Association of Salivary Human Papillomavirus Infection and Oral and Oropharyngeal Cancer: A Meta-Analysis


 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy and Study Selection
2.3. Eligibility Criteria
2.4. Protocol and Registration
2.5. Assessment of Risk Bias
2.6. Statistical Analysis
3. Results
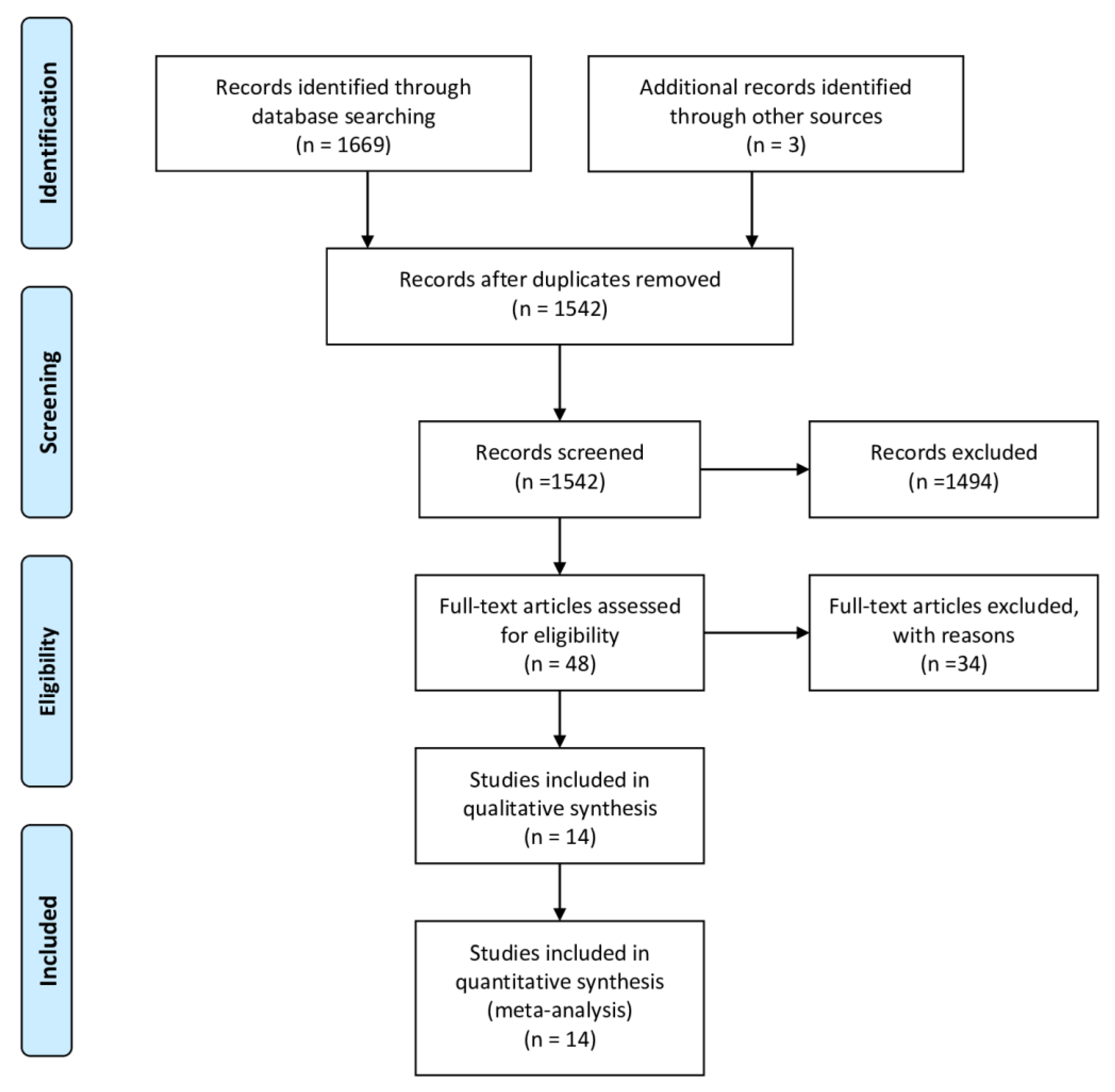
3.1. Study Selection
3.2. Study Characteristics
3.3. Study Quality
3.4. Meta-Analysis
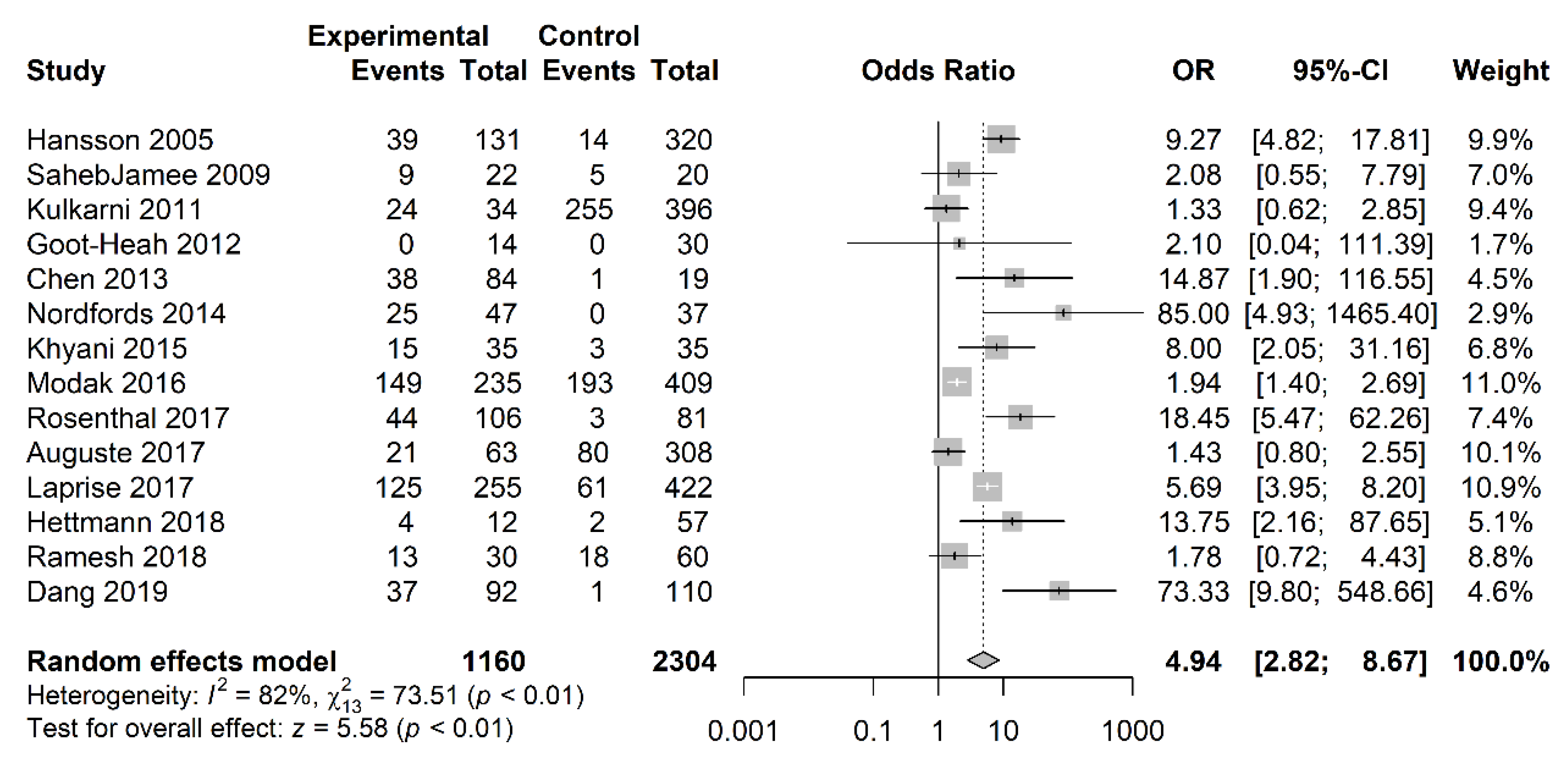
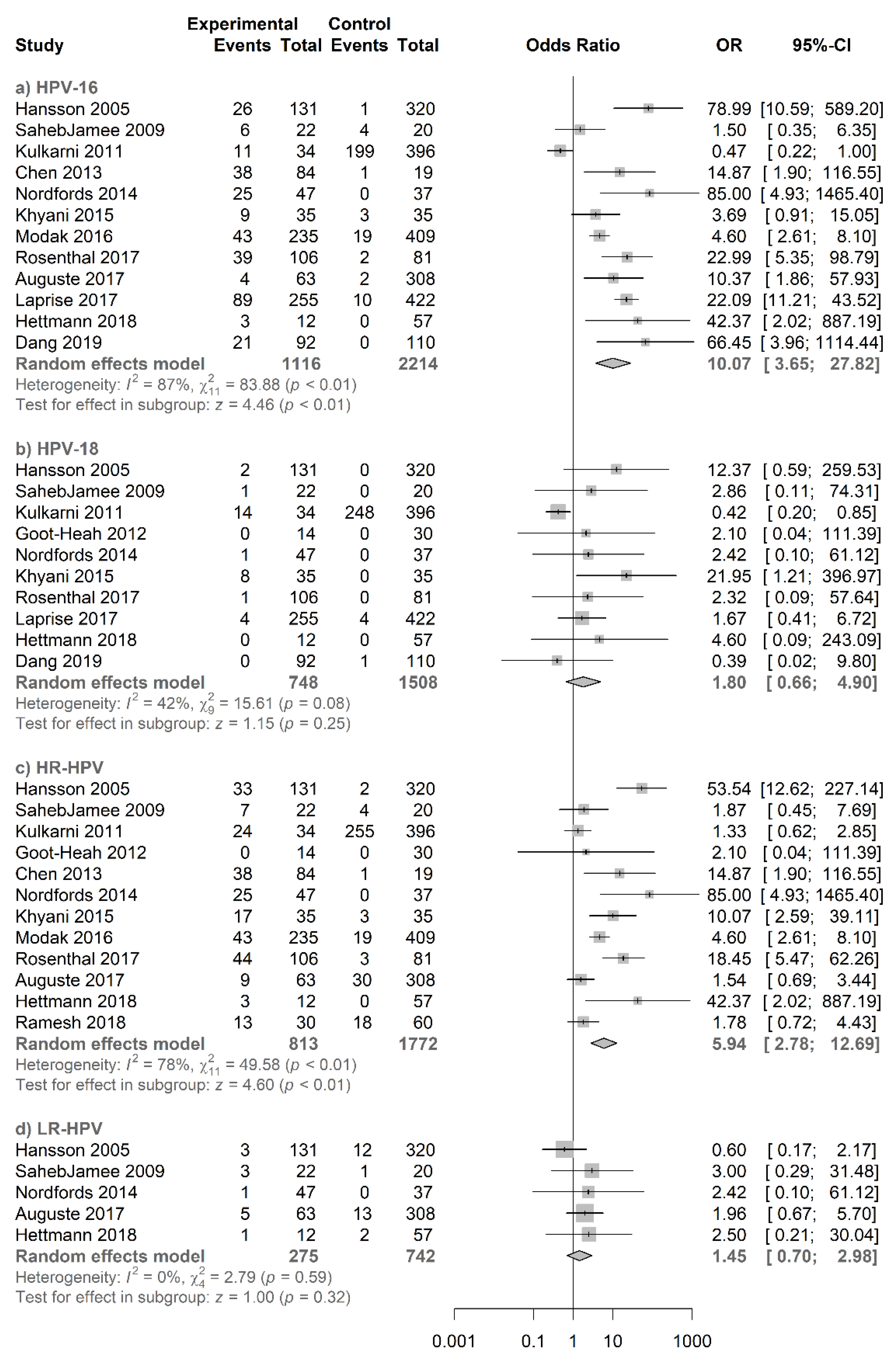
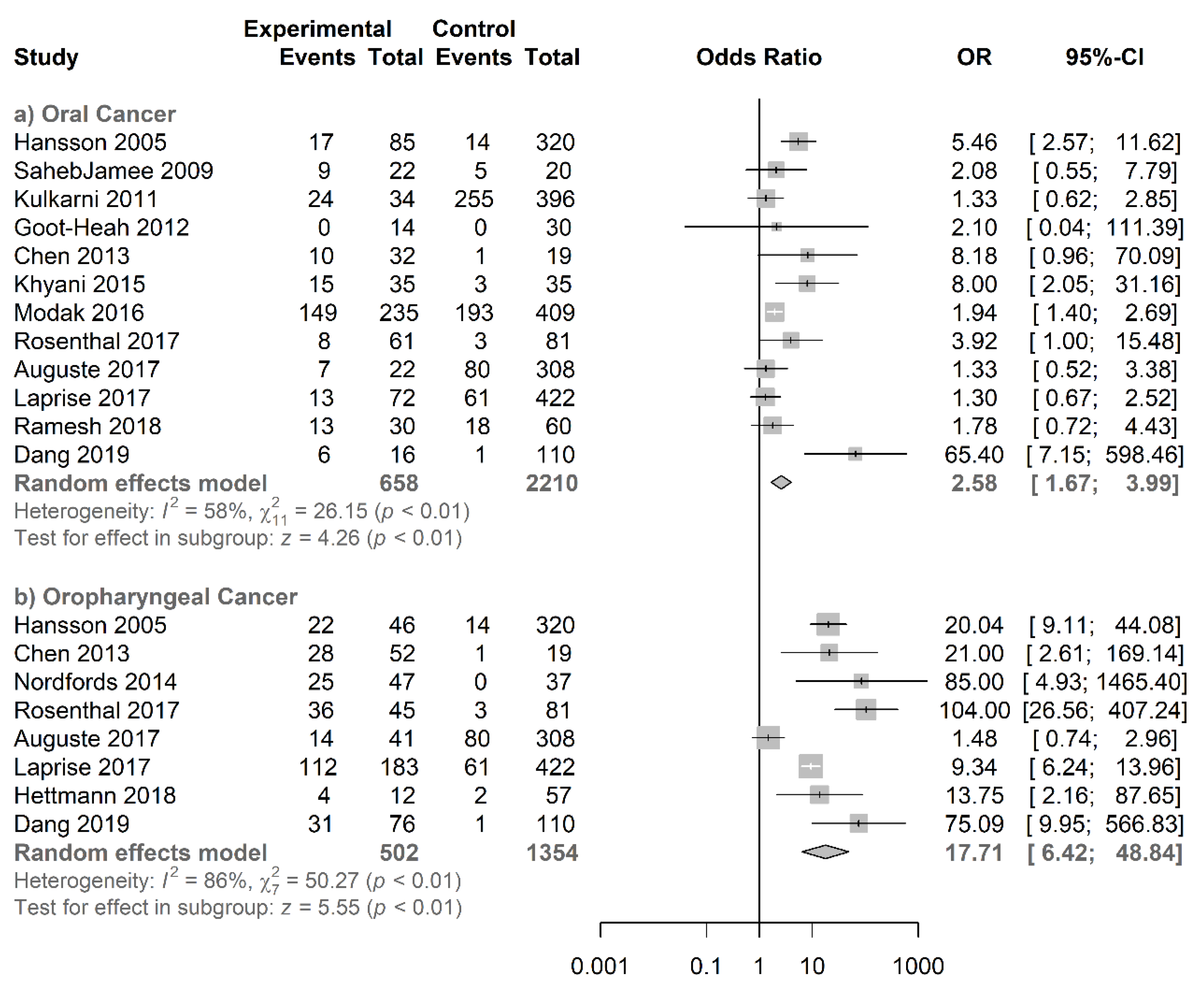
3.4.1. Salivary HPV Association with Oral and Oropharyngeal Cancer
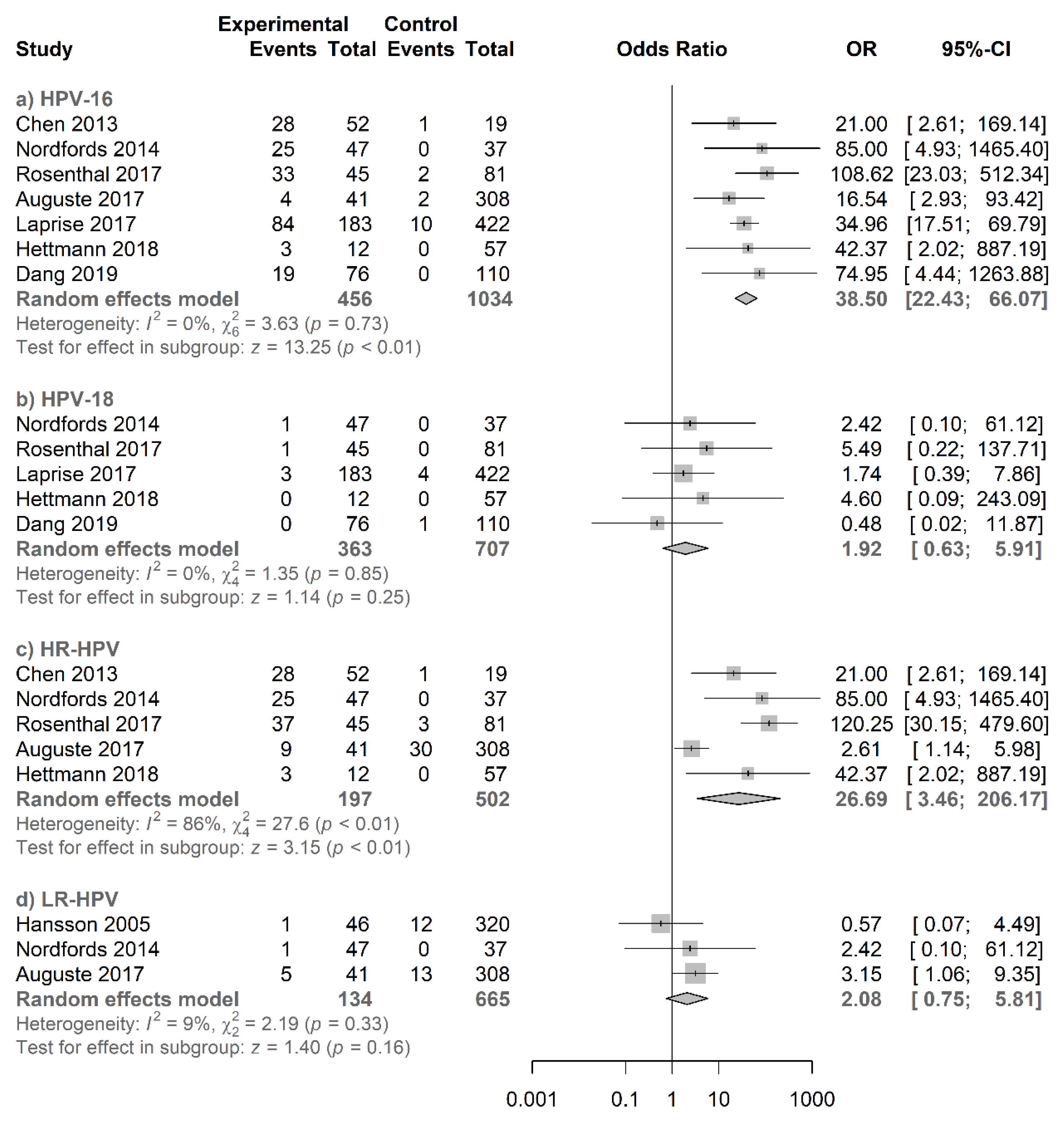
3.4.2. Type-Specific Salivary HPV Association with Oropharyngeal Cancer
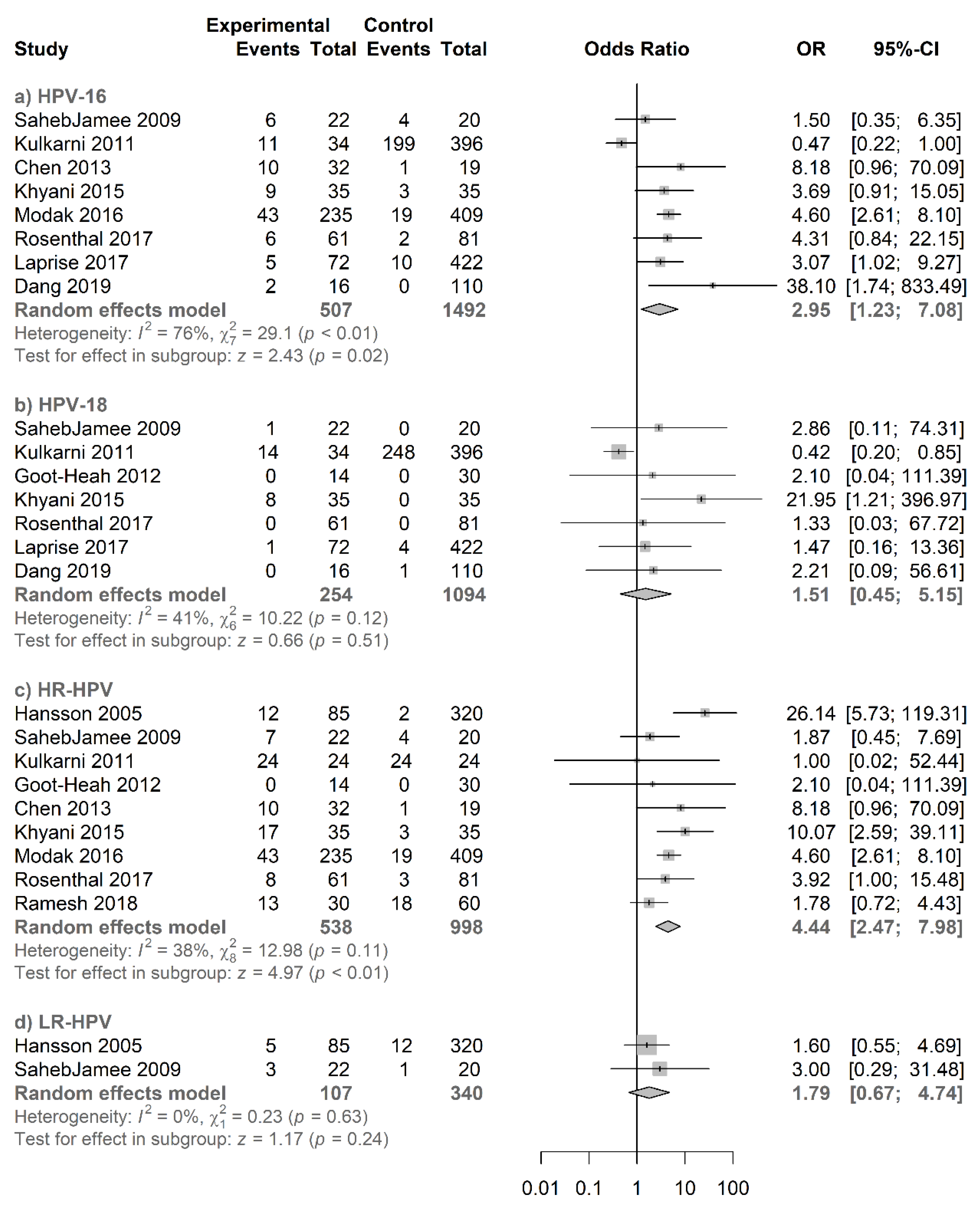
