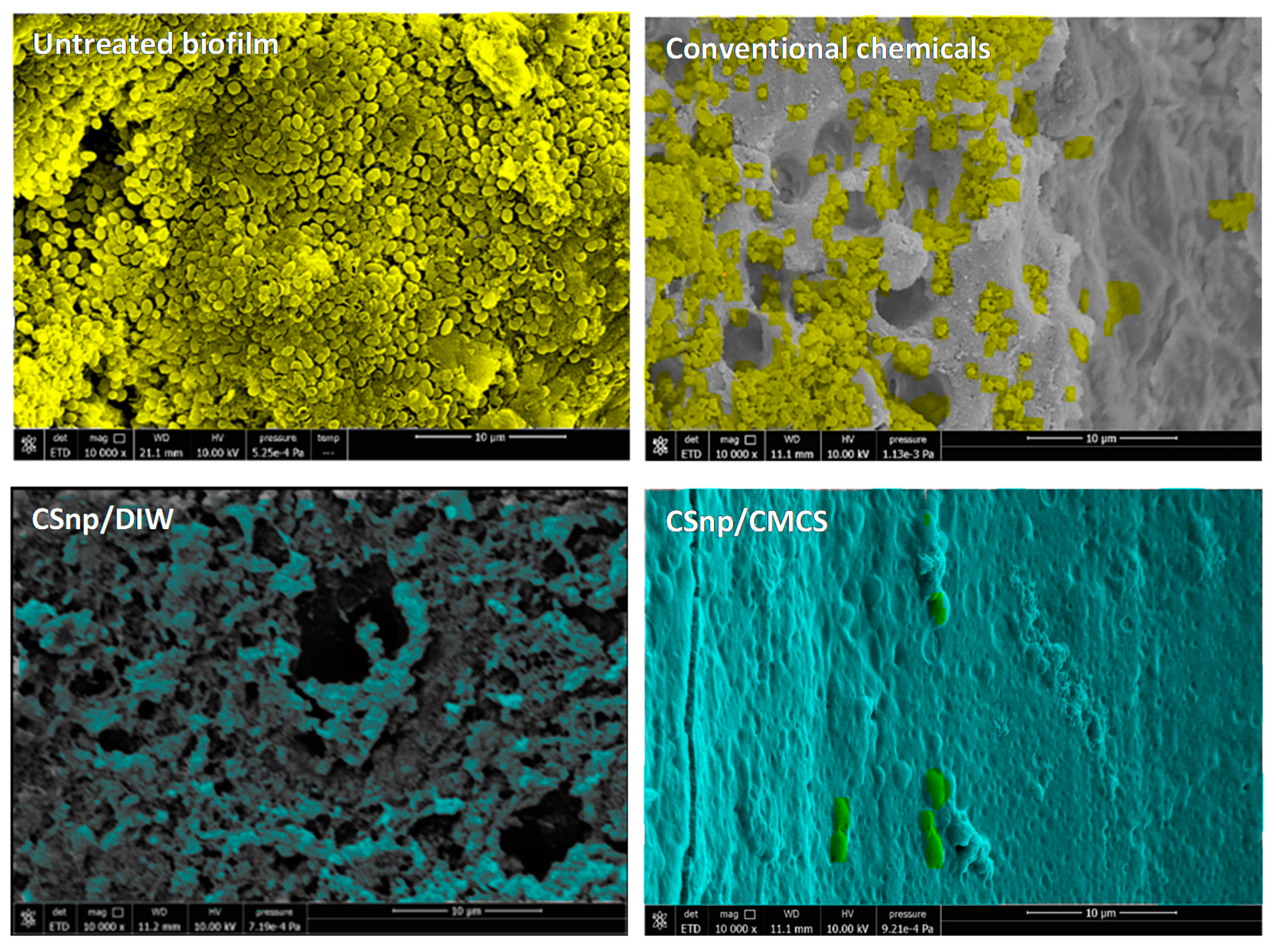
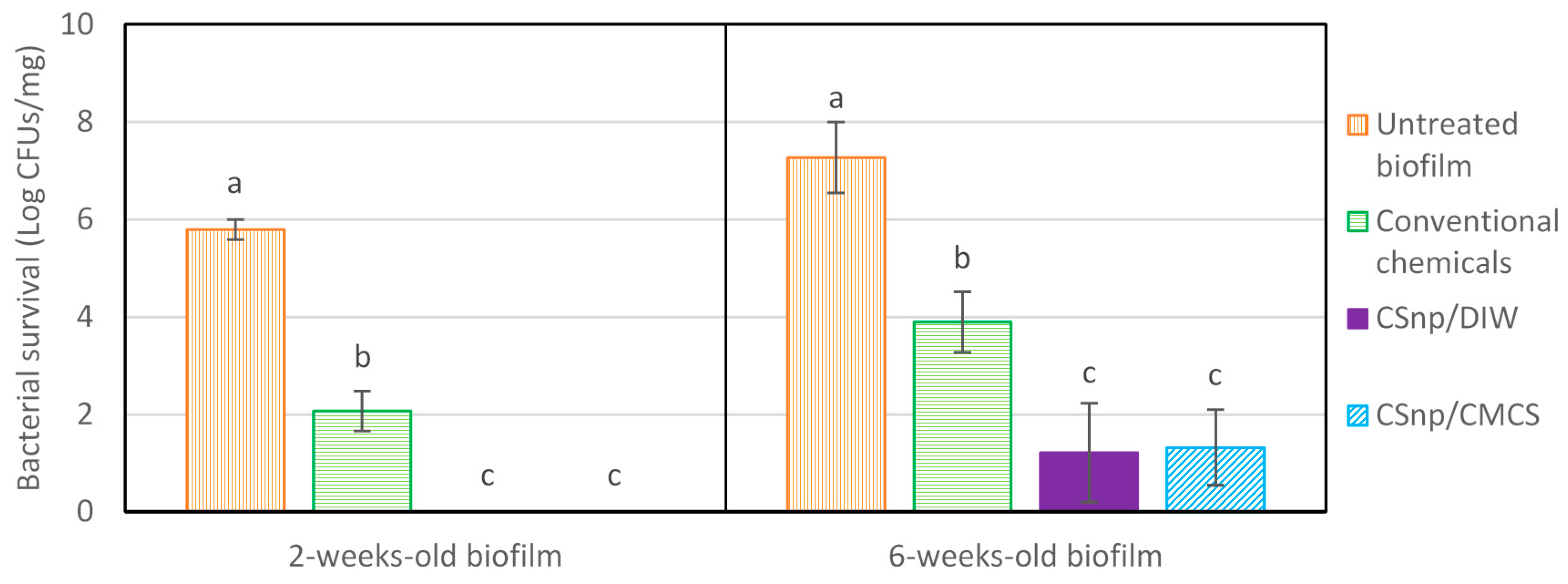
2.1.4. Evaluation of Antimicrobial Efficacy
2.2. Phase-2: Interaction of Engineered Nanoparticles Treated Biofilm and Macrophages
2.2.1. Cell Culture
2.2.2. Interaction of Treated Biofilm and Macrophages Cell Culture
2.3. Statistical Analysis
3. Results
3.1. Phase-1: Characterization of Post-Disinfection Biofilm Model
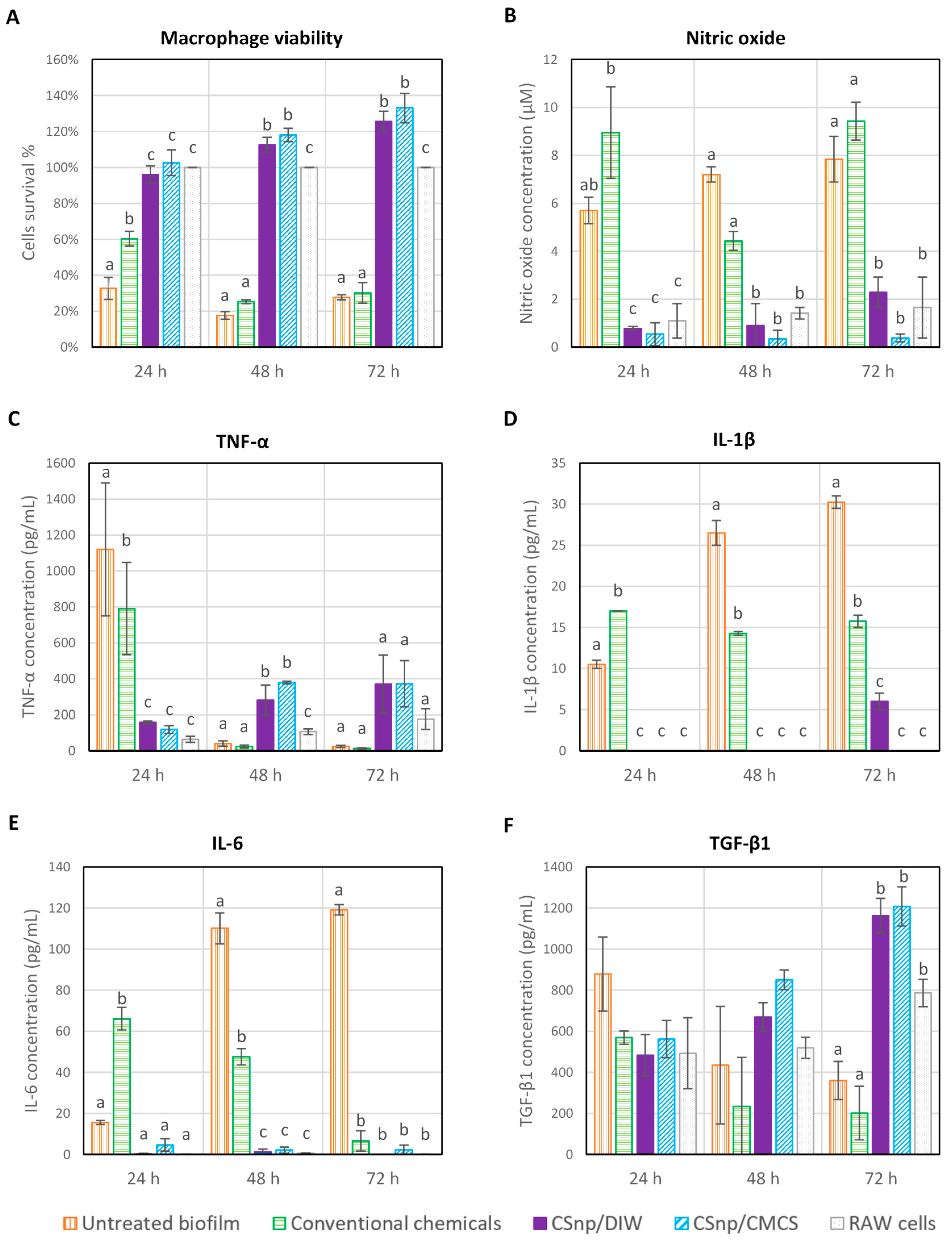
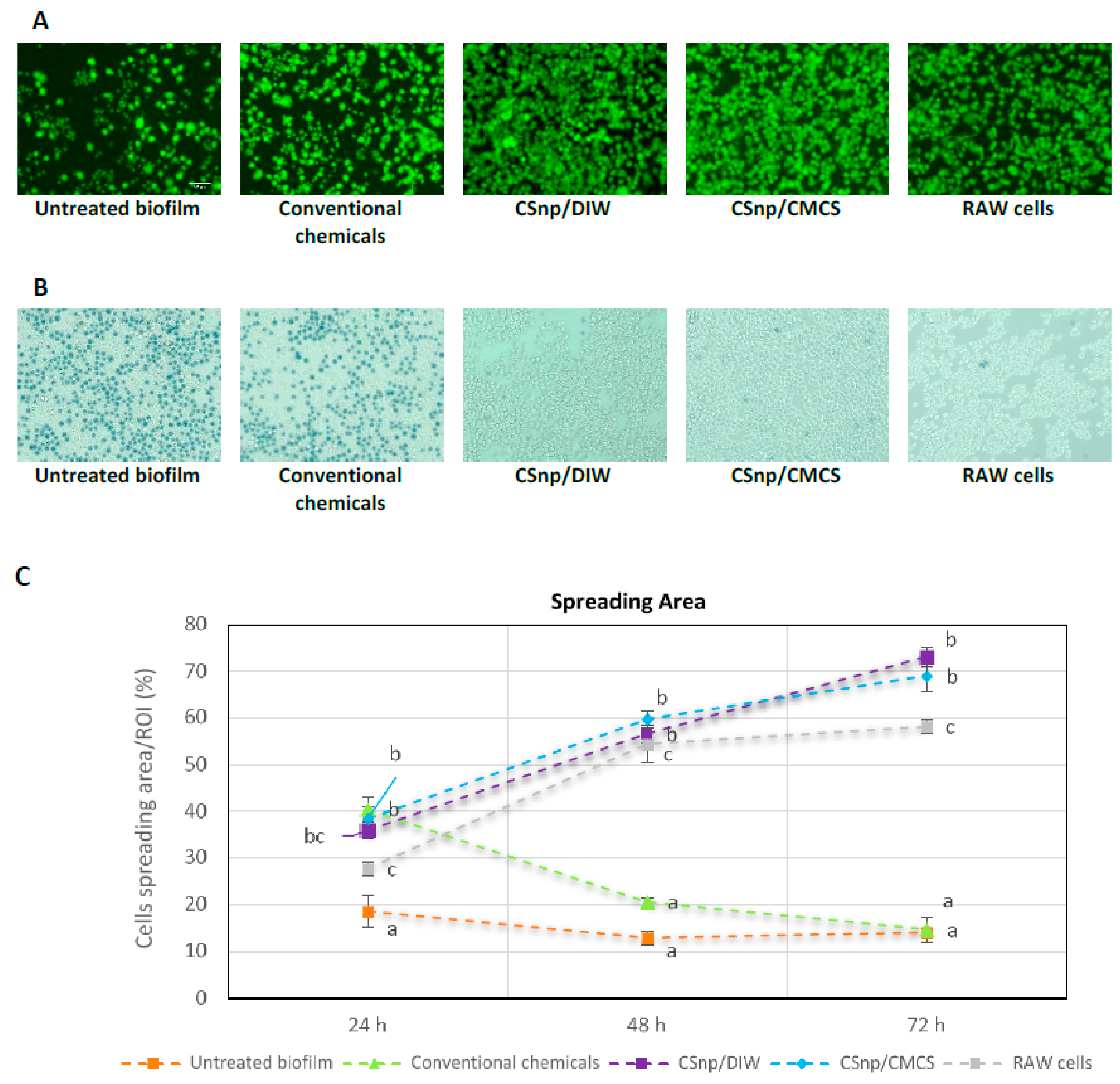
3.2. Phase 2: Interaction of Nanoparticles Treated Biofilm and Macrophages
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lin, L.M.; Rosenberg, P.A. Repair and regeneration in endodontics. Int. Endod. J. 2011, 44, 889–906. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.N. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.N. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit. Rev. Oral Biol. Med. 2004, 15, 348–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siqueira JR, J.F.; Rôças, I.N. Present status and future directions in endodontic microbiology. Endod. Top. 2014, 30, 3–22. [Google Scholar] [CrossRef]
- Bystrom, A.; Sundqvist, G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int. Endod. J. 1985, 18, 35–40. [Google Scholar] [CrossRef]
- Sundqvist, G.; Figdor, D. Life as an endodontic pathogen. Endod. Top. 2003, 6, 3–28. [Google Scholar] [CrossRef]
- Chávez de Paz, L.E. Aetiology of persistent endodontic infections in root-filled teeth. In Apical Periodontitis in Root-Filled Teeth: Endodontic Retreatment and Alternative Approaches, 1st ed.; Kvist, T., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 21–32. [Google Scholar]
