Predicting Stroke Outcomes Using Ankle-Brachial Index and Inter-Ankle Blood Pressure Difference

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
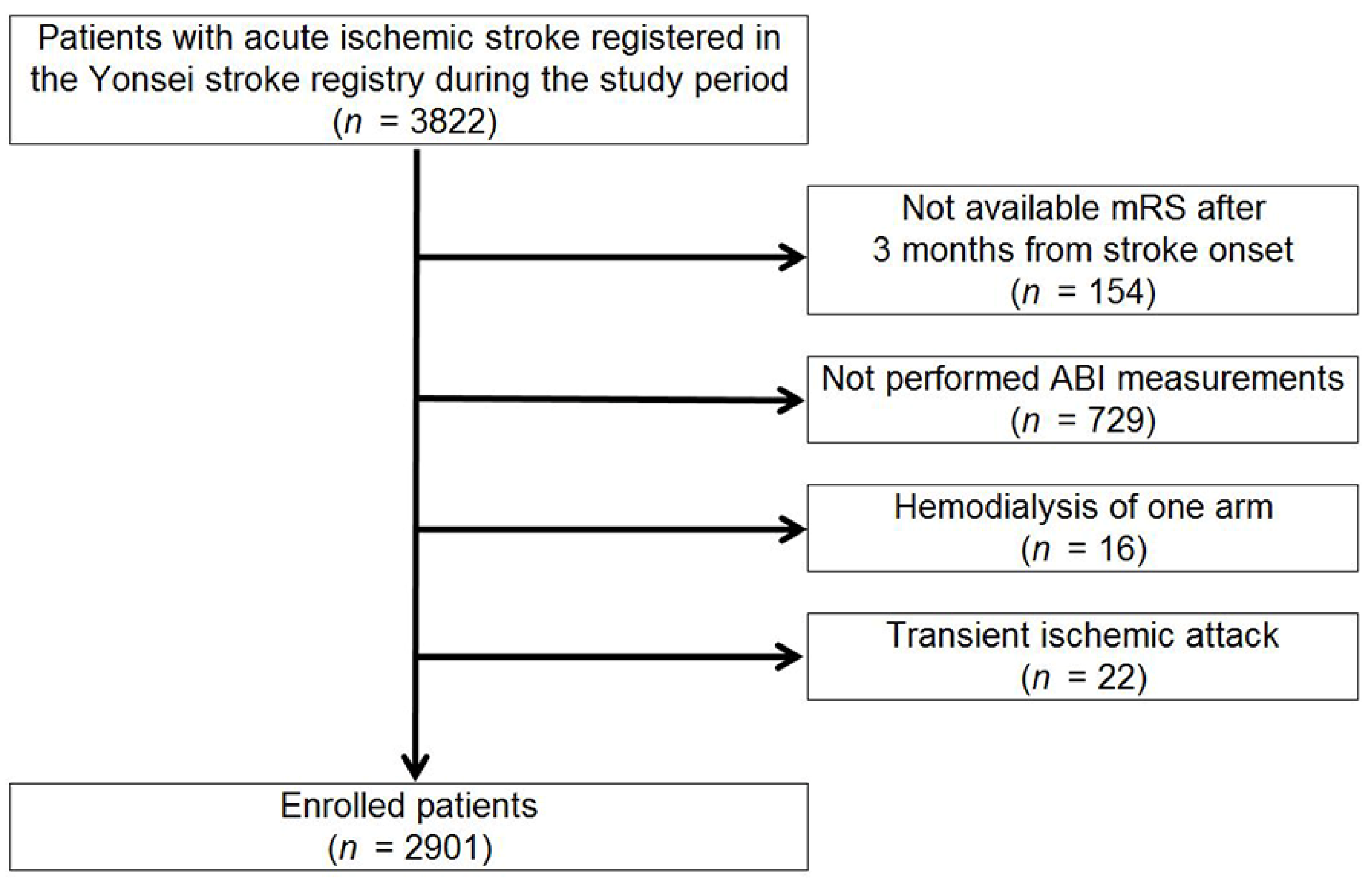
2.1. Patients and Evaluation
2.2. Demographic Characteristics and Risk Factors
2.3. ABI and Brachial-Ankle Pulse Wave Velocity Measurement
2.4. Follow-Up and Outcome Measures
2.5. Statistical Analysis
2.6. Standard Protocol Approval, Registration, and Patient Consent
2.7. Data availability Statement
3. Results
3.1. Patient Demographic and Clinical Characteristics
3.2. Poor Functional Outcome
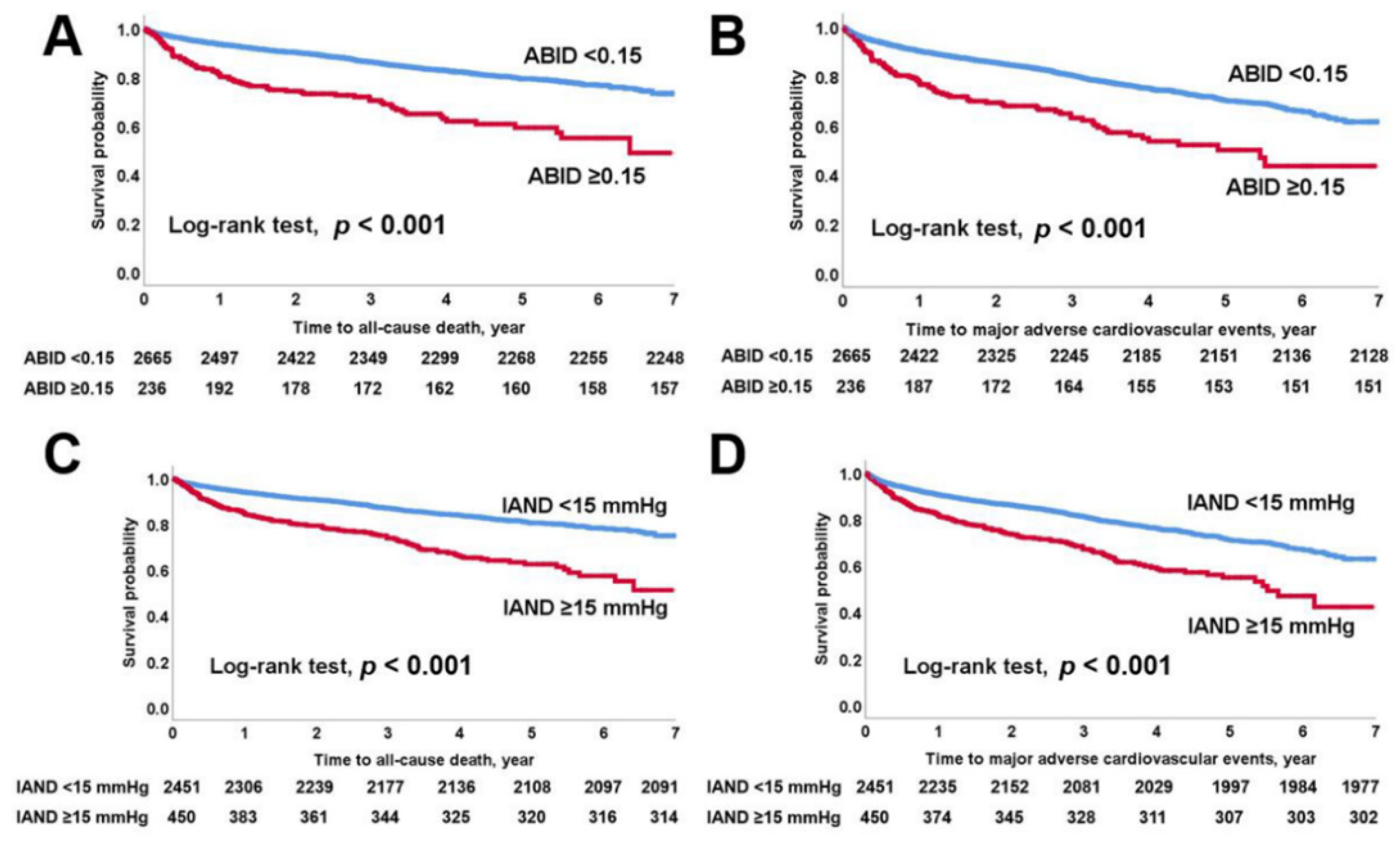
3.3. All-Cause Mortality and MACEs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guo, H.; Sun, F.; Dong, L.; Chang, H.; Gu, X.; Zhang, H.; Sheng, L.; Tian, Y. The Association of Four-Limb Blood Pressure with History of Stroke in Chinese Adults: A Cross-Sectional Study. PLoS ONE 2015, 10, e0139925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milionis, H.; Vemmou, A.; Ntaios, G.; Makaritsis, K.; Koroboki, E.; Papavasileiou, V.; Savvari, P.; Spengos, K.; Elisaf, M.; Vemmos, K. Ankle-brachial index long-term outcome after first-ever ischaemic stroke. Eur. J. Neurol. 2013, 20, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- Sheng, C.S.; Liu, M.; Zeng, W.F.; Huang, Q.F.; Li, Y.; Wang, J.G. Four-limb blood pressure as predictors of mortality in elderly Chinese. Hypertension 2013, 61, 1155–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.; Hiatt, W.R.; Jonsson, B.; Lacroix, P.; et al. Measurement and interpretation of the ankle-brachial index: A scientific statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.Y.; Leu, J.G.; Fang, Y.W.; Tsai, M.H. Association of interleg difference of ankle brachial index with overall and cardiovascular mortality in chronic hemodialysis patients. Ren. Fail. 2015, 37, 88–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Song, T.J.; Song, D.; Lee, H.S.; Nam, C.M.; Nam, H.S.; Kim, Y.D.; Heo, J.H. Interarm blood pressure difference and mortality in patients with acute ischemic stroke. Neurology 2013, 80, 1457–1464. [Google Scholar] [CrossRef]
- Huttner, H.B.; Kohrmann, M.; Mauer, C.; Lucking, H.; Kloska, S.; Doerfler, A.; Schwab, S.; Schellinger, P.D. The prevalence of peripheral arteriopathy is higher in ischaemic stroke as compared with transient ischaemic attack and intracerebral haemorrhage. Int. J. Stroke 2010, 5, 278–283. [Google Scholar] [CrossRef]
