Personal Autonomy as Quality of Life Predictor for Multiple Sclerosis Patients

 ,
, 
 ,
,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Ethical Issues
2.2. Participants
2.3. Materials and Measures
2.3.1. 15D-Instrument
2.3.2. Personal Autonomy Questionnaire (PAQ)
2.4. Statistical Analysis
3. Results
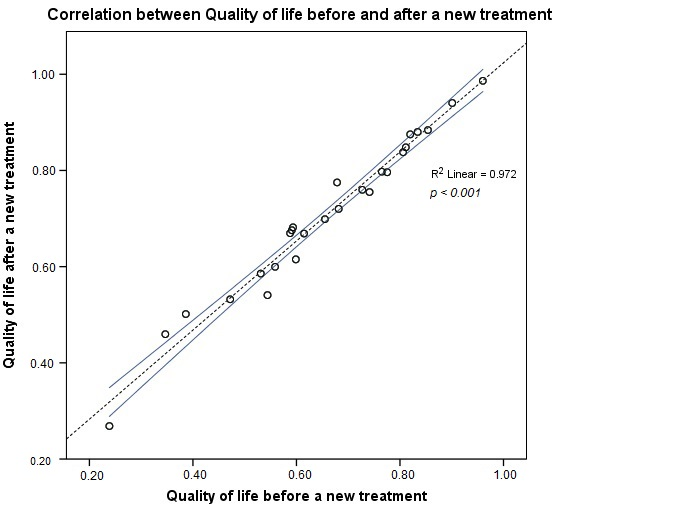
Changes in 15D Scores before and after a New Treatment
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- De Pasquale, C.; Pistorio, M.L.; Veroux, M.; Giaquinta, A.; Veroux, P.; Fornaro, M. Cognitive functioning and subjective quality of life in relapsing-remitting multiple sclerosis patients before and after percutaneous transluminal angioplasty: A preliminary report. Neuropsychiatr. Dis. Treat. 2014, 10, 1039–1044. [Google Scholar] [PubMed] [Green Version]
- Zimmermann, A.F.; Pizzichini, M.M. Update on etiopathogenesis of systemic sclerosis. Rev. Bras. Reumatol. 2013, 53, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCoyd, M. Update on therapeutic options for multiple sclerosis. Neurol. Clin. 2013, 31, 827–845. [Google Scholar] [CrossRef] [PubMed]
- Padureanu, R.; Albu, C.V.; Mititelu, R.R.; Bacanoiu, M.V.; Docea, A.O.; Calina, D.; Padureanu, V.; Olaru, G.; Sandu, R.E.; Malin, R.D.; et al. Oxidative Stress and Inflammation Interdependence in Multiple Sclerosis. J. Clin. Med. 2019, 8, 1815. [Google Scholar] [CrossRef] [Green Version]
- Santos, M.; Sousa, C.; Pereira, M.; Pereira, M.G. Quality of life in patients with multiple sclerosis: A study with patients and caregivers. Disabil. Health J. 2019, 12, 628–634. [Google Scholar] [CrossRef]
- Khan, F.; Turner-Stokes, L.; Ng, L.; Kilpatrick, T. Multidisciplinary rehabilitation for adults with multiple sclerosis. Postgrad. Med. 2008, 84, 385. [Google Scholar] [CrossRef]
- Adamopoulou, F.; Alikari, V.; Zyga, S.; Tsironi, M.; Tzavella, F.; Giannakopoulou, N.; Theofilou, P. The Effect of Fatigue and Pain Self- Efficacy on Health-Related Quality of Life Among Patients with Multiple Sclerosis. Mater. Sociomed. 2019, 31, 40–44. [Google Scholar] [CrossRef]
- Gelfand, J.M. Multiple sclerosis: Diagnosis, differential diagnosis, and clinical presentation. Handb. Clin. Neurol. 2014, 122, 269–290. [Google Scholar]
- Friedman, J.H.; Beck, J.C.; Chou, K.L.; Clark, G.; Fagundes, C.P.; Goetz, C.G.; Herlofson, K.; Kluger, B.; Krupp, L.B.; Lang, A.E.; et al. FatigueinParkinson’sdisease: Report from a multidisciplinary symposium. NPJ Parkinson’s Dis. 2016, 2, 15025. [Google Scholar] [CrossRef] [Green Version]
- Patejdl, R.; Penner, I.K.; Noack, T.K.; Zettl, U.K. Fatigue in patients with multiple sclerosis—Pathogenesis, clinical picture, diagnosis and treatment. Fortschr. Neurol. Psychiatr. 2015, 83, 211–220. [Google Scholar]
- Albu, C.V.; Padureanu, V.; Boldeanu, M.V.; Bumbea, A.M.; Enescu, A.S.; Albulescu, D.M.; Silosi, C.A.; Enescu, A. Vascular neurocognitive disorders and the vascular risk factors. J. Mind. Med. Sci. 2018, 5, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Mungo, S.; Fornaro, M. Adherence to Chronic Therapies in Psychiatry: From Treatment to Cure. The Relevance of Therapeutic Relationship. J. Psychol. Psychother. 2013, 3, S3. [Google Scholar] [CrossRef] [Green Version]
