Multiparametric Modelling of Survival in Pancreatic Ductal Adenocarcinoma Using Clinical, Histomorphological, Genetic and Image-Derived Parameters

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- SEER Cancer Statistics Review (CSR) 1975-2014. Available online: https://seer.cancer.gov/archive/csr/1975_2014/ (accessed on 23 April 2020).
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef]
- Biankin, A.V.; Waddell, N.; Kassahn, K.S.; Gingras, M.C.; Muthuswamy, L.B.; Johns, A.L.; Miller, D.K.; Wilson, P.J.; Patch, A.M.; Wu, J.; et al. Pancreatic cancer genomes reveal aberrations in axon guidance pathway genes. Nature 2012, 491, 399–405. [Google Scholar] [CrossRef]
- Waddell, N.; Pajic, M.; Patch, A.M.; Chang, D.K.; Kassahn, K.S.; Bailey, P.; Johns, A.L.; Miller, D.; Nones, K.; Quek, K.; et al. Whole genomes redefine the mutational landscape of pancreatic cancer. Nature 2015, 518, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Yachida, S.; White, C.M.; Naito, Y.; Zhong, Y.; Brosnan, J.A.; Macgregor-Das, A.M.; Morgan, R.A.; Saunders, T.; Laheru, D.A.; Herman, J.M.; et al. Clinical significance of the genetic landscape of pancreatic cancer and implications for identification of potential long-term survivors. Clin. Cancer Res. 2012, 18, 6339–6347. [Google Scholar] [CrossRef] [Green Version]
- Tascilar, M.; Skinner, H.G.; Rosty, C.; Sohn, T.; Wilentz, R.E.; Offerhaus, G.J.A.; Adsay, V.; Abrams, R.A.; Cameron, J.L.; Kern, S.E.; et al. The SMAD4 protein and prognosis of pancreatic ductal adenocarcinoma. Clin. Cancer Res. 2001, 7, 4115–4121. [Google Scholar] [PubMed]
