Association between the 2018 WCRF/AICR and the Low-Risk Lifestyle Scores with Colorectal Cancer Risk in the Predimed Study

 ,
,  , ,
, ,  ,
,  , ,
, ,  ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Ascertainment of Incident and Fatal CRC
2.4. Dietary Assessment
2.5. Other Lifestyle Variables Assessment
2.6. 2018 WCRF/AICR Score Operationalization
2.7. Low Risk Lifestyle Score Operationalization
2.8. Statistical Analyses
3. Results
3.1. Baseline Characteristics of the Participants
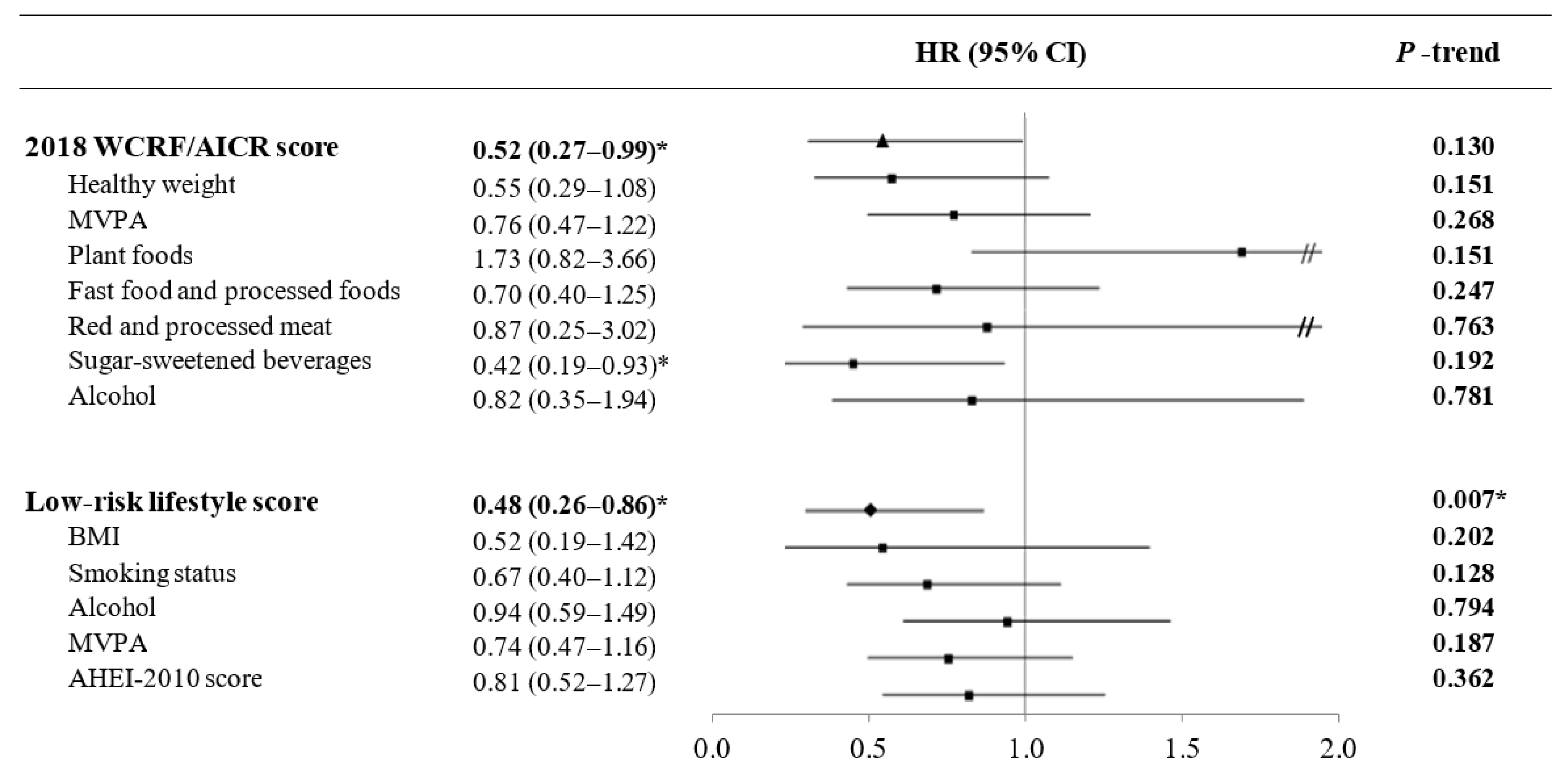
3.2. World Cancer Research Fund/American Institute for Cancer Research and Low Risk Lifestyle Scores and Risk of Colorectal Cancer
3.3. Individual Components of the Scores and Risk of CRC
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report. 2018. Available online: https://www.wcrf.org/dietandcancer (accessed on 15 February 2020).
