Evaluation of Obesity Management Recorded in Electronic Clinical History: A Cohort Study


Abstract
:1. Introduction
- Improve communication and motivation is essential for adherence to treatment.
- Avoid stigmatization in a health care setting.
- Measure waist circumference.
- Treat comorbidities as a priority to decrease mortality.
- Use a multidisciplinary team: GPs, nurses, dietitians, psychologist.
- Assess weight loss: 5–10% weight loss from initial weight is already sufficient to decreases comorbidities.
- Consider lifestyle behavior change: Nutrition and physical activity. It will also help to improve body image, self-esteem and quality of life.
- Avoid weight cycling: If the patient gains 3–4 kg quickly, he/she should not wait too long before visiting the GPs to be assessed.
2. Methods
3. Results
3.1. Characteristics of the Participants
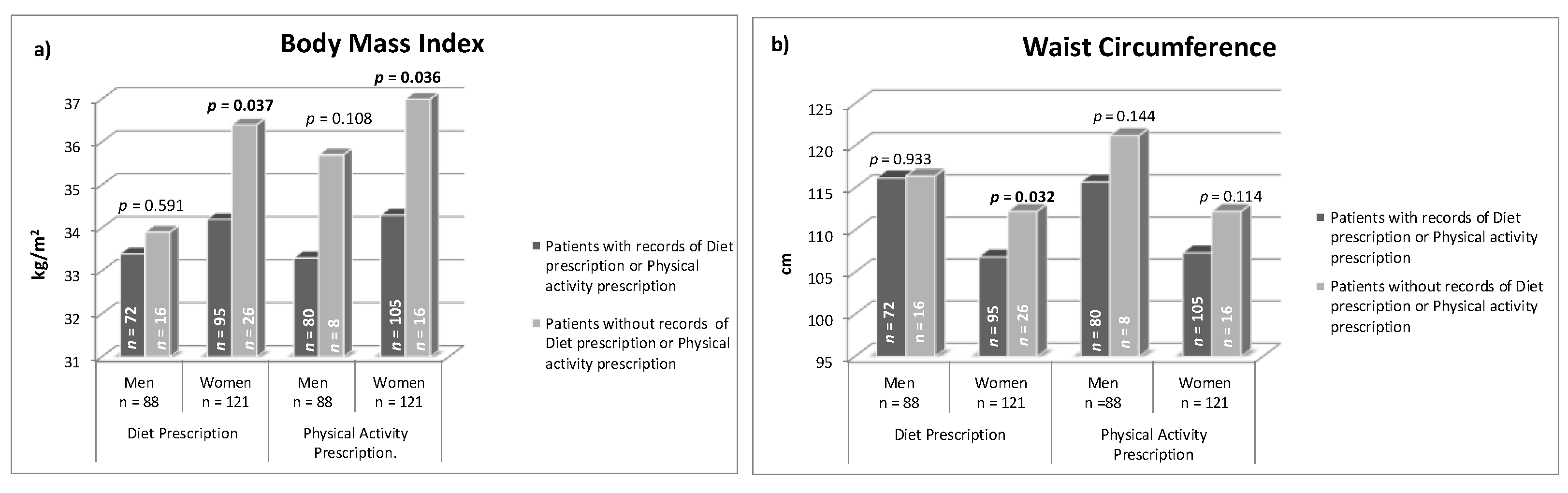
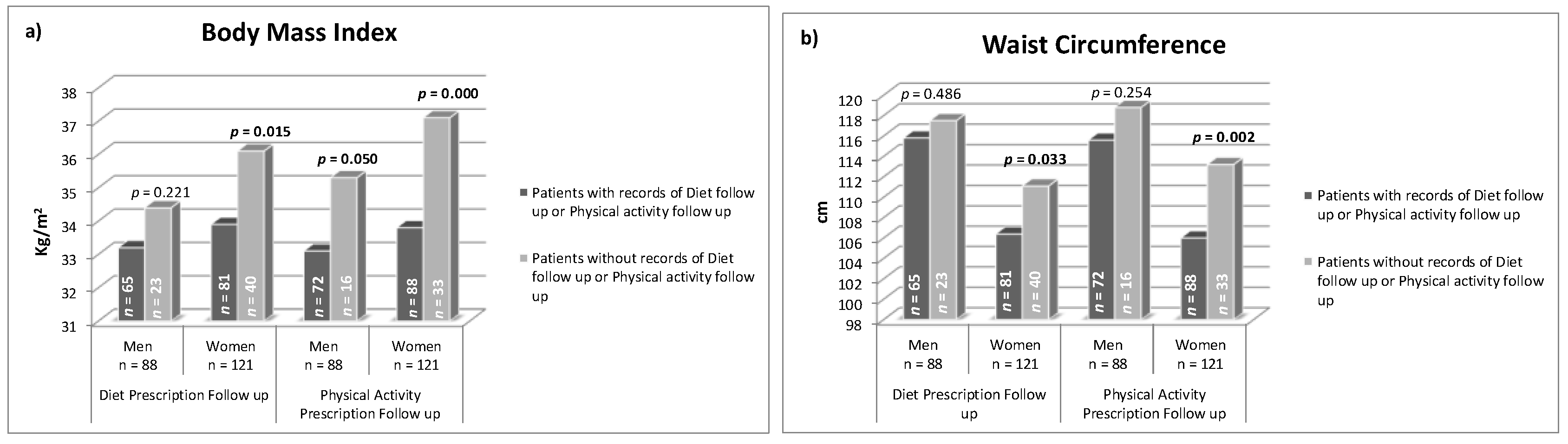
3.2. Treatment Recorded in Clinical History in Relation to the Recommendations of Obesity Guidelines and Patient Adherence to Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). Obesity and Overweight (Factsheet). Available online: www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 12 May 2020).
- World Health Organization (WHO). Implementation Plan to Guide Further Action on the Recommendations Included in the Report of the Commission on Ending Childhood Obesity. Available online: https://www.who.int/end-childhood-obesity/publications/echo-plan-executive-summary/en/ (accessed on 12 May 2020).
- Blundell, J.E.; Baker, J.L.; Boyland, E.; Blaak, E.; Charzewska, J.; de Henauw, S.; Frühbeck, G.; Gonzalez-Gross, M.; Hebebrand, J.; Holm, L.; et al. Variations in the prevalence of obesity among European countries, and a consideration of possible causes. Obes. Facts 2017, 10, 25–37. [Google Scholar] [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity among adults and youth: United States, 2015–2016. NCHS Data Brief 2017, 288, 1–8. [Google Scholar]
