Additional Physical Interventions to Conventional Physical Therapy in Parkinson’s Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials


 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Study Selection Process and Data Extraction
2.4. Assessment of the Methodological Quality of the RCTs Included in the Review
2.5. Statistical Analysis
3. Results
3.1. Assessment of the Methodological Quality of the RCTs Included in the Review
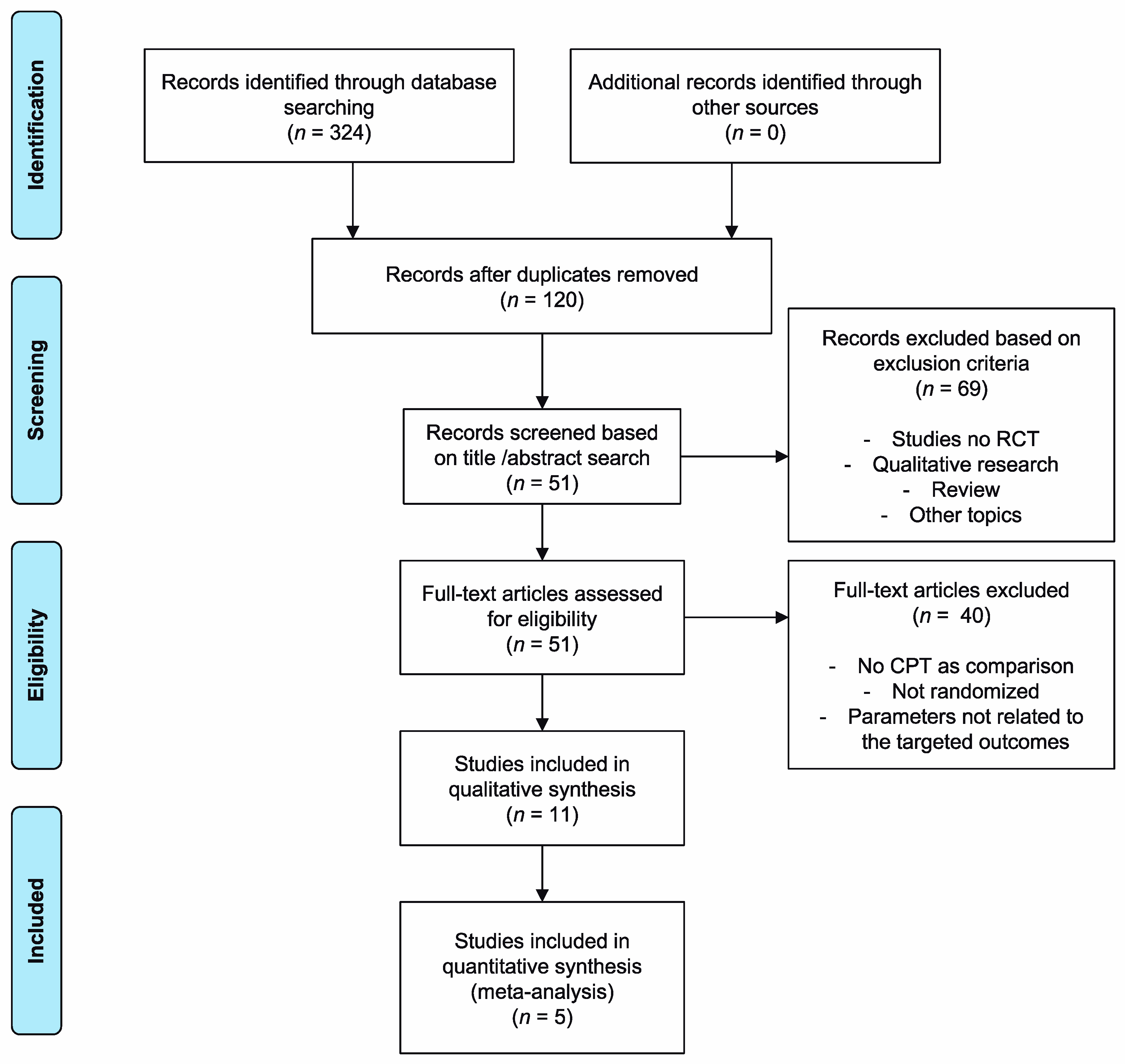
3.2. RCT Inclusion and Classification
3.3. Groups Included in the Meta-Analysis
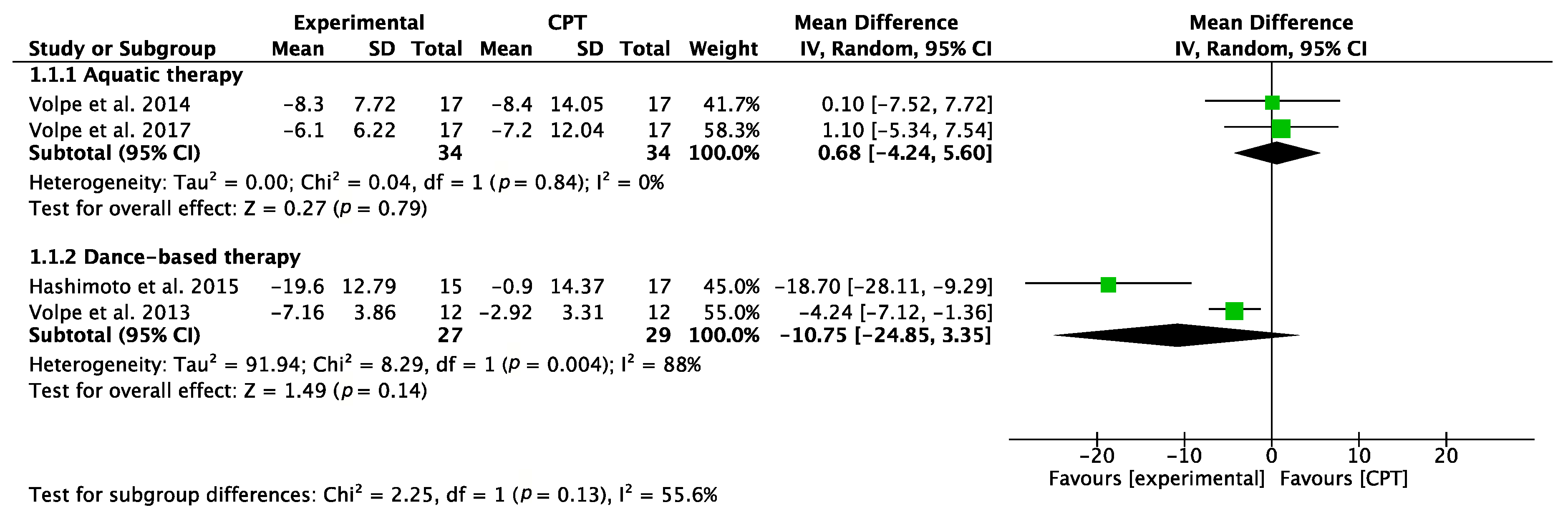
3.3.1. Motor Function (UPDRS-III)
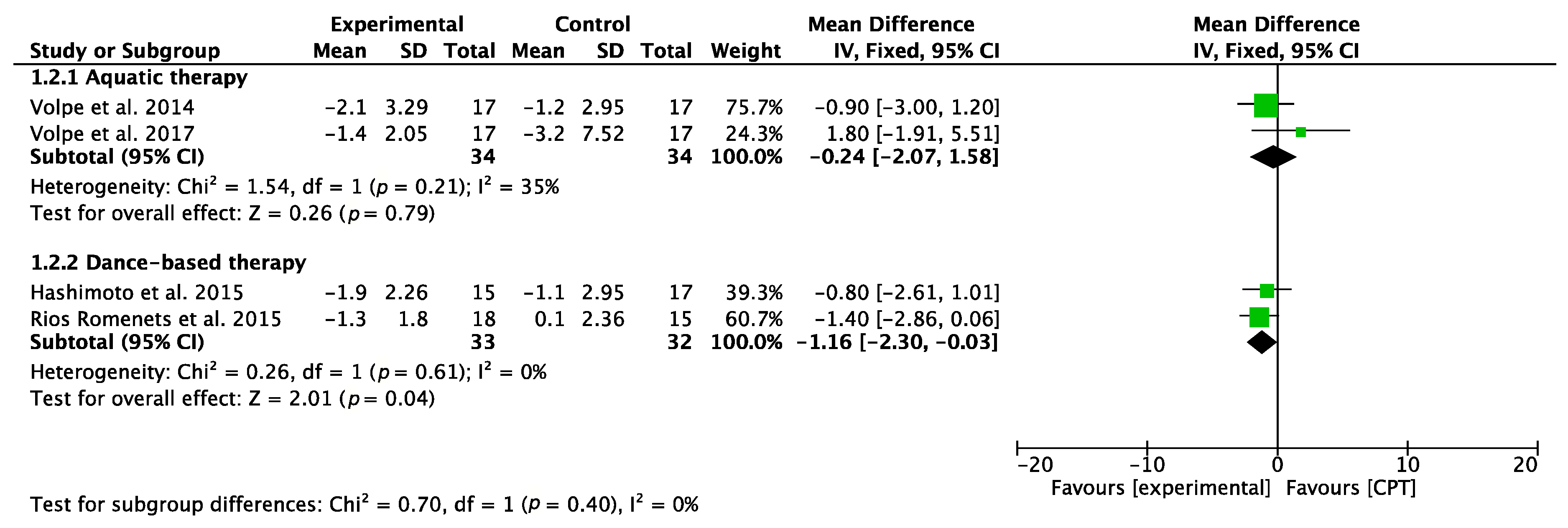
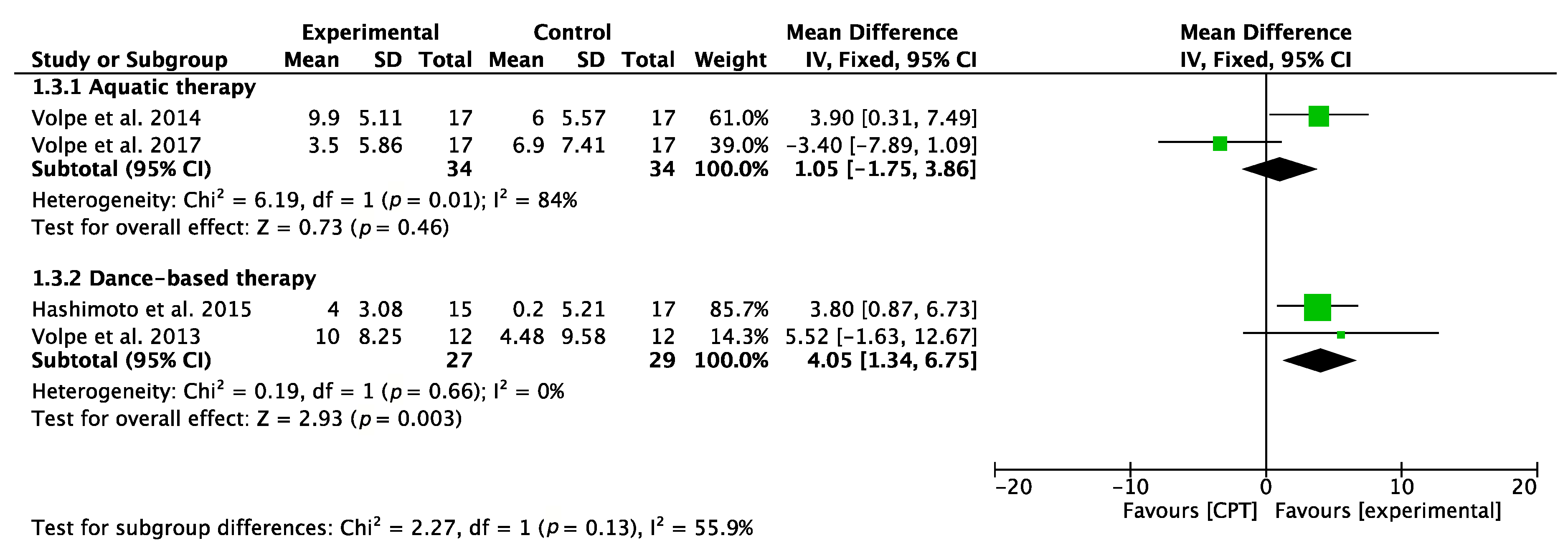
3.3.2. Balance (TUG and BBS)
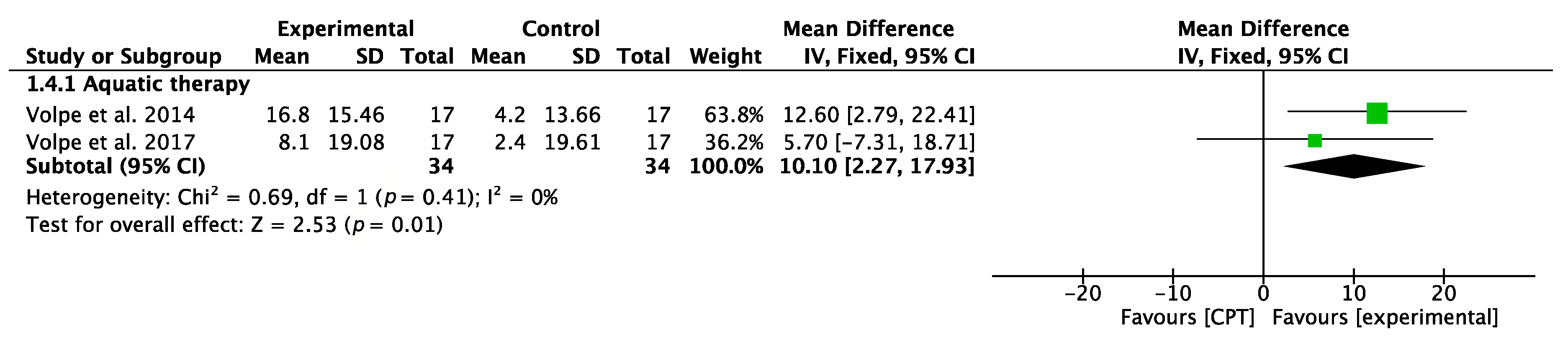
3.3.3. Balance Confidence (ABC)
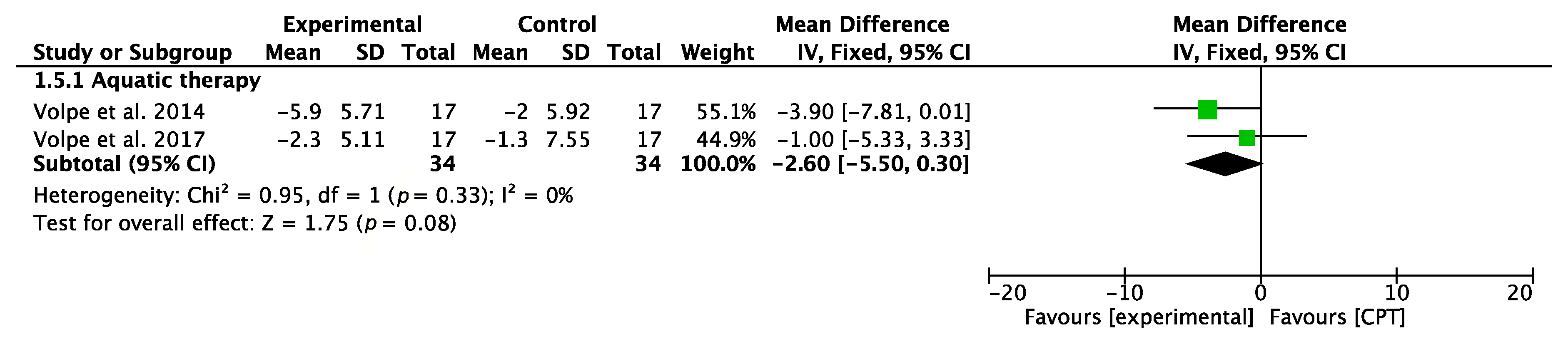
3.3.4. Fall-Related Self-Efficacy (FES)
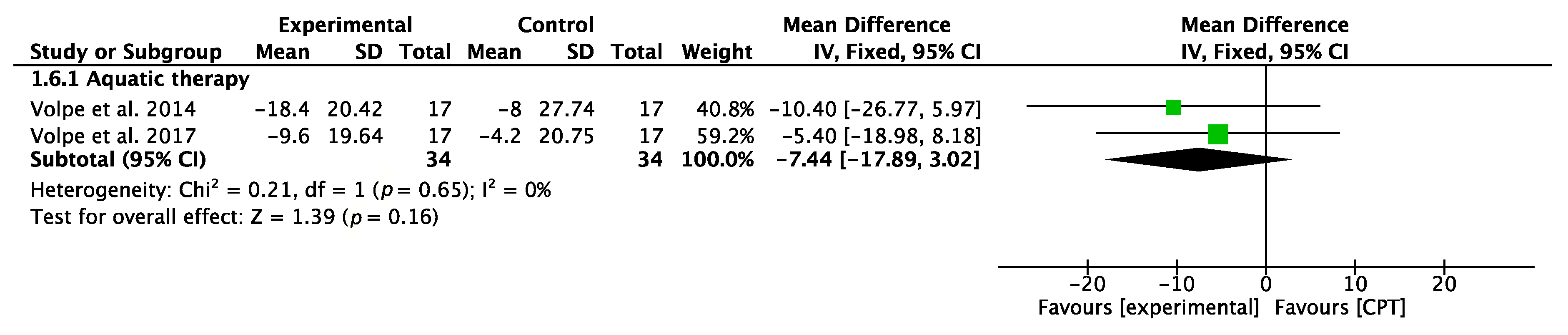
3.3.5. Quality of Life (PDQ-39)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Park, J.-H.; Kim, D.-H.; Kwon, D.-Y.; Choi, M.; Kim, S.; Jung, J.-H.; Han, K.; Park, Y.-G. Trends in the incidence and prevalence of Parkinson’s disease in Korea: a nationwide, population-based study. BMC Geriatr. 2019, 19, 320. [Google Scholar] [CrossRef] [Green Version]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.-E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 3, 1–21. [Google Scholar] [CrossRef]
- Levi, V.; Carrabba, G.; Rampini, P.; Locatelli, M. Short term surgical complications after subthalamic deep brain stimulation for Parkinson’s disease: does old age matter? BMC Geriatr. 2015, 15, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Fernández, R.; Gasca-Salas, C.C.; Sánchez-Ferro, A.; Obeso, J.A. Parkinson’s disease: A review. Rev. Médica Clínica Las Condes 2016, 27, 363–379. [Google Scholar]
- Palazón García, R.; Gómez del Monte, C.; Cantero Garlito, P.A.; Cabañas Elías, J.; Berrocal Sánchez, I. Treatment protocol in Parkinson’s disease. Rehabilitación 2001, 35, 175–178. Available online: https://doi.org/10.1016/S0048-7120(01)73164-7 (accessed on 19 January 2019). [CrossRef]
- Miranda, C.M.; Hudson, A.L. Severe leg edema associated with the use of dopaminergic drugs in Parkinson’s disease. Report of one case. Rev. Med. Chil. 2017, 145, 1624–1625. [Google Scholar]
- Toosizadeh, N.; Lei, H.; Schwenk, M.; Sherman, S.J.; Sternberg, E.; Mohler, J.; Najafi, B. Does integrative medicine enhance balance in aging adults? Proof of concept for the benefit of electroacupuncture therapy in Parkinson’s disease. Gerontology 2015, 61, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Santos, S.M.; da Silva, R.A.; Terra, M.B.; Almeida, I.A.; de Melo, L.B.; Ferraz, H.B. Balance versus resistance training on postural control in patients with Parkinson’s disease: a randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2017, 53, 173–183. [Google Scholar]