- Sen, S.; Lynch, D.R., Jr.; Kaltsas, E.; Simmons, J.; Tan, W.A.; Kim, J.; Beck, J.; Rosamond, W. Association of asymptomatic peripheral arterial disease with vascular events in patients with stroke or transient ischemic attack. Stroke 2009, 40, 3472–3477. [Google Scholar] [CrossRef] [Green Version]
- Han, M.; Kim, Y.D.; Park, H.J.; Hwang, I.G.; Choi, J.; Ha, J.; Heo, J.H.; Nam, H.S. Prediction of functional outcome using the novel asymmetric middle cerebral artery index in cryptogenic stroke patients. PLoS ONE 2019, 14, e0208918. [Google Scholar] [CrossRef]
- Sacco, R.L.; Adams, R.; Albers, G.; Alberts, M.J.; Benavente, O.; Furie, K.; Goldstein, L.B.; Gorelick, P.; Halperin, J.; Harbaugh, R.; et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: A statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: Co-sponsored by the Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology affirms the value of this guideline. Stroke 2006, 37, 577–617. [Google Scholar] [CrossRef]
- Adams, R.J.; Albers, G.; Alberts, M.J.; Benavente, O.; Furie, K.; Goldstein, L.B.; Gorelick, P.; Halperin, J.; Harbaugh, R.; Johnston, S.C.; et al. Update to the AHA/ASA recommendations for the prevention of stroke in patients with stroke and transient ischemic attack. Stroke 2008, 39, 1647–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furie, K.L.; Kasner, S.E.; Adams, R.J.; Albers, G.W.; Bush, R.L.; Fagan, S.C.; Halperin, J.L.; Johnston, S.C.; Katzan, I.; Kernan, W.N.; et al. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack: A guideline for healthcare professionals from the american heart association/american stroke association. Stroke 2011, 42, 227–276. [Google Scholar] [CrossRef] [PubMed]
- Jauch, E.C.; Saver, J.L.; Adams, H.P., Jr.; Bruno, A.; Connors, J.J.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W., Jr.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Han, M.; Kim, Y.D.; Park, H.J.; Hwang, I.G.; Choi, J.; Ha, J.; Heo, J.H.; Nam, H.S. Brachial-ankle pulse wave velocity for predicting functional outcomes in patients with cryptogenic stroke. J. Clin. Neurosci. 2019, 69, 214–219. [Google Scholar] [CrossRef]