- Semlitsch, T.; Stigler, F.L.; Jeitler, K.; Horvath, K.; Siebenhofer, A. Management of overweight and obesity in primary care—A systematic overview of international evidence-based guidelines. Obes. Rev. 2019, 20, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Montani, J.P.; Schutz, Y.; Dulloo, A.G. Review Dieting and weight cycling as risk factors for cardiometabolic diseases: Who is really at risk? Obes. Rev. 2015, 16 (Suppl. 1), 7–18. [Google Scholar] [CrossRef] [Green Version]
- Luca Montesi, L.; Ghoch, M.E.I.; Lucia Brodosi, L.; Simona Calugi, S.; Giulio Marchesini, G.; Riccardo Dalle Grave, R.D. Long-term weight loss maintenance for obesity: A multidisciplinary approach. Diabetol. Metab. Syndr. Obes. 2016, 9, 37–46. [Google Scholar]
- Sharma, A.M.; Padwal, R. Obesity is a sign-over-eating is a symptom: An etiological framework for the assessment and management of obesity. Obes. Rev. 2010, 11, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Rubino, F.; Puhl, R.M.; Cummings, D.E.; Eckel, R.H.; Ryan, D.H.; Mechanick, J.I.; Nadglowski, J.; Salas, X.R.; Schauer, P.R.; Twenefourm, D.; et al. Joint international consensus statement for ending stigma of obesity. Nat. Med. 2020, 26, 485–497. [Google Scholar] [CrossRef] [Green Version]
- Durrer Schutz, D.; Busetto, L.; Dicker, D.; Farpour-Lambert, N.; Pryke, R.; Toplak, H.; Widmer, D.; Yumuk, V.; Schutz, Y. European practical and patient centred guidelines for adult obesity management in primary care. Obes. Facts 2019, 12, 40–66. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Care and Health Excellence. Identification, Assessment and Management of Overweight and Obesity in Children, Young People and Adults (Clinical Guideline 189). 2014. Available online: www.nice.org.uk/guidance/cg189 (accessed on 15 May 2020).