- Qie, Y.; Yuan, H.; von Roemeling, C.A.; Chen, Y.; Liu, X.; Shih, K.D.; Knight, J.A.; Tun, H.W.; Wharen, R.E.; Jiang, W.; et al. Surface modification of nanoparticles enables selective evasion of phagocytic clearance by distinct macrophage phenotypes. Sci. Rep. 2016, 6, 26269. [Google Scholar] [CrossRef]
- Stashenko, P. Role of immune cytokines in the pathogenesis of periapical lesions. Endod. Dent. Traumatol. 1990, 6, 89–96. [Google Scholar] [CrossRef]
- Márton, I.J.; Kiss, C. Protective and destructive immune reactions in apical periodontitis. Oral Microbiol. Immunol. 2000, 15, 139–150. [Google Scholar] [CrossRef]
- Makvandi, P.; Gu, J.T.; Zare, E.N.; Ashtari, B.; Moeini, A.; Tay, F.R.; Niu, L.N. Polymeric and inorganic nanoscopical antimicrobial fillers in dentistry. Acta Biomater. 2020, 101, 69–101. [Google Scholar] [CrossRef]
- Samiei, M.; Farjami, A.; Dizaj, S.M.; Lotfipour, F. Nanoparticles for antimicrobial purposes in Endodontics: A systematic review of in vitro studies. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 58, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Kishen, A.; Shi, Z.; Shrestha, A.; Neoh, K.G. An investigation on the antibacterial and antibiofilm efficacy of cationic nanoparticulates for root canal disinfection. J. Endod. 2008, 34, 1515–1520. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Shi, Z.; Neoh, K.G.; Kishen, A. Nanoparticulates for antibiofilm treatment and effect of aging on its antibacterial activity. J. Endod. 2010, 36, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Kishen, A. Antibiofilm efficacy of photosensitizer-functionalized bioactive nanoparticles on multispecies biofilm. J. Endod. 2014, 40, 1604–1610. [Google Scholar] [CrossRef]
- Shrestha, A.; Cordova, M.; Kishen, A. Photoactivated polycationic bioactive chitosan nanoparticles inactivate bacterial endotoxins. J. Endod. 2015, 41, 686–691. [Google Scholar] [CrossRef]