- Nam, H.S.; Kim, H.C.; Kim, Y.D.; Lee, H.S.; Kim, J.; Lee, D.H.; Heo, J.H. Long-term mortality in patients with stroke of undetermined etiology. Stroke 2012, 43, 2948–2956. [Google Scholar] [CrossRef] [Green Version]
- Herraiz-Adillo, A.; Soriano-Cano, A.; Martinez-Hortelano, J.A.; Garrido-Miguel, M.; Mariana-Herraiz, J.A.; Martinez-Vizcaino, V.; Notario-Pacheco, B. Simultaneous inter-arm and inter-leg systolic blood pressure differences to diagnose peripheral artery disease: A diagnostic accuracy study. Blood Press. 2018, 27, 121–122. [Google Scholar] [CrossRef]
- Fowkes, F.G.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Ohman, E.M.; Hirsch, A.T.; Ikeda, Y.; Mas, J.L.; Goto, S.; Liau, C.S.; Richard, A.J.; Rother, J.; et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA 2006, 295, 180–189. [Google Scholar] [CrossRef] [Green Version]
- Hoshino, T.; Sissani, L.; Labreuche, J.; Ducrocq, G.; Lavallee, P.C.; Meseguer, E.; Guidoux, C.; Cabrejo, L.; Hobeanu, C.; Gongora-Rivera, F.; et al. Prevalence of systemic atherosclerosis burdens and overlapping stroke etiologies and their associations with long-term vascular prognosis in stroke with intracranial atherosclerotic disease. JAMA Neurol. 2018, 75, 203–211. [Google Scholar] [CrossRef]
- Lee, D.H.; Kim, J.; Lee, H.S.; Cha, M.J.; Kim, Y.D.; Nam, H.S.; Nam, C.M.; Heo, J.H. Low ankle-brachial index is a predictive factor for initial severity of acute ischaemic stroke. Eur. J. Neurol. 2012, 19, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Ma, J.; Tao, X.; Zhou, Y.; Liu, X.; Su, H. The prevalence and influence factors of inter-ankle systolic blood pressure difference in community population. PLoS ONE 2013, 8, e70777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.; Kim, J.; Kim, Y.J.; Song, T.J. Inter-arm blood pressure difference is associated with recurrent stroke in non-cardioembolic stroke patients. Sci. Rep. 2019, 9, 12758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.; Kim, J.; Kim, M.H.; Kim, Y.J.; Song, T.J. Interarm Blood Pressure Difference is Associated with Early Neurological Deterioration, Poor Short-Term Functional Outcome, and Mortality in Noncardioembolic Stroke Patients. J. Clin. Neurol. 2018, 14, 555–565. [Google Scholar] [CrossRef]
