On-Treatment Decrease of Serum Interleukin-6 as a Predictor of Clinical Response to Biologic Therapy in Patients with Inflammatory Bowel Diseases

 ,
,  , , ,
, , ,  , ,
, ,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Measurement of Serum Zonulin, sCD163, and Cytokines
2.3. Outcomes
2.4. Statistical Analysis
3. Results
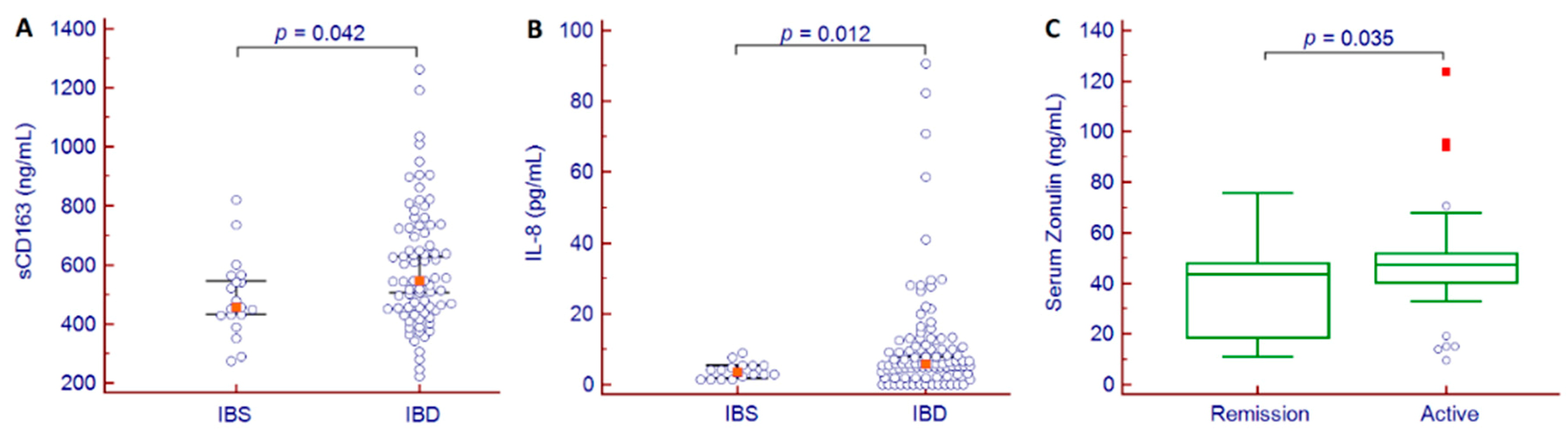
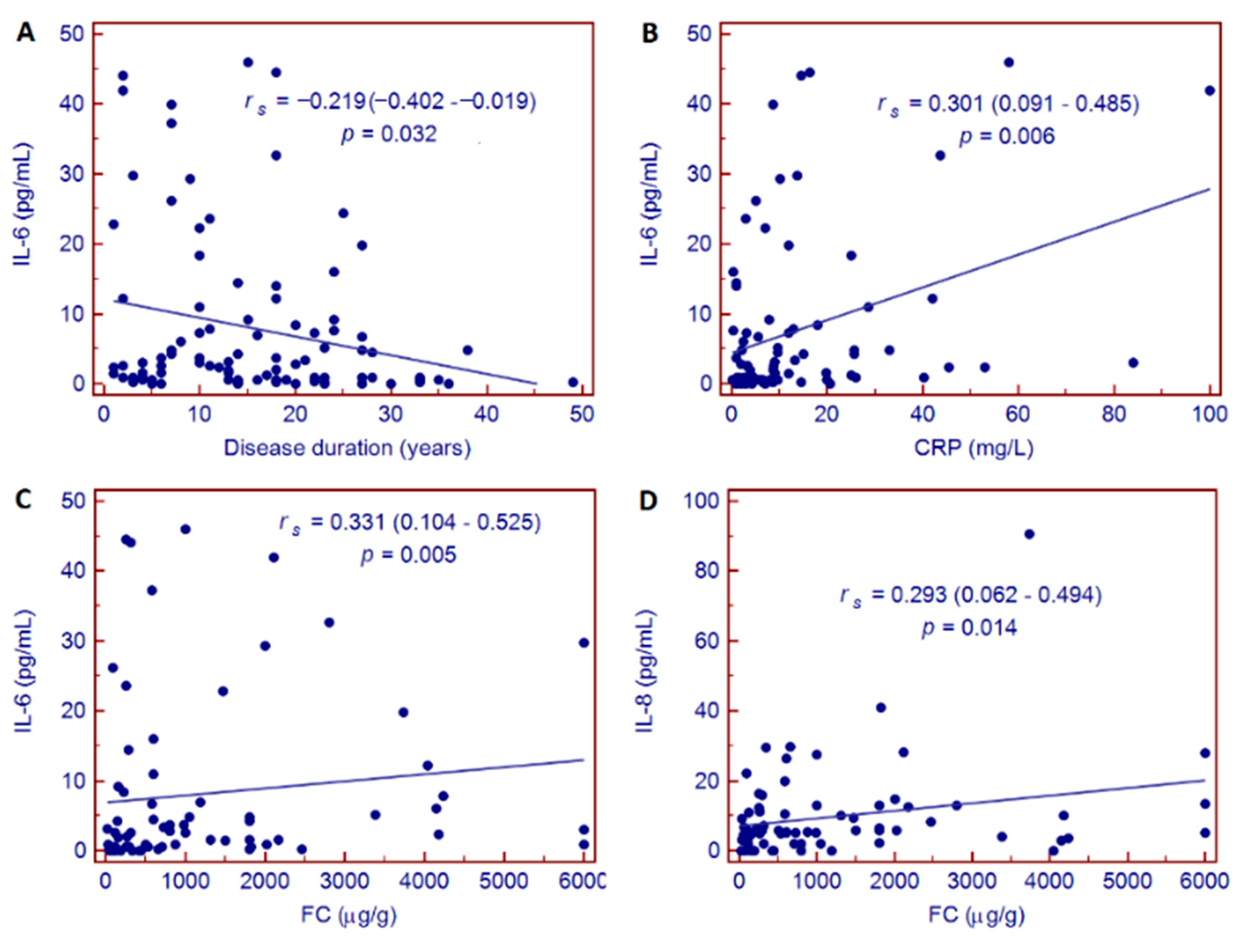
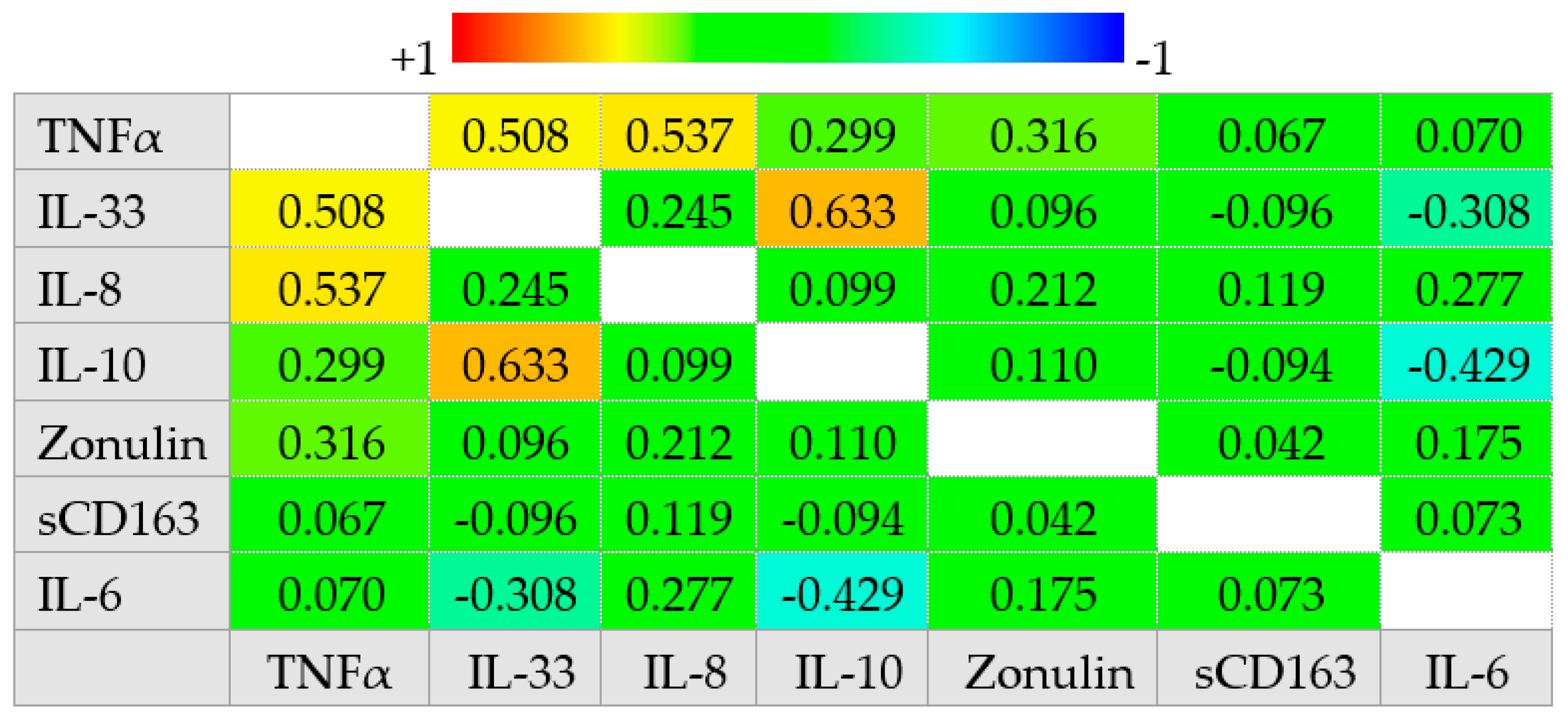
3.1. Cross-Sectional Analysis
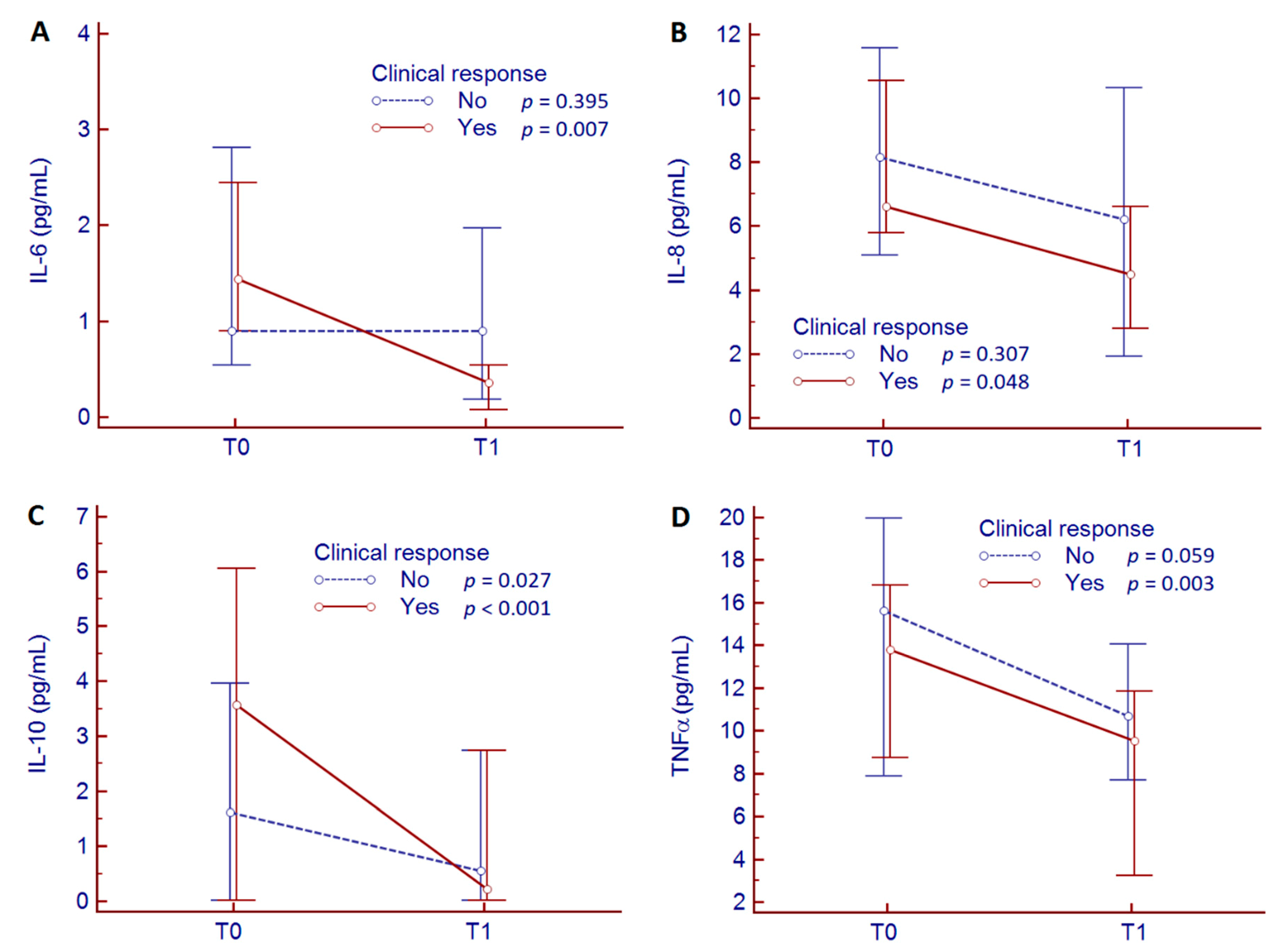
3.2. Longitudinal Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Gargallo, C.J.; Lué, A.; Gomollon, F. Biosimilars in inflammatory bowel disease. Minerva Med. 2017, 108, 239–254. [Google Scholar]
- Caviglia, G.P.; Rosso, C.; Ribaldone, D.G.; Dughera, F.; Fagoonee, S.; Astegiano, M.; Pellicano, R. Physiopathology of intestinal barrier and the role of zonulin. Minerva Biotecnol. 2019, 31, 83–92. [Google Scholar] [CrossRef]
- Khan, I.; Ullah, N.; Zha, L.; Bai, Y.; Khan, A.; Zhao, T.; Che, T.; Zhang, C. Alteration of Gut Microbiota in Inflammatory Bowel Disease (IBD): Cause or Consequence? IBD Treatment Targeting the Gut Microbiome. Pathogens 2019, 8, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Actis, G.C.; Pellicano, R.; Fagoonee, S.; Ribaldone, D.G. History of Inflammatory Bowel Diseases. J. Clin. Med. 2019, 8, 1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasano, A. Zonulin and its regulation of intestinal barrier function: The biological door to inflammation, autoimmunity, and cancer. Physiol. Rev. 2011, 91, 151–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Cheon, J.H. Pathogenesis of Inflammatory Bowel