Plasma Exchange or Immunoadsorption in Demyelinating Diseases: A Meta-Analysis


Abstract
:1. Introduction
2. Effects of Apheresis Therapy
3. Plasma Exchange
3.1. Multiple Sclerosis (with Relapsing-Remitting and Progressive MS Sub-Sections)
3.2. Clinically Isolated Syndrome
3.3. Optic Neuritis
4. Immunoadsorption
4.1. Multiple Sclerosis (with Relapsing-Remitting and Progressive MS Sub-Sections)
4.2. Clinically Isolated Syndrome
4.3. Neuromyelitis Optica
5. Plasma Exchange vs. Immunoadsorption
5.1. Multiple Sclerosis (with Relapsing-Remitting and Progressive MS Sub-Sections)
5.2. Clinically Isolated Syndrome
5.3. Neuromyelitis Optica
6. Meta-Analysis on Apheresis Effects on Demyelinating Diseases
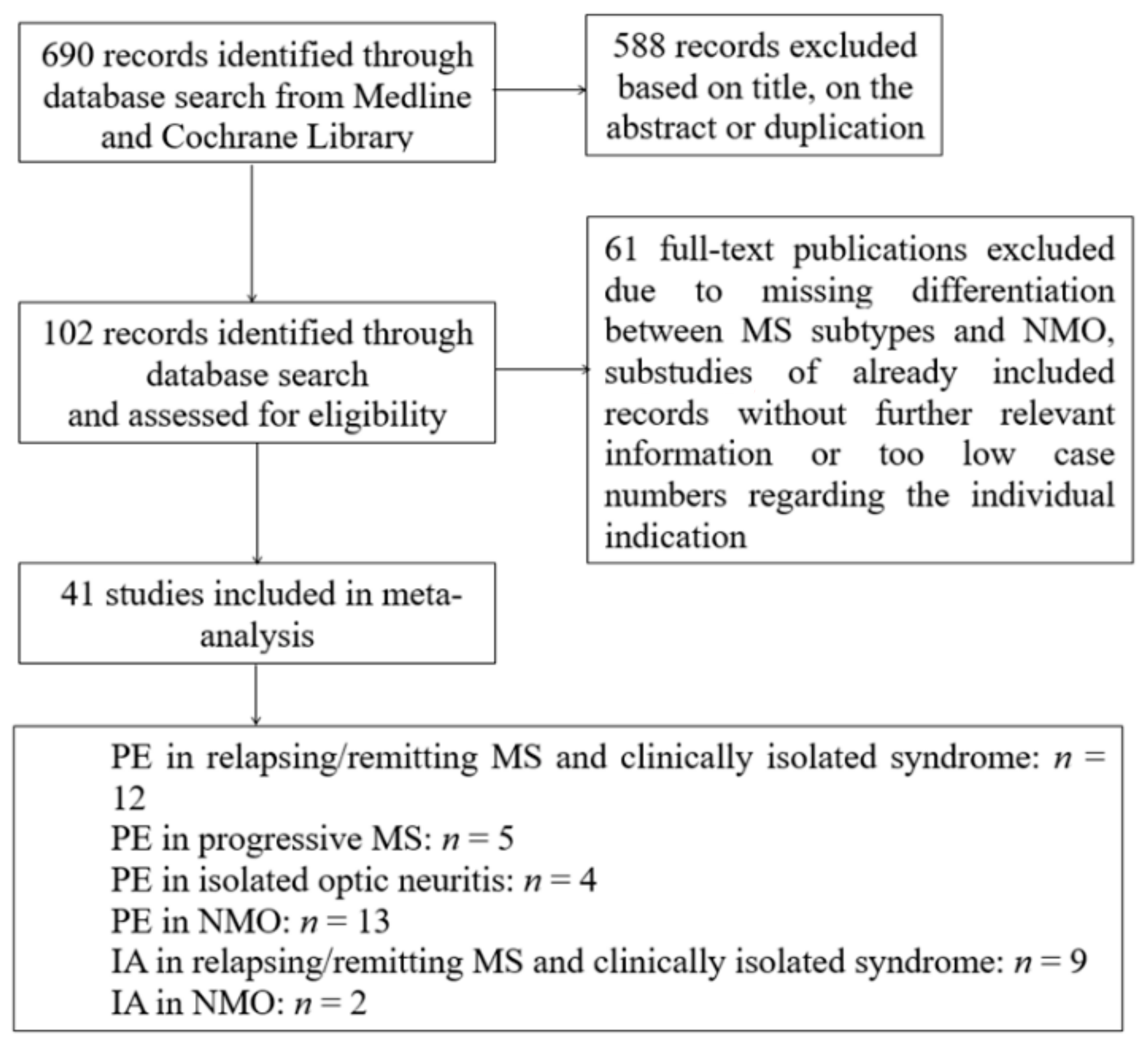
6.1. Search Strategy and Inclusion Criteria
6.2. Statistical Analysis
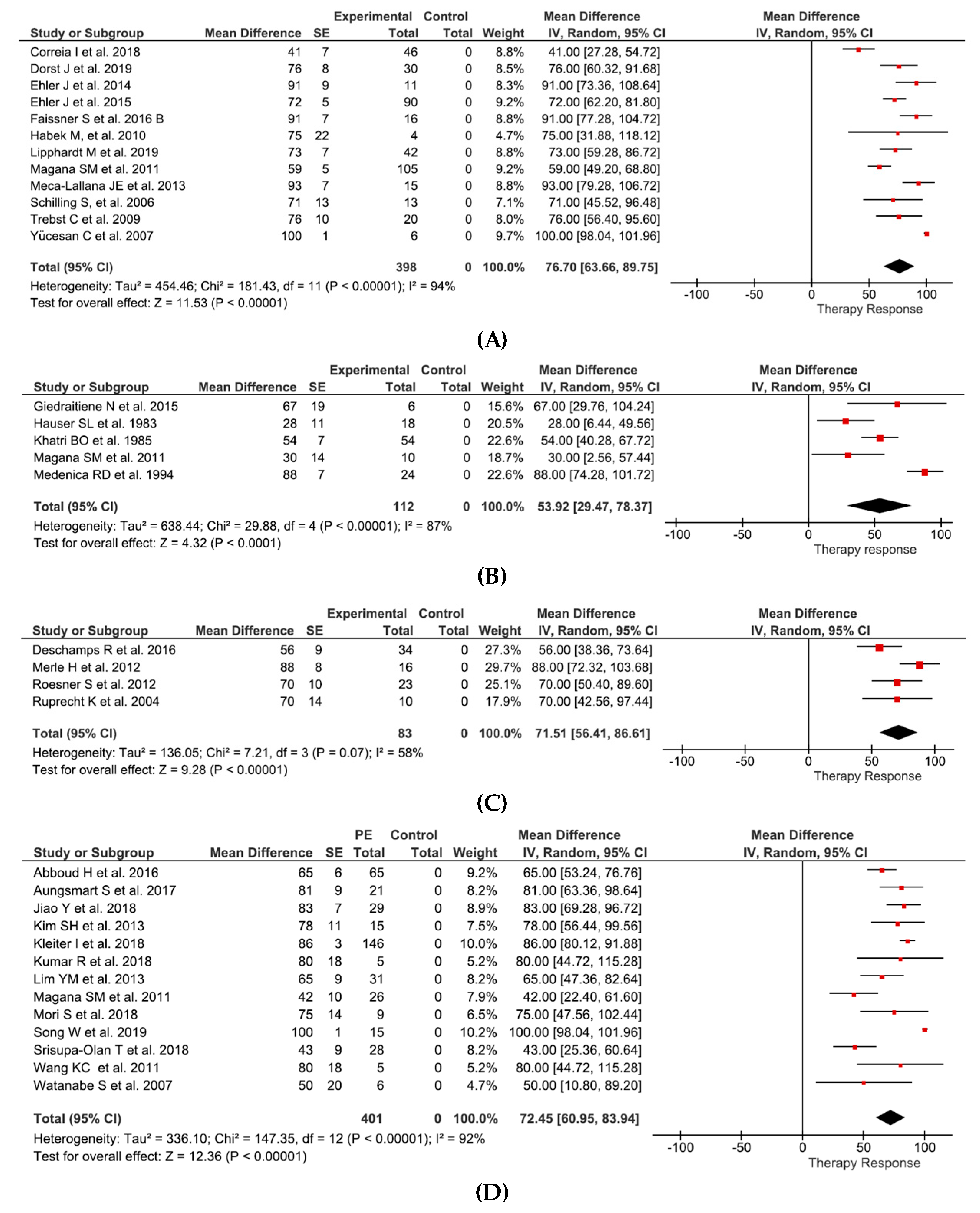
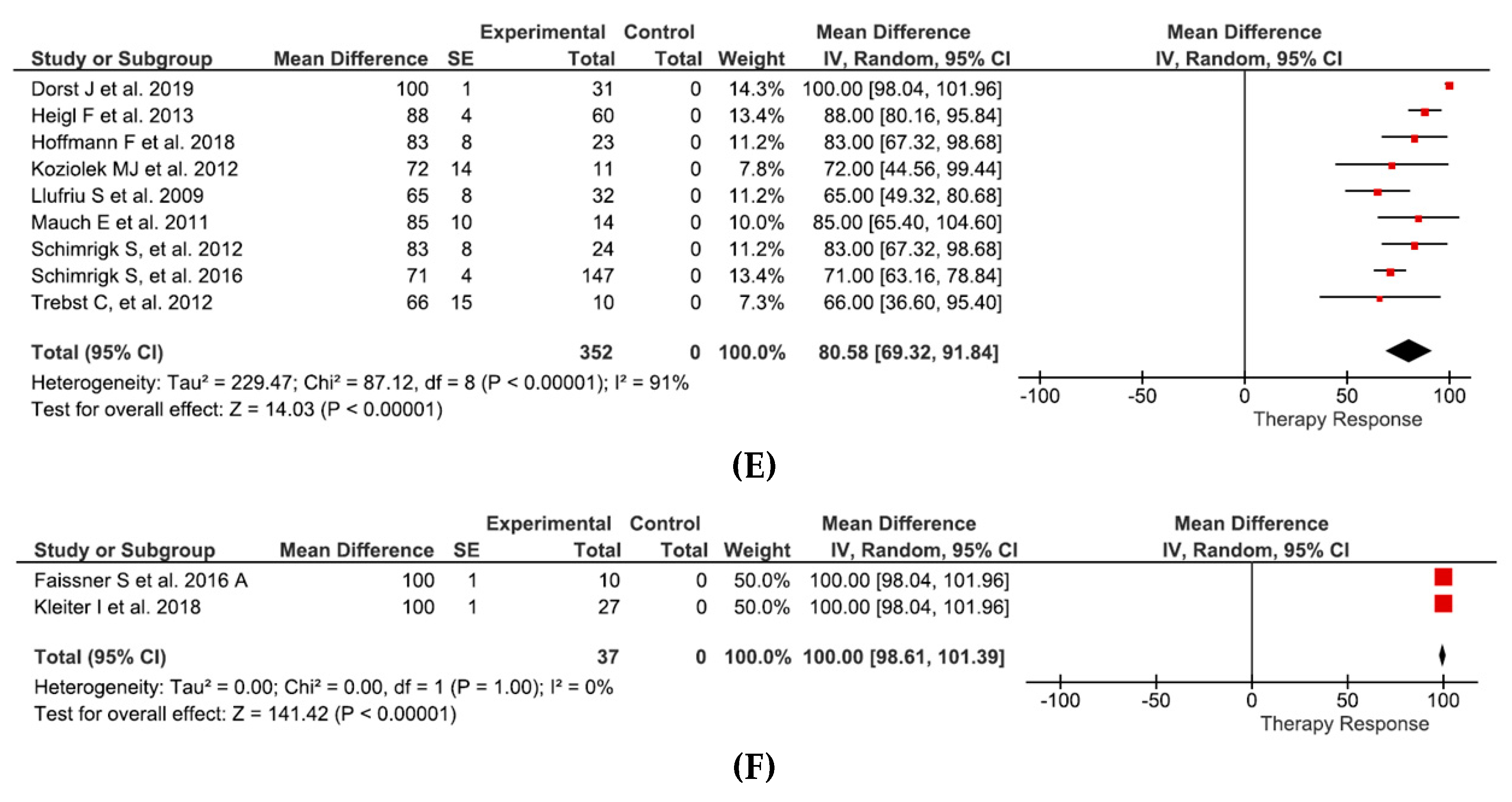
7. Results
8. Safety Profile
8.1. General
8.2. Multiple Sclerosis (with Relapsing-Remitting and Progressive MS Sub-Sections) and Clinically Isolated Syndrome
8.3. Multiple Sclerosis (with Relapsing-Remitting and Progressive MS Sub-Sections) and Neuromyelitis Optica
9. Treatment Predictors
9.1. General
9.2. Multiple Sclerosis (with Relapsing-Remitting and Progressive MS Sub-Sections)
9.3. Neuromyelitis Optica
10. Therapeutic Efficacy and Time Course
11. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| ASFA | American society for apheresis |
| CIS | Clinical isolated syndrome |
| Ig | Immunoglobulin |
| IL | Interleukin |
| IFNγ | Interferon gamma |
| NMO | Neuromyelitis optica |
| MS | Multiple Sclerosis |
| PE | Plasma exchange |
| PPMS | Primary-Progressive MS |
| PRMS | Progressive-Relapsing MS |
| RRMS | Relapsing remitting MS |
| SPMS | Secondary-Progressive MS |
| Th | T helper |
| Treg | T regulatory |
| TNF-α | Tumor necrosis factor alpha |
| VA | Visual acuity |
| VEP | Visual evoked potential |
References
- Brucklacher-Waldert, V.; Stuerner, K.; Kolster, M.; Wolthausen, J.; Tolosa, E. Phenotypical and functional characterization of T helper 17 cells in multiple sclerosis. Brain A J. Neurol. 2009, 132 Pt 12, 3329–3341. [Google Scholar] [CrossRef]
- Loma, I.; Heyman, R. Multiple sclerosis: Pathogenesis and treatment. Curr. Neuropharmacol. 2011, 9, 409–416. [Google Scholar] [CrossRef]
- Leray, E.; Moreau, T.; Fromont, A.; Edan, G. Epidemiology of multiple sclerosis. Rev. Neurol. 2016, 172, 3–13. [Google Scholar] [CrossRef]
- Compston, A.; Coles, A. Multiple sclerosis. Lancet 2008, 372, 1502–1517. [Google Scholar] [CrossRef]