- Yan, B.P.; Zhang, Y.; Kong, A.P.; Luk, A.O.; Ozaki, R.; Yeung, R.; Tong, P.C.; Chan, W.B.; Tsang, C.C.; Lau, K.P.; et al. Borderline ankle-brachial index is associated with increased prevalence of micro- and macrovascular complications in type 2 diabetes: A cross-sectional analysis of 12,772 patients from the Joint Asia Diabetes Evaluation Program. Diab. Vasc. Dis. Res. 2015, 12, 334–341. [Google Scholar] [CrossRef] [Green Version]
- Sanada, H.; Higashi, Y.; Goto, C.; Chayama, K.; Yoshizumi, M.; Sueda, T. Vascular function in patients with lower extremity peripheral arterial disease: A comparison of functions in upper and lower extremities. Atherosclerosis 2005, 178, 179–185. [Google Scholar] [CrossRef]
- Su, H.M.; Lin, T.H.; Hsu, P.C.; Lee, W.H.; Chu, C.Y.; Chen, S.C.; Lee, C.S.; Voon, W.C.; Lai, W.T.; Sheu, S.H. Association of interankle systolic blood pressure difference with peripheral vascular disease and left ventricular mass index. Am. J. Hypertens. 2014, 27, 32–37. [Google Scholar] [CrossRef] [Green Version]
- Su, H.M.; Lin, T.H.; Hsu, P.C.; Lee, W.H.; Chu, C.Y.; Chen, S.C.; Lee, C.S.; Voon, W.C.; Lai, W.T.; Sheu, S.H. Association of bilateral brachial-ankle pulse wave velocity difference with peripheral vascular disease and left ventricular mass index. PLoS ONE 2014, 9, e88331. [Google Scholar] [CrossRef]
- Lin, L.Y.; Hwu, C.M.; Chu, C.H.; Won, J.G.S.; Chen, H.S.; Chang, L.H. The ankle brachial index exhibits better association with cardiovascular outcomes than interarm systolic blood pressure difference in patients with type 2 diabetes. Medicine (Baltimore) 2019, 98, e15556. [Google Scholar] [CrossRef]
- Aboyans, V.; Ho, E.; Denenberg, J.O.; Ho, L.A.; Natarajan, L.; Criqui, M.H. The association between elevated ankle systolic pressures and peripheral occlusive arterial disease in diabetic and nondiabetic subjects. J. Vasc. Surg. 2008, 48, 1197–1203. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.C.; Chang, J.M.; Hwang, S.J.; Tsai, J.C.; Liu, W.C.; Wang, C.S.; Lin, T.H.; Su, H.M.; Chen, H.C. Ankle brachial index as a predictor for mortality in patients with chronic kidney disease and undergoing haemodialysis. Nephrology (Carlton) 2010, 15, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Resnick, H.E.; Lindsay, R.S.; McDermott, M.M.; Devereux, R.B.; Jones, K.L.; Fabsitz, R.R.; Howard, B.V. Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality: The Strong Heart Study. Circulation 2004, 109, 733–739. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.C.; Chang, J.M.; Tsai, Y.C.; Tsai, J.C.; Su, H.M.; Hwang, S.J.; Chen, H.C. Association of interleg BP difference with overall and cardiovascular mortality in hemodialysis. Clin. J. Am. Soc. Nephrol. 2012, 7, 1646–1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verberk, W.J.; Kessels, A.G.; Thien, T. Blood pressure measurement method and inter-arm differences: A meta-analysis. Am. J. Hypertens. 2011, 24, 1201–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Total | Good Outcomes (mRS of 0‒2; n = 2319) | Poor Outcomes (mRS of 3‒6; n = 582) | p Value | |
|---|---|---|---|---|
| (n = 2901) | ||||
| Age, y | 65.4 ± 12.2 | 64.0 ± 12.0 | 71.0 ± 11.4 | <0.001 |
| Men | 1793 (61.8) | 1489 (64.2) | 304 (52.2) | <0.001 |
| NIHSS score at admission | 3.0 (1.0, 6.0) | 2.0 (1.0, 4.0) | 8.0 (4.0, 15.0) | <0.001 |
| Risk factors | ||||
| Hypertension | 2164 (74.6) | 1712 (73.8) | 452 (77.7) | 0.057 |
| Diabetes mellitus | 920 (31.7) | 728 (31.4) | 192 (33.0) | 0.459 |
| Hypercholesterolemia | 622 (21.4) | 486 (21.0) | 136 (23.4) | 0.205 |
| Current smoking | 717 (24.7) | 622 (26.8) | 95 (16.3) | <0.001 |
| Congestive heart failure | 119 (4.1) | 92 (4.0) | 27 (4.6) | 0.465 |
| Coronary artery disease | 686 (23.6) | 549 (23.7) | 137 (23.5) | 0.946 |
| Cerebral artery atherosclerosis | 1727 (59.5) | 1292 (55.7) | 435 (74.7) | <0.001 |
| Peripheral artery disease | 258 (8.9) | 152 (6.6) | 106 (18.2) | <0.001 |
| Laboratory findings | ||||
| Glucose, mg/dL | 143.5 ± 63.9 | 142.7 ± 63.2 | 1468 ± 66.0 | 0.168 |
| HDL, mg/dL | 42.8 ± 11.0 | 42.6 ± 10.8 | 43.4 ± 11.6 | 0.127 |
| LDL, mg/dL | 114.5 ± 38.6 | 114.7 ± 37.5 | 113.8 ± 42.5 | 0.651 |
| Stroke subtype | ||||
| LAA | 587 (20.2) | 440 (19.0) | 147 (25.3) | <0.001 |
| CE | 754 (26.0) | 600 (25.9) | 154 (26.5) | |
| SVO | 261 (9.0) | 232 (10.0) | 29 (5.0) | |
| OC | 72 (2.5) | 58 (2.5) | 14 (2.4) | |
| UE | 1227 (42.3) | 989 (42.6) | 238 (40.9) | |
| Arm BP, mmHg | ||||
| Right SBP | 146.3 ± 23.5 | 146.7 ± 23.2 | 145.1 ± 24.6 | 0.147 |
| Left SBP | 145.3 ± 23.8 | 145.6 ± 23.6 | 144.0 ± 24.6 | 0.129 |
| IAD | 4.90 ± 6.51 | 4.71 ± 6.45 | 5.77 ± 7.15 | 0.001 |
| Ankle BP, mmHg | ||||
| Right SBP | 164.5 ± 31.3 | 166.3 ± 30.1 | 157.7 ± 35.1 | <0.001 |