Disease and Recent Advances in Biologic Therapies. Immune Netw. 2017, 17, 25–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caviglia, G.P.; Dughera, F.; Ribaldone, D.G.; Rosso, C.; Abate, M.L.; Pellicano, R.; Bresso, F.; Smedile, A.; Saracco, G.M.; Astegiano, M. Serum zonulin in patients with inflammatory bowel disease: A pilot study. Minerva Med. 2019, 110, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, B.; Moraes, L.; Magnusson, M.K.; Öhman, L. Immunopathogenesis of inflammatory bowel disease and mechanisms of biological therapies. Scand. J. Gastroenterol. 2018, 53, 379–389. [Google Scholar] [CrossRef]
- Fasano, A. All disease begins in the (leaky) gut: Role of zonulin-mediated gut permeability in the pathogenesis of some chronic inflammatory diseases. F1000Research 2020, 9. [Google Scholar] [CrossRef]
- Dige, A.; Støy, S.; Thomsen, K.L.; Hvas, C.L.; Agnholt, J.; Dahlerup, J.F.; Møller, H.J.; Grønbaek, H. Soluble CD163, a specific macrophage activation marker, is decreased by anti-TNF-α antibody treatment in active inflammatory bowel disease. Scand. J. Immunol. 2014, 80, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, P.; Neurath, M.F.; Ng, S.C.; El-Omar, E.M.; Sharara, A.I.; Kobayashi, T.; Hisamatsu, T.; Hibi, T.; Rogler, G. Mechanism-Based Treatment Strategies for IBD: Cytokines, Cell Adhesion Molecules, JAK Inhibitors, Gut Flora, and More. Inflamm. Intest. Dis. 2019, 4, 79–96. [Google Scholar] [CrossRef] [PubMed]
- Kayal, M.; Shah, S. Ulcerative Colitis: Current and Emerging Treatment Strategies. J. Clin. Med. 2020, 9, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, D.R.; Colombel, J.F.; Ungaro, R. The Role of Early Biologic Therapy in Inflammatory Bowel Disease. Inflamm. Bowel. Dis. 2019, 25, 1896–1905. [Google Scholar] [CrossRef]