3.4.3. Type-Specific Salivary HPV Association with Oral Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Smith, E.M.; Ritchie, J.M.; Summersgill, K.F.; Hoffman, H.T.; Wang, D.H.; Haugen, T.H.; Turek, L.P. Human papillomavirus in oral exfoliated cells and risk of head and neck cancer. J. Natl. Cancer Inst. 2004, 96, 449–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Souza, G.; Kreimer, A.R.; Viscidi, R.; Pawlita, M.; Fakhry, C.; Koch, W.M.; Westra, W.H.; Gillison, M.L. Case-control study of human papillomavirus and oropharyngeal cancer. N. Engl. J. Med. 2007, 356, 1944–1956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murtaza, M.; Dawson, S.J.; Tsui, D.W.Y.; Gale, D.; Forshew, T.; Piskorz, A.M.; Parkinson, C.; Chin, S.F.; Kingsbury, Z.; Wong, A.S.C.; et al. Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature 2013, 497, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef] [Green Version]
- O’Rorke, M.A.; Ellison, M.V.; Murray, L.J.; Moran, M.; James, J.; Anderson, L.A. Human papillomavirus related head and neck cancer survival: A systematic review and meta-analysis. Oral Oncol. 2012, 48, 1191–1201. [Google Scholar] [CrossRef]
- Tommasino, M. The human papillomavirus family and its role in carcinogenesis. Semin. Cancer Biol. 2014, 26, 13–21. [Google Scholar] [CrossRef]
- Sabatini, M.E.; Chiocca, S. Human papillomavirus as a driver of head and neck cancers. Br. J. Cancer 2020, 122, 306–314. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Human papillomaviruses. IARC Monogr. Eval. Carcinog. Risks Hum. 2007, 90, 1–636. [Google Scholar]