- Mourya, V.; Inamdar, N.; Tiwari, A. Carboxymethyl chitosan and its applications. Adv. Mater. Lett. 2010, 1, 11–33. [Google Scholar] [CrossRef]
- Bellamy, C.; Shrestha, S.; Torneck, C.; Kishen, A. Effects of a bioactive scaffold containing a sustained transforming growth factor-β1-releasing nanoparticle system on the migration and differentiation of Stem cells from the apical papilla. J. Endod. 2016, 42, 1385–1392. [Google Scholar] [CrossRef]
- Shrestha, S.; Diogenes, A.; Kishen, A. Temporal-controlled dexamethasone releasing chitosan nanoparticle system enhances odontogenic differentiation of stem cells from apical papilla. J. Endod. 2015, 41, 1253–1258. [Google Scholar] [CrossRef]
- Ma, J.; Wang, Z.; Shen, Y.; Haapasalo, M. A new noninvasive model to study the effectiveness of dentin disinfection by using confocal laser scanning microscopy. J. Endod. 2011, 37, 1380–1385. [Google Scholar] [CrossRef]
- Kishen, A.; Haapasalo, M. Biofilm models and methods of biofilm assessment. Endod. Top. 2012, 22, 58–78. [Google Scholar] [CrossRef]
- Cheung, G.S.; Ho, M.W. Microbial flora of root canal-treated teeth associated with asymptomatic periapical radiolucent lesions. Oral Microbiol. Immunol. 2001, 16, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Chavez de Paz, L.E. Redefining the persistent infection in root canals: Possible role of biofilm communities. J. Endod. 2007, 33, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Du, J.; Peng, Z. Correlation between Enterococcus faecalis and persistent intraradicular infection compared with primary intraradicular infection: A systematic review. J. Endod. 2015, 41, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.; Davies, J.K.; Sundqvist, G.; Figdor, D. Mechanisms involved in the resistance of Enterococcus faecalis to calcium hydroxide. Int. Endod. J. 2002, 35, 221–228. [Google Scholar] [CrossRef]