- Toosy, A.T.; Mason, D.F.; Miller, D.H. Optic neuritis. Lancet Neurol. 2014, 13, 83–99. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Correale, J.; Villa, A. Role of CD8+ CD25+ Foxp3+ regulatory T cells in multiple sclerosis. Ann. Neurol. 2010, 67, 625–638. [Google Scholar] [CrossRef]
- Schoenborn, J.R.; Wilson, C.B. Regulation of interferon-gamma during innate and adaptive immune responses. Adv. Immunol. 2007, 96, 41–101. [Google Scholar]
- Minty, A.; Chalon, P.; Derocq, J.M.; Dumont, X.; Guillemot, J.C.; Kaghad, M.; Labit, C.; Leplatois, P.; Liauzun, P.; Miloux, B.; et al. Interleukin-13 is a new human lymphokine regulating inflammatory and immune responses. Nature 1993, 362, 248–250. [Google Scholar] [CrossRef]
- Zhu, J.; Paul, W.E. CD4 T cells: Fates, functions, and faults. Blood 2008, 112, 1557–1569. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, N.; Razavi, S.; Nikzad, E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J. 2017, 19, 1–10. [Google Scholar]
- Nishimura, H.; Enokida, H.; Sakamoto, T.; Takahashi, T.; Hayami, H.; Nakagawa, M. Immunoadsorption plasmapheresis treatment for the recurrent exacerbation of neuromyelitis optica spectrum disorder with a fluctuating anti-aquaporin-4 antibody level. J. Artif. Organs 2018, 21, 378–382. [Google Scholar] [CrossRef]
- Ouyang, W.; Kolls, J.K.; Zheng, Y. The biological functions of T helper 17 cell effector cytokines in inflammation. Immunity 2008, 28, 454–467. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.R. The Balance of Th17 versus Treg Cells in Autoimmunity. Int. J. Mol. Sci. 2018, 19, 730. [Google Scholar] [CrossRef] [Green Version]
- Egg, R.; Reindl, M.; Deisenhammer, F.; Linington, C.; Berger, T. Anti-MOG and anti-MBP antibody subclasses in multiple sclerosis. Mult. Scler. J. 2001, 7, 285–289. [Google Scholar] [CrossRef]
- Dendrou, C.A.; Fugger, L.; Friese, M.A. Immunopathology of multiple sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar] [CrossRef]
- Grigoriadis, N.; van Pesch, V. A basic overview of multiple sclerosis immunopathology. Eur. J. Neurol. 2015, 22, 3–13. [Google Scholar] [CrossRef]
- Howell, O.W.; Reeves, C.A.; Nicholas, R.; Carassiti, D.; Radotra, B.; Gentleman, S.M.; Serafini, B.; Aloisi, F.; Roncaroli, F.; Magliozzi, R.; et al. Meningeal inflammation is widespread and linked to cortical pathology in multiple sclerosis. Brain A J. Neurol. 2011, 134, 2755–2771. [Google Scholar] [CrossRef]