- Ganesan, M.; Sathyaprabha, T.N.; Gupta, A.; Pal, P.K. Effect of partial weight-supported treadmill gait training on balance in patients with Parkinson disease. PM&R 2014, 6, 22–33. [Google Scholar]
- Ricciardi, L.; Ricciardi, D.; Lena, F.; Plotnik, M.; Petracca, M.; Barricella, S.; Bentivoglio, A.R.; Modugno, N.; Bernabei, R.; Fasano, A.; et al. Working on asymmetry in Parkinson’s disease: randomized, controlled pilot study. Neurol. Sci. 2015, 36, 1337–1343. [Google Scholar] [CrossRef]
- Picelli, A.; Melotti, C.; Origano, F.; Neri, R.; Waldner, A.; Smania, N. Robot-assisted gait training versus equal intensity treadmill training in patients with mild to moderate Parkinson’s disease: A randomized controlled trial. Parkinsonism Relat. Disord. 2013, 19, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.-Y.; Yang, Y.-R.; Cheng, S.-J.; Wu, Y.-R.; Fuh, J.-L.; Wang, R.-Y. Virtual Reality-Based Training to Improve Obstacle-Crossing Performance and Dynamic Balance in Patients With Parkinson’s Disease. Neurorehabil. Neural Repair 2015, 29, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Hely, M.A.; Reid, W.G.J.; Adena, M.A.; Halliday, G.M.; Morris, J.G.L. The Sydney Multicenter Study of Parkinson’s disease: The inevitability of dementia at 20 years. Mov. Disord. 2008, 23, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Keus, S.H.J.; Munneke, M.; Graziano, M.; Paltamaa, J.; Pelosin, E.; Domingos, J.; Brühlmann, S.; Ramaswamy, B.; Prins, J.; Struiksma, C.; et al. European guidelines for physiotherapy in Parkinson’s disease. Mov. Disord. 2013, 28, S382–S383. [Google Scholar]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: onset, progression, and mortality. Neurology 1967, 17, 427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metman, L.V.; Myre, B.; Verwey, N.; Hassin-Baer, S.; Arzbaecher, J.; Sierens, D.; Bakay, R. Test–Retest Reliability of UPDRS-III, Dyskinesia Scales, and Timed Motor Tests in Patients With Advanced Parkinson’ s Disease: An Argument Against Multiple Baseline Assessments. Mov. Disord. 2004, 19, 1079–1084. [Google Scholar] [CrossRef]
- Choi, Y.I.; Song, C.S.; Chun, B.Y. Activities of daily living and manual hand dexterity in persons with idiopathic Parkinson disease. J. Phys. Ther. Sci. 2017, 29, 457–460. [Google Scholar] [CrossRef] [Green Version]
- Crizzle, A.M.; Newhouse, I.J. Is Physical Exercise Beneficial for Persons with Parkinson’s Disease? Clin. J. Sport Med. 2006, 16, 422–425. [Google Scholar] [CrossRef]
- Kwakkel, G.; de Goede, C.J.T.; van Wegen, E.E.H. Impact of physical therapy for Parkinson’s disease: A critical review of the literature. Parkinsonism Relat. Disord. 2007, 13, S478–S487. [Google Scholar] [CrossRef]