- Collisson, E.A.; Sadanandam, A.; Olson, P.; Gibb, W.J.; Truitt, M.; Gu, S.; Cooc, J.; Weinkle, J.; Kim, G.E.; Jakkula, L.; et al. Subtypes of pancreatic ductal adenocarcinoma and their differing responses to therapy. Nat. Med. 2011, 17, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Porter, R.L.; Magnus, N.K.; Thapar, V.; Morris, R.; Szabolcs, A.; Neyaz, A.; Kulkarni, A.S.; Tai, E.; Chougule, A.; Hillis, A.; et al. Epithelial to mesenchymal plasticity and differential response to therapies in pancreatic ductal adenocarcinoma. Proc. Natl. Acad. Sci. USA 2019, 116, 26835–26845. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mei, D.; Luo, Y.; Wang, Y.; Gong, J. CT texture analysis of lung adenocarcinoma: Can Radiomic features be surrogate biomarkers for EGFR mutation statuses. Cancer Imaging 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kaissis, G.A.; Ziegelmayer, S.; Lohöfer, F.K.; Harder, F.N.; Jungmann, F.; Sasse, D.; Muckenhuber, A.; Yen, H.Y.; Steiger, K.; Siveke, J.; et al. Image-based molecular Phenotyping of pancreatic ductal adenocarcinoma. J. Clin. Med. 2020, 9, 724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaissis, G.; Ziegelmayer, S.; Lohöfer, F.; Steiger, K.; Algül, H.; Muckenhuber, A.; Yen, H.Y.; Rummeny, E.; Friess, H.; Schmid, R.; et al. A machine learning algorithm predicts molecular subtypes in pancreatic ductal adenocarcinoma with differential response to gemcitabine-based versus FOLFIRINOX chemotherapy. PLoS ONE 2019, 14, 664540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zhu, Y.; Burnside, E.S.; Drukker, K.; Hoadley, K.A.; Fan, C.; Conzen, S.D.; Whitman, G.J.; Sutton, E.J.; Net, J.M.; et al. MR imaging radiomics signatures for predicting the risk of breast cancer recurrence as given by research versions of MammaPrint, oncotype DX, and PAM50 gene assays. Radiology 2016, 281, 382–391. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.; Dong, D.; Chen, Z.; Fang, M.; Zhang, L.; Song, J.; Yu, D.; Zang, Y.; Liu, Z.; Shi, J.; et al. Radiomic signature as a diagnostic factor for histologic subtype classification of non-small cell lung cancer. Eur. Radiol. 2018, 28, 2772–2778. [Google Scholar] [CrossRef]
- Zhang, Y.; Lobo-Mueller, E.M.; Karanicolas, P.; Gallinger, S.; Haider, M.A.; Khalvati, F. CNN-based survival model for pancreatic ductal adenocarcinoma in medical imaging. BMC Med. Imaging 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (strobe) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Muckenhuber, A.; Berger, A.K.; Schlitter, A.M.; Steiger, K.; Konukiewitz, B.; Trumpp, A.; Eils, R.; Werner, J.; Friess, H.; Esposito, I.; et al. Pancreatic ductal adenocarcinoma subtyping using the biomarkers hepatocyte nuclear factor-1A and cytokeratin-81 correlates with outcome and treatment response. Clin. Cancer Res. 2018, 24, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Schlitter, A.M.; Segler, A.; Steiger, K.; Michalski, C.W.; Jäger, C.; Konukiewitz, B.; Pfarr, N.; Endris, V.; Bettstetter, M.; Kong, B.; et al. Molecular, morphological and survival analysis of 177 resected pancreatic ductal adenocarcinomas (PDACs): Identification of prognostic subtypes. Sci. Rep. 2017, 7, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kaissis, G.; Ziegelmayer, S.; Lohöfer, F.; Algül, H.; Eiber, M.; Weichert, W.; Schmid, R.; Friess, H.; Rummeny, E.; Ankerst, D.; et al. A machine learning model for the prediction of survival and tumor subtype in pancreatic ductal adenocarcinoma from preoperative diffusion-weighted imaging. Eur. Radiol. Exp. 2019, 3, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, 104–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alwosheel, A.; van Cranenburgh, S.; Chorus, C.G. Is your dataset big enough? Sample size requirements when using artificial neural networks for discrete choice analysis. J. Choice Model. 