- Stern, J.N.H.; Yaari, G.; Vander Heiden, J.A.; Church, G.; Donahue, W.F.; Hintzen, R.Q.; Huttner, A.J.; Laman, J.D.; Nagra, R.M.; Nylander, A.; et al. B cells populating the multiple sclerosis brain mature in the draining cervical lymph nodes. Sci. Transl. Med. 2014, 6, 248ra107. [Google Scholar] [CrossRef] [Green Version]
- Lucchinetti, C.; Bruck, W.; Parisi, J.; Scheithauer, B.; Rodriguez, M.; Lassmann, H. Heterogeneity of multiple sclerosis lesions: Implications for the pathogenesis of demyelination. Ann. Neurol. 2000, 47, 707–717. [Google Scholar] [CrossRef]
- Wingerchuk, D.M.; Lennon, V.A.; Lucchinetti, C.F.; Pittock, S.J.; Weinshenker, B.G. The spectrum of neuromyelitis optica. Lancet Neurol. 2007, 6, 805–815. [Google Scholar] [CrossRef]
- Bevan, C.; Gelfand, J.M. Therapeutic Management of Severe Relapses in Multiple Sclerosis. Curr. Treat. Options Neurol. 2015, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Sellebjerg, F.; Barnes, D.; Filippini, G.; Midgard, R.; Montalban, X.; Rieckmann, P.; Selmaj, K.; Visser, L.H.; Sorensen, P.S. EFNS guideline on treatment of multiple sclerosis relapses: Report of an EFNS task force on treatment of multiple sclerosis relapses. Eur. J. Neurol. 2005, 12, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Wiendl, H.; Toyka, K.V.; Rieckmann, P.; Gold, R.; Hartung, H.P.; Hohlfeld, R. Basic and escalating immunomodulatory treatments in multiple sclerosis: Current therapeutic recommendations. J. Neurol. 2008, 255, 1449–1463. [Google Scholar] [PubMed] [Green Version]
- Schroder, A.; Linker, R.A.; Gold, R. Plasmapheresis for neurological disorders. Expert Rev. Neurother. 2009, 9, 1331–1339. [Google Scholar] [CrossRef]
- Padmanabhan, A.; Connelly-Smith, L.; Aqui, N.; Balogun, R.A.; Klingel, R.; Meyer, E.; Pham, H.P.; Schneiderman, J.; Witt, V.; Wu, Y.; et al. Guidelines on the Use of Therapeutic Apheresis in Clinical Practice—Evidence-Based Approach from the Writing Committee of the American Society for Apheresis: The Eighth Special Issue. J. Clin. Apher. 2019, 34, 171–354. [Google Scholar] [CrossRef]
- Cortese, I.; Chaudhry, V.; So, Y.T.; Cantor, F.; Cornblath, D.R.; Rae-Grant, A. Evidence-based guideline update: Plasmapheresis in neurologic disorders: Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2011, 76, 294–300. [Google Scholar] [CrossRef] [Green Version]
- Paroder-Belenitsky, M.; Pham, H. Immunoadsorption, Transfusion Medicine and Hemostasis, 3rd ed.; Stacy Masucci: Cambridge, UK, 2019; pp. 497–500. [Google Scholar]
- Available online: https://www.kompetenznetz-multiplesklerose.de/wp-content/uploads/2016/02/dgn-kknms_ms-ll_20140813.pdf (accessed on 20 May 2020).