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Steck, S.E.; Guinter, M.; Zheng, J.; Thomson, C.A. Index-Based Dietary Patterns and Colorectal Cancer Risk: A Systematic Review. Adv. Nutr. Int. Rev. J. 2015, 6, 763–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: An Updated Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2018, 118, 74–100.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romaguera, D.; Vergnaud, A.-C.; Peeters, P.H.; van Gils, C.H.; Chan, D.S.M.; Ferrari, P.; Romieu, I.; Jenab, M.; Slimani, N.; Clavel-Chapelon, F.; et al. Is concordance with World Cancer Research Fund/American Institute for Cancer Research guidelines for cancer prevention related to subsequent risk of cancer? Results from the EPIC study. Am. J. Clin. Nutr. 2012, 96, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Pan, A.; Wang, D.D.; Liu, X.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C.; et al. Impact of Healthy Lifestyle Factors on Life Expectancies in the US Population. Circulation 2018, 138, 345–355. [Google Scholar] [CrossRef]
- Thomson, C.A.; McCullough, M.L.; Wertheim, B.C.; Chlebowski, R.T.; Martinez, M.E.; Stefanick, M.L.; Rohan, T.E.; Manson, J.E.; Tindle, H.A.; Ockene, J.; et al. Nutrition and physical activity cancer prevention guidelines, cancer risk, and mortality in the women’s health initiative. Cancer Prev. Res. 2014, 7, 42–53. [Google Scholar] [CrossRef] [Green Version]
- Kabat, G.C.; Matthews, C.E.; Kamensky, V.; Hollenbeck, A.R.; Rohan, T.E. Adherence to cancer prevention guidelines and cancer incidence, cancer mortality, and total mortality: A prospective cohort study. Am. J. Clin. Nutr. 2015, 101, 558–569. [Google Scholar] [CrossRef] [Green Version]
- Makarem, N.; Lin, Y.; Bandera, E.V.; Jacques, P.F.; Parekh, N. Concordance with World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) guidelines for cancer prevention and obesity-related cancer risk in the Framingham Offspring cohort (1991–2008). Cancer Causes Control 2015, 26, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Nomura, S.J.O.; Dash, C.; Rosenberg, L.; Yu, J.; Palmer, J.R.; Adams-Campbell, L.L. Is adherence to diet, physical activity, and body weight cancer prevention recommendations associated with colorectal cancer incidence in African American women? Cancer Causes Control 2016, 27, 869–879. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.; Cade, J.E.; Evans, C.E.L.; Hancock, N.; Greenwood, D.C. Does adherence to the World Cancer Research Fund/American Institute of Cancer Research cancer prevention guidelines reduce risk of colorectal cancer in the UK Women’s Cohort Study? Br. J. Nutr. 2018, 119, 340–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petimar, J.; Smith-Warner, S.A.; Rosner, B.; Chan, A.T.; Giovannucci, E.L.; Tabung, F.K. Adherence to the World Cancer Research Fund/American Institute for Cancer Research 2018 Recommendations for Cancer Prevention and Risk of Colorectal Cancer. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1469–1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romaguera, D.; Gracia-Lavedan, E.; Molinuevo, A.; de Batlle, J.; Mendez, M.; Moreno, V.; Vidal, C.; Castelló, A.; Pérez-Gómez, B.; Martín, V.; et al. Adherence to nutrition-based cancer prevention guidelines and breast, prostate and colorectal cancer risk in the MCC-Spain case-control study. Int. J. Cancer 2017, 141, 83–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turati, F.; Bravi, F.; Di Maso, M.; Bosetti, C.; Polesel, J.; Serraino, D.; Dalmartello, M.; Giacosa, A.; Montella, M.; Tavani, A.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations and colorectal cancer risk. Eur. J. Cancer 2017, 85, 86–94. [Google Scholar] [CrossRef] [PubMed]