- Boonstra, T.A.; van der Kooij, H.; Munneke, M.; Bloem, B.R. Gait disorders and balance disturbances in Parkinsonʼs disease: clinical update and pathophysiology. Curr. Opin. Neurol. 2008, 24, 461–471. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Patel, S.; Meek, C.; Herd, C.P.; Clarke, C.E.; Stowe, R.; Shah, L.; Sackley, C.; Deane, K.H.O.; Wheatley, K.; et al. Physiotherapy intervention in Parkinson’s disease: systematic review and meta-analysis. BMJ 2012, 345, e5004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloem, B.R.; de Vries, N.M.; Ebersbach, G. Nonpharmacological treatments for patients with Parkinson’s disease. Mov. Disord. 2015, 30, 1504–1520. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Catalá-López, F.; Moher, D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef]
- Description of Physical Therapy: Policy Statement. World Confederation for Physical Therapy. Appendix 1. 2011. Available online: https://www.wcpt.org/policy/ps-descriptionPT (accessed on 28 March 2020).
- VanSant, A.F. The International Classification of Functioning, Disability and Health. Pediatr. Phys. Ther. 2006, 18, 237. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Moseley, A.M.; Herbert, R.D.; Sherrington, C.; Maher, C.G. Evidence for physiotherapy practice: A survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef] [Green Version]
- van Nimwegen, M.; Speelman, A.D.; Overeem, S.; van de Warrenburg, B.P.; Smulders, K.; Dontje, M.L.; Borm, G.F.; Backx, F.J.G.; Bloem, B.R.; Munneke, M.; et al. Promotion of physical activity and fitness in sedentary patients with Parkinson’s disease: randomised controlled trial. BMJ 2013, 346, f576. [Google Scholar] [CrossRef] [Green Version]
- Volpe, D.; Signorini, M.; Marchetto, A.; Lynch, T.; Morris, M.E. A comparison of Irish set dancing and exercises for people with Parkinson’s disease: A phase II feasibility study. BMC Geriatr. 2013, 13, 54. [Google Scholar] [CrossRef] [Green Version]
- Volpe, D.; Giantin, M.G.; Maestri, R.; Frazzitta, G. Comparing the effects of hydrotherapy and land-based therapy on balance in patients with Parkinson’s disease: a randomized controlled pilot study. Clin. Rehabil. 2014, 28, 1210–1217. [Google Scholar] [CrossRef]
- Monticone, M.; Ambrosini, E.; Laurini, A.; Rocca, B.; Foti, C. In-patient multidisciplinary rehabilitation for Parkinson’s disease: A randomized controlled trial. Mov. Disord. 2015, 30, 1050–1058. [Google Scholar] [CrossRef]
- Hashimoto, H.; Takabatake, S.; Miyaguchi, H.; Nakanishi, H.; Naitou, Y. Effects of dance on motor functions, cognitive functions, and mental symptoms of Parkinson’s disease: A quasi-randomized pilot trial. Complement. Ther. Med. 2015, 23, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Romenets, S.R.; Anang, J.; Fereshtehnejad, S.-M.; Pelletier, A.; Postuma, R. Tango for treatment of motor and non-motor manifestations in Parkinson’s disease: A randomized control study. Complement. Ther. Med. 2015, 23, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Volpe, D.; Giantin, M.G.; Manuela, P.; Filippetto, C.; Pelosin, E.; Abbruzzese, G.; Antonini, A. Water-based vs. non-water-based physiotherapy for rehabilitation of postural deformities in Parkinson’s disease: A randomized controlled pilot study. Clin. Rehabil. 