- Navarro-Martinez, R.; Cauli, O. Therapeutic Plasmapheresis with Albumin Replacement in Alzheimer’s Disease and Chronic Progressive Multiple Sclerosis: A Review. Pharmaceuticals 2020, 13, 28. [Google Scholar] [CrossRef] [Green Version]
- Koziolek, M.; Muhlhausen, J.; Friede, T.; Ellenberger, D.; Sigler, M.; Huppke, B.; Gartner, J.; Muller, G.A.; Huppke, P. Therapeutic apheresis in pediatric patients with acute CNS inflammatory demyelinating disease. Blood Purif. 2013, 36, 92–97. [Google Scholar] [CrossRef]
- Koziolek, M.J.; Tampe, D.; Bahr, M.; Dihazi, H.; Jung, K.; Fitzner, D.; Klingel, R.; Muller, G.A.; Kitze, B. Immunoadsorption therapy in patients with multiple sclerosis with steroid-refractory optical neuritis. J. Neuroinflamm. 2012, 9, 80. [Google Scholar] [CrossRef] [Green Version]
- Jamshidian, A.; Kazemi, M.; Shaygannejad, V.; Salehi, M. The Effect of Plasma Exchange on the Expression of FOXP3 and RORC2 in Relapsed Multiple Sclerosis Patients. Iran. J. Immunol. 2015, 12, 311–318. [Google Scholar] [PubMed]
- Stork, L.; Ellenberger, D.; Beissbarth, T.; Friede, T.; Lucchinetti, C.F.; Bruck, W.; Metz, I. Differences in the Reponses to Apheresis Therapy of Patients With 3 Histopathologically Classified Immunopathological Patterns of Multiple Sclerosis. JAMA Neurol. 2018, 75, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Khatri, B.O.; McQuillen, M.P.; Harrington, G.J.; Schmoll, D.; Hoffmann, R.G. Chronic progressive multiple sclerosis: Double-blind controlled study of plasmapheresis in patients taking immunosuppressive drugs. Neurology 1985, 35, 312–319. [Google Scholar] [CrossRef]
- Weiner, H.L.; Dau, P.C.; Khatri, B.O.; Petajan, J.H.; Birnbaum, G.; McQuillen, M.P.; Fosburg, M.T.; Feldstein, M.; Orav, E.J. Double-blind study of true vs. sham plasma exchange in patients treated with immunosuppression for acute attacks of multiple sclerosis. Neurology 1989, 39, 1143–1149. [Google Scholar] [CrossRef]
- Weinshenker, B.G.; O’Brien, P.C.; Petterson, T.M.; Noseworthy, J.H.; Lucchinetti, C.F.; Dodick, D.W.; Pineda, A.A.; Stevens, L.N.; Rodriguez, M. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann. Neurol. 1999, 46, 878–886. [Google Scholar] [CrossRef]
- Habek, M.; Barun, B.; Puretic, Z.; Brinar, V.V. Treatment of steroid unresponsive relapse with plasma exchange in aggressive multiple sclerosis. Ther. Apher. Dial. 2010, 14, 298–302. [Google Scholar] [CrossRef]
- Schilling, S.; Linker, R.A.; Konig, F.B.; Koziolek, M.; Bahr, M.; Muller, G.A.; Paulus, W.; Gartner, J.; Bruck, W.; Chan, A.; et al. Plasma exchange therapy for steroid-unresponsive multiple sclerosis relapses: Clinical experience with 16 patients. Der Nervenarzt 2006, 77, 430–438. [Google Scholar] [CrossRef]
- Trebst, C.; Reising, A.; Kielstein, J.T.; Hafer, C.; Stangel, M. Plasma exchange therapy in steroid-unresponsive relapses in patients with multiple sclerosis. Blood Purif. 2009, 28, 108–115. [Google Scholar] [CrossRef]
- Magana, S.M.; Keegan, B.M.; Weinshenker, B.G.; Erickson, B.J.; Pittock, S.J.; Lennon, V.A.; Rodriguez, M.; Thomsen, K.; Weigand, S.; Mandrekar, J.; et al. Beneficial plasma exchange response in central nervous system inflammatory demyelination. Arch. Neurol. 2011, 68, 870–878. [Google Scholar] [CrossRef] [Green Version]
- Dorst, J.; Fangerau, T.; Taranu, D.; Eichele, P.; Dreyhaupt, J.; Michels, S.; Schuster, J.; Ludolph, A.C.; Senel, M.; Tumani, H. Safety and efficacy of immunoadsorption versus plasma exchange in steroid-refractory relapse of multiple sclerosis and clinically isolated syndrome: A randomised, parallel-group, controlled trial. EClinicalMedicine 2019, 16, 98–106. [Google Scholar] [CrossRef]
- Ehler, J.; Koball, S.; Sauer, M.; Mitzner, S.; Hickstein, H.; Benecke, R.; Zettl, U.K. Response to Therapeutic Plasma Exchange as a Rescue Treatment in Clinically Isolated Syndromes and Acute Worsening of Multiple Sclerosis: A Retrospective Analysis of 90 Patients. PLoS ONE 2015, 10, e0134583. [Google Scholar] [CrossRef]
- Lipphardt, M.; Muhlhausen, J.; Kitze, B.; Heigl, F.; Mauch, E.; Helms, H.J.; Muller, G.A.; Koziolek, M.J. Immunoadsorption or plasma exchange in steroid-refractory multiple sclerosis and neuromyelitis optica. J. Clin. Apher. 2019, 34, 381–391. [Google Scholar] [CrossRef]
- Deschamps, R.; Gueguen, A.; Parquet, N.; Saheb, S.; Driss, F.; Mesnil, M.; Vignal, C.; Aboab, J.; Depaz, R.; Gout, O. Plasma exchange response in 34 patients with severe optic neuritis. J. Neurol. 2016, 263, 883–887. [Google Scholar] [CrossRef]
- Ruprecht, K.; Klinker, E.; Dintelmann, T.; Rieckmann, P.; Gold, R. Plasma exchange for severe optic neuritis: Treatment of 10 patients. Neurology 2004, 63, 1081–1083. [Google Scholar] [CrossRef]
- Yucesan, C.; Arslan, O.; Arat, M.; Yucemen, N.; Ayyildiz, E.; Ilhan, O.; Mutluer, N. Therapeutic plasma exchange in the treatment of neuroimmunologic disorders: Review of 50 cases. Transfus. Apher. Sci. 2007, 36, 103–107. [Google Scholar] [CrossRef]
- Meca-Lallana, J.E.; Hernandez-Clares, R.; Leon-Hernandez, A.; Genoves Aleixandre, A.; Cacho Perez, M.; Martin-Fernandez, J.J. Plasma exchange for steroid-refractory relapses in multiple sclerosis: An observational, MRI pilot study. Clin. Ther. 2013, 35, 474–485. [Google Scholar] [CrossRef]
- Ehler, J.; Koball, S.; Sauer, M.; Hickstein, H.; Mitzner, S.; Benecke, R.; Zettl, U.K. Therapeutic plasma exchange in glucocorticosteroid-unresponsive patients with Clinically Isolated Syndrome. Ther. Apher. Dial. 2014, 18, 489–496. [Google Scholar] [CrossRef]
