Association of Lower Plasma Homoarginine Concentrations with Greater Risk of All-Cause Mortality in the Community: The Framingham Offspring Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Biomarkers
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Correlates of Circulating Homoarginine
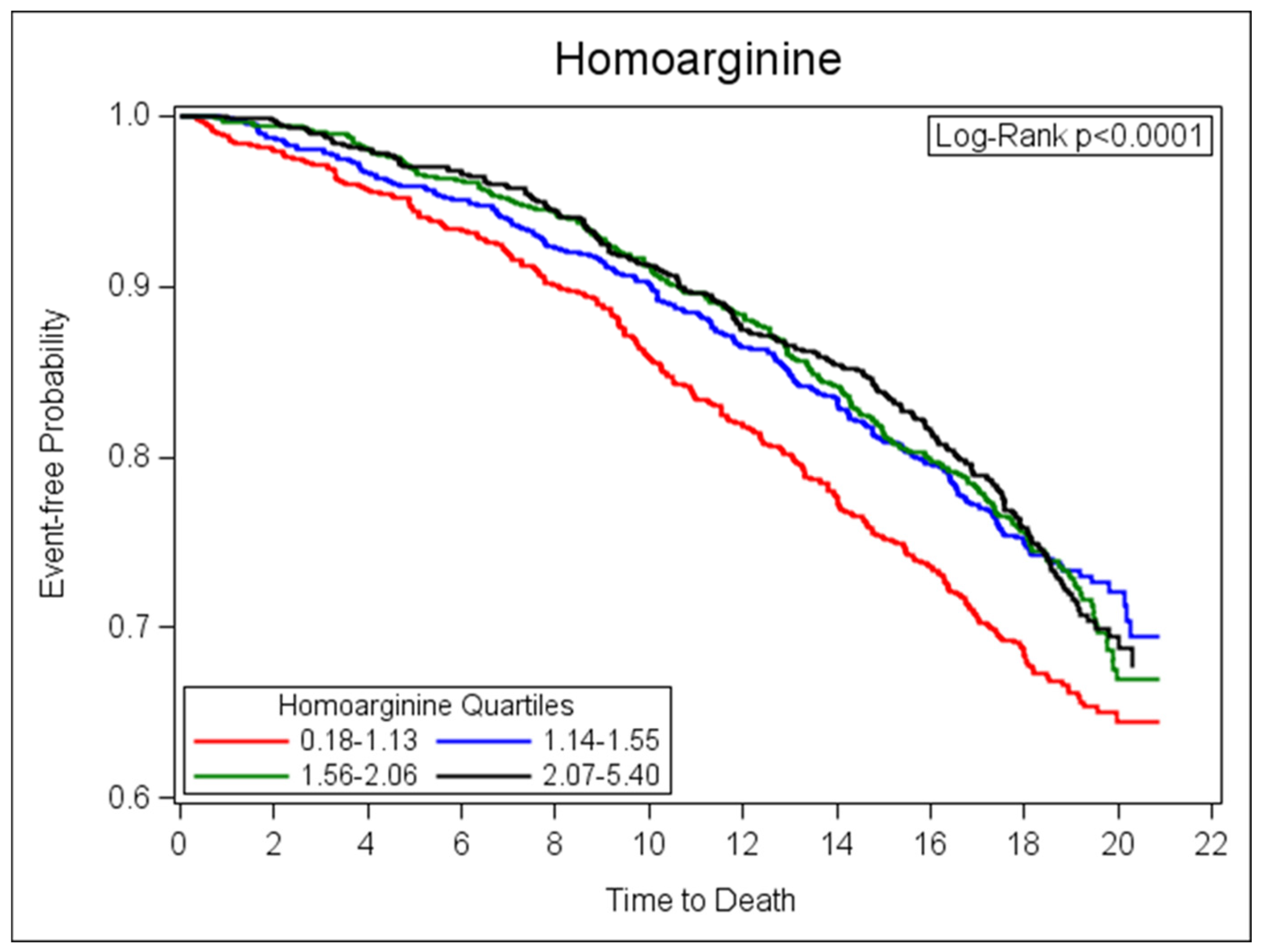
3.2. Relations of Homoarginine and All-Cause Mortality
3.3. Relations of Homoarginine and Incident CVD
4. Discussion
4.1. Homoarginine in the Community
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Karetnikova, E.S.; Jarzebska, N.; Markov, A.G.; Weiss, N.; Lentz, S.R.; Rodionov, R.N. Is Homoarginine a Protective Cardiovascular Risk Factor? Arterioscler. Thromb. Vasc. Biol. 2019, 39, 869–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinellu, A.; Paliogiannis, P.; Carru, C.; Mangoni, A.A. Homoarginine and All-Cause Mortality: A Systematic Review and Meta-Analysis. Eur. J. Clin. Invest. 2018, 48, e12960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choe, C.U.; Atzler, D.; Wild, P.S.; Carter, A.M.; Böger, R.H.; Ojeda, F.; Simova, O.; Stockebrand, M.; Lackner, K.; Nabuurs, C.; et al. Homoarginine levels are regulated by L-arginine: Glycine amidinotransferase and affect stroke outcome: Results from human and murine studies. Circulation 2013, 128, 1451–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atzler, D.; Baum, C.; Ojeda, F.; Keller, T.; Cordts, K.; Schnabel, R.B.; Choe, C.U.; Lackner, K.J.; Münzel, T.; Böger, R.H.; et al. Low Homoarginine Levels in the Prognosis of Patients With Acute Chest Pain. J. Am. Heart Assoc. 2016, 5, e002565. [Google Scholar] [CrossRef] [Green Version]
- Atzler, D.; Rosenberg, M.; Anderssohn, M.; Choe, C.U.; Lutz, M.; Zugck, C.; Böger, R.H.; Frey, N.; Schwedhelm, E. Homoarginine—An independent marker of mortality in heart failure. Int. J. Cardiol. 2013, 168, 4907–4909. [Google Scholar] [CrossRef]
- Atzler, D.; McAndrew, D.J.; Cordts, K.; Schneider, J.E.; Zervou, S.; Schwedhelm, E.; Neubauer, S.; Lygate, C.A. Dietary Supplementation with Homoarginine Preserves Cardiac Function in a Murine Model of Post-Myocardial Infarction Heart Failure. Circulation 2017, 135, 400–402. [Google Scholar] [CrossRef]
- Ryan, W.L.; Wells, I.C. Homocitrulline and homoarginine synthesis from lysine. Science 1964, 144, 1122–1127. [Google Scholar] [CrossRef]
