The Effects of Granulocyte Colony-Stimulating Factor in Patients with a Large Anterior Wall Acute Myocardial Infarction to Prevent Left Ventricular Remodeling: A 10-Year Follow-Up of the RIGENERA Study

 ,
,  ,
,  ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
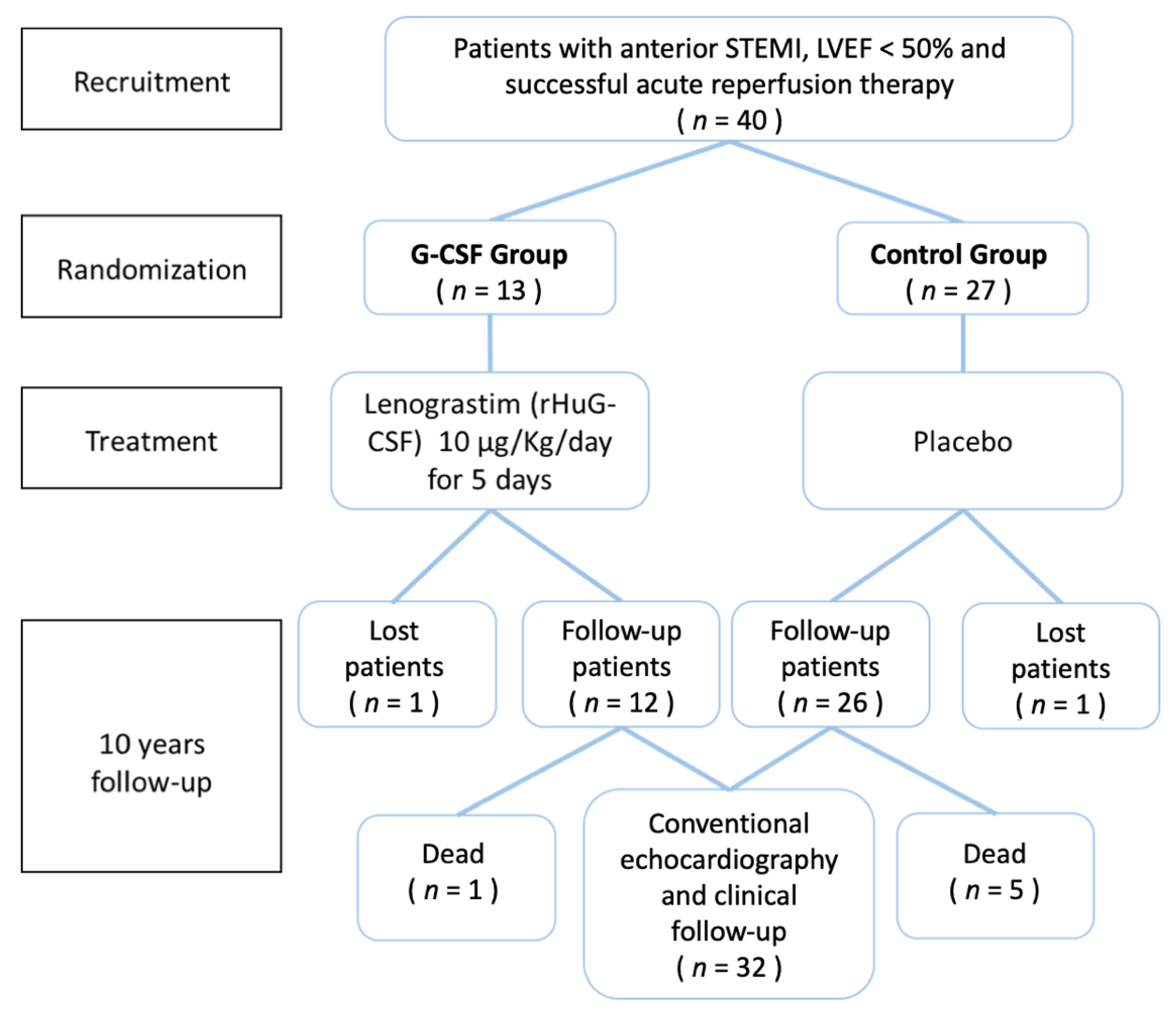
2.1. Patients and Protocol of Original RIGENERA Trial
2.2. Assessment at 10-Year Follow-Up
2.2.1. Clinical Evaluation
2.2.2. Echocardiography
2.2.3. Minnesota Living with Heart Failure Questionnaire (MLHFQ)
2.2.4. Seattle Heart Failure Model (SHFM)
2.2.5. Statistical Analysis
3. Results
3.1. Clinical Outcomes
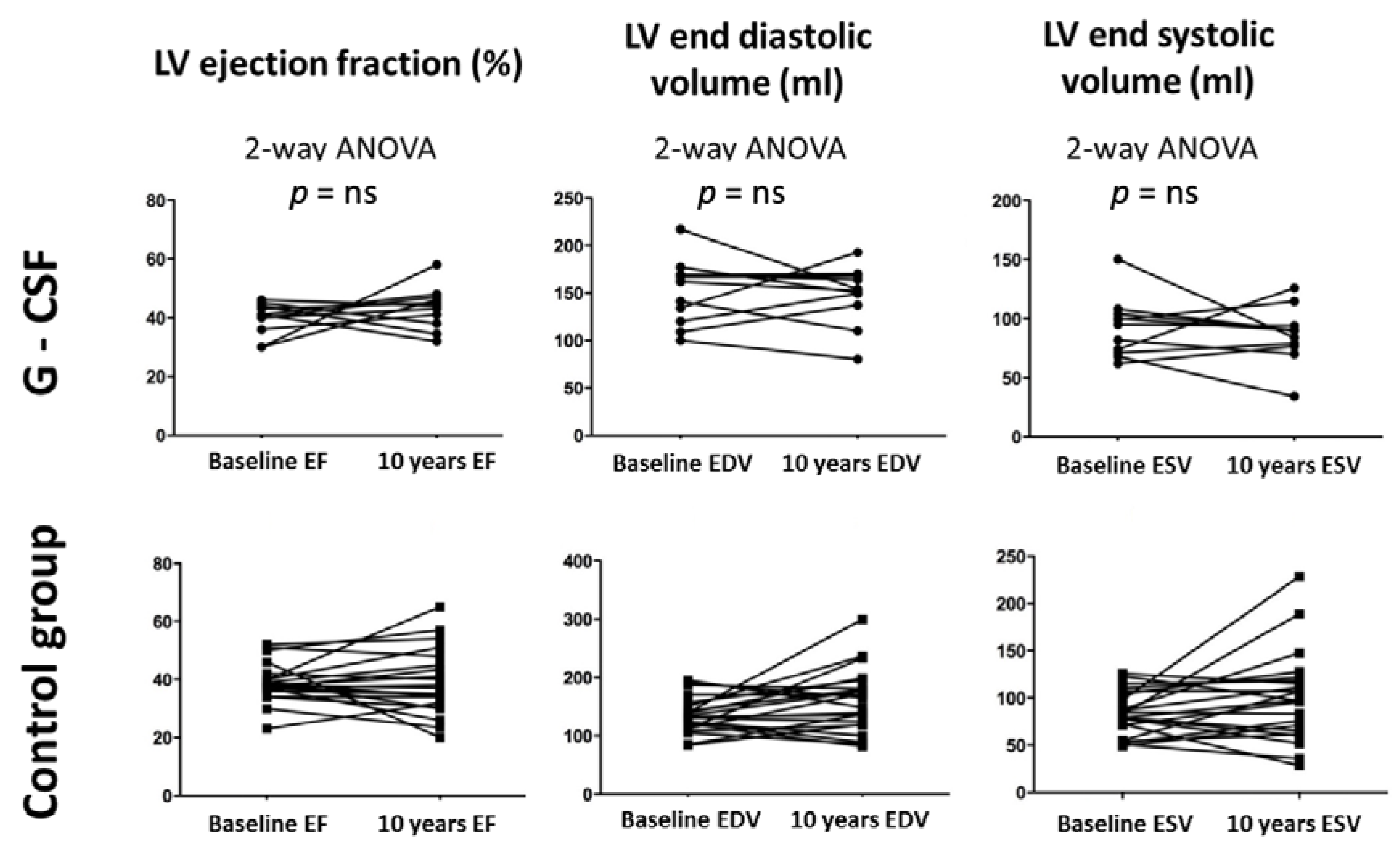
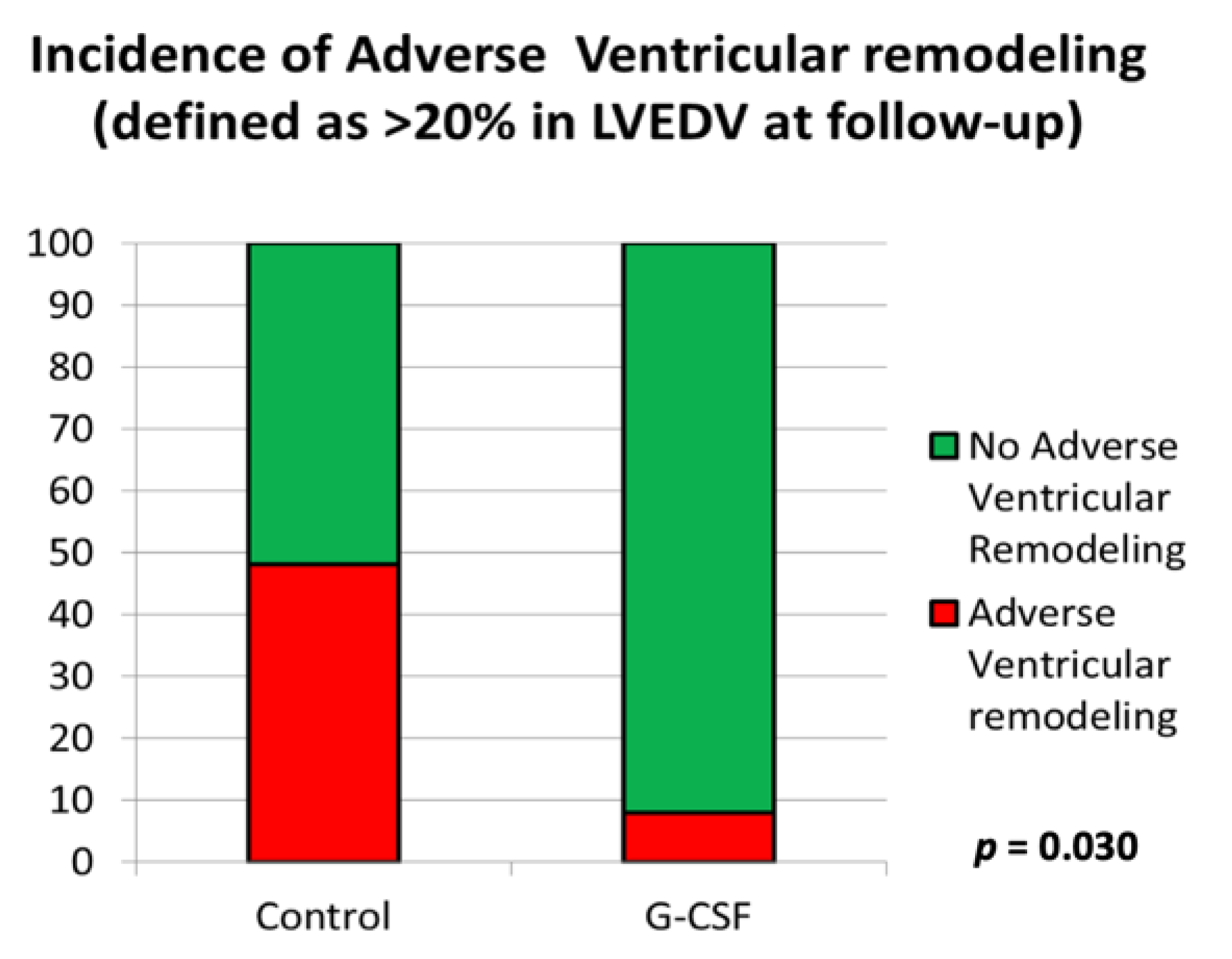
3.2. Echocardiographic Parameters of Ventricular Function
3.3. Rehospitalization Events, Life Expectancy Prognosis, Burden of Symptoms and Health-Related Quality of Life at 10-Year Follow-Up
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Fundings
Conflicts of Interest
References
- Ertl, G.; Frantz, S. Healing after myocardial infarction. Cardiovasc. Res. 2005, 66, 22–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talman, V.; Ruskoaho, H. Cardiac fibrosis in myocardial infarction-from repair and remodeling to regeneration. Cell Tissue Res. 2016, 365, 563–581. [Google Scholar] [CrossRef] [Green Version]
- Sürder, D.; Manka, R.; Cicero, V.L.; Moccetti, T.; Rufibach, K.; Soncin, S.; Turchetto, L.; Radrizzani, M.; Astori, G.; Schwitter, J.; et al. Intracoronary Injection of Bone Marrow-Derived Mononuclear Cells Early or Late After Acute Myocardial Infarction: Effects on Global Left Ventricular Function. Circulation 2013, 127, 1968–1979. [Google Scholar] [CrossRef] [Green Version]