- Faissner, S.; Nikolayczik, J.; Chan, A.; Hellwig, K.; Gold, R.; Yoon, M.S.; Haghikia, A. Plasmapheresis and immunoadsorption in patients with steroid refractory multiple sclerosis relapses. J. Neurol. 2016, 263, 1092–1098. [Google Scholar] [CrossRef]
- Correia, I.; Ribeiro, J.J.; Isidoro, L.; Batista, S.; Nunes, C.; Macario, C.; Borges, C.; Tomaz, J.; Sousa, L. Plasma exchange in severe acute relapses of multiple sclerosis—Results from a Portuguese cohort. Mult. Scler. Relat. Disord. 2018, 19, 148–152. [Google Scholar] [CrossRef]
- Hauser, S.L.; Dawson, D.M.; Lehrich, J.R.; Beal, M.F.; Kevy, S.V.; Weiner, H.L. Immunosuppression and plasmapheresis in chronic progressive multiple sclerosis. Design of a clinical trial. Arch. Neurol. 1983, 40, 687–690. [Google Scholar] [CrossRef]
- Medenica, R.D.; Mukerjee, S.; Huschart, T.; Corbitt, W. Interferon inhibitor factor predicting success of plasmapheresis in patients with multiple sclerosis. J. Clin. Apher. 1994, 9, 216–221. [Google Scholar] [CrossRef]
- Giedraitiene, N.; Kaubrys, G.; Kizlaitiene, R.; Bagdonaite, L.; Griskevicius, L.; Valceckiene, V.; Stoskus, M. Therapeutic Plasma Exchange in Multiple Sclerosis Patients with Abolished Interferon-beta Bioavailability. Med. Sci. Monit. 2015, 21, 1512–1519. [Google Scholar]
- Roesner, S.; Appel, R.; Gbadamosi, J.; Martin, R.; Heesen, C. Treatment of steroid-unresponsive optic neuritis with plasma exchange. Acta Neurol. Scand. 2012, 126, 103–108. [Google Scholar] [CrossRef]
- Merle, H.; Olindo, S.; Jeannin, S.; Valentino, R.; Mehdaoui, H.; Cabot, F.; Donnio, A.; Hage, R.; Richer, R.; Smadja, D.; et al. Treatment of optic neuritis by plasma exchange (add-on) in neuromyelitis optica. Arch. Ophthalmol. 2012, 130, 858–862. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, S.; Nakashima, I.; Misu, T.; Miyazawa, I.; Shiga, Y.; Fujihara, K.; Itoyama, Y. Therapeutic efficacy of plasma exchange in NMO-IgG-positive patients with neuromyelitis optica. Mult. Scler. 2007, 13, 128–132. [Google Scholar] [CrossRef]
- Wang, K.C.; Wang, S.J.; Lee, C.L.; Chen, S.Y.; Tsai, C.P. The rescue effect of plasma exchange for neuromyelitis optica. J. Clin. Neurosci. 2011, 18, 43–46. [Google Scholar] [CrossRef]
- Lim, Y.M.; Pyun, S.Y.; Kang, B.H.; Kim, J.; Kim, K.K. Factors associated with the effectiveness of plasma exchange for the treatment of NMO-IgG-positive neuromyelitis optica spectrum disorders. Mult. Scler. 2013, 19, 1216–1218. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, W.; Huh, S.Y.; Lee, K.Y.; Jung, I.J.; Kim, H.J. Clinical efficacy of plasmapheresis in patients with neuromyelitis optica spectrum disorder and effects on circulating anti-aquaporin-4 antibody levels. J. Clin. Neurol. 2013, 9, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Abboud, H.; Petrak, A.; Mealy, M.; Sasidharan, S.; Siddique, L.; Levy, M. Treatment of acute relapses in neuromyelitis optica: Steroids alone versus steroids plus plasma exchange. Mult. Scler. 2016, 22, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Aungsumart, S.; Apiwattanakul, M. Clinical outcomes and predictive factors related to good outcomes in plasma exchange in severe attack of NMOSD and long extensive transverse myelitis: Case series and review of the literature. Mult. Scler. Relat. Disord. 2017, 13, 93–97. [Google Scholar] [CrossRef]
- Srisupa-Olan, T.; Siritho, S.; Kittisares, K.; Jitprapaikulsan, J.; Sathukitchai, C.; Prayoonwiwat, N. Beneficial effect of plasma exchange in acute attack of neuromyelitis optica spectrum disorders. Mult. Scler. Relat. Disord. 2018, 20, 115–121. [Google Scholar] [CrossRef]
- Jiao, Y.; Cui, L.; Zhang, W.; Zhang, Y.; Wang, W.; Zhang, L.; Tang, W.; Jiao, J. Plasma Exchange for Neuromyelitis Optica Spectrum Disorders in Chinese Patients and Factors Predictive of Short-term Outcome. Clin. Ther. 2018, 40, 603–612. [Google Scholar] [CrossRef]
- Mori, S.; Kurimoto, T.; Ueda, K.; Nakamura, M. Short-term effect of additional apheresis on visual acuity changes in patients with steroid-resistant optic neuritis in neuromyelitis optica spectrum disorders. Jpn. J. Ophthalmol. 2018, 62, 525–530. [Google Scholar] [CrossRef]
- Kumar, R.; Paul, B.S.; Singh, G.; Kaur, A. Therapeutic Efficacy of Plasma Exchange in Neuromyelitis Optica. Ann. Indian Acad. Neurol. 2018, 21, 140–143. [Google Scholar]
- Kleiter, I.; Gahlen, A.; Borisow, N.; Fischer, K.; Wernecke, K.D.; Hellwig, K.; Pache, F.; Ruprecht, K.; Havla, J.; Kumpfel, T.; et al. Apheresis therapies for NMOSD attacks: A retrospective study of 207 therapeutic interventions. Neurol. Neuroimmunol. Neuroinflamm. 2018, 5, e504. [Google Scholar] [CrossRef] [Green Version]
- Song, W.; Qu, Y.; Huang, X. Plasma exchange: An effective add-on treatment of optic neuritis in neuromyelitis optica spectrum disorders. Int. Ophthalmol. 2019, 39, 2477–2483. [Google Scholar] [CrossRef]
- De Andres, C.; Anaya, F.; Gimenez-Roldan, S. Plasma immunoadsorption treatment of malignant multiple sclerosis with severe and prolonged relapses. Rev. Neurol. 2000, 30, 601–605. [Google Scholar]
- Heigl, F.; Hettich, R.; Arendt, R.; Durner, J.; Koehler, J.; Mauch, E. Immunoadsorption in steroid-refractory multiple sclerosis: Clinical experience in 60 patients. Atheroscler. Suppl. 2013, 14, 167–173. [Google Scholar] [CrossRef]
- Mauch, E.; Zwanzger, J.; Hettich, R.; Fassbender, C.; Klingel, R.; Heigl, F. Immunoadsorption for steroid-unresponsive multiple sclerosis-relapses: Clinical data of 14 patients. Der Nervenarzt 2011, 82, 1590–1595. [Google Scholar] [CrossRef]
- Trebst, C.; Bronzlik, P.; Kielstein, J.T.; Schmidt, B.M.; Stangel, M. Immunoadsorption therapy for steroid-unresponsive relapses in patients with multiple sclerosis. Blood Purif. 2012, 33, 1–6. [Google Scholar] [CrossRef]