2017, 31, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Carpinella, I.; Cattaneo, D.; Bonora, G.; Bowman, T.; Martina, L.; Montesano, A.; Ferrarin, M. Wearable Sensor-Based Biofeedback Training for Balance and Gait in Parkinson Disease: A Pilot Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2017, 98, 622–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shujaat, F.; Soomro, N.; Khan, M. The effectiveness of Kayaking exercises as compared to general mobility exercises in reducing axial rigidity and improve bed mobility in early to mid stage of Parkinson’s disease. Pak. J. Med. Sci. 2014, 30, 1094–1098. [Google Scholar] [PubMed] [Green Version]
- Keus, S.H.J.; Bloem, B.R.; Hendriks, E.J.M.; Bredero-Cohen, A.B.; Munneke, M. Evidence-based analysis of physical therapy in Parkinson’s disease with recommendations for practice and research. Mov. Disord. 2007, 22, 451–460. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed ”Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in Stroke Rehabilitation: A Systematic Review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]
- Shanahan, J.; Morris, M.E.; Bhriain, O.N.; Volpe, D.; Lynch, T.; Clifford, A.M. Dancing for Parkinson Disease: A Randomized Trial of Irish Set Dancing Compared With Usual Care. Arch. Phys. Med. Rehabil. 2017, 98, 1744–1751. [Google Scholar] [CrossRef] [Green Version]
- Aguiar, L.P.C.; da Rocha, P.A.; Morris, M. Therapeutic Dancing for Parkinson’s Disease. Int. J. Gerontol. 2016, 10, 64–70. [Google Scholar] [CrossRef]
- Jonasson, S.B.; Nilsson, M.H.; Lexell, J. Psychometric properties of four fear of falling rating scales in people with Parkinson’s disease. BMC Geriatr. 2014, 14, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Methajarunon, P.; Eitivipart, C.; Diver, C.J.; Foongchomcheay, A. Systematic review of published studies on aquatic exercise for balance in patients with multiple sclerosis, Parkinson’s disease, and hemiplegia. Hong Kong Physiother. J. 2016, 35, 12–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemper, K.J. What’s new in complementary therapies for Parkinson’s disease? Complement Ther. Med. 2019, 42, A1–A3. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Hu, J.; Wei, L.; Jia, Y.; Jin, Y. Effects of dance therapy on cognitive and mood symptoms in people with Parkinson’s disease: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2019, 36, 12–17. [Google Scholar] [CrossRef]
- dos Santos Delabary, M.; Komeroski, I.G.; Monteiro, E.P.; Costa, R.R.; Haas, A.N. Effects of dance practice on functional mobility, motor symptoms and quality of life in people with Parkinson’s disease: a systematic review with meta-analysis. Aging Clin. Exp. Res. 2018, 30, 727–735. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Records | Search Terms |
|---|---|---|
| PubMed | 127 | “Parkinson Disease”, “Physiotherapy” and “Physical Therapy” |
| PEDro | 33 | |
| WoS | 108 | |
| Scopus | 31 | |
| SciELO | 25 |
