2. Conceptualizing Religiousness/Spirituality
Religiousness/spirituality is a multidimensional construct, and meta-analyses highlight the myriad of ways in which religiousness/spirituality is conceptualized and operationalized, as well as the challenges this presents when categorizing R/S dimensions “based on their conceptual similarities” and distinctions (
Hodapp and Zwingmann 2019, p. 1985). Further,
Yonker et al. (
2012) noted the frequent “disconnect” between conceptualization and measurement (p. 311). Nevertheless, meta-analytic categorizations provide a useful foundation for conceptualizing religiousness/spirituality.
Hodapp and Zwingmann (
2019), for example, informed by the conceptualization and measurement of R/S centrality (
Huber and Huber 2012), subsumed belief in God, salience, public and private practices, intrinsic religiousness/spirituality, and subjective experiences under the dimension of centrality. Then, based on the comparable effect sizes between centrality and the dimensions of adaptive relating (e.g., positive religious coping, positive image of the sacred), spirituality, and other (e.g., quest religious motivation, R/S well-being), they merged these dimensions into a single dimension labeled positive overall. They labeled their second dimension maladaptive relating (e.g., extrinsic religiousness/spirituality, negative religious coping, negative image of the sacred), which tended to show larger effect sizes.
Garssen et al. (
2021) chose to keep the centrality subdimensions separate, and yet admitted their dimension labeled importance, which included R/S commitment, salience, and intrinsic religiousness/spirituality, “is rather confusing”, especially since intrinsic religiousness was also a distinct dimension (p. 8). Between
Hodapp and Zwingmann’s (
2019) two dimensions and
Garssen et al.’s (
2021) eight dimensions,
Yonker et al. (
2012) created five dimensions, with one labeled salience, which overlaps with the positive overall dimension, apart from public and private practices which were kept separate. Unique to
Yonker et al.’s (
2012) categorization was a distinct dimension labeled R/S searching (i.e., “actively engaged in exploring or questioning”, p. 304); however, there was only one study that examined searching.
Hodapp and Zwingmann (
2019) found that quest religious motivation, an operationalization of searching, was a nonsignificant predictor of mental health (n = 3 studies), consistent with the mixed findings for searching—well-being associations, and adaptive and maladaptive types of searching (
Jankowski et al. 2022a). Consistent across meta-analyses was the small effect size for the influence of greater centrality/importance/salience on better mental health, that is, lower symptoms and/or greater subjective (e.g., life satisfaction), eudaimonic (e.g., positive social functioning) and/or general well-being. Psychotherapy researchers have defined the outcome of both lower symptoms and greater well-being as flourishing (
Jankowski et al. 2020b).
The relational spirituality model (RSM) provided our conceptual framework for religiousness/spirituality, defined as “ways of relating to the sacred” (
Sandage et al. 2020, p. 24). The term sacred encompasses beliefs, practices, objects, and experiences that can (a) occur in religious and non-religious contexts, and (b) be perceived as associated with the divine or ultimate, that is, beyond the ordinary and beyond the self (
Sandage et al. 2020). Within the RSM, relating to the sacred is conceptualized developmentally along the two dimensions of dwelling and seeking (
Sandage et al. 2020). Dwelling fits the meta-analytic dimension of centrality/importance/salience, whereas seeking is consistent with the dimension of searching. The existing research on religiousness/spirituality, COVID-19 impact, and symptoms and/or well-being has predominantly focused on the dimensions of centrality/importance/salience and adaptive relating, typically using measures of R/S commitment/intrinsic-ness and positive religious coping, respectively. The dimension of maladaptive relating (e.g., negative religious coping, R/S struggles) has received lesser attention.
Consistent with the existing literature, we examined the influence of a measure of centrality/importance/salience on COVID-19 impact, that is, R/S dwelling. As
Bentzen (
2021) noted, “people use mainly their intrinsic religiosity (such as personal relation to God and private prayer) … to cope with adversity” (p. 543). We also included measures of R/S struggles and R/S exploration, the former which can capture R/S and existential aspects of coping with the pandemic. As
Bockrath et al. (
2021) stated, R/S struggles “have the capacity to disrupt the individual’s adjustment in the emotional and psychological realm” (p. 11). R/S exploration operationalizes the dimension of R/S seeking and represents efforts at meaning-making in the face of existential challenges (
Sandage et al. 2020), and a “way that believers … resolve their doubts and find the spiritual meaning to soothe their existential concerns” (
Arrowood et al. 2022, p. 114).
3. Religious/Spiritual Coping Hypothesis
The primary lens researchers have used to examine associations between religiousness/spirituality, COVID-19 impact, symptoms, and well-being seems to be a theoretical formulation of religiousness/spirituality as a coping resource. Such formulations suggest “that R/S factors have a stronger effect or have only an effect if a person is exposed to adverse conditions” (
Garssen et al. 2021, p. 15), or “that R/S can unfold its resources especially in times of a life crisis” (
Hodapp and Zwingmann 2019, p. 1990). However, recent meta-analyses of the R/S–well-being association did not find support for the coping hypothesis (
Garssen et al. 2021;
Hodapp and Zwingmann 2019), whereas a meta-analysis of the R/S–resilience association found a positive effect (
Schwalm et al. 2022).