- Kahan, S.I. Practical strategies for engaging individuals with obesity in primary care. Mayo Clin. Proc. 2018, 93, 351–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, H.P.; Prevost, A.T.; Wright, A.J.; Gulliford, M.C. Effectiveness of behavioral weight loss interventions delivered in a primary care setting: A systematic review and meta-analysis. Fam. Pract. 2014, 31, 643–653. [Google Scholar] [CrossRef] [Green Version]
- Johns, D.J.; Hartmann-Boyce, J.; Jebb, S.A.; Aveyard, P. Diet or exercise interventions vs combined behavioral weight management programs: A systematic review and meta-analysis of direct comparisons. J. Acad. Nutr. Diet. 2014, 114, 1557–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dombrowski, S.U.; Knittle, K.; Avenell, A.; Araújo-Soares, V.; Sniehotta, F.F. Long term maintenance of weight loss with non-surgical interventions in obese adults: Systematic review and meta-analyses of randomised controlled trials. BMJ 2014, 348, g2646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peirson, L.; Douketis, J.; Ciliska, D.; Fitzpatrick-Lewis, D.; Usman, M.; Parminder, R. Treatment for overweight and obesity in adult populations: A systematic review and metaanalysis. CMAJ Open 2014, 2, E306–E317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, H.P.; Prevost, A.T.; Gulliford, M.C. Access to weight reduction interventions for overweight and obese patients in UK primary care: Population-based cohort study. BMJ Open 2015, 5, e006624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perk, J.; De Backer, G.; Gohlke, H.; Graham, I.; Reiner, Z.; Verschuren, M.; Verschuren, M.; Albus, C.; Benlian, P.; Boysen, G.; et al. European guidelines on cardiovascular disease prevention in clinical practice (version 2012). Eur. Heart J. 2012, 33, 1635–1701. [Google Scholar]
- American Diabetes Association (ADA). Classification and diagnosis of diabetes. Diabetes Care 2015, 38 (Suppl. 1), S8–S16. [Google Scholar] [CrossRef] [Green Version]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H.; Obesity Management Task Force of the European Association for the Study of Obesity. European guidelines for obesity management in adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.; Donato, K.A.; Apovian, C.M.; Comuzzie, A.G.; Hu, F.B. Guidelines (2013) for managing overweight and obesity in adults. Obesity 2014, 22 (Suppl. 2), S1–S414. [Google Scholar]
- Patterson, L.; Kee, F.; Hughes, C.; O’Reilly, D. The relationship between BMI and the prescription of anti-obesity medication according to social factors: A population cross sectional study. BMC Public Health 2014, 14, 87. [Google Scholar] [CrossRef] [Green Version]
- Samaranayake, N.R.; Ong, K.L.; Leung, R.Y.H.; Cheung, B.M.Y. Management of obesity in the National Health and Nutrition Examination Survey (NHANES), 2007–2008. Ann. Epidemiol. 2012, 22, 349–353. [Google Scholar] [CrossRef] [Green Version]
