Outcome of Root Canal Treatments Provided by Endodontic Postgraduate Students. A Retrospective Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Methodology
2.1. Experimental Procedure
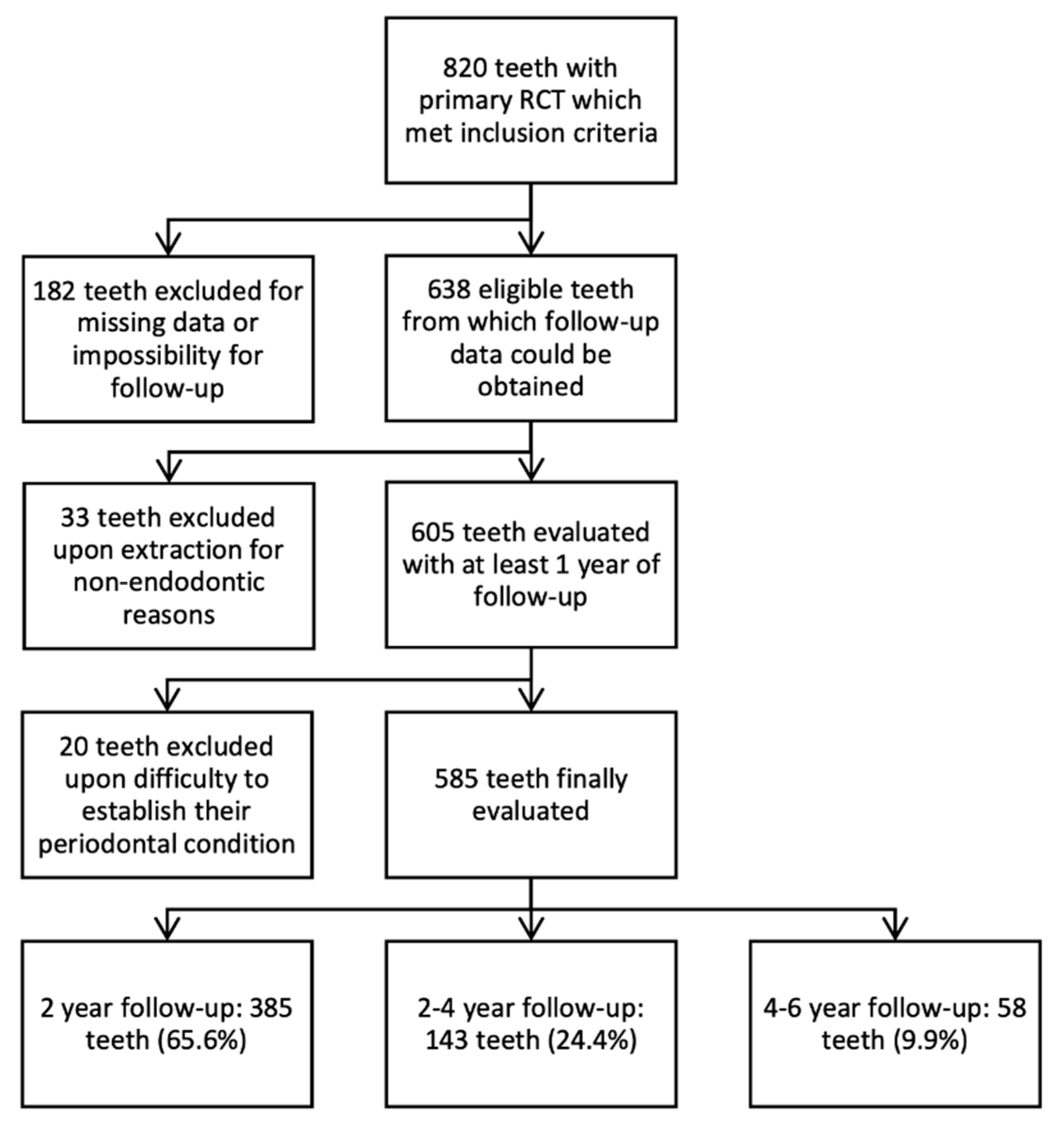
2.2. Clinical Follow-Up Evaluation
2.3. Healing Criteria
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Influence of Preoperative Factors on Periapical Lesion Healing
4.2. Influence of Intraoperative Factors on Periapical Lesion Healing
4.3. Influence of Postoperative Factors on Periapical Lesion Healing
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Figdor, D. Apical periodontitis: A very prevalent problem. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 94, 651–652. [Google Scholar] [CrossRef] [Green Version]
- Marending, M.; Peters, O.A.; Zehnder, M. Factors affecting the outcome of orthograde root canal therapy in a general dentistry hospital practice. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 99, 119–124. [Google Scholar] [CrossRef]
- Burry, J.C.; Stover, S.; Eichmiller, F.; Bhagavatula, P. Outcomes of Primary Endodontic Therapy Provided by Endodontic Specialists Compared with Other Providers. J. Endod. 2016, 42, 702–705. [Google Scholar] [CrossRef] [Green Version]
- Estrela, C.; Holland, R.; Estrela, C.R.D.A.; Alencar, A.H.G.; Sousa-Neto, M.D.; Pécora, J.D. Characterization of Successful Root Canal Treatment. Braz. Dent. J. 2014, 25, 3–11. [Google Scholar] [CrossRef]
- ESE. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef]
- Ricucci, D.; Russo, J.; Rutberg, M.; Burleson, J.A.; Spångberg, L.S. A prospective cohort study of endodontic treatments of 1369 root canals: Results after 5 years. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, 825–842. [Google Scholar] [CrossRef] [PubMed]
- Landys Borén, D.; Jonasson, P.; Kvist, T. Long-term Survival of Endodontically Treated Teeth at a Public Dental Specialist Clinic. J. Endod. 2015, 41, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 1. Effects of study characteristics on probability of success. Int. Endod. J. 2007, 40, 921–939. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 2007, 41, 6–31. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.-L.; Mann, V.; Gulabivala, K. Outcome of secondary root canal treatment: A systematic review of the literature. Int. Endod. J. 2008, 41, 1026–1046. [Google Scholar] [CrossRef]
- Ng, Y.-L.; Mann, V.; Gulabivala, K. Tooth survival following non-surgical root canal treatment: A systematic review of the literature. Int. Endod. J. 2010, 43, 171–189. [Google Scholar] [CrossRef] [PubMed]
- Fleming, C.H.; Litaker, M.S.; Alley, L.W.; Eleazer, P.D. Comparison of Classic Endodontic Techniques versus Contemporary Techniques on Endodontic Treatment Success. Endod. J. 2010, 36, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Khatri, R.K.; Khullar, P. A Survey Report on Effect of Root Canal Fillings and Coronal Restorations on the Periapical Status of Endodontically Treated Teeth in a Selected Group of Population. Int. J. Clin. Pediatr. Dent. 2013, 6, 89–94. [Google Scholar] [CrossRef]