Schwalm et al. (
2022) defined resilience as “cop[ing] satisfactorily with adverse circumstances” (p. 1219), and they used observational designs with an explicit measure of resilience to test the association. However,
Schwalm et al. (
2022) noted that the conflation between measures of R/S and resilience was a significant limitation to their study. In contrast, Garssen et al. excluded studies in which there was evidence of construct overlap between measures of R/S and well-being. Conflation or insufficient discriminant validity is a long-standing concern within the study of R/S–well-being associations (
Jankowski et al. 2022d). As such, studies testing the R/S coping hypothesis must attend closely to the construct validity evidence for the measures used to assess R/S and well-being, making sure there is sufficient evidence for related constructs from different measures and subscales within a measure to be distinct. Nevertheless, individual studies with the pandemic as a life stressor have found mixed support for the R/S coping hypothesis.
Prazeres et al. (
2021), in their cross-sectional study with healthcare workers in Portugal, found that public and private R/S involvement, and R/S intrinsic-ness, were nonsignificant predictors of COVID-19 fear and anxiety. Prazeres et al. interpreted their findings as contrary to the theoretical premise that religiousness/spirituality “offers cognitive and emotional tools to deal with uncertainty and to overcome adversity” (p. 7).
Cowden et al. (
2021) found that higher levels of positive religious coping exacerbated the greater pandemic-related resource loss–greater suffering longitudinal association, in a sample of chronically ill adults in the United States (US). Cowden et al. suggested that one possibility is that positive religious coping “compounded personal experiences of suffering by triggering religious/spiritual struggles when relief from the strains of resource loss were not readily evident” (p. 13).
Using the same sample of chronically ill adults,
Davis et al. (
2021) found that levels of symptoms, well-being, and R/S struggles remained stable over time, from one-month prior to three months post pandemic declaration. Positive religious coping declined, and particularly so among the religiously affiliated, with the decline less among those reporting greater symptoms pre-pandemic. Such findings offer mixed evidence for the R/S coping hypothesis. However, participants reporting greater suffering pre-pandemic reported gains in spiritual fortitude over time, relative to those reporting less suffering, the latter who declined in spiritual fortitude. Spiritual fortitude has been defined as the use of R/S “resources to cope with negative emotions in the face of stressors” (
Zhang et al. 2020, p. 288), and as such, is a measure that explicitly operationalizes the R/S coping hypothesis. In the
Davis et al. (
2021) study, tests involving spiritual fortitude seemed to provide evidence for the R/S coping hypothesis. Davis et al. interpreted their findings as evidence of resilience, and unique to their sample, suggested that their participants’ prior exposure to the stress associated with living with a chronic illness prepared them for coping with pandemic stress. Such an interpretation is consistent with the challenge or inoculation model of resilience (
Zimmerman and Arunkumar 1994).
In addition,
Kranz et al. (
2020), using a US sample of adults recruited via a crowdsourcing platform, found that greater R/S intrinsic-ness predicted greater COVID-19 somatic anxiety, which in turn predicted greater endorsement of unreasonable preventive behaviors (e.g., hoarding toilet paper). Kranz et al. referred to this indirect path as maladaptive coping. At the same time, greater R/S intrinsic-ness was associated with lower COVID-19 worry, which in turn predicted greater reasonable preventive behavior (e.g., avoiding crowded spaces). Kranz et al. surmised that religiousness/spirituality “can be a significant source of resilience; on the other [hand], it can be a risk factor” (p. 3). Findings in the larger literature have similarly documented protective and risk effects for measures of R/S dwelling (e.g.,
Ensz and Jankowski 2020;
Jankowski et al. 2020a;
Paine et al. 2018), often as a function of the interaction with other risk and/or protective factors. The latter is consistent with the protective factors model, which frames resilience as a process involving complex interactions between risk and protective factors (
Zimmerman and Arunkumar 1994). Last, similar to
Kranz et al. (
2020),
Milligan et al. (
2021) found that lower self-rated levels of religiousness/spirituality and Democratic party affiliation predicted willingness to receive a COVID-19 vaccine (no/yes), which is a reasonable preventive behavior.
At the same time, some researchers have found that R/S dwelling-related variables may help people cope with the impact of COVID-19.
Zhang et al. (
2020), in their cross-sectional community sample of adults recruited via an online crowdsourcing website, found that spiritual fortitude lessened the magnitude of the greater pandemic-related resource loss–greater suffering association. Also offering cross sectional support for the R/S coping hypothesis,
Prieto-Ursúa and Jódar (
2020) using a sample of adults in Spain found that greater R/S identification was associated with greater post-traumatic growth, as was COVID-19 diagnosis, knowing someone who died, and greater goals and purpose in life. They interpreted their findings as evidence of the capacity to experience positive growth amidst adversity (i.e., prioritizing personal values, finding support, group affiliation). Prieto-Ursúa and Jódar suggested that religiousness/spirituality can contribute to positive growth through meaning-making and social support; that is, positive religious coping.
