The Treatment of Ingrown Nail: Chemical Matricectomy With Phenol Versus Aesthetic Reconstruction. A Single Blinded Randomized Clinical Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Sample
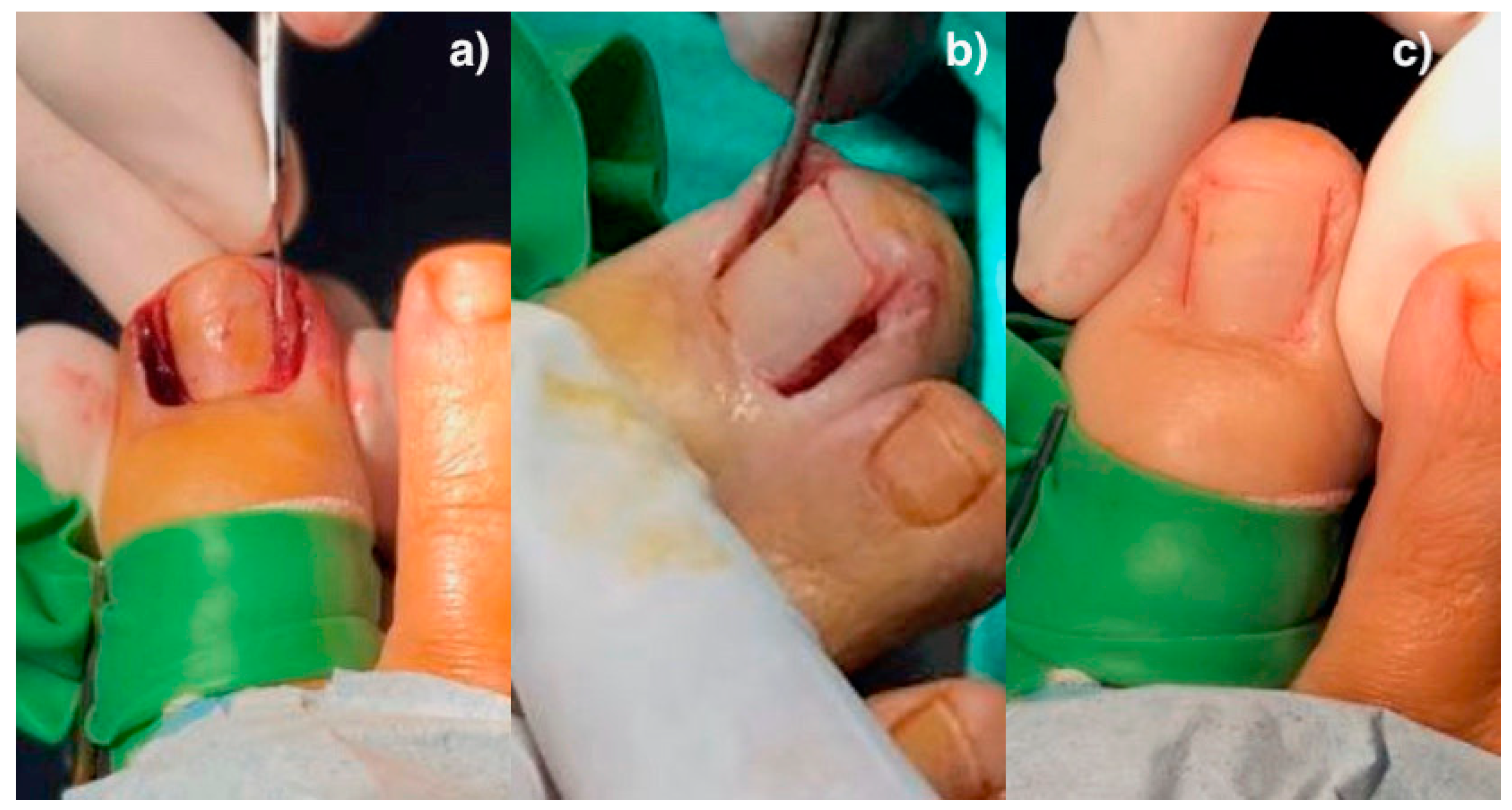
2.2. Surgical Procedures
2.3. Outcome Measurements
2.4. Sample Size Calculation
2.5. Ethical and Legal Considerations
2.6. Statistical Analysis
3. Results
3.1. Descriptive Data
3.2. Outcome Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Martínez-Nova, A.; Sánchez-Rodríguez, R.; Alonso-Peña, D. A new onychocryptosis classification and treatment plan. J. Am. Pod. Med. Assoc. 2007, 97, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, J.; Córdoba-Fernández, A.; Munuera, P.V. Effect of curettage after segmental phenolization in the treatment of onychocryptosis: A randomized double-blind clinical trial. Dermatol. Surg. 2012, 38, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Winograd, A. A modification in the technic of operation for ingrown toenail. J. Am. Pod. Med. Assoc. 2007, 97, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Cologlu, H.; Kocer, U.; Sungur, N.; Uysal, A.; Kankaya, Y.; Oruç, M. A new anatomical repair method for the treatment of ingrown nail. Annals Plastic. Surg. 2005, 54, 306–311. [Google Scholar]
- Zhang, N.; Huang, Z.; Cao, S.H.; Wang, Y.; Hu, Y. Cosmetic, minimally invasive, partial matricectomy of ingrown toenails with granulation tissue. J. Plast. Reconstruc. Aesth. Surg. 2018, 71, 774–775. [Google Scholar] [CrossRef]
- Córdoba-Fernández, A.; Montaño-Jiménez, P.; Coheña-Jiménez, M. Relationship between the presence of abnormal hallux interphalangeal angle and risk of ingrown hallux nail: A case control study. BMC Musculoskelet. Disord. 2015, 16, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Boll, O. Surgical correction of ingrowing nails. J. National Assoc. of Chir. 1945, 35, 8–10. [Google Scholar]
- Córdoba-Díaz, D.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Córdoba-Díaz, M. Effectiveness of standard lavage with supplemental chlorhexidine in patients undergoing chemical matricectomy for ingrown toenails: A clinical trial. J. Am. Acad. Dermatol. 2014, 70, 1092–1095. [Google Scholar] [CrossRef]
- Dika, E.; Balestri, R.; Vaccari, S.; Alessandro, P.; Misciali, C.; Patrizi, A. Successful treatment of pyogenic granulomas following gefitinib therapy with partial matricectomy and phenolization. J. Dermatol. Treat. 2009, 20, 374–375. [Google Scholar] [CrossRef]
- Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Viejo-Tirado, F.; Serrano-Pardo, R. Cauterization of the germinal nail matrix using phenol applications of differing durations: A histologic study. J. Am. Acad. Dermatol. 2012, 67, 706–711. [Google Scholar] [CrossRef]