- Craveiro, M.A.; Fontana, C.E.; de Martin, A.S.; Bueno, C.E.D.S. Influence of Coronal Restoration and Root Canal Filling Quality on Periapical Status: Clinical and Radiographic Evaluation. Endod. J. 2015, 41, 836–840. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Wolf, E.; Tegelberg, Å.; Petersson, K. Effect of education intervention on the quality and long-term outcomes of root canal treatment in general practice. Int. Endod. J. 2015, 48, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Karabucak, B.; Bunes, A.; Chehoud, C.; Kohli, M.R.; Setzer, F. Prevalence of Apical Periodontitis in Endodontically Treated Premolars and Molars with Untreated Canal: A Cone-beam Computed Tomography Study. Endod. J. 2016, 42, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Cakici, E.; Yildirim, E.; Cakici, F.; Erdogan, A. Assessment of periapical health, quality of root canal filling, and coronal restoration by using cone-beam computed tomography. Niger. J. Clin. Pract. 2016, 19, 673. [Google Scholar] [CrossRef]
- Chala, S.; Abouqal, R.; Abdallaoui, F. Prevalence of apical periodontitis and factors associated with the periradicular status. Acta Odontol. Scand. 2011, 69, 355–359. [Google Scholar] [CrossRef]
- Skupien, J.A.; Opdam, N.; Winnen, R.; Bronkhorst, E.; Kreulen, C.; Pereira-Cenci, T.; Huysmans, M.C. A Practice-based Study on the Survival of Restored Endodontically Treated Teeth. Endod. J. 2013, 39, 1335–1340. [Google Scholar] [CrossRef]
- Pirani, C.; Chersoni, S.; Montebugnoli, L.; Prati, C. Long-term outcome of non-surgical root canal treatment: A retrospective analysis. Odontology 2015, 103, 185–193. [Google Scholar] [CrossRef]
- Eyuboglu, T.F.; Olcay, K.; Özcan, M. A clinical study on single-visit root canal retreatments on consecutive 173 patients: Frequency of periapical complications and clinical success rate. Clin. Oral Investig. 2017, 21, 1761–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berrezouga, L.; Bouguezzi, A.; Belkhir, M.S. Outcome of Initial Endodontic Treatment Performed, by One Specialist, in 122 Tunisian Patients: A Retrospective Study. Int. J. Dent. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, E.; Vehkalahti, M.M.; Kotiranta, A.K. Impact of systemic diseases and tooth-based factors on outcome of root canal treatment. Int. Endod. J. 2019, 52, 1417–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restrepo-Restrepo, F.A.; Cañas-Jiménez, S.J.; Romero-Albarracín, R.D.; Villa-Machado, P.A.; Pérez-Cano, M.I.; Tobón-Arroyave, S.I. Prognosis of root canal treatment in teeth with preoperative apical periodontitis: A study with cone-beam computed tomography and digital periapical radiography. Int. Endod. J. 2019, 52, 1533–1546. [Google Scholar] [CrossRef]
- Blome, C.; Augustin, M. Measuring Change in Quality of Life: Bias in Prospective and Retrospective Evaluation. Value Health 2015, 18, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.-K.; Shemesh, H.; Wesselink, P.R. Limitations of previously published systematic reviews evaluating the outcome of endodontic treatment. Int. Endod. J. 2009, 42, 656–666. [Google Scholar] [CrossRef]