Additionally, in a cross-sectional sample of Polish adults who identified as “practicing Catholics”,
Dobrakowski et al. (
2021, p. 4) found that greater negative religious coping predicted lower life satisfaction and lower satisfaction with support, through greater COVID-19 anxiety. Positive religious coping was directly associated with greater life satisfaction and satisfaction with support. The greater negative religious coping–greater COVID-19 anxiety association is consistent with existing findings (e.g.,
Lee 2020). However, they also found a positive bivariate association between positive religious coping and COVID-19 anxiety.
Dobrakowski et al. (
2021) suggested that this unexpected finding may have been due to mixed messages about the pandemic from leadership, unanswered prayers, and/or because of the cross-sectional correlational data, with the latter specifically suggesting that greater positive religious coping could have been a response to greater anxiety. Last,
Pirutinsky et al. (
2020) found that among a cross-sectional sample of American Orthodox Jews, greater R/S intrinsic-ness corresponded to higher ratings of positive COVID-19 impact, and similarly, greater positive religious coping corresponded to perceptions of more positive COVID-19 impact.
Thus, while cross-sectional findings typically find support for the R/S coping hypothesis, longitudinal studies have found a general lack of support for the R/S coping hypothesis (
Cowden et al. 2021;
Garssen et al. 2021;
Mauritsen et al. 2022). One possible explanation for the difference seems to center on coping as a complex, heterogenous, and dynamic process. Research designs must cover a sufficient amount of elapsed time, “for the occurrence of life events that potentially change the level of mental health, and for which R/S might [then] act as a coping resource” (
Garssen et al. 2021, p. 7). Longitudinal designs that have mapped responses to pandemic-related stressors seem to follow an initial exacerbating influence among those who had higher pre-pandemic levels of distress (
Breslau et al. 2021), along with evidence that as the pandemic continued, individuals tended to return to pre-pandemic levels of distress (
Daly and Robinson 2021). Snapshots of data at different points within this dynamic process may differ from designs that track change over time. A second explanation for the discrepancy between cross-sectional and longitudinal findings may stem from the greater control of confounds inherent to causal inference (
Cowden et al. 2021). Possible confounds could include “secular institutions and norms … [which] might address social, epistemic, and material needs in a crisis” rather than R/S (
Mauritsen et al. 2022, p. 2), and further, “religious, secular, scientific, and political worldviews” may each serve as effective meaning-making frameworks in times of crisis (p. 3). Sufficiently tracking change over time should involve capturing heterogeneity in coping (
Crabtree et al. 2021) and covariates to rule out alternative explanations and discern the unique influence of R/S.
4. The Current Study
We extended this rapidly emerging research on religiousness/spirituality, COVID-19 impact, and symptoms and well-being to the largely neglected context of psychotherapy, and specifically, adult clients receiving psychotherapy at a community mental health center in the US. Support for the R/S coping hypothesis has resulted in suggestions for the design of interventions to promote positive religious coping (e.g.,
Dobrakowski et al. 2021) and contradictory evidence has corresponded to judicious approaches to integrating R/S into mental health treatment (e.g.,
Cowden et al. 2021). In the current naturalistic, practice-based study, we explored how R/S dimensions influenced the change trajectories of psychotherapy clients. Specifically, we used the RSM framework (
Sandage et al. 2020) to explore R/S struggles, dwelling, and seeking. R/S struggles have been identified as relevant to future research examining religiousness/spirituality, COVID-19 impact, and symptoms and well-being (e.g.,
Dein et al. 2020). Client reports of greater R/S struggles have predicted lower levels of life functioning over and above the effect of mental health symptoms, and R/S dwelling and R/S seeking were each positively associated with client preferences for R/S engagement in psychotherapy (
Sandage et al. 2022). Prior research has also shown the potential for balanced R/S dwelling–seeking to have a salutary influence on symptoms and well-being (e.g.,
Jankowski et al. 2021b).
We used person-centered analysis to generate distinct change trajectories in levels of symptoms and well-being over three time points during treatment. We postulated three hypotheses. First, we expected that the stress of the pandemic, assessed as COVID-19 impact, would influence change trajectories. Prior research has found that endorsement of life stressors increased the likelihood of no change for some clients, and for others, endorsement of life stressors predicted deterioration (
Jankowski et al. 2021a). As a second hypothesis, we expected that the influence of the COVID-19 impact stressor would vary as a function of R/S dwelling and seeking. We examined this expectation by modeling the interaction between R/S dwelling × R/S seeking × COVID-19 impact when predicting change trajectories. We expected that higher levels of R/S dwelling and seeking would condition the influence of COVID-19 impact such that clients reporting more positive COVID-19 impact ratings would be more likely to belong to subgroups showing lower initial levels of symptoms and higher well-being, and linear trajectories of improvement. As our third hypothesis, we expected that R/S struggles would be associated with non-growth trajectories, consistent with meta-analytic findings of a nonsignificant association between R/S struggles and positive adjustment, and a significant association between greater R/S struggles and greater maladjustment (
Bockrath et al. 2021).
6. Results
The 3-class solution fit better relative to other solutions based on the lowest BIC (e.g., 3-class model BIC = 2650.56; 2-class model BIC = 2718.22; 4-class model BIC = 2676.49), with acceptable entropy (entropy = 0.77) and AvePPs > 0.83.