- Lee Mortensen, G.; Rasmussen, P.V. The impact of quality of life on treatment preferences in multiple sclerosis patients. Patient. Prefer. Adherence 2017, 11, 1789–1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, F.; Amatya, B.; Galea, M. Management of fatigue in persons with multiple sclerosis. Front. Neurol. 2014, 5, 177. [Google Scholar] [CrossRef] [Green Version]
- Berrigan, L.I.; Fisk, J.D.; Patten, S.B.; Tremlett, H.; Wolfson, C.; Warren, S.; Fiest, K.M.; McKay, K.A.; Marrie, R.A.; CIHR Team in the Epidemiology and Impact of Comorbidity on Multiple Sclerosis (ECoMS). For the CIHR team in the epidemiology and impact of comorbidity on multiple sclerosis (ECoMS). Health-related quality of life in multiple sclerosis: Direct and indirect effects of comorbidity. Neurology 2016, 86, 1417–1424. [Google Scholar] [CrossRef] [Green Version]
- Tacchino, A.; Brichetto, G.; Zaratin, P.; Battaglia, M.A.; Ponzio, M. Self-assessment reliability in multiple sclerosis: The role of socio-demographic, clinical, and quality of life aspects. Neurol. Sci. 2019, 40, 617–620. [Google Scholar] [CrossRef]
- Feinstein, A.; Magalhaes, S.; Richard, J.F.; Audet, B.; Moore, C. The link between multiple sclerosis and depression. Nat. Rev. Neurol. 2014, 10, 507–517. [Google Scholar] [CrossRef]
- Dahl, O.P.; Stordal, E.; Lydersen, S.; Midgard, R. Anxiety and depression in multiple sclerosis. A comparative population-based study in Nord-Trøndelag County, Norway. Mult. Scler. J. 2009, 15, 1495–1501. [Google Scholar] [CrossRef]
- Shabani, A.; Moghadam, J.A.; Panaghi, L.; Seddigh, A. Anxiety disorders in multiple sclerosis: Significance of obsessive-compulsive disorder comorbidity. J. Res. Med. Sci. 2007, 12, 172–177. [Google Scholar]
- Da Silva, A.; Vilhena, E.; Lopes, A.; Santos, E.; Gonçalves, M.; Pinto, C.; Moreira, I.; Mendonca, D.; Cavaco, S. Depression and anxiety in a Portuguese MS population: Associations with physical disability and severity of disease. J. Neurol. Sci. 2011, 306, 66–70. [Google Scholar] [CrossRef]
- Tan-Kristanto, S.; Kiropoulos, L.A. Resilience, self-efficacy, coping styles and depressive and anxiety symptoms in those newly diagnosed with multiple sclerosis. Psychol. Health Med. 2015, 20, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Heesen, C.; Kopke, S.; Solari, A.; Geiger, F.; Kasper, J. Patient autonomy in multiple sclerosis—Possible goals ans assessment strategies. J. Neurol. Sci. 2013, 331, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, C.; Wasson, D.; Brighton, V.; Dixon, L.; Anderson, M.A. Personal Autonomy: Development of a NOC Label. Int. Nurs. Terminol. CL 2008, 14, S4. [Google Scholar] [CrossRef]
- Degner, L.F.; Sloan, J.A.; Venkatesh, P. The Control Preferences Scale. Can. J. Nurs. Res. 1997, 29, 21–43. [Google Scholar] [PubMed]
- Giordano, A.; Mattarozzi, K.; Pucci, E.; Leone, M.; Casini, F.; Collimedaglia, L.; Solari, A. Participation in medical decision-making: Attitudes of Italians with multiple sclerosis. J. Neurol. Sci. 2008, 275, 86–91. [Google Scholar] [CrossRef]