- Saxon, D.R.; Iwamoto, S.J.; Mettenbrink, C.J.; McCormick, E.; Arterburn, D.; Daley, M.F.; Oshiro, C.E.; Koebnick, C.; Horberg, M.; Young, D.R.; et al. Antiobesity medication use in 2.2 million adults across eight large health care organizations: 2009–2015. Obesity 2019, 27, 1975–1981. [Google Scholar] [CrossRef]
- Banegas, J.R.; López-García, E.; Dallongeville, J.; Guallar, E.; Halcox, J.P.; Borghi, C.; Massó-González, E.L.; Jiménez, F.J.; Perk, J.; Steg, P.G.; et al. Achievement of treatment goals for primary prevention of cardiovascular disease in clinical practice across Europe: The EURIKA study. Eur. Heart J. 2011, 32, 2143–2152. [Google Scholar] [CrossRef] [PubMed]
- Farran, N.; Ellis, P.; Lee Barron, M. Assessment of provider adherence to obesity treatment guidelines. J. Am. Acad. Nurse Pract. 2013, 25, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Menezes, M.C.; Duarte, C.K.; Costa, V.P.; Lopes, M.S.; Freitas, P.P.; Campo, S.F.; Lopes, A.C.S. A systematic review of effects, potentialities, and limitations of nutritional interventions aimed at managing obesity in primary and secondary health care. Nutrition 2020, 75–76, 110784. [Google Scholar] [CrossRef] [PubMed]
- Retat, L.; Pimpin, L.; Webber, L.; Jaccard, A.; Lewis, A.; Tearne, S.; Hood, K.; Christian-Brown, A.; Adab, P.; Begh, R.; et al. Screening and brief intervention for obesity in primary care: Cost-effectiveness analysis in the BWeL trial. Int. J. Obes. 2019, 43, 2066–2075. [Google Scholar] [CrossRef] [PubMed]
- William HDietz, W.H.; Gallagher, C. A proposed standard of obesity care for all providers and payers. Obesity 2019, 27, 1059–1062. [Google Scholar]
- Booth, H.P.; Prevost, A.T.; Gulliford, M.C. Epidemiology of clinical body mass index recording in an obese population in primary care: A cohort study. J. Public Health Oxf. Engl. 2013, 35, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S.; Maynard, L.M.; Li, C. Trends in mean waist circumference and abdominal obesity among us adults, 1999–2012. JAMA 2014, 312, 1151–1153. [Google Scholar] [CrossRef] [Green Version]
- Heindel, J.J.; Blumberg, B. Environmental obesogens: Mechanisms and controversies. Annu. Rev. Pharmacol. Toxicol. 2019, 59, 89–106. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total n = 209 | Men n = 88 (42.1) | Women n = 121 (57.9) | p | |
|---|---|---|---|---|
| Age (years) Mean ± SD | 65.8 ± 12.7 | 63.2 ± 13.6 | 67.6 ± 11.8 | 0.015 |
| BMI (kg/m2) Mean ± SD | 34.2 ± 4.5 | 33.5 ± 4.1 | 34.7 ± 4.7 | 0.059 |
| WC (cm) Mean ± SD | 111.4 ± 11.6 | 116.2 ± 10.1 | 107.9 ± 11.5 | <0.0001 |
| HBP n (%) | 179 (85.6) | 79 (89.8) | 100 (82.6) | 0.166 |
| T2DM n (%) | 81 (38.8) | 34 (38.6) | 47 (38.8) | 1 |
| HC n (%) | 130 (62.2) | 55 (62.5) | 75 (62.0) | 1 |