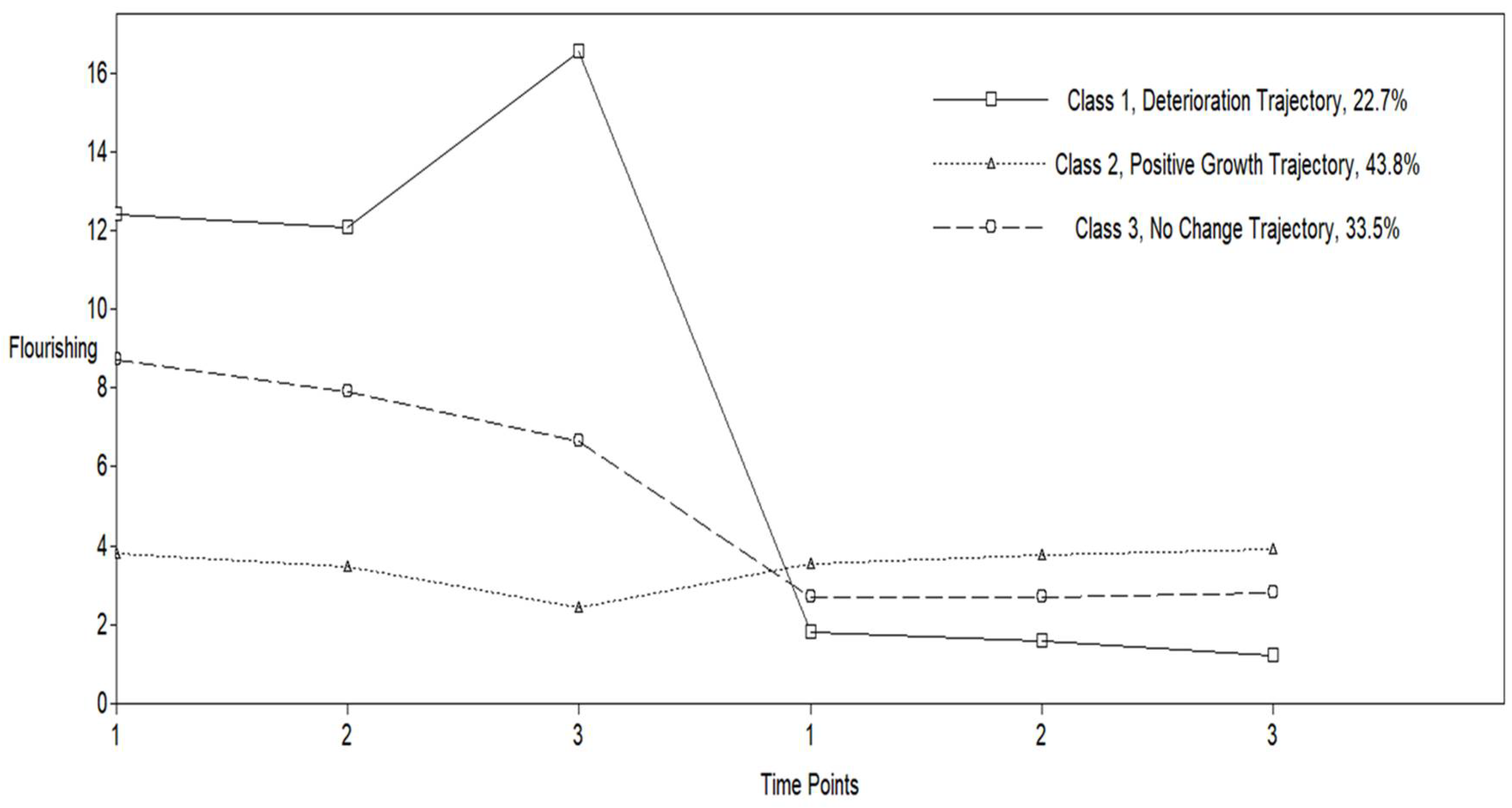
Figure 1 depicts the trajectories for symptoms and well-being. We found a trajectory with high levels of depression and low well-being that showed deterioration, and labeled this subgroup languishing, based on language used in prior research (
Jankowski et al. 2021a). We also found a positive growth trajectory, with low levels of depression and high well-being, relative to the other two trajectories. We labeled this subgroup flourishing (
Jankowski et al. 2021a). Last, we found a no change trajectory, with levels of depression and well-being in the mid-range relative to other two trajectories. We labeled this subgroup moderately healthy (
Jankowski et al. 2021a).