- Torabinejad, M.; Rice, D.D.; Maktabi, O.; Oyoyo, U.; Abramovitch, K. Prevalence and Size of Periapical Radiolucencies Using Cone-beam Computed Tomography in Teeth without Apparent Intraoral Radiographic Lesions: A New Periapical Index with a Clinical Recommendation. Endod. J. 2018, 44, 389–394. [Google Scholar] [CrossRef]
- Pak, J.G.; Fayazi, S.; White, S.N. Prevalence of Periapical Radiolucency and Root Canal Treatment: A Systematic Review of Cross-sectional Studies. Endod. J. 2012, 38, 1170–1176. [Google Scholar] [CrossRef]
- Castelot-Enkel, B.; Nguyen, J.M.; Armengol, V.; Volteau, C.; Laboux, O.; Lombrail, P.; Weiss, P. A recall program for the outcome of conventional root canal treatment performed in a teaching hospital. Acta Odontol. Scand. 2013, 71, 1399–1409. [Google Scholar] [CrossRef]
- Zhang, M.M.; Liang, Y.H.; Gao, X.J.; Jiang, L.; van der Sluis, L.; Wu, M.K. Management of Apical Periodontitis: Healing of Post-treatment Periapical Lesions Present 1 Year after Endodontic Treatment. Endod. J. 2015, 41, 1020–1025. [Google Scholar] [CrossRef]
- Aminoshariae, A.; Kulild, J.C.; Syed, A. Cone-beam Computed Tomography Compared with Intraoral Radiographic Lesions in Endodontic Outcome Studies: A Systematic Review. Endod. J. 2018, 44, 1626–1631. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shakiba, B.; Hamedy, R.; Pak, J.G.; Barbizam, J.V.; Ogawa, R.; White, S.N. Influence of increased patient age on longitudinal outcomes of root canal treatment: A systematic review. Gerodontology 2017, 34, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Marquis, V.L.; Dao, T.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment Outcome in Endodontics: The Toronto Study. Phase III: Initial Treatment. Endod. J. 2006, 32, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Vengerfeldt, V.; Mändar, R.; Nguyen, M.S.; Saukas, S.; Saag, M. Apical periodontitis in southern Estonian population: Prevalence and associations with quality of root canal fillings and coronal restorations. BMC Oral Health 2017, 17, 147. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Pinzón, A.; Segura-Egea, J.J.; Poyato-Ferrera, M.; Velasco-Ortega, E.; Rios-Santos, J.V. Prevalence of apical periodontitis and frequency of root-filled teeth in an adult Spanish population. Int. Endod. J. 2004, 37, 167–173. [Google Scholar] [CrossRef]
- Aminoshariae, A.; Kulild, J.C.; Mickel, A.; Fouad, A.F. Association between Systemic Diseases and Endodontic Outcome: A Systematic Review. Endod. J. 2017, 43, 514–519. [Google Scholar] [CrossRef]
- Ng, Y.-L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: Part 2: Tooth survival. Int. Endod. J. 2011, 44, 610–625. [Google Scholar] [CrossRef]
- Segura-Egea, J.J.; Martín-González, J.; Cabanillas-Balsera, D.; Fouad, A.F.; Velasco-Ortega, E.; López-López, J. Association between diabetes and the prevalence of radiolucent periapical lesions in root-filled teeth: Systematic review and meta-analysis. Clin. Oral Investig. 2016, 20, 1133–1141. [Google Scholar] [CrossRef]