- El Kinany, K.; Huybrechts, I.; Kampman, E.; Boudouaya, H.A.; Hatime, Z.; Mint Sidi Deoula, M.; El Asri, A.; Benslimane, A.; Nejjari, C.; Ibrahimi, S.A.; et al. Concordance with the World Cancer Research Fund/American Institute for Cancer Research recommendations for cancer prevention and colorectal cancer risk in Morocco: A large, population-based case–control study. Int. J. Cancer 2019, 145, 1829–1837. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Schoufour, J.; Wang, D.D.; Dhana, K.; Pan, A.; Liu, X.; Song, M.; Liu, G.; Shin, H.J.; Sun, Q.; et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: Prospective cohort study. BMJ 2020, 368, l6669. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.; Li, Y.; Hu, Y.; Zong, G.; Li, S.; Rimm, E.B.; Hu, F.B.; Manson, J.E.; Rexrode, K.M.; Shin, H.J.; et al. Influence of Lifestyle on Incident Cardiovascular Disease and Mortality in Patients With Diabetes Mellitus. J. Am. Coll. Cardiol. 2018, 71, 2867–2876. [Google Scholar] [CrossRef]
- Martínez-González, M.Á.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Covas, M.I.; Fiol, M.; Wärnberg, J.; Arós, F.; Ruíz-Gutiérrez, V.; Lamuela-Raventós, R.M.; et al. Cohort profile: Design and methods of the PREDIMED study. Int. J. Epidemiol. 2012, 41, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Mataix, V.J. Tabla de Composicion de Alimentos [Food Composition Tables], 4th ed.; Universidad de Granada: Granada, Spain, 2003. [Google Scholar]
- Moreiras, O.; Cabrera, L.C.A. Tablas de Composición de Alimentos [Food Composition Tables]; Ediciones Pirámide: Madrid, Spain, 2005; Volume 9. [Google Scholar]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the minnesota leisure time physical activity questionnaire in Spanish men. The MARATHOM Investigators. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Garcia, M.; Aguilar, A.; Molina, L.; Covas, M.I.; Marrugat, J. Validation of the minnesota leisure time physical activity questionnaire in Spanish women. Investigators of the MARATDON Group. Med. Sci. Sports Exerc. 2000, 32, 1431–1437. [Google Scholar] [CrossRef]
- Jankovic, N.; Geelen, A.; Winkels, R.M.; Mwungura, B.; Fedirko, V.; Jenab, M.; Illner, A.K.; Brenner, H.; Ordóñez-Mena, J.M.; Kiefte de Jong, J.C.; et al. Adherence to the WCRF/AICR dietary recommendations for cancer prevention and risk of cancer in elderly from Europe and the United States: A meta-analysis within the CHANCES project. Cancer Epidemiol. Biomark. Prev. 2017, 26, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Hastert, T.A.; White, E. Association between meeting the WCRF/AICR cancer prevention recommendations and colorectal cancer incidence: Results from the VITAL cohort. Cancer Causes Control 2016, 27, 1347–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; AICR: Washington, DC, USA, 2007.
- Lavalette, C.; Adjibade, M.; Srour, B.; Sellem, L.; Fiolet, T.; Hercberg, S.; Latino-Martel, P.; Fassier, P.; Deschasaux, M.; Kesse-Guyot, E.; et al. Cancer-specific and general nutritional scores and cancer risk: Results from the prospective nutrinet-santé cohort. Cancer Res. 2018, 78, 4427–4435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shams-White, M.M.; Brockton, N.T.; Mitrou, P.; Romaguera, D.; Brown, S.; Bender, A.; Kahle, L.L.; Reedy, J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) cancer prevention recommendations: A standardized scoring system. Nutrients 2019, 11, 1572. [Google Scholar] [CrossRef] [Green Version]
- Geneva: World Health Organization. World Health Organization (WHO) Global Health Observatory. Available online: https://www.who.int/gho/database/en/ (accessed on 15 February 2020).