Next, we examined the influence of demographic variables, R/S struggles, R/S dwelling, R/S seeking, and COVID-19 impact on class membership, with parameters fixed as a result of the 2-step procedure. We also explored the moderating influence of R/S dwelling and seeking on the COVID-19 impact prediction of class membership. Heterosexual identification predicted greater likelihood of belonging to the flourishing subgroup, relative to the languishing (B = 2.53, SE = 0.91, p = 0.01). In addition, as R/S struggles increased participants were less likely to belong to the flourishing (B = −1.68, SE = 0.58, p = 0.004), relative to the languishing. Further, the languishing reported significantly more R/S struggles relative to the flourishing (d = −1.17, SE = 0.33, p < 0.001). COVID-19 impact was a nonsignificant independent predictor of class membership, although the languishing did differ from the flourishing (d = 0.60, SE = 0.27, p = 0.03) and moderately healthy (d = 0.83, SE = 0.23, p < 0.001), with the languishing reporting more negative COVID-19 impact ratings. In addition, subgroups did not differ on levels of R/S seeking, but the flourishing did report significantly higher levels of R/S dwelling relative to the languishing (d = 0.73, SE = 0.25, p = 0.003). Nevertheless, the three-way interaction involving R/S dwelling × R/S seeking × COVID-19 impact predicted class membership, for languishing relative to moderately healthy subgroups (B = 0.02, SE = 0.01, p = 0.01). We probed the significant three-way interactions at low and high levels of the moderators (i.e., minimum value and maximum value of the range) using the MODEL CONSTRAINT command in Mplus. For the languishing subgroup (i.e., deterioration trajectory) relative to the moderately healthy (i.e., no change trajectory), when R/S dwelling and seeking were both high, as COVID-19 impact ratings became more positive, participants were more likely to belong to the moderately healthy (B = 0.29, SE = 0.10, p = 0.01).
7. Discussion
The influence of COVID-19 impact ratings on subgroup membership varied as a function of religiousness/spirituality, offering partial support for our first and second hypotheses. As expected, we found a protective influence for high levels of R/S dwelling and seeking on the influence of COVID-19 impact on subgroup membership, increasing the likelihood of belonging to the moderately healthy, relative to the languishing. However, this protective effect was not associated with linear trajectories of improvement. Nevertheless, the protective effect is consistent with prior findings that tested the RSM theoretical premise that integrated R/S dwelling and seeking can be adaptive (e.g.,
Jankowski et al. 2021b). Specifically,
Jankowski et al. (
2021b) found a subgroup of participants who reported high levels of R/S dwelling and seeking, and who also exhibited low symptoms and high levels of subjective and eudaimonic well-being. As such, the protective influence of high R/S dwelling and seeking could represent greater critical reflection on the complexities of R/S commitments and relational connection with the sacred in the face of the pandemic. Our results could therefore offer support for the R/S coping hypothesis. Greater R/S engagement can function as an adaptive coping strategy during adversity (
Hodapp and Zwingmann 2019). More positive COVID-19 impact ratings at higher levels of R/S dwelling and seeking suggests adaptive coping amidst pandemic stress.
Along these lines, our results suggest perhaps that high R/S dwelling and seeking actualized “psychological resources”, the latter defined as “all the mental dispositions and cognitive habits that are beneficial for well-being” (
Pellerin and Raufaste 2020, p. 3).
Pellerin and Raufaste (
2020) found, for example, that gratitude, acceptance, hope, and wisdom protected against the risk influence of the pandemic to lower levels of subjective and eudaimonic well-being over time. In our study, it is possible that greater R/S dwelling and seeking mobilized these virtues, respectively defined by
Pellerin and Raufaste (
2020) as “appreciation … of being” and “non-reactivity in the present moment” (p. 3), “new ways to attain … goals and … be more satisfied with their present situation”, (p. 16), and wisdom as a “meta-resource” activating the other virtues (p. 17). Greater R/S dwelling and R/S seeking have independently shown associations with greater virtuousness (e.g.,
Jankowski et al. 2022a,
2022d), as has an integrated high R/S dwelling and seeking profile (
Jankowski et al. 2021b). Further, in a cross-sectional study using a clinical sample of outpatient clients,
Paine et al. (
2018) found that higher humility enhanced the protective influence of R/S dwelling on levels of subjective and eudaimonic well-being, whereas at low levels of humility, R/S dwelling exhibited a risk effect on levels of well-being.
Gulliford and Roberts (
2018) suggested that humility may be a meta-resource, activating the other virtues, “foster[ing] the virtues of intelligent caring by the elimination of ego-pollution, and serv[ing] the virtues of willpower by allowing mental clarity about the need to deploy them” (p. 214), with wisdom as “the intelligence in intelligent caring” (p. 215).
Alternatively, the protective influence for greater R/S dwelling and seeking, could perhaps signal R/S bypass, given comparable levels of R/S struggles among the languishing and moderately healthy, and at the same time, more negative COVID-19 impact ratings among the languishing relative to the moderately healthy. R/S bypass can be defined as a form of experiential avoidance that involves exaggerating the “spiritual significance” of life events (
Fox and Picciotto 2019, p. 239). However, this avoidance can be adaptive, at least in the short term, by minimizing R/S struggles for example (
Fox and Picciotto 2019).
Umucu and Lee (
2020) explored the use of coping strategies during the pandemic and found that greater denial predicted greater general well-being, along with the more typical adaptive strategies of greater R/S, emotional support, humor, and active coping. In addition,
Jankowski et al. (
2021b) found five distinct RSM profiles, two of which showed comparably high levels of R/S dwelling and seeking. These two profiles showed similarly high levels of virtuousness and well-being and low levels of anxiety. However, one subgroup showed a greater tendency to exaggerate their religiousness/spirituality and reported greater levels of R/S struggles with God, scrupulosity, and God monitoring. Jankowski, Sandage et al. concluded that the latter high R/S dwelling and seeking subgroup seemed to be characterized by a relating to the sacred that consisted of an inner compulsory motivation to avoid guilt, and at the same time, an externally pressured motivation to avoid disapproval. Last, we found support for our third hypothesis, and specifically, that greater R/S struggles predicted membership in the languishing, relative to the flourishing, which is consistent with the meta-analytic finding of a positive association between R/S struggles and maladjustment (
Bockrath et al. 2021).