- Traverse, J.H.; Henry, T.D.; Pepine, C.J.; Willerson, J.T.; Zhao, D.X.M.; Ellis, S.G.; Forder, J.R.; Anderson, R.D.; Hatzopoulos, A.K.; Penn, M.S.; et al. Effect of the Use and Timing of Bone Marrow Mononuclear Cell Delivery on Left Ventricular Function After Acute Myocardial Infarction. JAMA 2012, 308, 2380–2389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leone, A.M.; Galiuto, L.; Garramone, B.; Rutella, S.; Giannico, M.B.; Brugaletta, S.; Perfetti, M.; Liuzzo, G.; Porto, I.; Burzotta, F.; et al. Usefulness of Granulocyte Colony-Stimulating Factor in Patients with a Large Anterior Wall Acute Myocardial Infarction to Prevent Left Ventricular Remodeling (The Rigenera Study). Am. J. Cardiol. 2007, 100, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Delewi, R.; Hirsch, A.; Tijssen, J.G.; Schächinger, V.; Wojakowski, W.; Roncalli, J.; Aakhus, S.; Erbs, S.; Assmus, B.; Tendera, M.; et al. Impact of intracoronary bone marrow cell therapy on left ventricular function in the setting of ST-segment elevation myocardial infarction: A collaborative meta-analysis. Eur. Heart J. 2013, 35, 989–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, S.A.; Zhang, H.; Doree, C.; Mathur, A.; Martin-Rendon, E.; Martin-Rendon, E. Stem cell treatment for acute myocardial infarction. Cochrane Database Syst. Rev. 2015, CD006536. [Google Scholar] [CrossRef]
- Clifford, D.M.; Fisher, S.A.; Brunskill, S.; Doree, C.; Mathur, A.; Watt, S.; Martin-Rendon, E. Stem cell treatment for acute myocardial infarction. Cochrane Database Syst. Rev. 2012, CD006536. [Google Scholar] [CrossRef] [Green Version]
- Clifford, D.M.; Fisher, S.A.; Brunskill, S.J.; Doree, C.; Mathur, A.; Clarke, M.J.; Watt, S.M.; Martin-Rendon, E. Long-Term Effects of Autologous Bone Marrow Stem Cell Treatment in Acute Myocardial Infarction: Factors That May Influence Outcomes. PLoS ONE 2012, 7, e37373. [Google Scholar] [CrossRef] [Green Version]
- Leone, A.M.; Rutella, S.; Bonanno, G.; Abbate, A.; Rebuzzi, A.G.; Giovannini, S.; Lombardi, M.; Galiuto, L.; Liuzzo, G.; Andreotti, F.; et al. Mobilization of bone marrow-derived stem cells after myocardial infarction and left ventricular function. Eur. Heart J. 2005, 26, 1196–1204. [Google Scholar] [CrossRef] [Green Version]