- Davids, M.; Ndika, J.D.; Salomons, G.S.; Blom, H.J.; Teerlink, T. Promiscuous activity of arginine: Glycine amidinotransferase is responsible for the synthesis of the novel cardiovascular risk factor homoarginine. FEBS Lett. 2012, 586, 3653–3657. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Chen, L.; Deng, Z.; Zhao, C. Characterization of AmtA, an amidinotransferase involved in the biosynthesis of phaseolotoxins. FEBS Open Bio. 2016, 6, 603–609. [Google Scholar] [CrossRef] [Green Version]
- Kleber, M.E.; Seppälä, I.; Pilz, S.; Hoffmann, M.M.; Tomaschitz, A.; Oksala, N.; Raitoharju, E.; Lyytikäinen, L.P.; Mäkelä, K.M.; Laaksonen, R.; et al. Genome-wide association study identifies 3 genomic loci significantly associated with serum levels of homoarginine: The AtheroRemo Consortium. Circ. Cardiovasc. Genet. 2013, 6, 505–513. [Google Scholar] [CrossRef]
- Choe, C.U.; Nabuurs, C.; Stockebrand, M.C.; Neu, A.; Nunes, P.; Morellini, F.; Sauter, K.; Schillemeit, S.; Hermans-Borgmeyer, I.; Marescau, B.; et al. L-arginine: Glycine amidinotransferase deficiency protects from metabolic syndrome. Hum. Mol. Genet. 2013, 22, 110–123. [Google Scholar] [CrossRef] [Green Version]
- Atzler, D.; Mieth, M.; Maas, R.; Böger, R.H.; Schwedhelm, E. Stable isotope dilution assay for liquid chromatography-tandem mass spectrometric determination of L-homoarginine in human plasma. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2011, 879, 2294–2298. [Google Scholar] [CrossRef]
- Rao, S.L.; Ramachandran, L.K.; Adiga, P.R. The isolation and characterization of l-homoarginine from seeds of Lathyrus sativus. Biochemistry 1963, 2, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Bell, E.A. The isolation of L-homoarginine from seeds of Lathyrus cicera. Biochem. J. 1962, 85, 91–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schönhoff, M.; Weineck, G.; Hoppe, J.; Hornig, S.; Cordts, K.; Atzler, D.; Gerloff, C.; Böger, R.; Neu, A.; Schwedhelm, E.; et al. Cognitive performance of 20 healthy humans supplemented with L-homoarginine for 4 weeks. J. Clin. Neurosci. 2018, 50, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Atzler, D.; Schönhoff, M.; Cordts, K.; Ortland, I.; Hoppe, J.; Hummel, F.C.; Gerloff, C.; Jaehde, U.; Jagodzinski, A.; Böger, R.H.; et al. Oral supplementation with L-homoarginine in young volunteers. Br. J. Clin. Pharmacol. 2016, 82, 1477–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tommasi, S.; Elliot, D.J.; Da Boit, M.; Gray, S.R.; Lewis, B.C.; Mangoni, A.A. Homoarginine and inhibition of human arginase activity: Kinetic characterization and biological relevance. Sci. Rep. 2018, 8, 3697. [Google Scholar] [CrossRef] [PubMed]