Taken together, the role of high R/S dwelling and seeking could depict either a relational religiousness/spirituality that experiences support and comfort in its relation with the sacred while engaging in active meaning making or a relational religiousness/spirituality that indiscriminately reports high dwelling and seeking and which uses religiousness/spirituality as an avoidant coping strategy by minimizing or denying the difficulties associated with the pandemic. The latter R/S characterization could account for the mid-level reports of symptoms and well-being and the lack of change experienced during treatment by the moderately healthy. As
Fox and Picciotto (
2019) noted, R/S bypass tends to be associated with stagnation. Further,
Cook et al. (
2014) found an “indiscriminately pro-religious” subgroup reporting high R/S dwelling and seeking that differed from another high R/S dwelling and seeking subgroup (p. 86). The indiscriminately pro-religious subgroup reported higher extrinsic R/S, lower satisfaction with their R/S life, and lower use of adaptive coping skills. Future research should investigate the complex connections between R/S dwelling, seeking, and struggles, and use additional indicators of religiousness/spirituality to parse out subtle distinctions among profiles of high R/S dwelling and seeking. These profiles could then be used as predictors of treatment outcome over time.
A third possible interpretation for the protective influence of R/S dwelling and seeking on the influence of COVID-19 impact on treatment change is that the apparent stagnation among the moderately healthy could represent an adaptive process which has not yet bore fruit. As we note below, some trajectories exhibit later treatment change. Additionally, some conceptualizations of resilience connote “maintaining stable functioning despite adversity” (
Crabtree et al. 2021, p. 3). It is possible therefore that the lack of change among the moderately healthy represented symptom stabilization during a crisis, and as such, a desirable treatment outcome (
Owen et al. 2019). In fact, the trajectory was trending down for depression symptoms, remaining within the mild range, albeit it was nonsignificant. In contrast, the flourishing reported comparable levels of COVID-19 impact to the moderately healthy, and yet, R/S dwelling and seeking did not condition the influence of COVID-19 impact on the change trajectory for the flourishing, relative to the languishing and moderately healthy. Despite comparable levels of R/S dwelling and R/S seeking among the flourishing relative to the moderately healthy, the nonsignificant interaction suggests that ratings of COVID-19 impact among the flourishing were independent of their R/S engagement, and independent of their change experienced during treatment. The latter is also consistent with our finding that COVID-19 impact was a nonsignificant independent predictor of change trajectories, which provided contradictory evidence for our first hypothesis. Together, these nonsignificant findings suggest that the flourishing may have used alternative strategies to cope with pandemic-related stress, other than R/S engagement.
As
Mauritsen et al. (
2022) noted, there are other resources that can serve “crisis-management function(s)” besides R/S (p. 3). In the context of our study, and consistent with CRP and the therapeutic alliance as a primary locus of intervention, psychotherapy may have been a sufficient source of “comfort and safety” and an active facilitator of meaning making (p. 18); and if it was not psychotherapy, the flourishing may have found relational coping resources elsewhere. Such an interpretation seems consistent with the higher levels of general well-being reported among the flourishing, which includes a dimension of belongingness (
Jankowski et al. 2022c), and particularly so relative to the languishing who declined in well-being. Previous qualitative findings suggested that clients in a high symptoms and low well-being subgroup, consistent with our languishing subgroup, were “most relationally disadvantaged”, as they were more likely to describe experiences of isolation and loneliness (
Crabtree et al. 2021, pp. 8–9).
Last, the R/S coping hypothesis connotes that adversity prompts felt distress, and then greater R/S engagement is employed to soothe that felt distress; and conversely, when felt distress is low, then R/S engagement might be expected to be lower, or that engagement might serve different functions. From an attachment perspective, the R/S coping hypothesis is consistent with the safe haven function, whereby persons relate to God as a secure attachment figure to soothe felt distress, and thus relating to God can serve as an emotion regulation strategy (
Granqvist 2005). Conversely, when felt distress is low, persons may enact the secure base function of attachment relating, or alternatively, engage in non-distress proximity seeking (
Bell 2009). As noted earlier, R/S dwelling and R/S seeking can each serve R/S coping functions in response to distress (
Arrowood et al. 2022;
Bentzen 2021;
Sandage et al. 2020), and yet, R/S dwelling and R/S seeking can also serve non-coping or non-affect regulation functions. As
Jankowski and Sandage (
2014) noted about the secure base function, “rather than moving closer and seeking comfort, the individual distances in order to question and experiment with difference and change from a position of felt security” (p. 71). As for the proximity seeking function, they noted that “other than affect regulation and exploration motivations, persons relate to [the sacred] … [in a way] that nurtures and maintains ongoing connection and felt security” (p. 71). In the current study, the flourishing reported low distress. It makes sense therefore that we did not find evidence to support the R/S coping hypothesis among the flourishing, relative to the languishing and moderately healthy. That is, R/S engagement seemed to serve different functions for the flourishing.