- Yanai, H.; Hanauer, S.B. Assessing response and loss of response to biological therapies in IBD. Am. J. Gastroenterol. 2011, 106, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 1: Definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders. J. Crohns Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: Part 1: Diagnosis and medical management. J. Crohn Colitis 2017, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, M.S.; Satsangi, J.; Ahmad, T.; Arnott, I.D.; Bernstein, C.N.; Brant, S.R.; Caprilli, R.; Colombel, J.F.; Gasche, C.; Geboes, K.; et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: Report of a working party of the 2005 Montreal world congress of gastroenterology. Can. J. Gastroenterol. 2005, 19, 5–36. [Google Scholar] [CrossRef]
- Harvey, R.F.; Bradshaw, M.J. Measuring Crohn’s disease activity. Lancet 1980, 1, 1134–1135. [Google Scholar] [CrossRef]
- Lewis, J.D.; Chuai, S.; Nessel, L.; Lichtenstein, G.R.; Aberra, F.N.; Ellenberg, J.H. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm. Bowel. Dis. 2008, 14, 1660–1666. [Google Scholar] [CrossRef] [Green Version]
- Peyrin-Biroulet, L.; Sandborn, W.; Sands, B.E.; Reinisch, W.; Bemelman, W.; Bryant, R.V.; D’Haens, G.; Dotan, I.; Dubinsky, M.; Feagan, B.; et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. Am. J. Gastroenterol. 2015, 110. [Google Scholar] [CrossRef]