| HTG n (%) | 66 (31.7) | 36 (41.4) | 30 (24.8) | 0.009 |
| Smoker n (%) | 27 (12.9) | 18 (20.5) | 9 (7.4) | 0.007 |
| 5 Years before | Current | 5 Years before vs. Current | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total N = 209 | Men n (%) 88 (42.1) | Women n (%) 121 (57.9) | p Men vs. Women | Total N = 209 | Men n (%) 88 (42.1) | Women n (%) 121 (57.9) | p Men vs. Women | p Total Group | |
| Age (years) Mean ± SD | - | - | - | - | 65.8 ± 12.7 | 63.2 ± 13.6 | 67.6 ± 11.8 | 0.015 | - |
| BMI kg/m2 Mean ± SD | 34.6 ± 4.2 | 33.7 ± 3.8 | 35.2 ± 4.3 | 0.015 | 34.2 ± 4.5 | 33.5 ± 4.1 | 34.7 ± 4.7 | 0.059 | 0.037 |
| WC cm Mean ± SD | 107.0 ± 9.9 | 110.6 ± 8.6 | 104.7 ± 10.2 | <0.0001 | 111.4 ± 11.6 | 116.2 ± 10.1 | 107.9 ± 11.5 | <0.0001 | <0.0001 |
| HBP n (%) | 161 (77.0) | 70 (79.5) | 91 (75.2) | 0.508 | 179 (85.6) | 79 (89.8) | 100 (82.6) | 0.166 | <0.0001 |
| T2DM n (%) | 57 (27.3) | 25 (28.4) | 32 (26.4) | 0.756 | 81 (38.8) | 34 (38.6) | 47 (38.8) | 1 | <0.0001 |
| HC n (%) | 94 (45.0) | 39 (44.3) | 55 (45.5) | 0.889 | 130 (62.2) | 55 (62.5) | 75 (62.0) | 1 | <0.0001 |
| HTG n (%) | 57 (30.5) | 31 (40.8) | 26 (23.4) | 0.015 | 66 (31.7) | 36 (41.4) | 30 (24.8) | 0.015 | <0.0001 |
| Smoker n (%) | 35 (16.7) | 24 (27.3) | 11 (9.1) | 0.001 | 27 (12.9) | 18 (20.5) | 9 (7.4) | 0.007 | 0.021 |
| AMI n (%) | 14 (6.7) | 12 (13.6) | 2 (1.7) | 0.001 | 22 (10.5) | 16 (18.2) | 6 (5.0) | 0.003 | 0.008 |
| OSAS n (%) | 7 (3.3) | 4 (4.5) | 3 (2.5) | 0.458 | 20 (9.6) | 11 (12.5) | 9 (7.4) | 0.241 | <0.0001 |
| Total (n = 209) | Men (n = 88) | Women (n = 121) | p | |
|---|---|---|---|---|
| Indication of obesity drug n (%) | 201 (96.2) | 85 (96.6) | 116 (95.9) | 1.000 |
| Prescription of Obesity drugs recorded n (%) | 3 (1.4) | 1 (1.1) | 2 (1.7) | 1.000 |
| (1) Diet | ||||
| (a) Prescription of diet recorded n (%) | 167 (79.9) | 72 (81.8) | 95 (78.5) | 0.603 |
| (b)Type of prescribed diet: Hypocaloric diet n (%) | 59 (28.2) | 34 (38.6) | 25 (20.7) | 0.005 |
| (c) Recorded follow up n (%) | 146 (69.9) | 65 (73.9) | 81 (66.9) | 0.291 |
| Clinical histories of patients that had records that met all recommendations on (a) prescription of diet, (b) type of diet and (c) follow up | 53 (25.4) | 32 (36.4) | 21 (17.4) | 0.002 |
| (2) Physical activity | ||||
| (a) Prescription of physical activity recorded n (%) | 185 (88.5) | 80 (90.9) | 105 (86.8) | 0.389 |
| (b) Type of physical activity (e.g., walking, running, etc.) recorded n (%) | 173 (82.8) | 73 (83.0) | 100 (82.6) | 1.000 |
| (c) Duration, frequency and intensity of physical activity recorded n (%) | 134 (64.1) | 58 (65.9) | 76 (62.8) | 0.664 |
| (d) Increasing physical activity recorded n (%) | 4 (1.9) | 2 (2.3) | 2 (1.7) | 1.000 |
| (e) Recorded follow up n (%) | 160 (76.6) | 72 (81.8) | 88 (72.7) | 0.139 |