- Kishen, A.; George, S.; Kumar, R. Enterococcus faecalis-mediated biomineralized biofilm formation on root canal dentine in vitro. J. Biomed. Mater. Res. A 2006, 77, 406–415. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Shalavi, S.; Yazdizadeh, M. Antimicrobial activity of calcium hydroxide in endodontics: A review. Chonnam. Med. J. 2012, 48, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Shen, Y.; Yang, Y.; Gao, Y.; Wan, P.; Gan, Y.; Patel, P.; Curtis, A.; Khakpour, M.; Haapasalo, M. In vitro study of calcium hydroxide removal from mandibular molar root canals. J. Endod. 2015, 41, 553–558. [Google Scholar] [CrossRef]
- Silva, L.J.; Pessoa, O.F.; Teixeira, M.B.; Gouveia, C.H.; Braga, R.R. Micro-CT evaluation of calcium hydroxide removal through passive ultrasonic irrigation associated with or without an additional instrument. Int. Endod. J. 2015, 48, 768–773. [Google Scholar] [CrossRef]
- Goldberg, F.; Alfie, D.; Roitman, M. Evaluation of the incidence of transportation after placement and removal of calcium hydroxide. J. Endod. 2004, 30, 646–648. [Google Scholar] [CrossRef]
- Shrestha, A.; Kishen, A. The effect of tissue inhibitors on the antibacterial activity of chitosan nanoparticles and photodynamic therapy. J. Endod. 2012, 38, 1275–1278. [Google Scholar] [CrossRef]
- Kishen, A.; Shrestha, A.; Del Carpio-Perochena, A. Validation of biofilm assays to assess antibiofilm efficacy in instrumented root canals after syringe irrigation and sonic agitation. J. Endod. 2018, 44, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Tran, K.T.; Torabinejad, M.; Shabahang, S.; Retamozo, B.; Aprecio, R.M.; Chen, J.W. Comparison of efficacy of pulverization and sterile paper point techniques for sampling root canals. J. Endod. 2013, 39, 1057–1059. [Google Scholar] [CrossRef] [PubMed]