- Garrido-Castells, X.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C.; Losa-Iglesias, M.E.; Palomo-López, P.; Navarro-Flores, E.; López-López, D. Efectiveness of leukocyte and platelet-rich fibrin versus nitrofurazone on nail post-surgery bleeding and wound cicatrization period reductions: A randomized single blinded clinical trial. J. Clin. Med. 2019, 8, 1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rounding, C.; Bloomfield, S. Surgical treatments for ingrowing toenail. Cochrane Database Syst. Rev. 2005, 18. [Google Scholar] [CrossRef] [Green Version]
- Becerro de Bengoa Vallejo, R.; Losa Iglesias, M.; Alou Cervera, L.; Sevillano Fernaández, D.; Prieto Prieto, J. Total nail ablation for onychodystrophy with optimized gauze-phenol application. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, M.E.L.; De bengoa vallejo, R. Topical Phenol as a Conservative Treatment for Periungual Pyogenic Granuloma. Dermatol. Surg. 2010, 36, 675–678. [Google Scholar] [CrossRef]
- Becerro de Bengoa Vallejo, R.; Losa Iglesias, M.E.; Sanchez Gomez, R.; Jules, K.T. Gauze application of phenol for matrixectomy. J. Am. Podiatr. Med. Assoc. 2008, 98, 418–421. [Google Scholar] [CrossRef]
- Eekhof, J.; Van-Wijk, B.; Knuistingh-Neven, A.; van-der-Wouden, J.C. Interventions for ingrowing toenails. Cochrane Database Syst. Rev. 2012, 18, CD001541. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.; Cho, M.; Eastwood, S. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. J. Am. Med. Assoc. 1996, 276, 637–639. [Google Scholar] [CrossRef]
- García-París, J.; Coheña-Jiménez, M.; Montaño-Jiménez, P.; Córdoba-Fernández, A. Implementation of the WHO Safe Surgery Saves Lives checklist in a podiatric surgery unit in Spain: A single-center retrospective observational study. Patient Saf. Surg. 2015, 9, 28–29. [Google Scholar] [CrossRef] [Green Version]
- Córdoba-Fernández, A.; Rayo-Rosado, R.; Juarez-Jiménez, J. Platelet gel for the surgical treatment of onychocryptosis. J. Am. Pod. Med. Assoc. 2008, 98, 296–301. [Google Scholar] [CrossRef]
- Ozawa, T.; Nose, K.; Harada, T.; Muraoka, M.; Ishii, M. Partial matricectomy with a CO2 laser for ingrown toenail after nail matrix staining. Dermatol. Surg. 2005, 31, 302–305. [Google Scholar] [CrossRef]
- Vaccari, S.; Dika, E.; Balestri, R.; Rech, G.; Piraccini, B.M.; Fanti, P.A. Partial excision of matrix and phenolic ablation for the treatment of ingrowing toenail: A 36-month follow-up of 197 treated patients. Dermatol. Surg. 2010, 36, 1288–1293. [Google Scholar] [CrossRef] [PubMed]