7.1. Psychotherapy Effectiveness
Our findings are consistent with other psychotherapy effectiveness studies that employed person-centered analyses to identify diverse change trajectories. These studies include evidence of positive growth trajectories, consisting of responders who score lower on initial levels of general mental health problems (i.e., “low distress therapy responders”,
Frankfurt et al. 2016, p. 642). This group of responders, represented by our flourishing subgroup, seems consistent with the phenomenon of the “rich get richer”, first noted by
Cooper (
2008, p. 68). As Fuertes and Nutt
Williams (
2017) summarized, “clients who have higher psychological functioning and better psychological mindedness going into therapy seem to get the most out of treatment” (p. 370).
Dolev-Amit et al. (
2021) extended this observation beyond symptom improvement to gains in subjective well-being, finding evidence to support their notion that interventions “may be effective for those who already enjoy reasonable levels of wellbeing” (p. 650). Further, as they noted, the rich get richer phenomenon seems most evident among “labile variables” such as mood disorder symptoms and subjective well-being (p. 661). We used depression symptoms and general well-being outcomes, the latter measurement tending to be more strongly associated with subjective well-being than eudaimonia (
Jankowski et al. 2022c). It could also be that the rich get richer phenomenon represented a “privilege effect” among the flourishing, relative to the languishing (
Crabtree et al. 2021, p. 13). In the current study, sexual minorities were more likely to belong to the languishing, relative to the flourishing, which is consistent with the meta-analytic finding that heterosexual persons reported lower levels of mental health symptoms relative to sexual minorities (
Ross et al. 2018). This mental health disparity can be attributed to the “additional burden of the minority stress processes sexual minorities experience in relation to their socially stigmatized identity” (p. 445). As
Crabtree et al. (
2021) concluded, “the pandemic’s effects may have disproportionately affected clients with marginalised identities” (p. 2). At the same time, we recognize the need to disaggregate sexual minorities into distinct subgroups given differences in levels of mental health symptoms among sexual minority subgroups (
Ross et al. 2018).
There is also evidence of no change trajectories, or non-responders who typically score higher on initial levels of general mental health problems (e.g.,
Frankfurt et al. 2016;
Nordberg et al. 2014), relative to the low distress responders. It is also not uncommon to find subgroups consisting of clients that show deterioration, especially during the early phase of treatment (
Frankfurt et al. 2016;
Owen et al. 2015), and these clients report the highest initial levels of general mental health problems (
Owen et al. 2015). Such clients may show improvement later in treatment (
Owen et al. 2015), and it may have been that our use of three time points in the context of long-term psychodynamic treatment did not capture later treatment change that may yet occur. In fact, in another study at the same clinic as the current study sample, using different measures of symptoms and well-being assessed over five time points during an earlier measurement window, we identified small subgroups displaying later treatment change, with one subgroup showing a nonsignificant decline in well-being during the early phase of treatment (
Jankowski et al. 2022b). In addition, prior person-centered analysis of emerging adult clients at the same clinic as the current study, using different measures of symptoms and well-being, found that endorsement of life stressors increased the likelihood of no change for some clients, and for others, endorsement of life stressors predicted deterioration (
Jankowski et al. 2021a). Life stressors that were found to significantly predict latent transitions included the death of an important person, serious problem with someone, not enough support or understanding from important people, work problems, and poor general physical health (
Jankowski et al. 2021a). In the current study, more negative COVID-19 impact ratings were associated with greater likelihood of belonging to the languishing subgroup, relative to the moderately healthy, when R/S dwelling and seeking were high. The latter suggests that the languishing experienced R/S coping as insufficient or ineffective in the face of pandemic stress, which is also consistent with their reports of greater levels of R/S struggles.
7.2. Practical Implications
Practical implications based on our findings highlight the need for R/S diversity-sensitive treatment, grounded in the judicious assessment of R/S and COVID-19 impact before integrating R/S into treatment. A recent meta-analysis found that the integration of R/S content into treatment was effective at reducing symptoms, and equally so relative to standard psychotherapy, whereas R/S-integrated psychotherapy was more effective at improving R/S dwelling-related outcomes and maladaptive relating to the sacred (
Captari et al. 2018).
Captari et al. (
2018) offered guidelines for integrating R/S into psychotherapy consistent with R/S diversity-sensitive treatment. R/S diversity-sensitive treatment requires the clinician to practice humility, with particular awareness of personal biases about R/S (
Captari et al. 2018). We suggest that bias can lead clinicians in rose-colored or skeptical directions in terms of the role of R/S in mental health treatment. Our results show complex patterns among R/S dimensions and their associations with change during treatment, and this necessitates a rather nuanced clinical assessment of clients’ particular R/S profiles and how those might be interacting with situational stressors and developmental transitions. In addition, R/S diversity-sensitive treatment will simultaneously “consider intersectionality with other dimensions of diversity” (p. 1949) and the potential challenges for non-dominant groups in accessing affirmative R/S resources. R/S diversity-sensitive treatment also focuses on the different ways R/S traditions conceptualize and promote well-being (
Tomlinson et al. 2021). In fact, central to the RSM and R/S diversity-sensitive treatment is the adoption of an emic perspective, that is, a bottom-up, contextual approach to understanding clients’ R/S that serves as a foundation for assessment and intervention (
Sandage et al. 2020).