| PEDro Scale | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Total Score | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
| Picelli et al. (2013) [11] | 8 | _ | X | X | X | X | X | X | X | X | ||
| Nimwegen et al. (2013) [28] | 8 | _ | X | X | X | X | X | X | X | X | ||
| Volpe et al. (2013) [29] | 6 | _ | X | X | X | X | X | X | ||||
| Shujaat et al. (2014) [36] | 5 | _ | X | X | X | X | X | |||||
| Volpe et al. (2014) [30] | 8 | _ | X | X | X | X | X | X | X | X | ||
| Ricciardi et al. (2015) [10] | 5 | _ | X | X | X | X | X | |||||
| Monticone et al. (2015) [31] | 6 | _ | X | X | X | X | X | X | ||||
| Hashimoto et al. (2015) [32] | 6 | _ | X | X | X | X | X | X | ||||
| Rios Romenets et al. (2015) [33] | 6 | _ | X | X | X | X | X | X | ||||
| Volpe et al. (2017) [34] | 6 | _ | X | X | X | X | X | X | ||||
| Carpinella et al. (2017) [35] | 6 | _ | X | X | X | X | X | X | ||||
| Study | Stage * | Medical Treatment | Intervention ** | Frequency | Session Duration | Intervention Duration | Outcome Measures | Measuring Instrument | Results |
|---|---|---|---|---|---|---|---|---|---|
| Nimwegen et al. (2013) [28] | 1–3 | Medical treatment was not described. | IG: n = 299 ParkFit program. CG: n = 287 CPT (Keus et al. (2007) [37] evidence-based recommendations) | 7 days/week | ND | 6, 12, 18, 24 months. months | Level of physical activity | LAPAQ questionnaire. PDQ-39, Daily Activity, Activity Monitor, Six-Minute Walk Test | There is no change in physical activity level after the ParkFit program. LAPAQ p = 0.19 (at 24 months). Secondary results suggest greater involvement in specific elements improving physical condition among the IG. Daily activity p < 0.001 Activity monitor p < 0.001 PDQ-39 p = 0.14 Six-minutes run p = 0.05 |
| Picelli et al. (2013) [11] | 3 | Participants continued their usual medical treatment, which remained stable for the full study period. Patients with severe dyskinesias or “on-off” fluctuations, and changes of PD medication during the study, were excluded. Patients were tested and trained during the “on” phase, 1–2.5 h after taking their morning dose. | IG 1: n = 20 Robotic assistance. IG 2: n = 20. Treadmill training CG: n = 20. CPT (PNF concept focused on gait) | 3 days/week | 45 min | 4 weeks | Ability to walk without assistance, travel speed, spatial-temporal gait, balance. | Main variables: 10MWT and 6MWT. Secondary variables: Spatial-temporal parameters for walking. | No significant evidence was found in the primary variables between the IG1 group and the IG2 group. Test 10MWT p = 0.869 Test 6MWT p = 0.941 Whether significant differences were found in the primary variables between the TGR and TT groups compared with PT. 10MWT: IG1 vs. CG p = 0.003 IG2 vs. CG p = 0.041 6MWT: IG1 vs. CG p = 0.021 IG2 vs. CG p = 0.048 |