- Roohi, A.; Moazzami, B. Granulocyte colony stimulating factor therapy for acute myocardial infarction. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Galli, A.; Lombardi, F. Postinfarct Left Ventricular Remodelling: A Prevailing Cause of Heart Failure. Cardiol. Res. Pract. 2016, 2016, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Flachskampf, F.A.; Schmid, M.; Rost, C.; Achenbach, S.; DeMaria, A.N.; Daniel, W.G. Cardiac imaging after myocardial infarction. Eur. Heart J. 2010, 32, 272–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rector, T.S.; Cohn, J.N. Assessment of patient outcome with the Minnesota Living with Heart Failure questionnaire: Reliability and validity during a randomized, double-blind, placebo-controlled trial of pimobendan. Am. Heart J. 1992, 124, 1017–1025. [Google Scholar] [CrossRef]
- Levy, W.; Mozaffarian, D.; Linker, D.T.; Sutradhar, S.C.; Anker, S.D.; Cropp, A.B.; Anand, I.; Maggioni, A.; Burton, P.; Sullivan, M.D.; et al. The Seattle Heart Failure Model. Circulation 2006, 113, 1424–1433. [Google Scholar] [CrossRef]
- Levy, W. Seattle Heart Failure Model. Am. J. Cardiol. 2013, 111, 1235. [Google Scholar] [CrossRef] [Green Version]
- Cohn, J.N.; Ferrari, R.; Sharpe, N.; on Behalf of an International Forum on Cardiac Remodeling. Cardiac remodeling—Concepts and clinical implications: A consensus paper from an international forum on cardiac remodeling. J. Am. Coll. Cardiol. 2000, 35, 569–582. [Google Scholar] [CrossRef] [Green Version]
- Ince, H.; Petzsch, M.; Kleine, H.D.; Eckard, H.; Rehders, T.; Burska, D.; Kische, S.; Freund, M.; Nienaber, C.A. Prevention of left ventricular remodeling with granulocyte colony-stimulating factor after acute myocardial infarction: Final 1-year results of the Front-Integrated Revascularization and Stem Cell Liberation in Evolving Acute Myocardial Infarction by Granulocyte Colony-Stimulating Factor (FIRSTLINE-AMI) Trial. Circulation 2005, 112, I73–I80. [Google Scholar]