- Arrieta, M.C.; Madsen, K.; Doyle, J.; Meddings, J. Reducing small intestinal permeability attenuates colitis in the IL10 gene-deficient mouse. Gut 2009, 58, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, P.; Silvester, J.; Chen, X.; Xu, H.; Sawhney, V.; Rangan, V.; Iturrino, J.; Nee, J.; Duerksen, D.R.; Lembo, A. Serum zonulin is elevated in IBS and correlates with stool frequency in IBS-D. United Eur. Gastroenterol. J. 2019, 7, 709–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linsalata, M.; Riezzo, G.; D’Attoma, B.; Clemente, C.; Orlando, A.; Russo, F. Noninvasive biomarkers of gut barrier function identify two subtypes of patients suffering from diarrhoea predominant-IBS: A case-control study. BMC Gastroenterol. 2018, 18, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamada, N.; Hisamatsu, T.; Okamoto, S.; Chinen, H.; Kobayashi, T.; Sato, T.; Sakuraba, A.; Kitazume, M.T.; Sugita, A.; Koganei, K.; et al. Unique CD14 intestinal macrophages contribute to the pathogenesis of Crohn disease via IL-23/IFN-gamma axis. J. Clin. Investig. 2008, 118, 2269–2280. [Google Scholar]
- Wallace, K.L.; Zheng, L.B.; Kanazawa, Y.; Shih, D.Q. Immunopathology of inflammatory bowel disease. World J. Gastroenterol. 2014, 20, 6–21. [Google Scholar] [CrossRef]
- Huang, Y.; Chen, Z. Inflammatory bowel disease related innate immunity and adaptive immunity. Am. J. Transl. Res. 2016, 8, 2490–2497. [Google Scholar]
- Franzè, E.; Caruso, R.; Stolfi, C.; Sarra, M.; Cupi, M.L.; Caprioli, F.; Monteleone, I.; Zorzi, F.; De Nitto, D.; Colantoni, A.; et al. Lesional accumulation of CD163-expressing cells in the gut of patients with inflammatory bowel disease. PLoS ONE 2013, 8, e69839. [Google Scholar] [CrossRef]
- Marafini, I.; Sedda, S.; Dinallo, V.; Monteleone, G. Inflammatory cytokines: From discoveries to therapies in IBD. Expert. Opin. Biol. 2019, 19, 1207–1217. [Google Scholar] [CrossRef]