- Schiffman, M.; Castle, P.E.; Jeronimo, J.; Rodriguez, A.C.; Wacholder, S. Human papillomavirus and cervical cancer. Lancet (Lond. Engl.) 2007, 370, 890–907. [Google Scholar] [CrossRef]
- Faber, M.T.; Sand, F.L.; Albieri, V.; Norrild, B.; Kjaer, S.K.; Verdoodt, F. Prevalence and type distribution of human papillomavirus in squamous cell carcinoma and intraepithelial neoplasia of the vulva. Int. J. Cancer 2017, 141, 1161–1169. [Google Scholar] [CrossRef] [Green Version]
- Schlenker, B.; Schneede, P. The role of human papilloma virus in penile cancer prevention and new therapeutic agents. Eur. Urol. Focus 2019, 5, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Franceschi, S.; Clifford, G.M. Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: A systematic review and meta-analysis. Lancet Infect. Dis. 2018, 18, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Tumban, E. A current update on human papillomavirus-associated head and neck cancers. Viruses 2019, 11, 922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Biological agents. Volume 100 B. A review of human carcinogens. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100 (Pt B), 1–441. [Google Scholar]
- Hübbers, C.U.; Akgül, B. HPV and cancer of the oral cavity. Virulence 2015, 6, 244–248. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, K.; Hisamatsu, K.; Suzui, N.; Hara, A.; Tomita, H.; Miyazaki, T. A review of HPV-related head and neck cancer. J. Clin. Med. 2018, 7, 241. [Google Scholar] [CrossRef] [Green Version]
- Tuna, M.; Amos, C.I. Next generation sequencing and its applications in HPV-associated cancers. Oncotarget 2017, 8, 8877–8889. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 18 February 2020).