- Friedman, S.; Abitbol, S.; Lawrence, H.P. Treatment outcome in endodontics: The Toronto study. Phase 1: Initial treatment. Endod. J. 2003, 29, 787–793. [Google Scholar] [CrossRef]
- de Chevigny, C.; Dao, T.T.; Basrani, B.R.; Marquis, V.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment Outcome in Endodontics: The Toronto Study—Phase 4: Initial Treatment. Endod. J. 2008, 34, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, A. The Factors Responsible for Endodontic Treatment Failure in the Permanent Dentitions of the Patients Reported to the College of Dentistry, the University of Aljouf, Kingdom of Saudi Arabia. J. Clin. Diagn. Res. 2016, 10, ZC146. [Google Scholar] [CrossRef] [PubMed]
- Fernández, R.; Cardona, J.A.; Cadavid, D.; Álvarez, L.G.; Restrepo, F.A. Survival of Endodontically Treated Roots/Teeth Based on Periapical Health and Retention: A 10-year Retrospective Cohort Study. Endod. J. 2017, 43, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Kojima, K.; Inamoto, K.; Nagamatsu, K.; Hara, A.; Nakata, K.; Morita, I.; Nakagaki, H.; Nakamura, H. Success rate of endodontic treatment of teeth with vital and nonvital pulps. A meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 97, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.-L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: Part 1: Periapical health. Int. Endod. J. 2011, 44, 583–609. [Google Scholar] [CrossRef]
- Hamasha, A.A.; Hatiwsh, A. Quality of life and satisfaction of patients after nonsurgical primary root canal treatment provided by undergraduate students, graduate students and endodontic specialists. Int. Endod. J. 2013, 46, 1131–1139. [Google Scholar] [CrossRef]
- Manfredi, M.; Figini, L.; Gagliani, M.; Lodi, G. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef]
- Paredes-Vieyra, J.; Enriquez, F.J.J. Success Rate of Single- versus Two-visit Root Canal Treatment of Teeth with Apical Periodontitis: A Randomized Controlled Trial. Endod. J. 2012, 38, 1164–1169. [Google Scholar] [CrossRef]
- Moreira, M.S.; Anuar AS, N.S.; Tedesco, T.K.; dos Santos, M.; Morimoto, S. Endodontic Treatment in Single and Multiple Visits: An Overview of Systematic Reviews. Endod. J. 2017, 43, 864–870. [Google Scholar] [CrossRef]
- Chugal, N.M.; Clive, J.M.; Spångberg, L.S.W. A prognostic model for assessment of the outcome of endodontic treatment: Effect of biologic and diagnostic variables. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 91, 342–352. [Google Scholar] [CrossRef]
- Connert, T.; Truckenmüller, M.; ElAyouti, A.; Eggmann, F.; Krastl, G.; Löst, C.; Weiger, R. Changes in periapical status, quality of root fillings and estimated endodontic treatment need in a similar urban German population 20 years later. Clin. Oral Investig. 2019, 23, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- Gündüz, K.; Avsever, H.; Orhan, K.; Demirkaya, K. Cross-sectional evaluation of the periapical status as related to quality of root canal fillings and coronal restorations in a rural adult male population of Turkey. BMC Oral Health 2011, 11, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connert, T.; Truckenmüller, M.; ElAyouti, A.; Eggmann, F.; Krastl, G.; Löst, C.; Weiger, R. Impact of the Quality of Coronal Restoration versus the Quality of Root Canal Fillings on Success of Root Canal Treatment: A Systematic Review and Meta-analysis. Endod. J. 2011, 37, 895–902. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Preoperative Factors | Teeth with RCT | Complete Healing | p |