- Franceschelli, S.; Ferrone, A.; Pesce, M.; Riccioni, G.; Speranza, L. Biological functional relevance of asymmetric dimethylarginine (ADMA) in cardiovascular disease. Int. J. Mol. Sci. 2013, 14, 24412–24421. [Google Scholar] [CrossRef] [Green Version]
- Valtonen, P.; Laitinen, T.; Lyyra-Laitinen, T.; Raitakari, O.T.; Juonala, M.; Viikari, J.S.; Heiskanen, N.; Vanninen, E.; Punnonen, K.; Heinonen, S. Serum L-homoarginine concentration is elevated during normal pregnancy and is related to flow-mediated vasodilatation. Circ. J. 2008, 72, 1879–1884. [Google Scholar] [CrossRef] [Green Version]
- Radomski, M.W.; Palmer, R.M.; Moncada, S. An L-arginine/nitric oxide pathway present in human platelets regulates aggregation. Proc. Natl. Acad. Sci. USA 1990, 87, 5193–5197. [Google Scholar] [CrossRef] [Green Version]
- Böger, R.H.; Sullivan, L.M.; Schwedhelm, E.; Wang, T.J.; Maas, R.; Benjamin, E.J.; Schulze, F.; Xanthakis, V.; Benndorf, R.A.; Vasan, R.S. Plasma asymmetric dimethylarginine and incidence of cardiovascular disease and death in the community. Circulation 2009, 119, 1592–1600. [Google Scholar] [CrossRef]
- Kannel, W.B.; Feinleib, M.; McNamara, P.M.; Garrison, R.J.; Castelli, W.P. An investigation of coronary heart disease in families. The Framingham offspring study. Am. J. Epidemiol. 1979, 110, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Wollert, K.C.; Larson, M.G.; Coglianese, E.; McCabe, E.L.; Cheng, S.; Ho, J.E.; Fradley, M.G.; Ghorbani, A.; Xanthakis, V.; et al. Prognostic utility of novel biomarkers of cardiovascular stress: The Framingham Heart Study. Circulation 2012, 126, 1596–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunkler, D.; Ploner, M.; Schemper, M.; Heinze, G. Weighted Cox regression using the R package coxphw. J. Stat. Soft. 2018, 84, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Atzler, D.; Appelbaum, S.; Cordts, K.; Ojeda, F.M.; Wild, P.S.; Münzel, T.; Blankenberg, S.; Böger, R.H.; Blettner, M.; Beutel, M.E.; et al. Reference intervals of plasma homoarginine from the German Gutenberg Health Study. Clin. Chem. Lab. Med. 2016, 54, 1231–1237. [Google Scholar] [CrossRef]