| Left SBP | 163.6 ± 31.3 | 165.2 ± 30.4 | 157.2 ± 34.6 | <0.001 |
| IAND | 9.23 ± 11.94 | 8.42 ± 10.82 | 12.65 ± 15.87 | <0.001 |
| ABI | ||||
| Right ABI | 1.111 ± 0.132 | 1.122 ± 0.118 | 1.071 ± 0.170 | <0.001 |
| Left ABI | 1.105 ± 0.130 | 1.114 ± 0.118 | 1.069 ± 0.171 | <0.001 |
| ABID | 0.063 ± 0.083 | 0.058 ± 0.077 | 0.086 ± 0.104 | <0.001 |
| Right ABI >1.30 | 58 (2.0) | 44 (1.9) | 14 (2.4) | 0.434 |
| Left ABI >1.30 | 44 (1.5) | 31 (1.3) | 13 (2.2) | 0.113 |
| Both ABI >1.30 | 18 (0.6) | 14 (0.6) | 4 (0.7) | 0.818 |
| ABID ≥0.15 | IAND ≥15 mmHg | IAD ≥15 mmHg | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p value * | OR (95% CI) | p value * | OR (95% CI) | p value * | |
| CAD | 1.290 (0.954‒1.745) | 0.098 | 0.957 (0.752‒1.217) | 0.718 | 0.912 (0.580‒1.434) | 0.689 |
| CAA | 1.718 (1.211‒2.437) | 0.002 | 1.646 (1.281‒2.114) | <0.001 | 1.451 (0.926‒2.274) | 0.104 |
| PAD | 22.124 (15.844‒30.894) | <0.001 | 13.328 (9.876‒17.987) | <0.001 | 3.044 (1.890‒4.904) | <0.001 |
| Right ABI >1.30 | Left ABI >1.30 | Both ABI >1.30 | ||||
|---|---|---|---|---|---|---|
| n (%) | p value | n (%) | p value | n (%) | p value | |
| ABID | ||||||
| ABID <0.15 | 45 (1.7) | 0.001 | 30 (1.1) | <0.001 | 18 (0.7) | 0.392 |
| ABID ≥0.15 | 13 (5.5) | 14 (5.9) | 0 (0.0) | |||
| IAND | ||||||
| IAND <15 mmHg | 36 (1.5) | <0.001 | 27 (1.1) | <0.001 | 16 (0.7) | 1.000 |
| IAND ≥15 mmHg | 22 (4.9) | 17 (3.8) | 2 (0.4) | |||
| IAD | ||||||
| IAD <15 mmHg | 55 (2.0) | 0.503 | 42 (1.5) | 0.695 | 17 (0.6) | 0.521 |
| IAD ≥15 mmHg | 3 (2.6) | 2 (1.7) | 1 (0.9) | |||
| All Patients (n = 2901) | Patients without PAD (n = 2643) | |||
|---|---|---|---|---|
| OR (95% CI) | p value* | OR (95% CI) | p value* | |
| ABI | ||||
| ABID | 5.289 (1.723‒16.236) | 0.004 | 5.774 (0.948‒35.151) | 0.057 |
| ABID ≥0.15 | 1.920 (1.361‒2.708) | <0.001 | 1.970 (1.175‒3.302) | 0.010 |
| Ankle BP, mmHg | ||||
| IAND | 1.015 (1.007‒1.023) | <0.001 | 1.025 (1.009‒1.041) | 0.002 |
| IAND ≥15 mmHg | 1.818 (1.389‒2.381) | <0.001 | 1.665 (1.188‒2.334) | 0.003 |
| Arm BP, mmHg | ||||
| IAD | 1.009 (0.995‒1.024) | 0.190 | 1.009 (0.991‒1.027) | 0.329 |
| IAD ≥15 mmHg | 1.623 (1.011‒2.605) | 0.045 | 1.337 (0.758‒2.360) | 0.316 |
| All Patients (n = 2901) | ||||
| All-Cause Mortality | MACE | |||
| HR (95% CI) | p value* | HR (95% CI) | p value* | |
| ABI | ||||