- Achilli, F.; Malafronte, C.; Maggiolini, S.; Lenatti, L.; Squadroni, L.; Gibelli, G.; Capogrossi, M.C.; Dadone, V.; Gentile, F.; Bassetti, B.; et al. G-CSF treatment for STEMI: Final 3-year follow-up of the randomised placebo-controlled STEM-AMI trial. Heart 2014, 100, 574–581. [Google Scholar] [CrossRef]
- D’Amario, D.; Leone, A.M.; Borovac, J.A.; Cannata, F.; Siracusano, A.; Niccoli, G.; Crea, F. Granulocyte colony-stimulating factor for the treatment of cardiovascular diseases: An update with a critical appraisal. Pharmacol. Res. 2018, 127, 67–76. [Google Scholar] [CrossRef]
- Mohri, T.; Iwakura, T.; Nakayama, H.; Fujio, Y. JAK-STAT signaling in cardiomyogenesis of cardiac stem cells. JAK-STAT 2012, 1, 125–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, M.; Qin, Y.; Takano, H.; Minamino, T.; Zou, Y.; Toko, H.; Ohtsuka, M.; Matsuura, K.; Sano, M.; Nishi, J.-I.; et al. G-CSF prevents cardiac remodeling after myocardial infarction by activating the Jak-Stat pathway in cardiomyocytes. Nat. Med. 2005, 11, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Okada, H.; Takemura, G.; Li, Y.; Ohno, T.; Li, L.; Maruyama, R.; Esaki, M.; Miyata, S.; Kanamori, H.; Ogino, A.; et al. Effect of a long-term treatment with a low-dose granulocyte colony-stimulating factor on post-infarction process in the heart. J. Cell. Mol. Med. 2008, 12, 1272–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeffer, M.A.; Braunwald, E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation 1990, 81, 1161–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leone, A.M.; D’Amario, D.; Teofili, L.; Basile, E.; Cannata, F.; Graziani, F.; Marzilli, M.; Russo, M.A.; Tarantini, G.; Ceconi, C.; et al. The combined effect of subcutaneous granulocyte- colony stimulating factor and myocardial contrast echocardiography with intravenous infusion of sulfur hexafluoride on post-infarction left ventricular function, the RIGENERA 2.0 trial: Study protocol for a randomized controlled trial. Trials 2016, 17, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Control Group n = 26 | G-CSF Group n = 12 | p |