- Hoffmann, F.; Kraft, A.; Heigl, F.; Mauch, E.; Koehler, J.; Harms, L.; Kumpfel, T.; Kohler, W.; Ehrlich, S.; Bayas, A.; et al. Tryptophan immunoadsorption during pregnancy and breastfeeding in patients with acute relapse of multiple sclerosis and neuromyelitis optica. Ther. Adv. Neurol. Disord. 2018, 11. [Google Scholar] [CrossRef] [PubMed]
- Moldenhauer, A.; Haas, J.; Wascher, C.; Derfuss, T.; Hoffmann, K.T.; Kiesewetter, H.; Salama, A. Immunoadsorption patients with multiple sclerosis: An open-label pilot study. Eur. J. Clin. Investig. 2005, 35, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Schimrigk, S.; Adibi, I.; Eberl, A.; Selka, I.; Galle, J.; Schmidt, S.; Fritz, H.G.; Fassbender, C.; Klingel, R.; Fuchtemann, D.; et al. Immunoadsorption as Relapse Escalation Therapy for Multiple Sclerosis. Aktuel. Neurol. 2012, 39, 174–179. [Google Scholar]
- Schimrigk, S.; Faiss, J.; Kohler, W.; Gunther, A.; Harms, L.; Kraft, A.; Ehrlich, S.; Eberl, A.; Fassbender, C.; Klingel, R.; et al. Escalation Therapy of Steroid Refractory Multiple Sclerosis Relapse with Tryptophan Immunoadsorption—Observational Multicenter Study with 147 Patients. Eur. Neurol. 2016, 75, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Faissner, S.; Nikolayczik, J.; Chan, A.; Gold, R.; Yoon, M.S.; Haghikia, A. Immunoadsorption in patients with neuromyelitis optica spectrum disorder. Ther. Adv. Neurol. Disord. 2016, 9, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Hohenstein, B.; Passauer, J.; Ziemssen, T.; Julius, U. Immunoadsorption with regenerating systems in neurological disorders --A single center experience. Atheroscler. Suppl. 2015, 18, 119–123. [Google Scholar] [CrossRef]
- Muhlhausen, J.; Kitze, B.; Huppke, P.; Muller, G.A.; Koziolek, M.J. Apheresis in treatment of acute inflammatory demyelinating disorders. Atheroscler. Suppl. 2015, 18, 251–256. [Google Scholar] [CrossRef]
- Llufriu, S.; Castillo, J.; Blanco, Y.; Ramio-Torrenta, L.; Rio, J.; Valles, M.; Lozano, M.; Castella, M.D.; Calabia, J.; Horga, A.; et al. Plasma exchange for acute attacks of CNS demyelination: Predictors of improvement at 6 months. Neurology 2009, 73, 949–953. [Google Scholar] [CrossRef]
- Bramlage, C.P.; Schroder, K.; Bramlage, P.; Ahrens, K.; Zapf, A.; Muller, G.A.; Koziolek, M.J. Predictors of complications in therapeutic plasma exchange. J. Clin. Apher. 2009, 24, 225–231. [Google Scholar] [CrossRef]
- Mokrzycki, M.H.; Kaplan, A.A. Therapeutic plasma exchange: Complications and management. Am. J. Kidney Dis. 1994, 23, 817–827. [Google Scholar] [CrossRef]
- Samtleben, W.; Blumenstein, M.; Liebl, L.; Gurland, H.J. Membrane plasma separation for treatment of immunologically mediated diseases. Trans. Am. Soc. Artif. Intern. Organs 1980, 26, 12–16. [Google Scholar] [PubMed]
- Sprenger, K.B.; Rasche, H.; Franz, H.E. Membrane plasma separation: Complications and monitoring. Artif. Organs 1984, 8, 360–363. [Google Scholar] [PubMed]
- Kohler, W.; Bucka, C.; Klingel, R. A randomized and controlled study comparing immunoadsorption and plasma exchange in myasthenic crisis. J. Clin. Apher. 2011, 26, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Zollner, S.; Pablik, E.; Druml, W.; Derfler, K.; Rees, A.; Biesenbach, P. Fibrinogen reduction and bleeding complications in plasma exchange, immunoadsorption and a combination of the two. Blood Purif. 2014, 38, 160–166. [Google Scholar] [CrossRef]
- Schneider-Gold, C.; Krenzer, M.; Klinker, E.; Mansouri-Thalegani, B.; Mullges, W.; Toyka, K.V.; Gold, R. Immunoadsorption versus plasma exchange versus combination for treatment of myasthenic deterioration. Ther. Adv. Neurol. Disord. 2016, 9, 297–303. [Google Scholar] [CrossRef] [Green Version]
- Keegan, M.; Pineda, A.A.; McClelland, R.L.; Darby, C.H.; Rodriguez, M.; Weinshenker, B.G. Plasma exchange for severe attacks of CNS demyelination: Predictors of response. Neurology 2002, 58, 143–146. [Google Scholar] [CrossRef]
- Heigl, F.; Hettich, R.; Suckfuell, M.; Luebbers, C.W.; Osterkorn, D.; Osterkorn, K.; Canis, M. Fibrinogen/LDL apheresis as successful second-line treatment of sudden hearing loss: A retrospective study on 217 patients. Atheroscler. Suppl. 2009, 10, 95–101. [Google Scholar] [CrossRef]
- Sim, F.J.; Zhao, C.; Penderis, J.; Franklin, R.J. The age-related decrease in CNS remyelination efficiency is attributable to an impairment of both oligodendrocyte progenitor recruitment and differentiation. J. Neurosci. 2002, 22, 2451–2459. [Google Scholar] [CrossRef]
- Freedman, M.S.; De Stefano, N.; Barkhof, F.; Polman, C.H.; Comi, G.; Uitdehaag, B.M.; Casset-Semanaz, F.; Hennessy, B.; Lehr, L.; Stubinski, B.; et al. Patient subgroup analyses of the treatment effect of subcutaneous interferon beta-1a on development of multiple sclerosis in the randomized controlled REFLEX study. J. Neurol. 2014, 261, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Kleiter, I.; Gahlen, A.; Borisow, N.; Fischer, K.; Wernecke, K.D.; Wegner, B.; Hellwig, K.; Pache, F.; Ruprecht, K.; Havla, J.; et al. Neuromyelitis optica: Evaluation of 871 attacks and 1153 treatment courses. Ann. Neurol. 2016, 79, 206–216. [Google Scholar] [CrossRef]
- Zekeridou, A.; Lennon, V.A. Aquaporin-4 autoimmunity. Neurol. Neuroimmunol. Neuroinflamm. 2015, 2, e110. [Google Scholar] [CrossRef] [PubMed]
- Savransky, A.; Rubstein, A.; Rios, M.H.; Vergel, S.L.; Velasquez, M.C.; Sierra, S.P.; Marcarian, G.; Alba, R.; Pugliese, A.M.; Tenembaum, S. Prognostic indicators of improvement with therapeutic plasma exchange in pediatric demyelination. Neurology 2019, 93, 2065–2073. [Google Scholar] [CrossRef] [PubMed]