| ABID | 6.221 (2.973‒13.018) | <0.001 | 3.926 (1.906‒8.087) | <0.001 |
| ABID ≥0.15 | 1.567 (1.223‒2.009) | <0.001 | 1.416 (1.117‒1.794) | 0.004 |
| Ankle BP, mmHg | ||||
| IAND | 1.013 (1.007‒1.019) | <0.001 | 1.010 (1.005‒1.015) | <0.001 |
| IAND ≥15 mmHg | 1.616 (1.317‒1.982) | <0.001 | 1.380 (1.139‒1.672) | 0.001 |
| Arm BP, mmHg | ||||
| IAD | 1.009 (0.999‒1.019) | 0.068 | 1.010 (1.001‒1.019) | 0.027 |
| IAD ≥15 mmHg | 1.176 (0.810‒1.708) | 0.395 | 1.151 (0.820‒1.617) | 0.417 |
| Patients without PAD (n = 2643) | ||||
| All-cause mortality | MACE | |||
| HR (95% CI) | p value* | HR (95% CI) | p value* | |
| ABI | ||||
| ABID | 9.221 (3.013‒28.220) | <0.001 | 6.605 (2.281‒19.124) | 0.001 |
| ABID ≥0.15 | 1.524 (1.039‒2.235) | 0.031 | 1.514 (1.058‒2.166) | 0.023 |
| Ankle BP, mmHg | ||||
| IAND | 1.017 (1.004‒1.030) | 0.010 | 1.015 (1.004‒1.027) | 0.010 |
| IAND ≥15 mmHg | 1.516 (1.164‒1.973) | 0.002 | 1.343 (1.051‒1.716) | 0.019 |
| Arm BP, mmHg | ||||
| IAD | 1.007 (0.993‒1.021) | 0.333 | 1.006 (0.993‒1.018) | 0.374 |
| IAD ≥15 mmHg | 1.075 (0.681‒1.697) | 0.755 | 1.032 (0.682‒1.563) | 0.881 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, M.; Kim, Y.D.; Choi, J.K.; Choi, J.; Ha, J.; Park, E.; Kim, J.; Song, T.-J.; Heo, J.H.; Nam, H.S. Predicting Stroke Outcomes Using Ankle-Brachial Index and Inter-Ankle Blood Pressure Difference. J. Clin. Med. 2020, 9, 1125. https://doi.org/10.3390/jcm9041125
Han M, Kim YD, Choi JK, Choi J, Ha J, Park E, Kim J, Song T-J, Heo JH, Nam HS. Predicting Stroke Outcomes Using Ankle-Brachial Index and Inter-Ankle Blood Pressure Difference. Journal of Clinical Medicine. 2020; 9(4):1125. https://doi.org/10.3390/jcm9041125
Chicago/Turabian StyleHan, Minho, Young Dae Kim, Jin Kyo Choi, Junghye Choi, Jimin Ha, Eunjeong Park, Jinkwon Kim, Tae-Jin Song, Ji Hoe Heo, and Hyo Suk Nam. 2020. "Predicting Stroke Outcomes Using Ankle-Brachial Index and Inter-Ankle Blood Pressure Difference" Journal of Clinical Medicine 9, no. 4: 1125. https://doi.org/10.3390/jcm9041125
APA StyleHan, M., Kim, Y. D., Choi, J. K., Choi, J., Ha, J., Park, E., Kim, J., Song, T. -J., Heo, J. H., & Nam, H. S. (2020). Predicting Stroke Outcomes Using Ankle-Brachial Index and Inter-Ankle Blood Pressure Difference. Journal of Clinical Medicine, 9(4), 1125. https://doi.org/10.3390/jcm9041125