- Choi, Y.; Giovannucci, E.; Lee, J.E. Glycaemic index and glycaemic load in relation to risk of diabetes-related cancers: A meta-analysis. Br. J. Nutr. 2012, 108, 1934–1947. [Google Scholar] [CrossRef]
- Suikkari, A.-M.; Koivisto, V.A.; Rutanen, E.-M.; YKI-Järvinen, H.; Karonen, S.-L.; Seppälä, M. Insulin Regulates the Serum Levels of Low Molecular Weight Insulin-Like Growth Factor-Binding Protein*. J. Clin. Endocrinol. Metab. 1988, 66, 266–272. [Google Scholar] [CrossRef]
- Le Roith, D. Insulin-like growth factors. N. Engl. J. Med. 1997, 336, 633–640. [Google Scholar] [CrossRef]
- Bruce, W.R.; Wolever, T.M.S.; Giacca, A. Mechanisms linking diet and colorectal cancer: The possible role of insulin resistance. Nutr. Cancer 2000, 37, 19–26. [Google Scholar] [CrossRef]
- Miele, C.; Rochford, J.J.; Filippa, N.; Giorgetti-Peraldi, S.; Van Obberghen, E. Insulin and insulin-like growth factor-i induce vascular endothelial growth factor mrna expression via different signaling pathways. J. Biol. Chem. 2000, 275, 21695–21702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, T.J.S.; Wolfson, J.A.; Jiao, D.; Crupain, M.J.; Rangan, U.; Sapkota, A.; Bleich, S.N.; Nachman, K.E. Caramel color in soft drinks and exposure to 4-methylimidazole: A quantitative risk assessment. PLoS ONE 2015, 10, e0118138. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total Study Population n = 7216 | Colorectal Cancer Events n = 97 | Non-Events n = 7119 | p-Value b | |
|---|---|---|---|---|
| 2018 WCRF/AICR score | 3.8 (3.3–4.4) | 3.8 (3.2–4.2) | 3.8 (3.3–4.4) | 0.110 |
| Low-risk lifestyle score | 2 (1–2) | 1 (1–2) | 2 (1–2) | 0.021 * |
| Age, years | 67 (62–72) | 67 (62–72) | 67 (62–72) | 0.269 |
| Women, % (n) | 57.4 (4145) | 41.2 (40) | 57.7 (4105) | 0.001 * |
| Education level, % (n) | ||||
| Primary, secondary, high school | 92.9 (6700) | 92.8 (90) | 92.9 (6610) | 0.980 |
| University/graduate | 7.2 (516) | 7.2 (7) | 7.2 (509) | |
| Age at diagnosis of cancer, years | 72.4 (66.8–76.4) | 72.4 (66.8–76.4) | – | – |
| Family history of cancer, % (n) | 49.2 (3548) | 41.2 (40) | 49.3 (3508) | 0.116 |
| Cancer location | ||||
| Colon, % (n) | 77 (79.4) | 77 (79.4) | – | – |
| Rectum, % (n) | 20 (20.6) | 20 (20.6) | – | – |
| Diabetes, % (n) | 48.9 (3527) | 51.6 (50) | 48.8 (3477) | 0.597 |
| Hypertension, % (n) | 82.7 (5970) | 80.4 (78) | 82.8 (5892) | 0.543 |
| Waist circumference, cm | ||||
| Women | 99 (91–105) | 98.2 (92–107) | 99 (91–105) | 0.614 |
| Men | 103 (97–109) | 103 (96–11) | 103 (97–109) | 0.441 |
| BMI, kg/m2 | 29.7 (27.2–32.5) | 29.9 (27.6–32.3) | 29.7 (27.2–32.5) | 0.813 |
| MVPA, min./wk. | 42.2 (0–296.5) | 52.5 (0–311) | 42.1 (0–296.5) | 0.982 |