| Volpe et al. (2013) [29] | 1–2.5 | Participants continued their usual medical treatment, which remained stable for the full study period. Tests were performed at the same time of day. | IG: n = 12 Irish dance. CG: n = 12 CPT (KNGF Guidelines for physical therapy in PD) | 1.5 h/week | 90 min | 6 months | Level of mobility, balance, quality of life. | UPDRS (engine), BBS, TUG, FOG, PDQ-39 | Multicenter studies with larger sample sizes are needed to determine which therapy is most effective. UPDRS III (motor) p = 0.019 TUG test p = 0.007 BBS p = 0.051 FOG p = 0.000 PDQ-39 p = 0.153 |
| Shujaat et al. (2014) [36] | 1–3 | Participants continued their usual medical treatment, which remained stable for the full study period. | IG: n = 24 Kayak intervention. CG: n = 24 CPT (strengthening exercise and core stability) | 6 days/week | 75 min | 4 weeks | Ability to rotate cervical and thoracolumbar, mobility in bed. | Goniometer and MPAS | The rotation capacity at the cervical and thoracolumbar level is significantly increased in both groups after analyzing the measurements with the goniometer p < 0.001. Bed mobility is also significantly increased in both groups p < 0.001. The results are significantly better in the IG. |
| Volpe et al. (2014) [30] | 2.5–3 | Participants continued their usual medical treatment, which remained stable for the full study period. The evaluation of the different scales was performed one hour after the first dose of Levodopa (“on” medication phase). | IG: n = 17 Aquatic therapy CG: n = 17 CPT (KNGF Guidelines for physical therapy in PD) | 5 days/week | 60 min | 2 months | Balance, functional capacity, motor capacity, number of falls, motor performance, ability to perform ADL. | Centre of pressure with stabilometric platform, UPDRS II and III, BBS, TUG(s), ABC, FES, PDQ-39, Falls diary. | Significant increases were observed in the variables analyzed in both groups p = <0.002. These improvements are significantly greater in the IG. Centre of pressure p = 0.05 BBS p = 0.005 ABC p = 0.0001 FES p = 0.003 PDQ-39 p = 0.006 Falls diary p = 0.001 |
| Monticone et al. (2015) [31] | 2.5–4 | Participants continued their usual medical treatment, which remained stable for the full study period. Patients with previous “on-off” fluctuations were excluded. Patients were assessed during “on” state approximately 1 h after the first drug assumption. | IG: n = 32 Multidisciplinary rehabilitative care CG: n = 32 CPT (neuromotor techniques, joint mobilization, strengthening and stretching exercises, proprioceptive and walking training) | 7 days/ week | IG and CG: 90 min. Physical training. IG: 30 min Psychology (2 sessions per week). 30 min occupational therapy 1 session per week | 8 weeks | Motor development, balance, ability to perform ADL, quality of life. | MDS-UPDRS-III, BBS, FIM, PDQ-39 | The multidisciplinary intervention shows better results in parameters such as motor development, balance, ADL and quality of life. MDS-UPDRS-III p < 0.001 BBS p < 0.001 FIM p < 0.001 PDQ-39 p < 0.012 |