Pomerville et al. (
2016) referred to this emic perspective as a process of “indigenizing psychotherapy” (p. 1034).
Further, as noted by
Crabtree et al. (
2021), “psychotherapy clients present as heterogeneous subgroups, and more nuanced conceptualisations of their experiences are necessary for effective treatment planning” (p. 2). We suggest that the pandemic creates a challenging context for the integration of R/S into treatment, and as our literature review and our findings show, R/S dimensions can be complexly related to perceptions about the COVID-19 pandemic and its impact on individuals’ life functioning, and in turn, the lack of progress during treatment. Crabtree et al. employed cross-sectional person-centered analysis on a subset of the clients from the current study sample, and found that qualitative responses among the high symptom and lower well-being subgroups suggested coping responses consisting of apathy, passivity, and a lack of agency. Interventions with these clients might therefore explicitly seek to foster a greater sense of agency (
Crabtree et al. 2021). In contrast, subgroups reporting lower symptoms and greater well-being, such as our flourishing subgroup, seemed to engage in meaning-based coping and themes of finding benefits associated with the pandemic amidst the challenges. Careful assessment of the role of R/S in clients’ lives is needed, including the different dimensions of R/S, with particular attention to R/S as a potential risk and protective factor. Further, given the comparable effects among R/S integrative and standard treatments (
Captari et al. 2018), integrating R/S into treatment may not be needed if the focus of treatment is on reducing symptoms and promoting well-being. In fact, as our findings for the flourishing suggested, R/S coping may not be relevant for certain clients, and alternative means of support and meaning making may foster growth apart from explicit R/S integrative efforts. However, if a client is interested in R/S integration, or the clinician and client collaboratively discern that religiousness/spirituality may be part of the presenting problem or inhibiting psychotherapeutic change, thereby making religiousness/spirituality clinically indicated, then proceeding on the basis of careful R/S assessment and “follow[ing] the client’s lead” may be useful (
Captari et al. 2018, p. 1950).
7.3. Limitations and Future Directions
The present findings are limited by data from an outpatient clinic in the Northeastern US using data from three time points over six months during the pandemic. Research is needed in other geographic and treatment contexts, and with a longer duration of longitudinal measurement, which could allow tracking non-linear trajectories of change. Compared to national surveys of outpatient mental health clients in the US (
Oxhandler et al. 2018,
2021), our sample had higher percentages of sexual and gender minorities, agnostic, and Asian identifying clients, and lower percentages of Hispanic, African American/Black, Jewish, and Christian identifying clients. Future research might intentionally sample certain groups to investigate the variables in this study in particular communities or in regions of the US where there might be higher levels of overall R/S engagement.
This study was also limited by the use of a single-item measure of COVID-19 impact. Future research might utilize existing multi-item measures (e.g.,
Lee 2020;
Prazeres et al. 2021), or develop a scale specific to clinical contexts, although the evolving nature of the pandemic could make scale development difficult. Future research could also benefit from examining trajectories of different symptoms other than depression. Depression tends to be the most frequently measured outcome in studies of religiousness/spirituality and mental health/well-being (
Yonker et al. 2012), with some collapsing depression, anxiety, and general distress into the outcome of distress (
Garssen et al. 2021). Further, there is evidence that self-reported levels of depression symptoms increased during the pandemic, relative to pre-pandemic levels (
Ettman et al. 2020), and yet, future research could assess generalized anxiety symptoms, or post-traumatic stress, in addition to depression.
In addition, the practice-based design in this study did not allow us to test the effect of particular psychotherapy interventions nor directly infer causal effects to the treatment. Furthermore, time 1 assessments did not always represent baseline symptoms and well-being since participants were recruited from clients already in treatment and those just beginning treatment during the measurement window for the current study. Prior research at the same clinic as the current study, using different measures of symptoms and well-being, found that pre-baseline treatment (i.e., elapsed time between the treatment start date and the initial assessment) was not associated with initial levels of depression and well-being (
Jankowski et al. 2019). Nevertheless, it is possible that pre-baseline treatment lag could have affected class membership. In addition, other structured research designs and process research techniques could be useful for identifying effective clinical strategies for clients based on their scores on multiple R/S dimensions. The focus of this study on client experiences and outcomes could also be usefully extended to clinicians and the role of R/S and other factors on their mental health and well-being. Last, interdisciplinary research in this area could usefully bring together methods from the social sciences and the humanities (e.g., religious studies, philosophy, theology, history). For example, interesting historical comparisons might be explored in religion and psychiatry movements that intensified around other social crises, such as the Great Depression (e.g.,
Capps 2009;
Hirshbein 2021). There also seem to be possibilities for the interdisciplinary integration of religion and mental health in response to the systemic challenges of the COVID-19 crisis.



{kind=link}