- Kho, P.; Baumgartner, J.C. A comparison of the antimicrobial efficacy of NaOCl/Biopure MTAD versus NaOCl/EDTA against Enterococcus faecalis. J. Endod. 2006, 32, 652–655. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Kishen, A. Photophysical, photochemical, and photobiological characterization of methylene blue formulations for light-activated root canal disinfection. J. Biomed. Opt. 2007, 12, 034029. [Google Scholar] [CrossRef]
- Stojicic, S.; Shen, Y.; Haapasalo, M. Effect of the source of biofilm bacteria, level of biofilm maturation, and type of disinfecting agent on the susceptibility of biofilm bacteria to antibacterial agents. J. Endod. 2013, 39, 473–477. [Google Scholar] [CrossRef]
- Lima, S.M.; Sousa, M.G.; Freire, M.e.S.; de Almeida, J.A.; Cantuária, A.P.; Silva, T.A.; de Freitas, C.G.; Dias, S.C.; Franco, O.L.; Rezende, T.M. Immune response profile against persistent endodontic pathogens Candida albicans and Enterococcus faecalis in vitro. J. Endod. 2015, 41, 1061–1065. [Google Scholar] [CrossRef]
- Rabea, E.I.; Badawy, M.E.; Stevens, C.V.; Smagghe, G.; Steurbaut, W. Chitosan as antimicrobial agent: Applications and mode of action. Biomacromolecules 2003, 4, 1457–1465. [Google Scholar] [CrossRef]
- Jiang, L.Q.; Wang, T.Y.; Webster, T.J.; Duan, H.J.; Qiu, J.Y.; Zhao, Z.M.; Yin, X.X.; Zheng, C.L. Intracellular disposition of chitosan nanoparticles in macrophages: Intracellular uptake, exocytosis, and intercellular transport. Int. J. Nanomed. 2017, 12, 6383–6398. [Google Scholar] [CrossRef] [Green Version]
- Nair, P.N. Apical periodontitis: A dynamic encounter between root canal infection and host response. Periodontology 2000 1997, 13, 121–148. [Google Scholar] [CrossRef]