- Bertani, L.; Antonioli, L.; Fornai, M.; Tapete, G.; Baiano Svizzero, G.; Marchi, S.; Blandizzi, C.; Costa, F. Evaluation of cytokine levels as putative biomarkers to predict the pharmacological response to biologic therapy in inflammatory bowel diseases. Minerva Gastroenterol. Dietol. 2019, 65, 298–308. [Google Scholar] [CrossRef]
- Bertani, L.; Baglietto, L.; Antonioli, L.; Fornai, M.; Tapete, G.; Albano, E.; Ceccarelli, L.; Mumolo, M.G.; Pellegrini, C.; Lucenteforte, E.; et al. Assessment of serum cytokines predicts clinical and endoscopic outcomes to vedolizumab in ulcerative colitis patients. Br. J. Clin. Pharm. 2020. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Matsui, T.; Ito, H.; Ashida, T.; Nakamura, S.; Motoya, S.; Matsumoto, T.; Sato, N.; Ozaki, K.; Watanabe, M.; et al. Circulating Interleukin 6 and Albumin, and Infliximab Levels Are Good Predictors of Recovering Efficacy After Dose Escalation Infliximab Therapy in Patients with Loss of Response to Treatment for Crohn’s Disease: A Prospective Clinical Trial. Inflamm. Bowel. Dis. 2015, 21, 2114–2122. [Google Scholar] [CrossRef] [PubMed]
- Nishida, Y.; Hosomi, S.; Watanabe, K.; Watanabe, K.; Yukawa, T.; Otani, K.; Nagami, Y.; Tanaka, F.; Taira, K.; Kamata, N.; et al. Serum interleukin-6 level is associated with response to infliximab in ulcerative colitis. Scand. J. Gastroenterol. 2018, 53, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Wine, E.; Mack, D.R.; Hyams, J.; Otley, A.R.; Markowitz, J.; Crandall, W.V.; Leleiko, N.; Muise, A.M.; Griffiths, A.M.; Turner, D. Interleukin-6 is associated with steroid resistance and reflects disease activity in severe pediatric ulcerative colitis. J. Crohns Colitis 2013, 7, 916–922. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IBD (n = 101) | IBS (n = 19) | p-Value | |