- Pilz, S.; Teerlink, T.; Scheffer, P.G.; Meinitzer, A.; Rutters, F.; Tomaschitz, A.; Drechsler, C.; Kienreich, K.; Nijpels, G.; Stehouwer, C.D.; et al. Homoarginine and mortality in an older population: The Hoorn study. Eur. J. Clin. Invest. 2014, 44, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Faller, K.M.E.; Atzler, D.; McAndrew, D.J.; Zervou, S.; Whittington, H.J.; Simon, J.N.; Aksentijevic, D.; Ten Hove, M.; Choe, C.U.; Isbrandt, D.; et al. Impaired cardiac contractile function in arginine: Glycine amidinotransferase knockout mice devoid of creatine is rescued by homoarginine but not creatine. Cardiovasc. Res. 2018, 114, 417–430. [Google Scholar] [CrossRef] [Green Version]
- Atzler, D.; Gore, M.O.; Ayers, C.R.; Choe, C.U.; Böger, R.H.; de Lemos, J.A.; McGuire, D.K.; Schwedhelm, E. Homoarginine and cardiovascular outcome in the population-based Dallas Heart Study. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2501–2507. [Google Scholar] [CrossRef] [Green Version]
- Stockebrand, M.; Sauter, K.; Neu, A.; Isbrandt, D.; Choe, C.U. Differential regulation of AMPK activation in leptin- and creatine-deficient mice. FASEB J. 2013, 27, 4147–4156. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic 1 | Men (N = 1552) | Women (N = 1779) |
|---|---|---|
| Age (yr) | 59 ± 10 | 59 ± 10 |
| Current cigarette smoking (%) | 14 | 16 |
| Total cholesterol (mg/dL) | 199 ± 41 | 212 ± 39 |
| HDL cholesterol (mg/dL) | 43 ± 12 | 58 ± 16 |
| Total/HDL Ratio | 4.9 ± 2.0 | 4.0 ± 1.4 |
| Body Mass Index (kg×m2) | 28.5 ± 4.4 | 27.4 ± 5.7 |
| Systolic Blood Pressure (mmHg) | 130 ± 17 | 127 ± 20 |
| Diastolic Blood Pressure (mmHg) | 77.2 ± 9.5 | 73.8 ± 9.2 |
| Hypertension (%) | 45 | 38 |
| Use of antihypertensive agents (%) | 31 | 25 |
| Blood glucose (mg/dL) | 107 ± 28 | 100 ± 26 |
| Diabetes mellitus (%) | 12 | 8 |
| Serum creatinine (mg/dL) | 1.24 ± 0.19 | 1.07 ± 0.18 |
| eGFR (mL/min/1.73 m2) | 86 ± 18 | 85 ± 19 |
| Prevalent CVD (%) | 15 | 7 |
| Homoarginine (µmol/L) | 1.73 (1.33, 2.23) | 1.38 (1.01, 1.88) |
| ADMA (µmol/L) | 0.54 (0.47, 0.62) | 0.53 (0.46, 0.61) |
| CRP (mg/dL) | 1.8 (0.9, 3.8) | 2.4 (1.0, 5.8) |
| GDF15 (ng/L) | 1058 (822, 1406) | 1021 (811, 1305) |
| BNP (pg/mL) | 6.6 (4.0, 16.8) | 10.0 (4.0, 20.2) |
| Troponin I (pg/mL) | 1.63 (1.05, 2.65) | 1.15 (0.78, 1.91) |
| Variable 1 | Unit of Increase | Regression Coefficient (SE) | p Value |
|---|---|---|---|
| Sex | men vs. women | 0.293 (0.025) | <0.001 |