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Kulkarni, S.S.; Kulkarni, S.S.; Vastrad, P.P.; Kulkarni, B.B.; Markande, A.R.; Kadakol, G.S.; Hiremath, S.V.; Kaliwal, S.; Patil, B.R.; Gai, P.B. Prevalence and distribution of high risk human papillomavirus (HPV) types 16 and 18 in carcinoma of cervix, saliva of patients with oral squamous cell carcinoma and in the general population in Karnataka, India. Asian Pac. J. Cancer Prev. 2011, 12, 645–648. [Google Scholar] [PubMed]
- Goot-Heah, K.; Kwai-Lin, T.; Froemming, G.R.A.; Abraham, M.T.; Nik Mohd Rosdy, N.M.M.; Zain, R.B. Human papilloma virus 18 detection in oral squamous cell carcinoma and potentially malignant lesions using saliva samples. Asian Pac. J. Cancer Prev. 2012, 13, 6109–6113. [Google Scholar] [CrossRef] [Green Version]
- Modak, H.; Sayad, T.; Fernandes, N. Molecular detection of HPV 16 in saliva of patients with oral squamous cell carcinoma and in the normal population of Southwesterly Indians. Int. J. Adv. Biol. Res. 2016, 6, 25–29. [Google Scholar]
- Ramesh, P.S.; Devegowda, D.; Naik, P.R.; Doddamani, P.; Nataraj, S.M. Evaluating the feasibility of nested PCR as a screening tool to detect HPV infection in saliva of oral squamous cell carcinoma subjects. J. Clin. Diagnostic Res. 2018, 12, BC22–BC25. [Google Scholar] [CrossRef]
- Rosenthal, M.; Huang, B.; Katabi, N.; Migliacci, J.; Bryant, R.; Kaplan, S.; Blackwell, T.; Patel, S.; Yang, L.; Pei, Z.; et al. Detection of HPV related oropharyngeal cancer in oral rinse specimens. Oncotarget 2017, 8, 109393–109401. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.M.; Stephen, J.K.; Ghanem, T.; Stachler, R.; Gardner, G.; Jones, L.; Schweitzer, V.P.; Hall, F.; Divine, G.; Worsham, M.J. Human papilloma virus prevalence in a multiethnic screening population. Otolaryngol. Neck Surg. 2013, 148, 436–442. [Google Scholar] [CrossRef] [Green Version]
- Dang, J.; Bruce, G.A.; Zhang, Q.; Kiviat, N.B. Identification and characterization of novel human papillomaviruses in oral rinse samples from oral cavity and oropharyngeal cancer patients. J. Oral Biosci. 2019, 61, 190–194. [Google Scholar] [CrossRef]
- Hansson, B.G.; Rosenquist, K.; Antonsson, A.; Wennerberg, J.; Schildt, E.-B.; Bladström, A.; Andersson, G. Strong association between infection with human papillomavirus and oral and oropharyngeal squamous cell carcinoma: A population-based case-control study in southern Sweden. Acta Otolaryngol. 2005, 125, 1337–1344. [Google Scholar] [CrossRef]
- Nordfors, C.; Vlastos, A.; Du, J.; Ahrlund-Richter, A.; Tertipis, N.; Grün, N.; Romanitan, M.; Haeggblom, L.; Roosaar, A.; Dahllöf, G.; et al. Human papillomavirus prevalence is high in oral samples of patients with tonsillar and base of tongue cancer. Oral Oncol. 2014, 50, 491–497. [Google Scholar] [CrossRef]
- Laprise, C.; Madathil, S.A.; Schlecht, N.F.; Castonguay, G.; Soulières, D.; Nguyen-Tan, P.F.; Allison, P.; Coutlée, F.; Hier, M.; Rousseau, M.C.; et al. Human papillomavirus genotypes and risk of head and neck cancers: Results from the HeNCe Life case-control study. Oral Oncol. 2017, 69, 56–61. [Google Scholar] [CrossRef]
- Auguste, A.; Gaëte, S.; Herrmann-Storck, C.; Michineau, L.; Joachim, C.; Deloumeaux, J.; Duflo, S.; Luce, D. Prevalence of oral HPV infection among healthy individuals and head and neck cancer cases in the French West Indies. Cancer Causes Control. 2017, 28, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Hettmann, A.; Demcsák, A.; Bach, Á.; Decsi, G.; Dencs, Á.; Pálinkó, D.; Rovó, L.; Terhes, G.; Urbán, E.; Buzás, K.; et al. Prevalence and genotypes of human papillomavirus in saliva and tumor samples of head and neck cancer patients in Hungary. Infect. Genet. Evol. 2018, 59, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Khyani, I.A.M.; Qureshi, M.A.; Mirza, T.; Farooq, M.U. Salivary detection of human papilloma virus 16 & 18 in pre-malignant and malignant lesions of oral cavity: Is it feasible in Pakistani context of socio-cultural taboos? Pak. J. Med. Sci. 2015, 31, 1104–1109. [Google Scholar] [PubMed]
- SahebJamee, M.; Boorghani, M.; Ghaffari, S.R.; AtarbashiMoghadam, F.; Keyhani, A. Human papillomavirus in saliva of patients with oral squamous cell carcinoma. Med. Oral Patol. Oral Cir. Bucal 2009, 14, e525–e528. [Google Scholar] [CrossRef] [Green Version]
- Chaitanya, N.C.; Allam, N.S.; Gandhi Babu, D.B.; Waghray, S.; Badam, R.K.; Lavanya, R. Systematic meta-analysis on association of human papilloma virus and oral cancer. J. Cancer Res. Ther. 2016, 12, 969–974. [Google Scholar] [CrossRef]