2018, 28, 167–182. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 103 | % | |
|---|---|---|
| Sex | ||
| Male | 59 | 57.2 |
| Female | 44 | 42.8 |
| Age | ||
| Mean in years | 67.3 | |
| Range | 32–88 | |
| Subtype | ||
| QM | 16 | 15.5 |
| Non-QM | 87 | 84.5 |
| pT | ||
| 1 | 1 | 0.9 |
| 2 | 10 | 9.7 |
| 3 | 80 | 77.7 |
| 4 | 12 | 11.7 |
| pN | ||
| 0 | 30 | 30.1 |
| 1 | 73 | 70.9 |
| Grading | ||
| 1 | 5 | 4.9 |
| 2 | 44 | 42.8 |
| 3 | 54 | 52.3 |
| Resection status | ||
| 0 | 53 | 51.4 |
| 1 | 50 | 48.6 |
| Morphology | ||
| Conventional | 55 | 53.4 |
| Combined | 48 | 46.6 |
| Adjuvant Chemotherapy | ||
| Gemcitabine | 55 | 53.3 |
| Did not receive | 48 | 46.7 |
| Tumor Location | ||
| Head | 71 | 68.9 |
| Body | 19 | 18.4 |
| Tail | 13 | 12.7 |
| TP53 | ||
| Wild type | 21 | 20.3 |
| mutated | 82 | 79.7 |
| KRAS | ||
| wildtype | 9 | 8,8 |
| mutated | 94 | 91.2 |
| CDKN2A/p16 | ||
| intact | 19 | 81.5 |
| altered | 84 | 18.5 |
| SMAD4 | ||
| intact | 41 | 39.2 |
| altered | 62 | 60.8 |
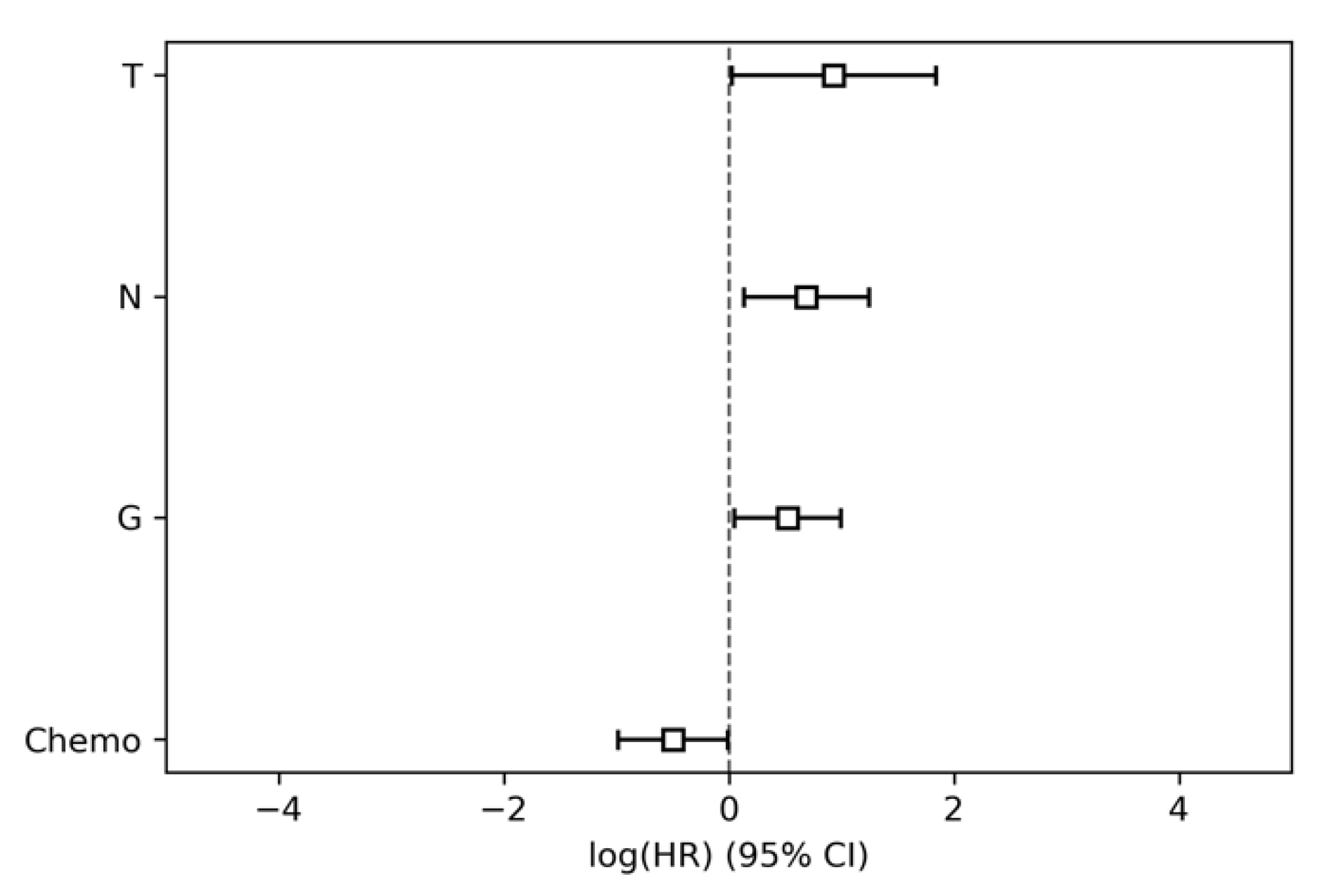
| HR | Lower 95% Conf. Int. | Upper 95% Conf. Int. | p | |
|---|---|---|---|---|
| T | 2.54 | 1.03 | 6.27 | 0.04 |
| N | 1.99 | 1.14 | 3.47 | 0.02 |
| G | 1.68 | 1.05 | 2.71 | 0.03 |
| R | 1.37 | 0.87 | 2.16 | 0.18 |
| Sex | 1.04 | 0.64 | 1.71 | 0.86 |
| Age | 1.0 | 0.98 | 1.02 | 0.85 |
| Location | 0.93 | 0.56 | 1.54 | 0.77 |
| Adjuvant Chemo | 0.61 | 0.37 | 0.99 | 0.04 |
| HR | Lower 95% Conf. Int. | Upper 95% Conf. Int. | p | |
|---|---|---|---|---|