- Steinberg, L. Autonomy, Conflict, and Harmony in the Family Relationship. In At the Threshold: The Developing Adolescent; Feldman, S.S., Elliott, G.R., Eds.; Harvard University Press: Cambridge, MA, USA, 1996; pp. 255–276. [Google Scholar]
- Russell, S.T.; Bakken, R. Development of Autonomy in Adolescence. Lincoln, Neb.: Cooperative Extension, Institute of Agriculture and Natural Resources; University of Nebraska-Lincoln: Lincoln, NE, USA, 2002. [Google Scholar]
- Beyers, W.; Goossens, L.; Vansant, I.; Moors, E. A structural model of autonomy in middle and late adolescence: Connectedness, separation, detachment, and agency. J. Youth Adolesc. 2003, 32, 351–365. [Google Scholar] [CrossRef]
- Killaspy, H.; Priebe, S.; Bremner, S.; McCrone, P.; Dowling, S.; Harrison, I.; Krotofil, J.; McPherson, P.; Sandhu, S.; Arbuthnott, M.; et al. Quality of life, autonomy, satisfaction, and costs associated with mental health supported accommodation services in England: A national survey. Lancet Psychiat 2016, 3, 1129–1137. [Google Scholar] [CrossRef] [Green Version]
- Vartiainen, P.; Mäntyselkä, P.; Heiskanen, T.; Hagelberg, N.; Mustola, S.; Forssell, H.; Kautiainen, H.; Kalso, E. Validation of EQ-5D and 15D in the assessment of health-related quality of life in chronic pain. PAIN 2017, 158, 1577–1585. [Google Scholar] [CrossRef]
- Sintonen, H. The 15D instrument of health-related quality of life: Properties and applications. Ann. Med. 2001, 33, 328–336. [Google Scholar] [CrossRef]
- Subtirelu, M.S.; Turcu-Stiolica, A.; Sintonen, H. Translation and cultural adaptation of 15D quality of life questionnaire from English to Romanian language. Value Health 2019, 22, S731. [Google Scholar] [CrossRef]
- Albu, M. Un nou Instrument Pentru Evaluarea Autonomiei Personale la Adolescenţi/A New Instrument for Personal Autonomy Evaluation in Adolescents; Anuarul Institutului de Istorie George Barit; Seria Humanistica: Cluj-Napoca, Romania, 2007; pp. 99–114. [Google Scholar]
- Gross, H.; Watson, C. Characteristics, burden of illness, and physical functioning of patients with relapsing-remitting and secondary progressive multiple sclerosis: A cross-sectional US survey. Neuropsych. Dis. Treat. 2017, 13, 1349–1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magyari, M. Gender differences in multiple sclerosis epidemiology and treatment response. Dan. Med. J. 2016, 63, B5212. [Google Scholar] [PubMed]
- Petersen, M.; Kristensen, E.; Giraldi, L.; Giraldi, A. Sexual dysfunction and mental health in patients with multiple sclerosis and epilepsy. BMC Neurol. 2020, 20, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somerset, M.; Peters, T.J.; Sharp, D.J.; Campbell, R. Factors that contribute to quality of life outcomes prioritized by people with multiple sclerosis. Qual. Life Res. 2003, 12, 21–29. [Google Scholar] [CrossRef]
- Alanne, S.; Roine, R.P.; Räsänen, P.; Vainiola, T.; Sintonen, H. Estimating the minimum important change in the 15D scores. Qual. Life Res. 2015, 24, 599–606. [Google Scholar] [CrossRef]