- Ndiaye, C.; Mena, M.; Alemany, L.; Arbyn, M.; Castellsagué, X.; Laporte, L.; Bosch, F.X.; de Sanjosé, S.; Trottier, H. HPV DNA, E6/E7 mRNA, and p16INK4a detection in head and neck cancers: A systematic review and meta-analysis. Lancet Oncol. 2014, 15, 1319–1331. [Google Scholar] [CrossRef]
- Haeggblom, L.; Ramqvist, T.; Tommasino, M.; Dalianis, T.; Näsman, A. Time to change perspectives on HPV in oropharyngeal cancer. A systematic review of HPV prevalence per oropharyngeal sub-site the last 3 years. Papillomavirus Res. (Amst. Neth.) 2017, 4, 1–11. [Google Scholar] [CrossRef]
- Guo, L.; Yang, F.; Yin, Y.; Liu, S.; Li, P.; Zhang, X.; Chen, D.; Liu, Y.; Wang, J.; Wang, K.; et al. Prevalence of human papillomavirus type-16 in head and neck cancer among the Chinese Population: A Meta-Analysis. Front. Oncol. 2018, 8, 619. [Google Scholar] [CrossRef] [Green Version]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: A systematic review. Cancer Epidemiol. Biomark. Prev. 2005, 14, 467–475. [Google Scholar] [CrossRef] [Green Version]
- Smitha, T.; Mohan, C.V.; Hemavathy, S. Prevalence of human papillomavirus16 DNA and p16INK4a protein in oral squamous cell carcinoma: A systematic review and meta-analysis. J. Oral Maxillofac. Pathol. 2017, 21, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Termine, N.; Panzarella, V.; Falaschini, S.; Russo, A.; Matranga, D.; Lo Muzio, L.; Campisi, G. HPV in oral squamous cell carcinoma vs head and neck squamous cell carcinoma biopsies: A meta-analysis (1988–2007). Ann. Oncol. 2008, 19, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Ling, Y.; Dong, C.; Zhou, X.; Wang, F. The relationship between oral squamous cell carcinoma and human papillomavirus: A meta-analysis of a Chinese population (1994–2011). PLoS ONE 2012, 7, e36294. [Google Scholar] [CrossRef] [Green Version]
- Clifford, G.; Franceschi, S. Members of the human papillomavirus type 18 family (alpha-7 species) share a common association with adenocarcinoma of the cervix. Int. J. Cancer 2008, 122, 1684–1685. [Google Scholar] [CrossRef] [PubMed]
- Grabowska, A.K.; Riemer, A.B. The invisible enemy—How human papillomaviruses avoid recognition and clearance by the host immune system. Open Virol. J. 2012, 6, 249–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, M.H.; McMillan, N.A.J.; Johnson, N.W. HPV-associated head and neck cancers in the Asia Pacific: A critical literature review & meta-analysis. Cancer Epidemiol. 2015, 39, 923–938. [Google Scholar] [PubMed] [Green Version]
- Hobbs, C.G.L.; Sterne, J.A.C.; Bailey, M.; Heyderman, R.S.; Birchall, M.A.; Thomas, S.J. Human papillomavirus and head and neck cancer: A systematic review and meta-analysis. Clin. Otolaryngol. 2006, 31, 259–266. [Google Scholar] [CrossRef]
- Saulle, R.; Semyonov, L.; Mannocci, A.; Careri, A.; Saburri, F.; Ottolenghi, L.; Guerra, F.; La Torre, G. Human papillomavirus and cancerous diseases of the head and neck: A systematic review and meta-analysis. Oral Dis. 2015, 21, 417–431. [Google Scholar] [CrossRef]
- Smith, E.M.; Hoffman, H.T.; Summersgill, K.S.; Kirchner, H.L.; Turek, L.P.; Haugen, T.H. Human papillomavirus and risk of oral cancer. Laryngoscope 1998, 108, 1098–1103. [Google Scholar] [CrossRef]
- Zhao, M.; Rosenbaum, E.; Carvalho, A.L.; Koch, W.; Jiang, W.; Sidransky, D.; Califano, J. Feasibility of quantitative PCR-based saliva rinse screening of HPV for head and neck cancer. Int. J. Cancer 2005, 117, 605–610. [Google Scholar] [CrossRef]
- Chai, R.C.; Lim, Y.; Frazer, I.H.; Wan, Y.; Perry, C.; Jones, L.; Lambie, D.; Punyadeera, C. A pilot study to compare the detection of HPV-16 biomarkers in salivary oral rinses with tumour p16(INK4a) expression in head and neck squamous cell carcinoma patients. BMC Cancer 2016, 16, 178. [Google Scholar] [CrossRef] [Green Version]
- Martin-Gomez, L.; Fulp, W.J.; Schell, M.J.; Sirak, B.; Abrahamsen, M.; Isaacs-Soriano, K.A.; Lorincz, A.; Wenig, B.; Chung, C.H.; Caudell, J.J.; et al. Oral gargle-tumor biopsy human papillomavirus (HPV) agreement and associated factors among oropharyngeal squamous cell carcinoma (OPSCC) cases. Oral Oncol. 2019, 92, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.D.; Baeten, K.; Kenny, L.; Frazer, I.H.; Scheper, G.; Punyadeera, C. Unlocking the potential of saliva-based test to detect HPV-16-driven oropharyngeal cancer. Cancers 2019, 11, 473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, K.D.; Menezes, L.; Baeten, K.; Walsh, L.J.; Whitfield, B.C.S.; Batstone, M.D.; Kenny, L.; Frazer, I.H.; Scheper, G.C.; Punyadeera, C. Oral HPV16 prevalence in oral potentially malignant disorders and oral cavity cancers. Biomolecules 2020, 10, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Tumor Location (n) | Type of Sample/Method of Collection | HPV-Positive Cases (n/N) | HPV-Positive Case Types | HPV-Positive Controls (n/N) | HPV-Positive Control Types | HPV Detection Method | |