| Subtype | 1.69 | 0.92 | 3.13 | 0.09 |
| P16 | 1.28 | 0.74 | 2.24 | 0.38 |
| Morphology | 1.21 | 0.76 | 1.92 | 0.42 |
| P53 | 1.09 | 0.7 | 1.71 | 0.7 |
| SMAD4 | 0.72 | 0.46 | 1.14 | 0.16 |
| KRAS | 0.61 | 0.28 | 1.34 | 0.22 |
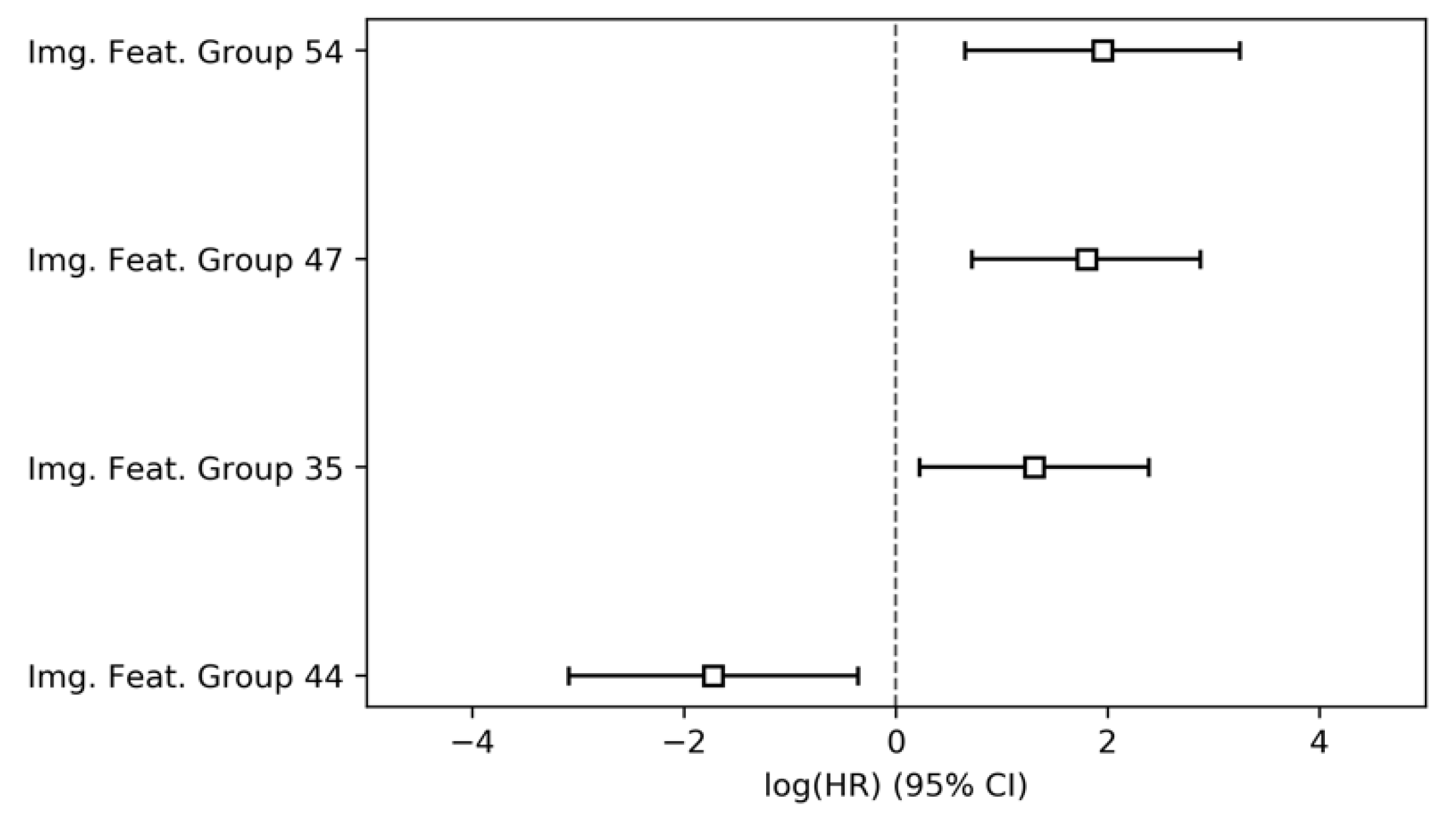
| HR | Lower 95% Conf. Int. | Upper 95% Conf Int. | p | |
|---|---|---|---|---|
| Img. Feat. Group 54 | 7.0 | 1.91 | 25.61 | <0.001 |
| Img. Feat. Group 47 | 6.03 | 2.05 | 17.72 | <0.001 |
| Img. Feat. Group 35 | 3.67 | 1.24 | 10.87 | 0.02 |
| Img. Feat. Group 56 | 3.46 | 1.01 | 11.81 | 0.05 |
| Img. Feat. Group 67 | 1.33 | 0.44 | 4.02 | 0.62 |
| Img. Feat. Group 21 | 0.58 | 0.15 | 2.17 | 0.42 |
| Img. Feat. Group 27 | 0.34 | 0.08 | 1.39 | 0.13 |
| Img. Feat. Group 44 | 0.18 | 0.05 | 0.7 | 0.01 |
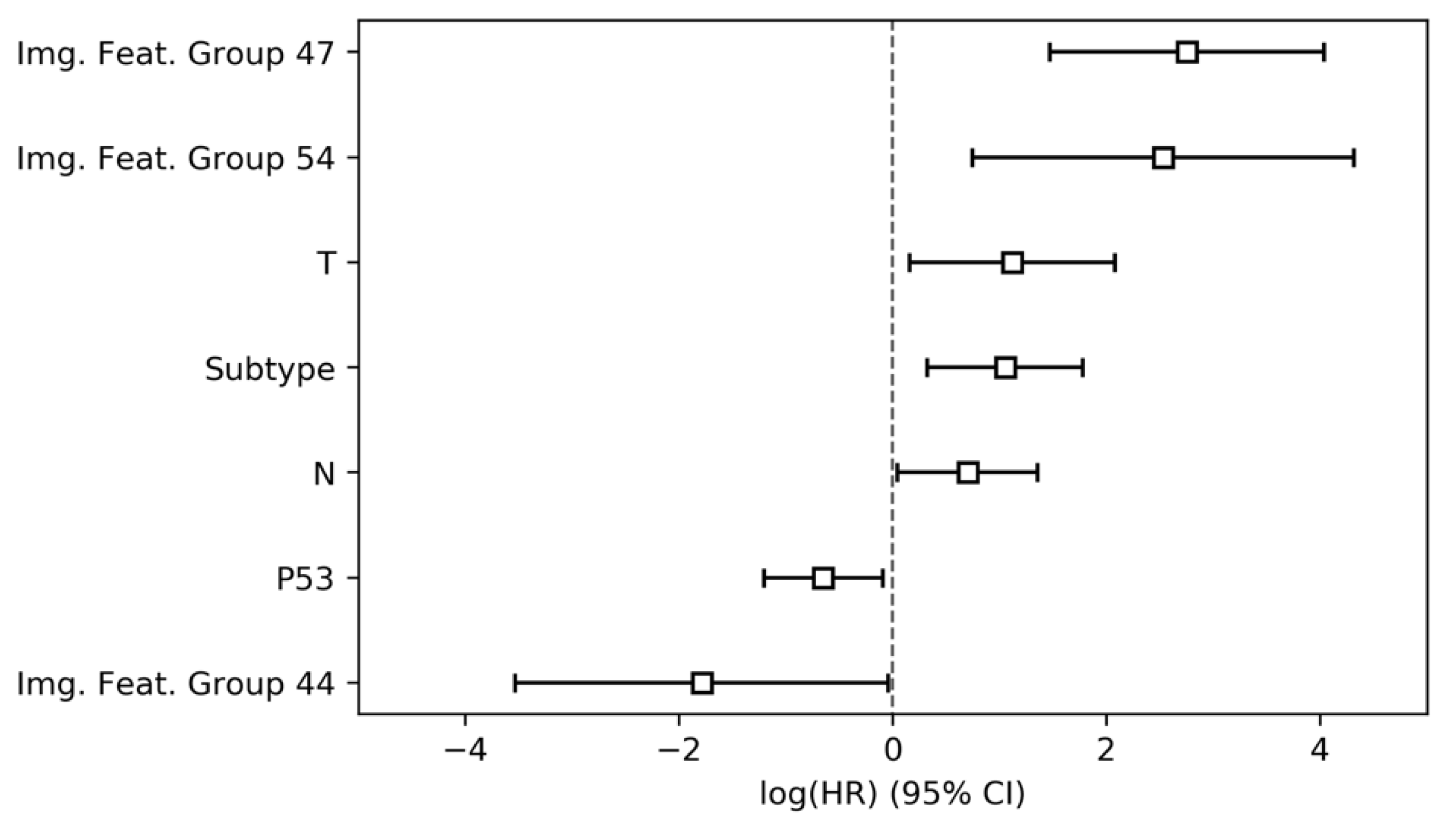
| HR | Lower 95% Conf Int. | Upper 95% Conf Int. | p | |
|---|---|---|---|---|
| Img. Feat. Group 47 | 15.68 | 4.35 | 56.45 | <0.001 |
| Img. Feat. Group 54 | 12.56 | 2.11 | 74.81 | <0.001 |
| Img. Feat. Group 35 | 3.08 | 0.86 | 11.04 | 0.08 |
| T | 3.05 | 1.17 | 7.96 | 0.02 |
| Subtype | 2.86 | 1.38 | 5.92 | <0.001 |
| N | 2.01 | 1.04 | 3.87 | 0.04 |
| Img. Feat. Group 56 | 1.66 | 0.37 | 7.42 | 0.51 |
| P16 | 1.49 | 0.82 | 2.73 | 0.19 |
| G | 1.33 | 0.79 | 2.23 | 0.28 |
| R | 1.28 | 0.71 | 2.3 | 0.41 |
| Location | 1.08 | 0.6 | 1.97 | 0.79 |
| Sex | 1.01 | 0.59 | 1.72 | 0.97 |
| Age | 1.0 | 0.97 | 1.02 | 0.82 |
| Img. Feat. Group 67 | 0.85 | 0.23 | 3.1 | 0.81 |
| SMAD4 | 0.83 | 0.48 | 1.41 | 0.48 |
| Chemo | 0.67 | 0.37 | 1.23 | 0.2 |
| KRAS | 0.67 | 0.24 | 1.88 | 0.45 |
| Img. Feat. Group 21 | 0.58 | 0.13 | 2.47 | 0.46 |
| P53 | 0.52 | 0.3 | 0.91 | 0.02 |
| Img. Feat. Group 27 | 0.35 | 0.07 | 1.69 | 0.19 |