|---|---|---|---|
| Men | 252 (43.1%) | 234 (92.9%) | 0.06 |
| Women | 333 (56.9%) | 298 (88.9%) | |
| Anterior teeth and premolars | 256 (43.8%) | 227 (88.7%) | 0.06 |
| First molars | 178 (30.4%) | 158 (88.8%) | |
| Second and third molars | 151 (25.8%) | 145 (96%) | |
| ASA I | 413 (70.6%) | 382 (92.5%) | 0.01 |
| ASA II | 172 (29.4% | 148 (86%) | |
| Vital teeth | 365 (62.3%) | 349 (95.6%) | 0.00 |
| Non-vital teeth | 220 (37.7%) | 181 (82.3%) | |
| Absence of periapical radiolucency | 348 (59.5) | 339 (97.4%) | 0.00 |
| Periapical radiolucency (1–4 mm) | 203 (34.7%) | 175 (86.2%) | |
| Periapical radiolucency (>4 mm) | 34 (5.8%) | 16 (47.1%) | |
| No walls lost | 216 (36.9%) | 195 (90.3%) | 0.96 |
| One wall lost | 222 (37.9%) | 201 (90.5% | |
| Two or more walls lost | 147 (25.1%) | 134 (91.2% | |
| Absence of pain | 218(37.3%) | 190 (87.2%) | 0.04 |
| Prolonged spontaneous or stimuli-induced pain | 367 (62.2%) | 208 (94.1%) | |
| Pain upon percussion | 146 (24.9%) | 132 (90.4) | |
| Treatment cause: caries, pain, or inflammation | 499 (85.3%) | 463 (92.8%) | 0.00 |
| Other causes | 86 (14.7%) | 67 (77.9%) | |
| No inflammatory abscess or sinus tract | 484 (82.7%) | 443 (91.5) | 0.07 |
| Inflammation, abscess, or sinus tract | 101 (17.3) | 87 (86.1%) | |
| <4 mm probing depth | 480 (82.1%) | 446 (92.9%) | 0.00 |
| >4 mm probing depth | 105 (17.9%) | 84 (80%) | |
| Absence of mobility | 523 (89.4%) | 480 (91.8%) | 0.00 |
| Slight mobility | 62 (10.6%) | 50 (80.6%) |
| Intraoperative Factors | Teeth with RCT | Complete Healing | p |
| Manual instrumentation | 118 (20.2%) | 103 (87.3%) | 0.11 |
| Rotatory instrumentation | 467 (79.8%) | 427 (91.4%) | |
| Filling to 0–2 mm of the radiographic apex | 410 (70.1%) | 373 (91%) | 0.36 |
| Infra/over filling | 175 (29.9%) | 157 (89.7%) | |
| One to two treatment sessions | 471 (80.5%) | 429 (91.1% | 0.25 |
| More than two treatment sessions | 114 (19.5%) | 101 (88.6%) | |
| No intraoperative complications | 545 (93.2%) | 493 (90.5%) | 0.48 |
| Intraoperative complications | 40 (6.8%) | 37 (92.5%) | |
| Postoperative Factors | Teeth with RCT | Complete Healing | p |
| Direct composite restoration | 493 (84.3%) | 459 (93.1%) | 0.00 |
| Crown | 44 (7.5%) | 33 (75.1%) | |
| Prosthetic bridge | 48 (8.2%) | 38 (79.2%) | |
| Presence of antagonist tooth | 524 (89.6%) | 474 (90.5%) | 0.47 |
| Absence of antagonist tooth | 61 (10.4%) | 56 (91.8%) | |
| Favorable restoration condition at follow-up | 551 (94.2%) | 507 (92%) | 0.00 |
| Maladjusted or leaked restoration | 34 (5.8%) | 23 (67.6%) | |
| 1–2 years follow-up | 350 (91.1%) | 350 (91.1%) | 0.48 |
| >2–4 years follow-up | 130 (90.9%) | 130 (90.9%) | |
| >4–6 years follow-up | 50 (86.2%) | 50 (86.2%) |