- Alonso-Sardon, M.; Iglesis-de-Sena, H.; Fernandez-Martin, L.C.; Miron-Canelo, J.A. Do health and social support and personal autonomy have an influence on the health-related quality of life of individuals with intellectual disability? BMC Health Serv. Res. 2019, 19, 63. [Google Scholar] [CrossRef]
- Lyam, I.; Catley, D.; Goggin, K.; Rabinowitz, J.; Gerkovich, M.; Williams, K.; Wright, J. Autonomous regulation and locus of control as predictors of antiretroviral medication adherence. J. Health Psychol. 2009, 14, 578–586. [Google Scholar] [CrossRef] [Green Version]
- Turcu-Stiolica, A.; Taerel, A.E.; Turcu-Stiolica, R. Identifying and Measuring Compliance and Adherence in Antidepressants Taking. In Emerging Markets Queries in Finance and Business (EMQ 2013); Book Series: Procedia Economics and Finance; Elsevier Science BV: Amsterdam, The Netherlands, 2014; Volume 15, pp. 836–839. [Google Scholar]
- Kahle-Wrobleski, K.; Ye, W.; Henley, D.; Hake, A.M.; Siemers, E.; Chen, Y.F.; Liu-Seifert, H. Assessing quality of life in Alzheimer’s disease: Implications for clinical trials. Alzheimer’s Dement. (Amst. Neth.) 2016, 6, 82–90. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Patient Group | p-Value | |||
|---|---|---|---|---|---|
| Relapsing–Remitting MS (N = 15) | Secondary Progressive MS (N = 11) | ||||
| Count | Mean (±SD) | Count | Mean (±SD) | ||
| Age, years (43 ± 10) | 39.7 (±5.97) | 47.5 (±12.7) | 0.032 | ||
| Gender | 0.743 | ||||
| Men (n = 3) | 2 (8%) | 1 (4%) | |||
| Women (n = 23) | 13 (50%) | 10 (38%) | |||
| Marital status | 0.442 | ||||
| Married (n = 18) | 11 (42%) | 7 (27%) | |||
| Unmarried (n = 6) | 4 (4%) | 2 (8%) | |||
| Divorced (n = 1) | 0 | 1 (4%) | |||
| Widow (n = 1) | 0 | 1 (4%) | |||
| Employment status | 0.014 | ||||
| Working (n = 3) | 3 (12%) | 0 | |||
| Not working (n = 17) | 11 (42%) | 6 (23%) | |||
| Unemployed (n = 2) | 0 | 2 (8%) | |||
| Pensioner (n = 4) | 1 (4%) | 3 (12%) | |||
| Environment status | 0.509 | ||||
| Urban (n = 17) | 9 (35%) | 8 (31%) | |||
| Rural (n = 9) | 6 (23%) | 3 (12%) | |||
| Level of education | 0.997 | ||||
| Middle school (n = 8) | 4 (4%) | 4 (4%) | |||
| High school (n = 15) | 10 (38%) | 5 (19%) | |||
| Faculty (n = 3) | 1 (4%) | 2 (8%) | |||
| Variables | Patient Group | p-Value | |||
|---|---|---|---|---|---|
| Relapsing–Remitting MS (N = 15) | Secondary Progressive MS (N = 11) | ||||
| Count | Mean (±SD) | Count | Mean (±SD) | ||
| EDSS | 5 (19%) | 1 (4%) | 0.061 | ||
| 1–1.5 (No disability) (n = 6) | 1 (4%) | 2 | |||
| 2–2.5 (Disability is minimal) (n = 3) | 6 (23%) | 0 | |||
| 3–3.5 (Disability is mild to moderate) (n = 6) | 1 (4%) | 4 (4%) | |||
| 4–4.5 (Disability is moderate) (n = 5) | 2 (8%) | 1 (4%) | |||
| 5–5.5 (Increasing limitation in ability to walk) (n = 3) | 0 | 2 (8%) | |||
| 6–6.5 (Walking assistance is needed) (n = 2) | 0 | 1 (4%) | |||
| 7–7.5 (Confined to wheelchair) (n = 1) | 0 | 0 | |||
| 8–8.5 (Confined to bed or chair) (n = 0) | 0 | 0 | |||
| 9–9.5 (Completely dependent) (n = 0) | 0 | 0 | |||
| Duration of MS, years (9.5 ± 5.12) | 9 (±4.5) | 10.18 (±6) | 0.646 | ||