| Ricciardi et al. (2015) [10] | 2–3 | Participants continued their usual medical treatment, which remained stable for the full study period. | IG 1: n = 9 Best side improvement. IG 2: n = 9 Worst side improvement. CG: n = 10 CPT (strengthening and mobility exercises) | 2 times/week | 1 h | 3 months | Motor development, balance, ability to perform ADL, quality of life. | UPDRS-III, Tinetti (total score), Tinetti (gait), GFQ, SPPB. | Better results are evidenced in IG1 UPDRS-III (IG1 vs CG) p = 0.01. Tinetti (total score) p = 0.05. Tinetti (gait) p = 0.01. |
| Hashimoto et al. (2015) [32] | IG and CG1: 2–3, CG2: 2–4. | Participants continued their usual medical treatment, which remained stable for the full study period. Participants whose medications changed during the study period were excluded from the analysis | IG: n = 15 Dance-based therapy. CG 1: n = 17 CPT (joint mobilization, balance and walking training by video or book) CG 2: n = 14 No intervention. | 1 time/week | 60 min | 12 weeks | Motor and cognitive functions, mental symptoms related to Parkinson’s disease | TUG time, TUG step number, BBS, FAB, MRT response time, AS, SDS, UPDRS | Significant improvements are evident before and after the intervention in the IG dance group. TUG time p = 0.006 TUG step number p = 0.005 BBS p = 0.001 FAB p = 0.001 MRT response time p < 0.79 AS p < 0.001 SDS p = 0.006 UPDRS p < 0.001 |
| Rios Romenets et al. (2015) [33] | 1–3 | Participants continued their usual medical treatment, which remained stable for the full study period. | IG: n = 18 Dance-based therapy. CG: n = 15 CPT (Pamphlet about PD exercise from the Parkinson Society of Canada) | IG. 2 times/week | IG. 1 h | 12 weeks | General motor severity, other motor conditions, balance, cognitive level, fatigue, apathy, depression and quality of life. | MDS-UPDRS-III, General clinical impression by the patient, examiner evaluation, MiniBESTest, TUGtime, TUGstep, improvements in turns, MoCa, FES. | MDS-UPDRS-III p = 0.85 General clinical impression by patient p = 0.33 Examiner’s evaluation p = 0.02 MiniBESTest p = 0.032 TUGtime p = 0.042 TUGdts p = 0.012 Improvements in turns p = 0.066 MoCa p = 0.080 FES p = 0.057 |
| Volpe et al. (2017) [34] | 2–3 | Participants continued their usual medical treatment, which remained stable for the full study period. Patients were always tested at the time of their optimal antiparkinsonian medication (‘on’ phase) and no change in medication was allowed during the study period. | IG: n = 15 Aquatic therapy. CG: n = 15 CPT (Postural realignment exercises) | 5 times/week | 60 min | 8 weeks | Degrees of cervical and dorsal flexion, lateral inclination angle of the trunk. Motor symptoms, balance, balance confidence, fall-related self-efficacy, and quality of life. | Posturographic system and Body Analysis Kapture (BAK) System. UPDRS-III, BBS, ABC, TUG, FES, PDQ-39 | No significant differences between groups. Statistical data supports significant improvements in IG: UPDRS-III p = 0.001 BBS p < 0.001 ABC p = 0.02 TUG p = 0.036 FES p = 0.027 PDQ-39 p < 0.001 At 16 weeks there is a follow-up that shows less significant results. |