|---|---|---|---|
| Age (years), median (range) | 48 (18–80) | 43 (18–69) | 0.067 |
| Gender (M/F) | 62/39 | 6/13 | 0.023 |
| Disease (CD/UC) | 72/29 | ||
| Montreal classification | |||
| CD (L1/L2/L3) | 24/4/43 | ||
| UC (E1/E2/E3) | 4/9/16 | ||
| Clinical activity | |||
| Remission | 27 | ||
| Mild | 40 | ||
| Moderate | 28 | ||
| Severe | 6 | ||
| Disease duration (years), median (range) | 14 (1–49) | ||
| Previous surgery (yes/no) | 48/53 | ||
| Smoke (current/never/ex) | 23/42/36 | ||
| Biochemical activity | |||
| FC (µg/g), median (95% CI) | 602 (395–997) | ||
| CRP (mg/L), median (95% CI) | 7.0 (5.0–9.0) | ||
| ESR (positive/negative/N/A) | 45/35/21 |
| IBD (n = 101) | IBS (n = 19) | p-Value | |
|---|---|---|---|
| Zonulin (ng/mL), median (95% CI) | 45.3 (43.5–47.8) | 43.3 (37.2–46.4) | 0.322 |
| sCD163 (ng/mL), median (95% CI) | 547 (506–629) | 456 (432–548) | 0.042 |
| IL-1β (pg/mL), median (95% CI) | n.q. | n.q. | |
| IL-4 (pg/mL), median (95% CI) | n.q. | n.q. | |
| IL-6 (pg/mL), median (95% CI) | 2.52 (1.43–4.27) | 4.23 (2.87–7.06) | 0.140 |
| IL-8 (pg/mL), median (95% CI) | 5.79 (5.15–7.96) | 3.47 (1.97–5.32) | 0.012 |
| IL-10 (pg/mL), median (95% CI) | 0.01 (0.01–1.12) | n.q. | |
| IL-12(p70) (pg/mL), median (95% CI) | n.q. | n.q. | |
| IL-17 (pg/mL), median (95% CI) | n.q. | n.q. | |
| IL-23 (pg/mL), median (95% CI) | n.q. | n.q. | |
| IL-33 (pg/mL), median (95% CI) | 0.18 (0.01–15.50) | n.q. | |
| IFNγ (pg/mL), median (95% CI) | n.q. | n.q. | |