- Persichetti, P.; Simone, P.; Li-Vecchi, G.; Di-Lella, F.; Cagli, B.; Marangi, G.F. Wedge excision of the nail fold in the treatment of ingrown toenail. Annals Plast. Surg. 2004, 52, 617–620. [Google Scholar] [CrossRef] [PubMed]
- Shaath, N.; Shea, J.; Whiteman, I.; Zarugh, A. A prospective randomized comparison of the Zadik procedure and chemical ablation in the treatment of ingrown toenails. Foot Ankle Int. 2005, 26, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Bostanci, S.; EkmekçI, P.; Gürgey, E. Chemical matricectomy with phenol for the treatment of ingrowing toenail: A review of the literature and follow-up of 172 treated patients. Acta Derm. Venerol. 2001, 81, 181–183. [Google Scholar] [CrossRef]
- Hassel, J.; Hassel, A.; Loser, C. Phenol chemical matricectomy is less painful, with shorter recovery times but higher recurrence rates, than surgical matricectomy: A patient’s view. Dermatol. Surg. 2010, 36, 1294–1299. [Google Scholar] [CrossRef]
- Shaikh, F.; Jafri, M.; Giri, S.; Keane, R. Efficacy of wedge resection with phenolization in the treatment of ingrowing toenails. J. Am. Pod. Med. Assoc. 2008, 98, 118–122. [Google Scholar] [CrossRef]
- Guerritsma-Bleeker, C.; Klaase, J.; Geelkerken, R.; Hermans, J.; van-Det, R.J. Partial matrix excision or segmental phenolizationfor ingrowing toenails. Arch. Surg. 2002, 137, 320–325. [Google Scholar] [CrossRef] [Green Version]
- Akkus, A.; Demirseren, D.D.; Demirseren, M.E.; Aktas, A. The treatment of ingrown nail: Chemical matricectomy with NAOH versus wedge resection. Dermatol. Ther. 2018, 31, 2677. [Google Scholar] [CrossRef]
- Buckley, D. Segmental phenolic ablation for ingrowing toenails in general practice. Ir. Med. J. 2000, 93, 242–244. [Google Scholar]
- Karaca, N.; Dereli, T. Treatment of ingrown toenail with proximolateral matrix partial excision and matrix phenolization. Ann. Fam. Med. 2012, 10, 556–559. [Google Scholar] [CrossRef] [Green Version]
- Morkane, A.; Robertson, R.; Inglis, G. Segmental phenolization of ingrowing toenails: A randomized controlled study. Br. J. Surg. 1984, 71, 526–527. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rey, J.; Mediavilla-Saldaña, L.; Martínez-Nova, A. Exploring postoperative outcomes for ingrown toenails. NaOH vs Wedge resection techniques. Dermatol. Surg. 2014, 40, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Ozan, F.; Doğar, F.; Altay, T.; Uğur, S.G.; Koyuncu, Ş. Partial matricectomy with curettage and electrocautery: A comparison of two surgical methods in the treatment of ingrown toenails. Dermatol. Surg. 2014, 40, 1132–1139. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Chemical Matricectomy with Phenol | Aesthetic Reconstruction Group | Total Analyzed |