| Carpinella et al. (2017) [35] | 2–4 | Participants continued their usual medical treatment, which remained stable for the full study period. Assessment and treatment were performed always in “on” medication phase | IG: n = 17 Wearable Sensor-Based Biofeedback training. CG: n = 20 CPT (Keus et al. (2007) [37] evidence-based recommendations) | 3 times/week | 45 min | 20 sessions 7 weeks | Balance and ability to walk. | BBS, 10MWT. Stabilometric instruments, telequestionnaire of satisfaction in health care. | Statistically significant differences can be seen comparing both groups in favor of IG1. BBS p = 0.047 Post-training stabilometric indices p = 0.003 |
| Group/Instrument | Studies | Type of Intervention | Outcome |
|---|---|---|---|
| UPDRS-III | Volpe et al. (2014) [30] Volpe et al. (2017) [34] | Aquatic physical therapy | Motor function |
| Volpe et al. (2013) [29] Hashimoto et al. (2015) [32] | Dance-based therapy | ||
| TUG (s) | Volpe et al. (2014) [30] Volpe et al. (2017) [34] | Aquatic physical therapy | Balance |
| Hashimoto et al. (2015) [32] Rios Romenets et al. (2015) [33] | Dance-based therapy | ||
| BBS | Volpe et al. (2014) [30] Volpe et al. (2017) [34] | Aquatic physical therapy | Balance |
| Volpe et al. (2013) [29] Hashimoto et al. (2015) [32] | Dance-based therapy | ||
| ABC | Volpe et al. (2014) [30] Volpe et al. (2017) [34] | Aquatic physical therapy | Balance confidence |
| FES | Volpe et al. (2014) [30] Volpe et al. (2017) [34] | Aquatic physical therapy | Fall-related self-efficacy |
| PDQ-39 | Volpe et al. (2014) [30] Volpe et al. (2017) [34] | Aquatic physical therapy | Quality of life |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hidalgo-Agudo, R.D.; Lucena-Anton, D.; Luque-Moreno, C.; Heredia-Rizo, A.M.; Moral-Munoz, J.A. Additional Physical Interventions to Conventional Physical Therapy in Parkinson’s Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Clin. Med. 2020, 9, 1038. https://doi.org/10.3390/jcm9041038
Hidalgo-Agudo RD, Lucena-Anton D, Luque-Moreno C, Heredia-Rizo AM, Moral-Munoz JA. Additional Physical Interventions to Conventional Physical Therapy in Parkinson’s Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Journal of Clinical Medicine. 2020; 9(4):1038. https://doi.org/10.3390/jcm9041038
Chicago/Turabian StyleHidalgo-Agudo, Ruben D., David Lucena-Anton, Carlos Luque-Moreno, Alberto Marcos Heredia-Rizo, and Jose A. Moral-Munoz. 2020. "Additional Physical Interventions to Conventional Physical Therapy in Parkinson’s Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials" Journal of Clinical Medicine 9, no. 4: 1038. https://doi.org/10.3390/jcm9041038
APA StyleHidalgo-Agudo, R. D., Lucena-Anton, D., Luque-Moreno, C., Heredia-Rizo, A. M., & Moral-Munoz, J. A. (2020). Additional Physical Interventions to Conventional Physical Therapy in Parkinson’s Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Journal of Clinical Medicine, 9(4), 1038. https://doi.org/10.3390/jcm9041038