|---|---|---|---|---|---|---|---|---|
| Hansson et al.; 2005 | Sweden | OC (85) OPC (46) | Oral rinse/7 mL of 0.9% NaCl solution for 30s | 39/131 | 16, 18, 33, 45, 58, 59, 13, 32, 62, 10, 76 | 14/320 | 16, 67, 54, 55, 62, 87, 75, 76, RTRX9 | Nested PCR (MY09/ MY11 and GP5+/6+ primers) DNA sequencing |
| SahebJamee et al.; 2009 | Iran | OC (22) | Oral rinse/10 mL of normal saline | 9/22 | 16, 18, 6/11 | 5/20 | 16, 6/11 | PCR (GP5+/ 6+ primers for L1 region) |
| Kulkarni et al.; 2011 | India | OC (34) | Saliva | 24/34 | 16, 18 | 255/396 | 16, 18 | PCR (16 and 18 specific primers) |
| Goot-Heah et al.; 2012 | India | OC (14) | Saliva | 0/14 | - | 0/30 | - | Nested PCR (MY09/11 and GP5+/6+ primers for L1 region) |
| Chen et al.; 2013 | USA | OC (32) OPC (52) | Saliva/Oragene DNA kits (DNA Genotek) | 38/84 | 16 | 1/19 | 16 | qPCR (specific primers and probe for E6 region of HPV16) |
| Nordfors et al.; 2014 | Sweden | OPC (47) | Oral rinse/15 mL 50% Listerine® (Johnson and Johnson) for 30s | 25/47 | 16, 18, 67, 6, 51 | 0/37 | - | Bead-based multiplex assay on a MagPix instrument (Luminex Corporation), GP5+/6+ primers for the L1 region and specific primers and probe for E6 region of HPV16 |
| Khyani et al.; 2015 | Pakistan | OC (35) | Saliva | 15/35 | 16, 18 | 3/35 | 16 | qPCR using Real-time PCR Kit HPV16/18 Real-TM Quant (Sacace Biotechnologies) |
| Modak et al.; 2016 | India | OC (235) | Saliva | 149/235 | 16 | 193/409 | 16 | PCR (HPV 16 specific primer) |
| Rosenthal et al.; 2017 | USA | OC (61) OPC (45) | Oral rinse/10 mL of 0.9% NaCl solution for 30s | 44/106 | 16, 18, * HR-HPV other | 3/81 | 16, * HR-HPV other | qPCR from the HPV L1 region (Cobas® HPV Test-Roche Diagnostics) |
| Auguste et al.; 2017 | France | OC (22) OPC (41) | Saliva/Oragene OG-500 kit (DNA Genotek) | 21/63 | 16, 33, 51 | 80/308 | 16 | PCR (SPF10 primer system for L1 region, INNO-LiPA® HPV Genotyping Extra; Innogenetics) |
| Laprise et al.; 2017 | Canada | OC (72) OPC (183) | Oral rinse/alcohol-based solution for 15–30s | 125/255 | 16, 18, ** HPV α-9 other than HPV16, *** HPV other | 61/422 | 16, 18, ** HPV α-9 other than HPV16, *** HPV other | PCR (MY09/11 primers for HPV) and genotyping by Linear Array assay (Roche Molecular diagnostics) |
| Hettman et al.; 2018 | Hungary | OPC (12) | Unstimulated saliva | 4/12 | 16, 13 | 2/57 | 13, 11 | PCR (MY09/11 primers for L1 region) Nested PCR (MY09/11 and GP5+/6+ primers for L1 region), sequencing for genotyping |
| Ramesh et al.; 2018 | India | OC (30) | Oral rinse/10mL of 0.9% normal saline | 13/30 | 16, 18 | 18/60 | 16, 18 | Nested PCR (MY09/ 11 primers for L1 region) |
| Dang et al.; 2019 | USA | OC (16) OPC (76) | Oral rinse/Original Mint Scope® mouthwash or Crest® Alcohol-free mouthwash (Proctor and Gamble) for 30s | 37/92 | 16, NV14.4, NV69.1, NV95 | 1/110 | 18 | qPCR (HPV16 E7/HPV18 E7 primers and probe) FAP-PCR from the L1 region NGS and Sanger sequencing |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rapado-González, Ó.; Martínez-Reglero, C.; Salgado-Barreira, Á.; Rodríguez-Fernández, A.; Aguín-Losada, S.; León-Mateos, L.; Muinelo-Romay, L.; López-López, R.; Suarez-Cunqueiro, M.M. Association of Salivary Human Papillomavirus Infection and Oral and Oropharyngeal Cancer: A Meta-Analysis. J. Clin. Med. 2020, 9, 1305. https://doi.org/10.3390/jcm9051305
Rapado-González Ó, Martínez-Reglero C, Salgado-Barreira Á, Rodríguez-Fernández A, Aguín-Losada S, León-Mateos L, Muinelo-Romay L, López-López R, Suarez-Cunqueiro MM. Association of Salivary Human Papillomavirus Infection and Oral and Oropharyngeal Cancer: A Meta-Analysis. Journal of Clinical Medicine. 2020; 9(5):1305. https://doi.org/10.3390/jcm9051305
Chicago/Turabian StyleRapado-González, Óscar, Cristina Martínez-Reglero, Ángel Salgado-Barreira, Almudena Rodríguez-Fernández, Santiago Aguín-Losada, Luis León-Mateos, Laura Muinelo-Romay, Rafael López-López, and María Mercedes Suarez-Cunqueiro. 2020. "Association of Salivary Human Papillomavirus Infection and Oral and Oropharyngeal Cancer: A Meta-Analysis" Journal of Clinical Medicine 9, no. 5: 1305. https://doi.org/10.3390/jcm9051305
APA StyleRapado-González, Ó., Martínez-Reglero, C., Salgado-Barreira, Á., Rodríguez-Fernández, A., Aguín-Losada, S., León-Mateos, L., Muinelo-Romay, L., López-López, R., & Suarez-Cunqueiro, M. M. (2020). Association of Salivary Human Papillomavirus Infection and Oral and Oropharyngeal Cancer: A Meta-Analysis. Journal of Clinical Medicine, 9(5), 1305. https://doi.org/10.3390/jcm9051305