- Goto, H.; Matsuo, H.; Nakane, S.; Izumoto, H.; Fukudome, T.; Kambara, C.; Shibuya, N. Plasmapheresis affects T helper type-1/T helper type-2 balance of circulating peripheral lymphocytes. Ther. Apher. 2001, 5, 494–496. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| “Relapsing-Remitting Multiple Sclerosis” and “Clinically Isolated Syndrome” | |||||||
| Citation | Year | n | Design | No. of Treatments | Treated Plasma Volume (mL) | Outcome | Limitation |
| [36] | 1989 | 116 | Double-blind, multi-center, randomized | 11 | n.a. | Significant improvement after 4 weeks | No plasmapheresis protocol specifications |
| [37] | 1999 | 36 | Double-blind | 7 | 3000 | Therapy response in 42% of patients | Patient collective with heterogenous MS-types |
| [39] | 2005 | 13 | Retrospective | 5 | 3000 | Therapy response in 71% of patients | Small number of subjects |
| [47] | 2007 | 6 | Retrospective | 4 | 1.0-fold plasma volume | Therapy response in 100% of patients | Small number of subjects |
| [40] | 2009 | 20 | Retrospective | 3–7 | 1.5-fold plasma volume | Therapy response in 76% of patients regarding visual acuity | Small number of subjects |
| [38] | 2010 | 4 | Retrospective | 5 | 2750 | Therapy response in 75% of patients | no placebo, Small number of subjects, the study was observational in character |
| [41] | 2011 | 153 | Retrospective | 7 | n.a. | Therapy response in 59% of patients | Patient collective with heterogenous MS-types |
| [48] | 2013 | 15 | Retrospective | ≥7 | 1.0-fold plasma volume | Therapy response in 93.3% of patients | RRMS + CIS |
| [49] | 2014 | 11 | Retrospective | Median 7 (3–8) | 3000 (2200–3500) | Therapy response in 91% of patients | CIS only |
| [43] | 2015 | 90 | Retrospective | 3–8 | 1.0-fold plasma volume | Therapy response in 72% of patients | The lack of a control group |
| [50] | 2016 | 16 | Retrospective | n.a. | 2000 | Therapy response in 91% of patients regarding visual evoked potential | Small number of subjects and a higher expanded disability status scale in patients in the PE only group |
| [51] | 2018 | 46 | Retrospective | Mean 7.39 sessions | n.a. | Complete therapy response in 41% of patients and partial therapy response in 39% of patients | Patient collective with heterogenous MS-types |
| [44] | 2019 | 42 | Retrospective | 4–11 | Mean 2930 median 2000 | Therapy response in 73% of patients | patients without sufficient follow-up data had a significantly higher patient age and longer duration of disease |
| [42] | 2019 | 30 | Double-blind, randomized, uni-center | On 5 days | 0.69 ± 0.12-fold individual total plasma volume | Therapy response in 76% of patients | Lack of blinding and small number of subjects |
| “Progressive Multiple Sclerosis” | |||||||
| Citation | Year | n | Design | No. of Treatments | Treated Plasma Volume (mL) | Outcome | Limitation |
| [52] | 1983 | 18 | Prospective, randomized | 4–5 | n.a. | Therapy response in 27.8% of patients | Small number of subjects, no plasmapheresis protocol specifications |
| [35] | 1985 | 54 | Double-blind controlled | 20 | n.a. | Therapy response in 54% of patients | No plasmapheresis protocol specifications |
| [53] | 1994 | 24 | Prospective | 8 | n.a. | Therapy response in 87.5% of patients | Small number of subjects, no plasmapheresis protocol specifications |
| [41] | 2011 | 10 | Retrospective | 7 | n.a. | Therapy response in 30% of patients | Small number of subjects |
| [54] | 2015 | 6 | open-label, single-center proof of concept study | 4 | 2000–2500 | Therapy response in 66.7% of patients | Small number of subjects |
| “Isolated Optic Neuritis” | |||||||
| Citation | Year | n | Design | No. of Treatments | Treated Plasma Volume (mL) | Outcome | Limitation |
| [46] | 2004 | 10 | Retrospective | n.a. | n.a. | Therapy response in 70% of patients | Small number of subjects |
| [55] | 2012 | 23 | Retrospective | 5 | ~3000 | Therapy response in 70% of patients | heterogenous |
| [56] | 2012 | 16 | Retrospective | 5 | 1.0-fold plasma volume | Therapy response in 87.5% of patients | Small number of subjects |
| [45] | 2016 | 34 | Retrospective | Median 5, range 5–10 | 1.5-fold body mass volume | Therapy response in 56% of patients regarding visual acuity | The lack of a control group |
| “Neuromyelitis Optica” | |||||||
| Citation | Year | n | Design | No. of Treatments | Treated Plasma Volume (mL) | Outcome | Limitation |
| [57] | 2007 | 6 | Retrospective | 3–5 | 2000–3000 | Therapy response in 50% of patients | Small number of subjects |
| [58] | 2011 | 5 | Retrospective | ≥5 | 1.0-fold plasma volume | Therapy response in 80% of patients | Small number of subjects |
| [41] | 2011 | 26 | Retrospective | 7 | n.a. | Therapy response in 42.3% of patients | Historical cohort study |
| [59] | 2013 | 31 | Retrospective | n.a. | n.a. | Therapy response in 65% of patients | No study controlled treatment regimes |
| [60] | 2013 | 15 | Retrospective | 6 | 1.0–1.5-fold plasma volume | Therapy response in 78% of patients | Small number of subjects |
| [61] | 2016 | 65 | Retrospective | 5–7 | 1.5-fold plasma volume | Therapy response in 65% of patients | Selection bias; use of EDSS scores as the primary outcome measure |
| [62] | 2017 | 21 | Retrospective | 5 | n.a. | Therapy response in 81% of patients | Use of EDSS scores as the primary outcome measure |
| [63] | 2018 | 28 | Retrospective | 5 | 1000 | Therapy response in 42.9% of patients | Use of EDSS scores as the primary outcome measure |
| [64] | 2018 | 29 | Retrospective | 2–7 | 1.0-fold plasma volume | Therapy response in 82.8% of patients | Heterogenous treatment protocols |