| Follow-Up Factors | Teeth with RCT |
|---|---|
| Absence of pain | 568 (97%) |
| Spontaneous pain upon percussion, palpation, or mastication | 17 (3%) |
| No inflammatory abscess or sinus tract | 582 (99.5%) |
| Inflammation, abscess, or sinus tract | 3 (0.5%) |
| <4 mm probing depth | 572 (97.8%) |
| >4 mm probing depth | 13 (2.2%) |
| Absence of mobility | 537 (91.8%) |
| Slight mobility | 48 (8.2%) |
| Absence of periapical radiolucency | 530 (90.6%) |
| Presence of periapical radiolucency with minor or no reduction in size | 39 (6.7%) |
| Presence of periapical radiolucency with an increased size | 7 (1.2%) |
| Presence of a new periapical lesion | 9 (1.5%) |
| Favorable restoration condition at follow-up | 551 (94.2%) |
| Maladjusted or leaked restoration | 34 (5.8%) |
| 95% C.I. for EXP(B) | ||||||||
|---|---|---|---|---|---|---|---|---|
| B | SE | Wald | Gl | Sig. | Exp(B) | Inferior | Superior | |
| Absence of periapical radiolucency | 52.062 | 2 | 0.000 | |||||
| 1–4 mm periapical radiolucency | −3.766 | 0.522 | 52.052 | 1 | 0.000 | 0.023 | 0.008 | 0.064 |
| >4 mm periapical radiolucency | −2.167 | 0.456 | 22.557 | 1 | 0.000 | 0.115 | 0.047 | 0.280 |
| <4 mm probing depth | −1.270 | 0.371 | 11.681 | 1 | 0.001 | 0.281 | 0.136 | 0.582 |
| Treatment cause: caries, pain, abscess, or sinus tract | −0.839 | 0.411 | 4.172 | 1 | 0.041 | 0.432 | 0.193 | 0.967 |
| Direct composite restoration | 8.616 | 2 | 0.013 | |||||
| Crown | −1.060 | 0.500 | 4.496 | 1 | 0.034 | 0.346 | 0.130 | 0.923 |
| Prosthetic bridge | 0.164 | 0.654 | 0.063 | 1 | 0.802 | 1.178 | 0.327 | 4.242 |
| Favorable restoration condition at follow-up | −1.942 | 0.505 | 14.806 | 1 | 0.000 | 0.143 | 0.053 | 0.386 |
| Constant | 4.348 | 0.908 | 22.950 | 1 | 0.000 | 77.315 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llena, C.; Nicolescu, T.; Perez, S.; Gonzalez de Pereda, S.; Gonzalez, A.; Alarcon, I.; Monzo, A.; Sanz, J.L.; Melo, M.; Forner, L. Outcome of Root Canal Treatments Provided by Endodontic Postgraduate Students. A Retrospective Study. J. Clin. Med. 2020, 9, 1994. https://doi.org/10.3390/jcm9061994
Llena C, Nicolescu T, Perez S, Gonzalez de Pereda S, Gonzalez A, Alarcon I, Monzo A, Sanz JL, Melo M, Forner L. Outcome of Root Canal Treatments Provided by Endodontic Postgraduate Students. A Retrospective Study. Journal of Clinical Medicine. 2020; 9(6):1994. https://doi.org/10.3390/jcm9061994
Chicago/Turabian StyleLlena, Carmen, Teodora Nicolescu, Salvadora Perez, Silvia Gonzalez de Pereda, Ana Gonzalez, Iris Alarcon, Angela Monzo, José Luis Sanz, Maria Melo, and Leopoldo Forner. 2020. "Outcome of Root Canal Treatments Provided by Endodontic Postgraduate Students. A Retrospective Study" Journal of Clinical Medicine 9, no. 6: 1994. https://doi.org/10.3390/jcm9061994
APA StyleLlena, C., Nicolescu, T., Perez, S., Gonzalez de Pereda, S., Gonzalez, A., Alarcon, I., Monzo, A., Sanz, J. L., Melo, M., & Forner, L. (2020). Outcome of Root Canal Treatments Provided by Endodontic Postgraduate Students. A Retrospective Study. Journal of Clinical Medicine, 9(6), 1994. https://doi.org/10.3390/jcm9061994