|---|---|---|---|
| Patients | 10 (29.4%) | 24 (70.6%) | 34 (100%) |
| Males | 4 | 8 | 12 (35.3%) |
| Females | 6 | 16 | 22 (64.7%) |
| Feet | 18 | 38 | 56 |
| Nail Folds | 36 (32.1%) | 76 (67.9%) | 112 (100%) |
| Average Age | 37.1 | 32.4 | 34.0 |
| SD | 20.3 | 17.7 | 18.3 |
| Outcome Measurements | Chemical Matricectomy with Phenol | Aesthetic Reconstruction Group | p-Value |
|---|---|---|---|
| Mean ± SD (95% CI) Median (IR) | Mean ± SD (95% CI) Median (IR) | ||
| Healing time (days) | 21.3 ± 3.1 (20.20–22.39) 20,5 (11) | 8.2 ± 1.4 (7.92–8.55) 8 (7) | <0.001 * |
| Recurrence rate | 1 (2.8%) ** | 2 (1.52%) ** | 0.98 *** |
| Post-surgical bleeding (Mild = 1; moderate = 2; abundant = 3) | 1.67 ± 0.58 (1.48–1.86) 2 (1) | 1.65 ± 0.62 (1.51–1.79) 2 (1) | 0.91 * |
| Post-surgical pain at 1st day (VAS) | 1.9 ± 1.8 (1.31–2.49) 1.5 (3) | 2.6 ± 2.5 (2.04–3.16) 2 (4) | 0.41 * |
| Post-surgical pain at 2nd day (VAS) | 1.2 ± 1.4 (0.74–1.66) 1 (2) | 1.9 ± 2.2 (1.41–2.39) 1 (4) | 0.28 * |
| Post-surgical pain at 3rd day (VAS) | 0.8 ± 1.2 (0.41–1.19) 0 (1) | 1 ± 1.3 (0.71–1.29) 1 (2) | 0.33 * |
| Post-surgical inflammation (mm; digital circumference) | 0.2 ± 0.1(0.17–0.23) 0.2 | 0.3 ± 0.3 (0.23–0.37) 0.3 | 0.72 * |
| Infection rate | 2 (5.6%) ** | 2 (1.5%) ** | 0.82 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muriel-Sánchez, J.M.; Becerro-de-Bengoa-Vallejo, R.; Montaño-Jiménez, P.; Coheña-Jiménez, M. The Treatment of Ingrown Nail: Chemical Matricectomy With Phenol Versus Aesthetic Reconstruction. A Single Blinded Randomized Clinical Trial. J. Clin. Med. 2020, 9, 845. https://doi.org/10.3390/jcm9030845
Muriel-Sánchez JM, Becerro-de-Bengoa-Vallejo R, Montaño-Jiménez P, Coheña-Jiménez M. The Treatment of Ingrown Nail: Chemical Matricectomy With Phenol Versus Aesthetic Reconstruction. A Single Blinded Randomized Clinical Trial. Journal of Clinical Medicine. 2020; 9(3):845. https://doi.org/10.3390/jcm9030845
Chicago/Turabian StyleMuriel-Sánchez, Juan Manuel, Ricardo Becerro-de-Bengoa-Vallejo, Pedro Montaño-Jiménez, and Manuel Coheña-Jiménez. 2020. "The Treatment of Ingrown Nail: Chemical Matricectomy With Phenol Versus Aesthetic Reconstruction. A Single Blinded Randomized Clinical Trial" Journal of Clinical Medicine 9, no. 3: 845. https://doi.org/10.3390/jcm9030845
APA StyleMuriel-Sánchez, J. M., Becerro-de-Bengoa-Vallejo, R., Montaño-Jiménez, P., & Coheña-Jiménez, M. (2020). The Treatment of Ingrown Nail: Chemical Matricectomy With Phenol Versus Aesthetic Reconstruction. A Single Blinded Randomized Clinical Trial. Journal of Clinical Medicine, 9(3), 845. https://doi.org/10.3390/jcm9030845