| [65] | 2018 | 9 | Retrospective | 7 | 1.0-fold plasma volume | Therapy response in 75% of patients | Small number of subjects |
| [66] | 2018 | 5 | Retrospective | 5 (3–7) | 1.0-fold plasma volume | Therapy response in 80% of patients | Small number of subjects |
| [67] | 2018 | 146 | Retrospective | ≥3 | n.a. | Therapy response in 86% of patients | Heterogenous treatment protocols |
| [68] | 2019 | 15 | Retrospective | 2–3 | n.a | Therapy response in 100% of patients | Small number of subjects |
| “RRMS” and “CIS” | ||||||||
| Citation | Year | n | Design | No. of Treatments | Treated Plasma Volume (mL) | Matrix of Adsorber | Outcome | Limitation |
| [69] | 2000 | 3 | Retrospective | 5–6 | n.a. | n.a. | Therapy response in 100% of patients | small number of subjects |
| [74] | 2005 | 12 | Prospective | 14 | 1.5-fold plasma volume | Sepharose-conjugated sheep antibodies to human immunoglobulin (IgG) | No significant therapy response | small number of subjects and patient collective with heterogenous MS-types |
| [71] | 2011 | 14 | Retrospective | 5–6 | n.a. | Tryptophan | Therapy response in 85% of patients | small number of subjects |
| [75] | 2012 | 24 | Retrospective | Mean 5 (range 3–6) | 2000–2500 | Tryptophan | Therapy response in 83% of patients | small number of subjects and patient collective with heterogenous MS-types |
| [72] | 2012 | 10 | Retrospective | 5–7 | 2500 | Tryptophan | Therapy response in 66% of patients | small number of subjects |
| [32] | 2012 | 11 | Prospective | 5 | 2500 | Tryptophan | Therapy response in 72% of patients | small number of subjects |
| [70] | 2013 | 60 | Retrospective | 6 | 2000 | Tryptophan | Therapy response in 88% of patients | only qualitative data regarding the therapeutic success and clinical data on tolerability were available |
| [76] | 2016 | 147 | Retrospective | n.a. | 2000–2500 | Tryptophan | Therapy response in 71% of patients | Expanded Disability Status Scale was used to measure a change in relapse-related disability |
| [73] | 2018 | 23 | Retrospective | Mean 5.8 | 2031 ± 230 | Tryptophan | Therapy response in 83% of patients | Lack of a control group; use of immunoadsorption was limited in some study centers |
| [44] | 2019 | 32 | Retrospective | 5–7 | 2000–2500 | Tryptophan | Therapy response in 65% of patients | patients without sufficient follow-up data had a significantly higher patient age and longer duration of disease |
| [42] | 2019 | 31 | Prospective, double-blind, randomized, uni-center | On 5 days | 2.0-fold total plasma volume on day 1, and the 2.5-fold total plasma volume on day 2–5 | protein A | Therapy response in 100% of patients | Lack of blinding and small number of subjects |
| “NMO” | ||||||||
| Citation | Year | n | Design | No. of Treatments | Treated Plasma Volume (mL) | Matrix of Adsorber | Outcome | Limitation |
| [77] | 2016 | 10 | Retrospective | Mean 5.2 (3–7) | 2000–2500 | Tryptophan | Therapy response in 100% of patients | Small number of subjects |
| [67] | 2018 | 27 | Retrospective | ≥3 | n.a. | Tryptophan or Protein A | Therapy response in 100% of patients | Heterogenous treatment protocols |
| “Multiple Sclerosis” (with Relapsing-Remitting and Progressive MS Sub-Sections) | |||
| Classification | Predictor | Citation | Meaning |
| Clinical signs and symptoms | EDSS ≤ 5 | [43] | Indicates good apheresis response |
| Preserved deep tendon reflexes | [41] | Indicates good apheresis response | |
| Demographics | Younger age | [44] | Indicates good apheresis response |
| Female | [37,91] | Indicates good apheresis response | |
| Histological classification and localization | Gadolinium positive MRI lesions | [43] | Indicates good apheresis response |
| Histological type 1 and 2 pattern | [34] | Indicates good apheresis response | |
| Histological type 3 pattern | [34] | Indicates poor apheresis response | |
| Pre-treatment | No disease modifying drugs | [43] | Indicates good apheresis response |
| Short duration of disease | [41] | Indicates good apheresis response | |
| “Neuromyelitis Optica” | |||
| Classification | Predictor | Citation | Meaning |
| Histological classification and localization | Isolated myelitis | [85] | Indicates good apheresis response |
| Laboratory values | Anti-aquaporin-4 IgG positive | [12] | Indicates good apheresis response |
| “Mixed” | |||
| Classification | Predictor | Citation | Meaning |
| Apheresis | Early initiation | [44,60,80,88] | Indicates good apheresis response |
| Clinical signs and symptoms | Lower baseline scores on the EDSS, visual outcome, and gait scales | [94] * | Indicates good apheresis response |
| Pre-treatment | Cumulative corticosteroid doses | [44] | Irrelevant for apheresis response |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipphardt, M.; Wallbach, M.; Koziolek, M.J. Plasma Exchange or Immunoadsorption in Demyelinating Diseases: A Meta-Analysis. J. Clin. Med. 2020, 9, 1597. https://doi.org/10.3390/jcm9051597
Lipphardt M, Wallbach M, Koziolek MJ. Plasma Exchange or Immunoadsorption in Demyelinating Diseases: A Meta-Analysis. Journal of Clinical Medicine. 2020; 9(5):1597. https://doi.org/10.3390/jcm9051597
Chicago/Turabian StyleLipphardt, Mark, Manuel Wallbach, and Michael J. Koziolek. 2020. "Plasma Exchange or Immunoadsorption in Demyelinating Diseases: A Meta-Analysis" Journal of Clinical Medicine 9, no. 5: 1597. https://doi.org/10.3390/jcm9051597
APA StyleLipphardt, M., Wallbach, M., & Koziolek, M. J. (2020). Plasma Exchange or Immunoadsorption in Demyelinating Diseases: A Meta-Analysis. Journal of Clinical Medicine, 9(5), 1597. https://doi.org/10.3390/jcm9051597