Gamifying Motor Rehabilitation Therapies: Challenges and Opportunities of Immersive Technologies


Abstract
:1. Introduction
Related Work
2. Background
2.1. Recovering from Stroke and Typical Clinical Condition
2.2. Common Therapeutic Practices
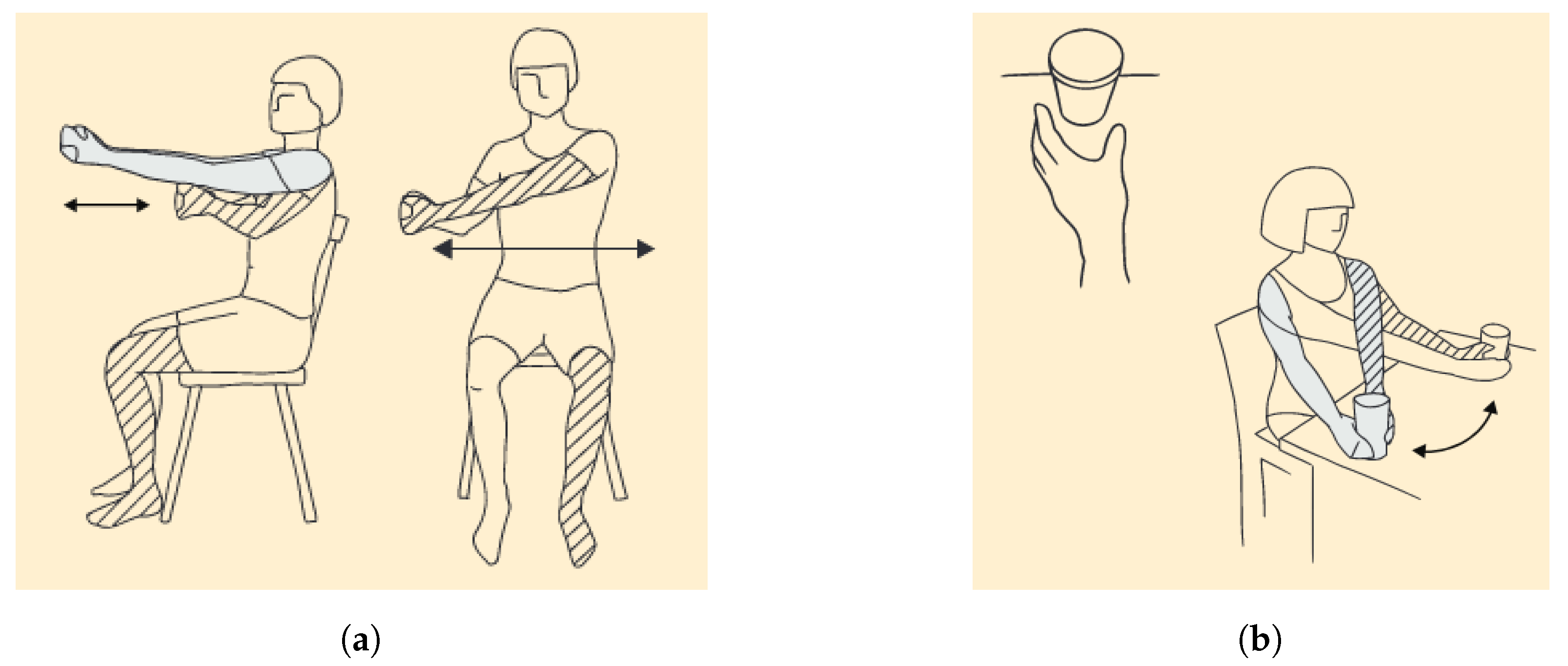
- Bilateral arm training refers to the use of the non-paretic upper limb to support movements of the affected one, while performing identical activities simultaneously.
- Mirror therapy is described as the process of placing a mirror in a certain condition that reflects the healthy limb as if it was the paretic one. Therefore, it creates the visual illusion of executing normal movements with the paretic limb.
- Occupational therapy focus on aiding patients to recover the ability to perform ADLs, such as dressing or cooking.