| Smoking status, % (n) | ||||
| Never smokers | 61.5 (4438) | 47.4 (46) | 61.7 (4392) | 0.011 * |
| Former smokers | 24.6 (1774) | 30.9 (30) | 24.5 (1744) | |
| Current smokers | 13.9 (1004) | 21.7 (21) | 13.8 (983) | |
| Current medication, % (n) | ||||
| Aspirin | 22.4 (1613) | 24.7 (24) | 22.3 (1589) | 0.758 |
| HRT (only in women) | 2.8 (115) | 5 (2) | 2.8 (113) | 0.234 |
| Intervention groups, % (n) | ||||
| MedDiet + EVOO | 34.3 (2474) | 39.2 (38) | 34.2 (2436) | 0.390 |
| MedDiet + nuts | 32.7 (2360) | 34.0 (33) | 32.7 (2327) | |
| Control low–fat diet | 33.0 (2382) | 26.8 (26) | 33.1 (2356) | |
| Energy intake (kcal/day) | 2184.4 (1842.9–2579.7) | 2183.4 (1942–2669.3) | 2184.5 (1841.6–2578.2) | 0.263 |
| AHEI–2010 score | 64.4 (58.8–70.2) | 62.6 (57.4–69.1) | 64.4 (58.9–70.2) | 0.210 |
| Food consumption, g/day | ||||
| Vegetables | 313.7 (235–408.7) | 289.2 (221.2–367) | 314 (235–409.3) | 0.164 |
| Fruits | 333.1 (227.2–475) | 324.5 (222.4–459.2) | 333.3 (227.6–475) | 0.454 |
| Legumes | 17.1 (12.6–25.1) | 17.1 (16–25.1) | 17.1 (12.6–25.1) | 0.778 |
| Red and processed meat | 68.1 (42.6–100) | 68.3 (45.7–111.7) | 68.1 (42.4–100) | 0.073 |
| Fast food and processed foods | 72.4 (45.7–109.2) | 77.2 (51–108.6) | 72.4 (45.7–109.2) | 0.746 |
| Sugar-sweetened beverages | 13.3 (0–85.7) | 13.3 (0–99.1) | 13.3 (0–85.7) | 0.388 |
| Alcohol | 1.5 (0–10.4) | 4.3 (0–12.2) | 1.5 (0–10.4) | 0.093 |
| 2018 WCRF/AICR Score | Low-Risk Lifestyle Score | |||
|---|---|---|---|---|
| Continuous Analysis (1-Point Increment), HR (95% CI) | p for Trend | Continuous Analysis (1-Point Increment), HR (95% CI) | p for Trend | |
| Events/non-events (n) | 97/7216 | - | 97/7216 | - |
| Crude model | 0.79 (0.63–0.98) * | 0.033 * | 0.77 (0.62–0.95) * | 0.016 * |
| Model 1 | 0.78 (0.62–0.98) * | 0.034 * | 0.78 (0.64–0.96) * | 0.019 * |
| Model 2 | 0.79 (0.63–0.99) * | 0.045 * | 0.78 (0.64–0.96) * | 0.017 * |
| Component Score, HR (95% CI) | |||||
|---|---|---|---|---|---|
| Healthy weight | 0 | 0.25 | 0.5 | >0.75 | p for trend |
| Events/non-events (n) | 22/1381 | 22/1723 | 33/2233 | 20/1782 | - |
| Crude model | 1.00 | 0.77 (0.41–1.45) | 0.90 (0.50–1.60) | 0.62 (0.33–1.17) | 0.220 |
| Model 1 | 1.00 | 0.71 (0.37–1.33) | 0.85 (0.48–1.54) | 0.54 (0.28–1.06) | 0.135 |
| Model 2 | 1.00 | 0.71 (0.38–1.33) | 0.87 (0.48–1.55) | 0.54 (0.28–1.05) | 0.134 |
| Model 3 | 1.00 | 0.71 (0.38–1.35) | 0.88 (0.49–1.56) | 0.55 (0.29–1.08) | 0.151 |
| Physical activity | 0 | 0.5 | 1 | - | p for trend |
| Events/non-events (n) | 53/3893 | 11/590 | 33/2636 | - | |
| Crude model | 1.00 | 1.25 (0.63–2.48) | 0.82 (0.51–1.32) | - | 0.441 |