| Quality of Life_T0 (0.66 ± 0.18) | 0.69 (±0.15) Median = 0.68 | 0.61 (±0.2) Median = 0.60 | 0.330 | ||
| Quality of Life_T1 (0.71 ± 0.16) | 0.74 (±0.13) Median = 0.76 | 0.66 (±0.2) Median = 0.68 | 0.305 | ||
| Cognitive Autonomy | 39.53 (±10.44) Median = 41 | 36.18 (±8.7) Median = 35 | 0.721 | ||
| Behavior Autonomy | 51.4 (±14.77) Median = 51 | 45.1 (±13.7) Median = 37 | 0.217 | ||
| Emotional Autonomy | 45.9 (±7.7) Median = 44 | 45 (±5.5) Median = 46 | 0.281 | ||
| Value Autonomy | 43.53 (±10.27) | 45.18 (±8.8) | 0.683 | ||
| Autonomy | 44 (±12.23) Median = 44 | 40.54 (±9.3) Median = 39 | 0.357 | ||
| Dimensions | Pre-Treatment (Mean ± SD) | Post-Treatment (Mean ± SD) | Difference between Scores Post- and Pre-Treatment (Mean ± SD) | p-Value |
|---|---|---|---|---|
| Moving | 0.64 (±0.25) | 0.68 (±0.27) | 0.03 (±0.09) | 0.102 |
| Seeing | 0.73 (±0.21) | 0.78 (±0.19) | 0.05 (±0.10) | 0.039 |
| Hearing | 0.88 (±0.17) | 0.87 (±0.19) | −0.01 (±0.06) | 0.317 |
| Breathing | 0.69 (±0.3) | 0.77 (±0.25) | 0.08 (±0.12) | 0.007 |
| Sleeping | 0.58 (±0.21) | 0.73 (±0.22) | 0.15 (±0.13) | <0.001 |
| Eating | 0.65 (±0.26) | 0.68 (±0.26) | 0.02 (±0.08) | 0.180 |
| Speech | 0.73 (±0.2) | 0.77 (±0.22) | 0.03 (±0.10) | 0.083 |
| Excretion | 0.49 (±0.28) | 0.53 (±0.27) | 0.04 (±0.10) | 0.059 |
| Usual Activities | 0.51 (±0.31) | 0.56 (±0.3) | 0.05 (±0.10) | 0.027 |
| Mental Function | 0.69 (±0.25) | 0.71 (±0.25) | 0.02 (±0.09) | 0.180 |
| Discomfort | 0.65 (±0.24) | 0.71 (±0.26) | 0.06 (±0.15) | 0.165 |
| Depression | 0.62 (±0.2) | 0.69 (±0.21) | 0.07 (±0.15) | 0.016 |
| Distress | 0.71 (±0.21) | 0.76 (±0.22) | 0.05 (±0.13) | 0.046 |
| Vitality | 0.58 (±0.24) | 0.64 (±0.19) | 0.06 (±0.11) | 0.018 |
| Sexual Activity | 0.77 (±0.22) | 0.78 (±0.23) | 0.01 (±0.06) | 0.317 |
| Total | 0.66 (±0.18) | 0.71 (±0.16) | 0.05 (±0.03) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padureanu, R.; Albu, C.V.; Pirici, I.; Mititelu, R.R.; Subtirelu, M.S.; Turcu-Stiolica, R.A.; Sintonen, H.; Padureanu, V.; Turcu-Stiolica, A. Personal Autonomy as Quality of Life Predictor for Multiple Sclerosis Patients. J. Clin. Med. 2020, 9, 1349. https://doi.org/10.3390/jcm9051349
Padureanu R, Albu CV, Pirici I, Mititelu RR, Subtirelu MS, Turcu-Stiolica RA, Sintonen H, Padureanu V, Turcu-Stiolica A. Personal Autonomy as Quality of Life Predictor for Multiple Sclerosis Patients. Journal of Clinical Medicine. 2020; 9(5):1349. https://doi.org/10.3390/jcm9051349
Chicago/Turabian StylePadureanu, Rodica, Carmen Valeria Albu, Ionica Pirici, Radu Razvan Mititelu, Mihaela Simona Subtirelu, Razvan Aurelian Turcu-Stiolica, Harri Sintonen, Vlad Padureanu, and Adina Turcu-Stiolica. 2020. "Personal Autonomy as Quality of Life Predictor for Multiple Sclerosis Patients" Journal of Clinical Medicine 9, no. 5: 1349. https://doi.org/10.3390/jcm9051349
APA StylePadureanu, R., Albu, C. V., Pirici, I., Mititelu, R. R., Subtirelu, M. S., Turcu-Stiolica, R. A., Sintonen, H., Padureanu, V., & Turcu-Stiolica, A. (2020). Personal Autonomy as Quality of Life Predictor for Multiple Sclerosis Patients. Journal of Clinical Medicine, 9(5), 1349. https://doi.org/10.3390/jcm9051349