| TNFα (pg/mL), median (95% CI) | 10.48 (8.30–14.21) | 5.69 (2.23–11.09) | 0.159 |
| n | T0 | T1 | p-Value | |
|---|---|---|---|---|
| Zonulin (ng/mL), median (95% CI) | 60 | 46.0 (43.4–49.3) | 45.6 (42.0–50.9) | 0.722 |
| Responders | 32 | 44.2 (41.8–48.0) | 43.1 (39.4–50.2) | 0.981 |
| Non-responders | 28 | 48.6 (43.3–53.4) | 48.7 (42.1–54.0) | 0.568 |
| sCD163 (ng/mL), median (95% CI) | 60 | 520 (464–603) | 567 (498–607) | 0.818 |
| Responders | 32 | 503 (450–560) | 515 (447–599) | 0.838 |
| Non-responders | 28 | 552 (465–652) | 607 (500–670) | 0.864 |
| IL-6 (pg/mL), median (95% CI) | 60 | 1.08 (0.71–2.32) | 0.54 (0.18–1.09) | 0.013 |
| Responders | 32 | 1.44 (0.90–2.45) | 0.36 (0.07–0.54) | 0.007 |
| Non-responders | 28 | 0.90 (0.54–2.81) | 0.90 (0.18–1.97) | 0.395 |
| IL-8 (pg/mL), median (95% CI) | 60 | 7.30 (5.79–10.02) | 5.04 (3.19–6.86) | 0.043 |
| Responders | 32 | 6.62 (5.79–10.56) | 4.50 (2.79–6.62) | 0.048 |
| Non-responders | 28 | 8.15 (5.09–11.57) | 6.22 (1.92–10.33) | 0.307 |
| IL-10 (pg/mL), median (95% CI) | 60 | 1.89 (0.48–4.95) | 0.26 (0.01–2.74) | <0.001 |
| Responders | 32 | 3.56 (0.01–6.05) | 0.23 (0.01–2.74) | <0.001 |
| Non-responders | 28 | 1.61 (0.01–3.96) | 0.56 (0.01–2.74) | 0.027 |
| IL-33 (pg/mL), median (95% CI) | 60 | 8.76 (0.09–43.16) | 4.64 (0.01–33.56) | 0.126 |
| Responders | 32 | 8.76 (0.07–49.86) | 4.64 (0.01–46.01) | 0.433 |
| Non-responders | 28 | 16.87 (0.01–57.87) | 0.01 (0.01–36.71) | 0.151 |
| TNFα (pg/mL), median (95% CI) | 60 | 14.46 (9.78–16.76) | 10.40 (7.86–11.86) | <0.001 |
| Responders | 32 | 13.79 (8.75–16.82) | 9.51 (3.25–11.86) | 0.003 |