- Mathew, S.; Yaw-Chyn, L.; Kishen, A. Immunogenic potential of Enterococcus faecalis biofilm under simulated growth conditions. J. Endod. 2010, 36, 832–836. [Google Scholar] [CrossRef]
- Ozbey, G.; Gorczynski, R.; Erin, N. Stability of cytokines in supernatants of stimulated mouse immune cells. Eur. Cytokine Netw. 2014, 25, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Colić, M.; Gazivoda, D.; Vucević, D.; Vasilijić, S.; Rudolf, R.; Lukić, A. Proinflammatory and immunoregulatory mechanisms in periapical lesions. Mol. Immunol. 2009, 47, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Kishen, A.; Shrestha, S.; Shrestha, A.; Cheng, C.; Goh, C. Characterizing the collagen stabilizing effect of crosslinked chitosan nanoparticles against collagenase degradation. Dent. Mater. 2016, 32, 968–977. [Google Scholar] [CrossRef] [PubMed]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussein, H.; Kishen, A. Antibiofilm and Immune Response of Engineered Bioactive Nanoparticles for Endodontic Disinfection. J. Clin. Med. 2020, 9, 730. https://doi.org/10.3390/jcm9030730
Hussein H, Kishen A. Antibiofilm and Immune Response of Engineered Bioactive Nanoparticles for Endodontic Disinfection. Journal of Clinical Medicine. 2020; 9(3):730. https://doi.org/10.3390/jcm9030730
Chicago/Turabian StyleHussein, Hebatullah, and Anil Kishen. 2020. "Antibiofilm and Immune Response of Engineered Bioactive Nanoparticles for Endodontic Disinfection" Journal of Clinical Medicine 9, no. 3: 730. https://doi.org/10.3390/jcm9030730
APA StyleHussein, H., & Kishen, A. (2020). Antibiofilm and Immune Response of Engineered Bioactive Nanoparticles for Endodontic Disinfection. Journal of Clinical Medicine, 9(3), 730. https://doi.org/10.3390/jcm9030730