| Model 1 | 1.00 | 1.25 (0.63–2.48) | 0.75 (0.46–1.22) | - | 0.254 |
| Model 2 | 1.00 | 1.24 (0.62–2.48) | 0.76 (0.47–1.22) | - | 0.271 |
| Model 3 | 1.00 | 1.24 (0.63–2.46) | 0.76 (0.47–1.22) | - | 0.268 |
| Plant foods | 0-0.5 | >0.5–0.75 | >0.75 | - | p for trend |
| Events/non-events (n) | 14/1345 | 56/3952 | 27/1822 | - | |
| Crude model | 1.00 | 1.38 (0.77–2.47) | 1.66 (0.82–3.34) | - | 0.158 |
| Model 1 | 1.00 | 1.34 (0.75–2.40) | 1.57 (0.78–3.16) | - | 0.210 |
| Model 2 | 1.00 | 1.34 (0.75–2.41) | 1.60 (0.77–3.32) | - | 0.206 |
| Model 3 | 1.00 | 1.38 (0.76–2.49) | 1.73 (0.82–3.66) | - | 0.151 |
| Fast food and processed foods | 0 | 0.5 | 1 | - | p for trend |
| Events/non-events (n) | 18/1201 | 39/2766 | 40/3152 | - | - |
| Crude model | 1.00 | 0.82 (0.46–1.45) | 0.72 (0.41–1.26) | - | 0.258 |
| Model 1 | 1.00 | 0.84 (0.47–1.49) | 0.72 (0.41–1.28) | - | 0.260 |
| Model 2 | 1.00 | 0.85 (0.48–1.49) | 0.73 (0.41–1.29) | - | 0.278 |
| Model 3 | 1.00 | 0.81 (0.47–1.42) | 0.70 (0.40–1.25) | - | 0.247 |
| Red and processed meat | 0 | 0.5 | 1 | - | p for trend |
| Events/non-events (n) | 36/2263 | 58/4577 | 3/279 | - | - |
| Crude model | 1.00 | 0.89 (0.58–1.36) | 0.77 (0.23–2.55) | - | 0.531 |
| Model 1 | 1.00 | 0.95 (0.60–1.48) | 0.87 (0.26–2.94) | - | 0.771 |
| Model 2 | 1.00 | 0.97 (0.62–1.54) | 0.90 (0.26–3.07) | - | 0.868 |
| Model 3 | 1.00 | 0.94 (0.60–1.48) | 0.88 (0.25–3.06) | - | 0.771 |
| Sugar-sweetened beverages | 0 | 0.5 | 1 | - | p for trend |
| Events/non-events (n) | 8/326 | 48/3675 | 41/3118 | - | - |
| Crude model | 1.00 | 0.45 (0.21–0.96) * | 0.45 (0.21–0.94) * | - | 0.298 |
| Model 1 | 1.00 | 0.46 (0.22–0.98) * | 0.43 (0.20–0.90) * | - | 0.174 |
| Model 2 | 1.00 | 0.47 (0.21–1.02) | 0.43 (0.20–0.94) * | - | 0.185 |
| Model 3 | 1.00 | 0.45 (0.21–1.00) | 0.42 (0.19–0.93) * | - | 0.192 |
| Alcohol intake | 0 | 0.5 | 1 | - | p for trend |
| Events/non-events (n) | 7/389 | 60/4111 | 30/2619 | - | - |
| Crude model | 1.00 | 0.86 (0.40–1.86) | 0.68 (0.31–1.52) | - | 0.221 |
| Model 1 | 1.00 | 0.86 (0.40–1.85) | 0.85 (0.38–1.89) | - | 0.771 |
| Model 2 | 1.00 | 0.96 (0.43–2.12) | 0.98 (0.42–2.27) | - | 0.979 |
| Model 3 | 1.00 | 0.82 (0.36–1.87) | 0.82 (0.35–1.94) | - | 0.781 |
| Component Score, HR (95% CI) | |||
|---|---|---|---|
| BMI | 0 | 1 | p for trend |
| Events/non-events (n) | 93/6607 | 4/512 | |
| Crude model | 1.00 | 0.54 (0.20–1.46) | 0.222 |
| Model 1 | 1.00 | 0.52 (0.19–1.41) | 0.200 |
| Model 2 | 1.00 | 0.51 (0.19–1.39) | 0.190 |
| Model 3 | 1.00 | 0.52 (0.19–1.42) | 0.202 |
| Smoking status | 0 | 1 | p for trend |
| Events/non-events (n) | 51/2727 | 46/4392 | |