|---|---|---|---|
| Clinical Characteristics | |||
| Age (years ± SD) | 66 ± 11 | 63 ± 11 | 0.35 |
| Male (n, (%)) | 21 (81) | 12 (100) | 0.10 |
| Female (n, (%)) | 5 (19) | 0 (0) | 0.10 |
| Hypertension (n, (%)) | 18 (69) | 6 (50) | 0.25 |
| Current smoker (n, (%)) | 17 (65) | 9 (75) | 0.55 |
| Dyslipidemia (n, (%)) | 10 (39) | 8 (67) | 0.11 |
| Diabetes mellitus (n, (%)) | 4 (15) | 3 (25) | 0.48 |
| Family history of CAD (n, (%)) | 7 (27) | 7 (59) | 0.06 |
| STEMI (n, (%)) | 26 (100) | 12 (100) | 1 |
| Primary percutaneous intervention (n, (%)) | 26 (100) | 12 (100) | 1 |
| Thrombolysis (n, (%)) | 11 (42) | 7 (58) | 0.36 |
| Troponin T (mean ± SD) (ng/mL) | 14.7 ± 8.55 | 11.3 ± 7.1 | 0.20 |
| Multivessel CAD (n, (%)) | 2 (8) | 0 (0) | 0.32 |
| Pharmacotherapy | |||
| Beta-blockers (n, (%)) | 25 (96) | 11 (92) | 0.56 |
| ACE inhibitors (n, (%)) | 22 (85) | 12 (100) | 0.15 |
| Statins (n, (%)) | 22 (85) | 11 (92) | 0.55 |
| Aspirin (n, (%)) | 25 (96) | 12 (100) | 0.49 |
| ARBs (n, (%)) | 5 (19) | 3 (25) | 0.69 |
| Diuretics (n, (%)) | 13 (50) | 8 (67) | 0.34 |
| Heparin (n, (%)) | 1 (4) | 1 (8) | 0.56 |
| Clopidogrel (n, (%)) | 14 (54) | 10 (83) | 0.08 |
| Echocardiography at enrollment | |||
| LV Ejection Fraction (LVEF) (%) | 39.1 ± 8 | 39.3 ± 5 | 0.95 |
| LV End Diastolic Volume (LVEDV) (mL) | 141 ± 35 | 149 ± 34 | |
| LV End Systolic Volume (LVESV) (mL) | 86 ± 24 | 91 ± 24 | |
| Wall Motion Score Index (WMSI) | 2.1 ± 0.4 | 2.0 ± 0.2 | |
| Control Group n = 21 | G-CSF Group n = 11 | p | |
|---|---|---|---|
| Medications at 10-years follow-up | |||
| Beta-blockers (n, (%)) | 19 (90) | 9 (82) | 0.48 |
| ACE inhibitors/ARBs (n, (%)) | 18 (86) | 10 (91) | 0.67 |
| Statins (n, (%)) | 18 (86) | 9 (82) | 0.77 |
| Aspirin (n, (%)) | 20 (95) | 10 (91) | 0.63 |
| Diuretics (n, (%)) | 14 (67) | 7 (64) | 0.86 |