| Img. Feat. Group 44 | 0.17 | 0.03 | 0.96 | 0.04 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaissis, G.A.; Jungmann, F.; Ziegelmayer, S.; Lohöfer, F.K.; Harder, F.N.; Schlitter, A.M.; Muckenhuber, A.; Steiger, K.; Schirren, R.; Friess, H.; et al. Multiparametric Modelling of Survival in Pancreatic Ductal Adenocarcinoma Using Clinical, Histomorphological, Genetic and Image-Derived Parameters. J. Clin. Med. 2020, 9, 1250. https://doi.org/10.3390/jcm9051250
Kaissis GA, Jungmann F, Ziegelmayer S, Lohöfer FK, Harder FN, Schlitter AM, Muckenhuber A, Steiger K, Schirren R, Friess H, et al. Multiparametric Modelling of Survival in Pancreatic Ductal Adenocarcinoma Using Clinical, Histomorphological, Genetic and Image-Derived Parameters. Journal of Clinical Medicine. 2020; 9(5):1250. https://doi.org/10.3390/jcm9051250
Chicago/Turabian StyleKaissis, Georgios A., Friederike Jungmann, Sebastian Ziegelmayer, Fabian K. Lohöfer, Felix N. Harder, Anna Melissa Schlitter, Alexander Muckenhuber, Katja Steiger, Rebekka Schirren, Helmut Friess, and et al. 2020. "Multiparametric Modelling of Survival in Pancreatic Ductal Adenocarcinoma Using Clinical, Histomorphological, Genetic and Image-Derived Parameters" Journal of Clinical Medicine 9, no. 5: 1250. https://doi.org/10.3390/jcm9051250
APA StyleKaissis, G. A., Jungmann, F., Ziegelmayer, S., Lohöfer, F. K., Harder, F. N., Schlitter, A. M., Muckenhuber, A., Steiger, K., Schirren, R., Friess, H., Schmid, R., Weichert, W., Makowski, M. R., & Braren, R. F. (2020). Multiparametric Modelling of Survival in Pancreatic Ductal Adenocarcinoma Using Clinical, Histomorphological, Genetic and Image-Derived Parameters. Journal of Clinical Medicine, 9(5), 1250. https://doi.org/10.3390/jcm9051250