| Smoking | current vs. not current | −0.195 (0.035) | <0.001 |
| Age | 10 years | −0.051 (0.016) | 0.002 |
| BMI | 1 kg×m2 | 0.013 (0.002) | <0.001 |
| Anti-hypertensive medication use | yes vs. no | 0.069 (0.030) | 0.019 |
| Systolic blood pressure | 10 mm Hg | 0.017 (0.007) | 0.022 |
| eGFR | 1 mL/min | 0.001 (0.001) | 0.063 |
| Outcome | Age- and Sex-Adjusted HR (95% CI) 2 | p Value | Multivariable-Adjusted 1 HR (95% CI) | p Value |
|---|---|---|---|---|
| All-cause mortality | 0.81 (0.72–0.91) | <0.001 | 0.83 (0.74–0.93) | 0.002 |
| Incident CVD | 1.12 (1.00–1.25) | 0.041 | 1.06 (0.95–1.19) | 0.291 |
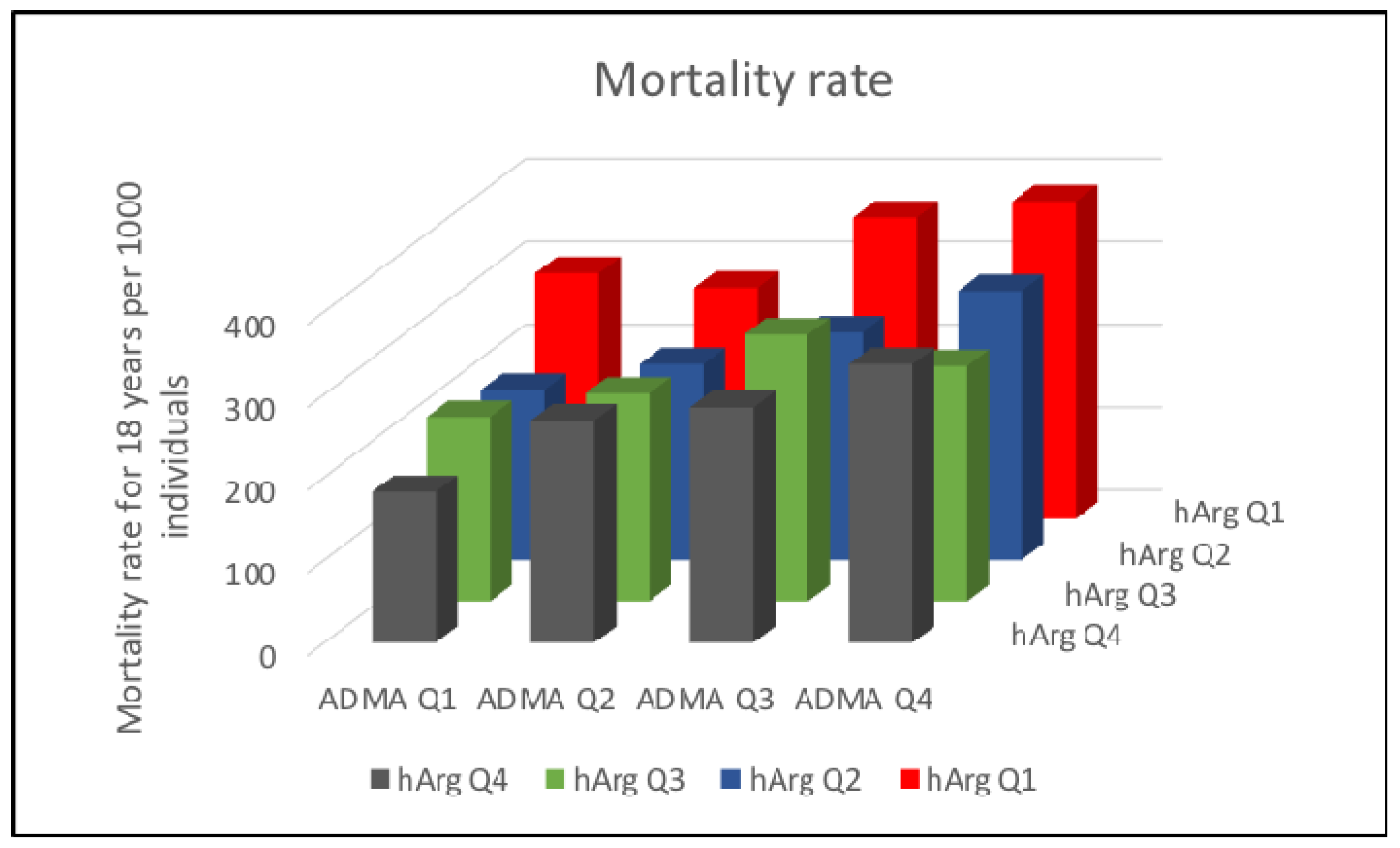
| Cross-Classification Group | Multivariable-Adjusted 1 HR (95% CI) | p Value |
|---|---|---|
| Low Homoarginine and Low ADMA | 1.00 (ref) | |
| Low Homoarginine and High ADMA | 0.97 (0.82, 1.15) | 0.722 |
| High Homoarginine and High ADMA | 0.99 (0.77, 1.28) | 0.958 |
| High Homoarginine and Low ADMA | 0.81 (0.67, 0.98) | 0.028 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwedhelm, E.; Song, R.J.; Vasan, R.S.; van den Heuvel, E.R.; Hannemann, J.; Xanthakis, V.; Böger, R. Association of Lower Plasma Homoarginine Concentrations with Greater Risk of All-Cause Mortality in the Community: The Framingham Offspring Study. J. Clin. Med. 2020, 9, 2016. https://doi.org/10.3390/jcm9062016
Schwedhelm E, Song RJ, Vasan RS, van den Heuvel ER, Hannemann J, Xanthakis V, Böger R. Association of Lower Plasma Homoarginine Concentrations with Greater Risk of All-Cause Mortality in the Community: The Framingham Offspring Study. Journal of Clinical Medicine. 2020; 9(6):2016. https://doi.org/10.3390/jcm9062016
Chicago/Turabian StyleSchwedhelm, Edzard, Rebecca J. Song, Ramachandran S. Vasan, Edwin R. van den Heuvel, Juliane Hannemann, Vanessa Xanthakis, and Rainer Böger. 2020. "Association of Lower Plasma Homoarginine Concentrations with Greater Risk of All-Cause Mortality in the Community: The Framingham Offspring Study" Journal of Clinical Medicine 9, no. 6: 2016. https://doi.org/10.3390/jcm9062016
APA StyleSchwedhelm, E., Song, R. J., Vasan, R. S., van den Heuvel, E. R., Hannemann, J., Xanthakis, V., & Böger, R. (2020). Association of Lower Plasma Homoarginine Concentrations with Greater Risk of All-Cause Mortality in the Community: The Framingham Offspring Study. Journal of Clinical Medicine, 9(6), 2016. https://doi.org/10.3390/jcm9062016