| P2Y12 inhibitor (n, (%)) | 3 (14) | 2 (18) | 0.77 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leone, A.M.; D’Amario, D.; Cannata, F.; Graziani, F.; Borovac, J.A.; Leone, G.; De Stefano, V.; Basile, E.; Siracusano, A.; Galiuto, L.; et al. The Effects of Granulocyte Colony-Stimulating Factor in Patients with a Large Anterior Wall Acute Myocardial Infarction to Prevent Left Ventricular Remodeling: A 10-Year Follow-Up of the RIGENERA Study. J. Clin. Med. 2020, 9, 1214. https://doi.org/10.3390/jcm9041214
Leone AM, D’Amario D, Cannata F, Graziani F, Borovac JA, Leone G, De Stefano V, Basile E, Siracusano A, Galiuto L, et al. The Effects of Granulocyte Colony-Stimulating Factor in Patients with a Large Anterior Wall Acute Myocardial Infarction to Prevent Left Ventricular Remodeling: A 10-Year Follow-Up of the RIGENERA Study. Journal of Clinical Medicine. 2020; 9(4):1214. https://doi.org/10.3390/jcm9041214
Chicago/Turabian StyleLeone, Antonio Maria, Domenico D’Amario, Francesco Cannata, Francesca Graziani, Josip A. Borovac, Giuseppe Leone, Valerio De Stefano, Eloisa Basile, Andrea Siracusano, Leonarda Galiuto, and et al. 2020. "The Effects of Granulocyte Colony-Stimulating Factor in Patients with a Large Anterior Wall Acute Myocardial Infarction to Prevent Left Ventricular Remodeling: A 10-Year Follow-Up of the RIGENERA Study" Journal of Clinical Medicine 9, no. 4: 1214. https://doi.org/10.3390/jcm9041214
APA StyleLeone, A. M., D’Amario, D., Cannata, F., Graziani, F., Borovac, J. A., Leone, G., De Stefano, V., Basile, E., Siracusano, A., Galiuto, L., Locorotondo, G., Porto, I., Vergallo, R., Canonico, F., Restivo, A., Rebuzzi, A. G., & Crea, F. (2020). The Effects of Granulocyte Colony-Stimulating Factor in Patients with a Large Anterior Wall Acute Myocardial Infarction to Prevent Left Ventricular Remodeling: A 10-Year Follow-Up of the RIGENERA Study. Journal of Clinical Medicine, 9(4), 1214. https://doi.org/10.3390/jcm9041214