| Crude model | 1.00 | 0.55 (0.36–0.83) * | 0.004 * |
| Model 1 | 1.00 | 0.66 (0.40–1.11) | 0.119 |
| Model 2 | 1.00 | 0.66 (0.39–1.10) | 0.113 |
| Model 3 | 1.00 | 0.67 (0.40–1.12) | 0.128 |
| Alcohol consumption | 0 | 1 | p for trend |
| Events/non-events (n) | 65/4992 | 32/2127 | |
| Crude model | 1.00 | 1.12 (0.73–1.71) | 0.594 |
| Model 1 | 1.00 | 0.90 (0.58–1.39) | 0.626 |
| Model 2 | 1.00 | 0.88 (0.56–1.39) | 0.594 |
| Model 3 | 1.00 | 0.94 (0.59–1.49) | 0.794 |
| Physical activity | 0 | 1 | p for trend |
| Events/non-events (n) | 64/4483 | 33/2636 | |
| Crude model | 1.00 | 0.79 (0.51–1.24) | 0.303 |
| Model 1 | 1.00 | 0.72 (0.45–1.13) | 0.155 |
| Model 2 | 1.00 | 0.71 (0.45–1.12) | 0.146 |
| Model 3 | 1.00 | 0.74 (0.47–1.16) | 0.187 |
| AHEI-2010 score | 0 | 1 | p for trend |
| Events/non-events (n) | 64/4266 | 33/2853 | 0.268 |
| Crude model | 1.00 | 0.81 (0.52–1.25) | 0.269 |
| Model 1 | 1.00 | 0.78 (0.51–1.21) | 0.268 |
| Model 2 | 1.00 | 0.78 (0.50–1.21) | 0.268 |
| Model 3 | 1.00 | 0.81 (0.52–1.27) | 0.362 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrubés, L.; Babio, N.; Hernández-Alonso, P.; Toledo, E.; Ramírez Sabio, J.B.; Estruch, R.; Ros, E.; Fitó, M.; Alonso-Gómez, A.M.; Fiol, M.; et al. Association between the 2018 WCRF/AICR and the Low-Risk Lifestyle Scores with Colorectal Cancer Risk in the Predimed Study. J. Clin. Med. 2020, 9, 1215. https://doi.org/10.3390/jcm9041215
Barrubés L, Babio N, Hernández-Alonso P, Toledo E, Ramírez Sabio JB, Estruch R, Ros E, Fitó M, Alonso-Gómez AM, Fiol M, et al. Association between the 2018 WCRF/AICR and the Low-Risk Lifestyle Scores with Colorectal Cancer Risk in the Predimed Study. Journal of Clinical Medicine. 2020; 9(4):1215. https://doi.org/10.3390/jcm9041215
Chicago/Turabian StyleBarrubés, Laura, Nancy Babio, Pablo Hernández-Alonso, Estefania Toledo, Judith B. Ramírez Sabio, Ramón Estruch, Emilio Ros, Montserrat Fitó, Angel M Alonso-Gómez, Miquel Fiol, and et al. 2020. "Association between the 2018 WCRF/AICR and the Low-Risk Lifestyle Scores with Colorectal Cancer Risk in the Predimed Study" Journal of Clinical Medicine 9, no. 4: 1215. https://doi.org/10.3390/jcm9041215
APA StyleBarrubés, L., Babio, N., Hernández-Alonso, P., Toledo, E., Ramírez Sabio, J. B., Estruch, R., Ros, E., Fitó, M., Alonso-Gómez, A. M., Fiol, M., Lapetra, J., Serra-Majem, L., Pintó, X., Ruiz-Canela, M., Corella, D., Castañer, O., Macías-González, M., & Salas-Salvadó, J. (2020). Association between the 2018 WCRF/AICR and the Low-Risk Lifestyle Scores with Colorectal Cancer Risk in the Predimed Study. Journal of Clinical Medicine, 9(4), 1215. https://doi.org/10.3390/jcm9041215