- Constraint-induced movement therapy (CIMT) promotes motor (re)learning of the affected upper limb by performing several repetitions of task-specific training while having the healthy one immobilized.
- Repetitive task training requires having individuals performing a large amount of repetitions for a clear functional objective within a single training session.
- Strength training consists on planning a set of resistance exercises over time to progressively improve muscle strength.
- Splinting or Orthosis techniques are based on the used of external devices as a way to improve functional movement while reducing spasticity or pain. In fact, they might be used to prevent frequent secondary complications, such as contractures.
- For changes in sensation, patients might need to retrain their senses by feeling different materials, objects, or even textures to (re)learn what they feel like.
2.3. Adherence Issues
2.4. Advantages of Virtual Reality and Game-Based Therapies
2.5. The Sensory Side of Post-Stroke Rehabilitation
3. Therapies, Games, and Gamification of Therapies: Challenges and Opportunities
3.1. How Can a Game Be Used for Rehabilitation?
- The therapeutic gestures should be perfectly comprised inside the virtual environment.
- Ability to adapt game’s mechanics based on players’ motor capabilities by some type of initial calibration.
- Monitor and record players’ performance for later evaluation.
- Adaptive and progressive change of game’s level of challenge.
- Maintain diversity of contents to accommodate different personal preferences.
- Provide meaningful cognitive and sensory stimuli during gameplay to allow players to acknowledge both correct and incorrect actions, game’s events, etc.
- Provide positive rewards and reinforcements that inspire players to keep engaged.