| Clinical histories of patients that had records that met all recommendations on (a) prescription of physical activity, (b) type of physical activity (c) duration, frequency and intensity, (d) increasing physical activity and (e) follow up | 3 (1.4) | 1 (1.1) | 2 (1.7) | 1.000 |
| (3) Behavior change | ||||
| (a) Prescription of behavior change recorded n (%) | 6 (2.9) | 3 (3.4) | 3 (2.5) | 0.698 |
| (b) Type of behavior change recorded n (%) | 2 (1.5) | 1 (1.8) | 1 (1.3) | 1.000 |
| (c) Recorded follow up n (%) | 4 (1.9) | 2 (2.3) | 2 (1.7) | 1.000 |
| Clinical histories of patients that had records that met all recommendations on (a) Prescription of behavior change, (b) type of behavior change and (c) follow up | 2 (1.5) | 1 (1.8) | 1 (1.3) | 1.000 |
| Patients adherence to treatment | ||||
| Patients adherence to the prescribed diet n (%) | 26 (12.4) | 17 (19.3) | 9 (7.4) | 0.018 |
| Patients adherence to the prescribed physical activity n (%) | 49 (23.4) (49) | 23 (26.1) | 26 (21.5) | 0.509 |
| Patients adherence to the prescribed behavior change n (%) | 1 (0.5) | 0 (0.0) | 1 (0.8) | 1.000 |
| (A) BMI | Standardized ß | p | CI 95% |
|---|---|---|---|
| Prescription of diet recorded (79.9%) | 0.089 | 0.400 | −1.373/3.411 |
| Follow up diet recorded (69.9%) | −0.028 | 0.813 | −2.607/2.049 |
| Prescription of PA recorded (88.5%) | −0.121 | 0.196 | −4.229/0.875 |
| Follow up PA (76.6%) | 0.172 | 0.119 | −0.474/4.105 |
| Age | −0.115 | 0.086 | −0.099/0.007 |
| (B) WC | Standardized ß | p | CI 95% |
| Prescription of diet recorded (79.9%) | 0.066 | 0.656 | −8.437/13.322 |
| Follow up diet recorded (69.9%) | −0.250 | 0.163 | −18.265/3.131 |
| Prescription of PA recorded (88.5%) | 0.132 | 0.263 | −5.173/18.630 |
| Follow up PA recorded (76.6%) | 0.238 | 0.192 | −3.975/19.400 |
| Age | −0.068 | 0.491 | −0.291/0.141 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trujillo-Garrido, N.; Bernal-Jiménez, M.Á.; Santi-Cano, M.J. Evaluation of Obesity Management Recorded in Electronic Clinical History: A Cohort Study. J. Clin. Med. 2020, 9, 2345. https://doi.org/10.3390/jcm9082345
Trujillo-Garrido N, Bernal-Jiménez MÁ, Santi-Cano MJ. Evaluation of Obesity Management Recorded in Electronic Clinical History: A Cohort Study. Journal of Clinical Medicine. 2020; 9(8):2345. https://doi.org/10.3390/jcm9082345
Chicago/Turabian StyleTrujillo-Garrido, Nuria, María Ángeles Bernal-Jiménez, and María J. Santi-Cano. 2020. "Evaluation of Obesity Management Recorded in Electronic Clinical History: A Cohort Study" Journal of Clinical Medicine 9, no. 8: 2345. https://doi.org/10.3390/jcm9082345
APA StyleTrujillo-Garrido, N., Bernal-Jiménez, M. Á., & Santi-Cano, M. J. (2020). Evaluation of Obesity Management Recorded in Electronic Clinical History: A Cohort Study. Journal of Clinical Medicine, 9(8), 2345. https://doi.org/10.3390/jcm9082345