| Non-responders | 28 | 15.60 (7.86–19.97) | 10.69 (7.67–14.04) | 0.059 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caviglia, G.P.; Rosso, C.; Stalla, F.; Rizzo, M.; Massano, A.; Abate, M.L.; Olivero, A.; Armandi, A.; Vanni, E.; Younes, R.; et al. On-Treatment Decrease of Serum Interleukin-6 as a Predictor of Clinical Response to Biologic Therapy in Patients with Inflammatory Bowel Diseases. J. Clin. Med. 2020, 9, 800. https://doi.org/10.3390/jcm9030800
Caviglia GP, Rosso C, Stalla F, Rizzo M, Massano A, Abate ML, Olivero A, Armandi A, Vanni E, Younes R, et al. On-Treatment Decrease of Serum Interleukin-6 as a Predictor of Clinical Response to Biologic Therapy in Patients with Inflammatory Bowel Diseases. Journal of Clinical Medicine. 2020; 9(3):800. https://doi.org/10.3390/jcm9030800
Chicago/Turabian StyleCaviglia, Gian Paolo, Chiara Rosso, Francesco Stalla, Martina Rizzo, Alessandro Massano, Maria Lorena Abate, Antonella Olivero, Angelo Armandi, Ester Vanni, Ramy Younes, and et al. 2020. "On-Treatment Decrease of Serum Interleukin-6 as a Predictor of Clinical Response to Biologic Therapy in Patients with Inflammatory Bowel Diseases" Journal of Clinical Medicine 9, no. 3: 800. https://doi.org/10.3390/jcm9030800
APA StyleCaviglia, G. P., Rosso, C., Stalla, F., Rizzo, M., Massano, A., Abate, M. L., Olivero, A., Armandi, A., Vanni, E., Younes, R., Fagoonee, S., Pellicano, R., Astegiano, M., Saracco, G. M., Bugianesi, E., & Ribaldone, D. G. (2020). On-Treatment Decrease of Serum Interleukin-6 as a Predictor of Clinical Response to Biologic Therapy in Patients with Inflammatory Bowel Diseases. Journal of Clinical Medicine, 9(3), 800. https://doi.org/10.3390/jcm9030800