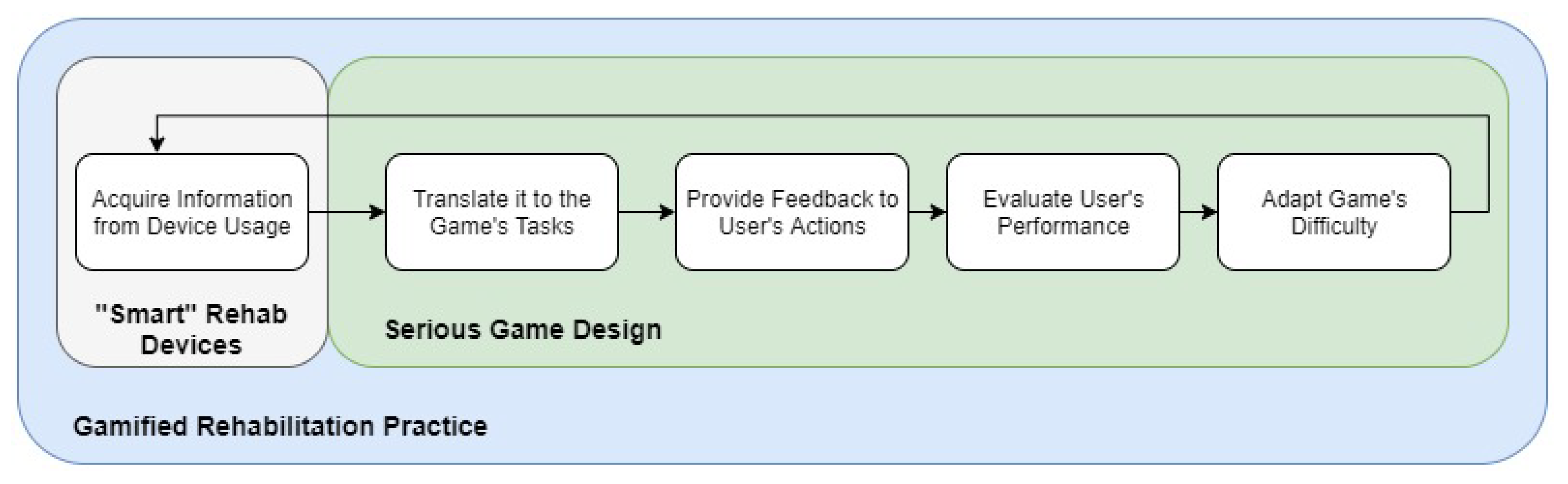
3.2. How Can a Rehabilitation Procedure Be Turned into a Game?
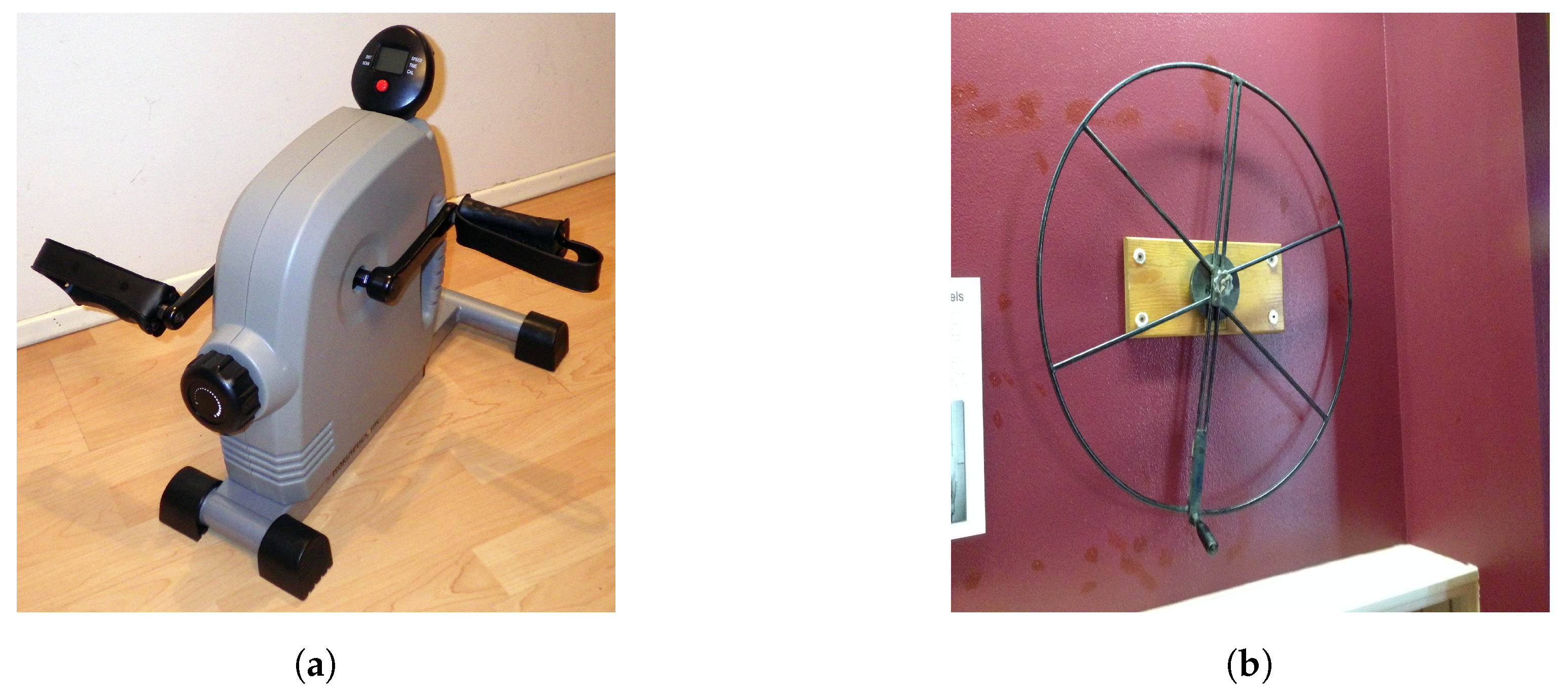
- Pedal exercise bikes—games that simulate activities like canoeing or swimming. For instance, a treasure hunt game, where players navigate in a virtual sea by using their arms or legs motion to propel a boat. The objective is to meet different checkpoints that are spread across a map, which will provide hints for the hidden treasure.
- Shoulder wheel—this physiotherapy device can be used to perform different therapeutic exercises for strengthening the shoulder muscles. When used with both hands, the executed gestures can be used for a multiplayer racing car simulator. On the other side, when using it with only one hand for the fully extension of the arm, it can be translated for a firefighter pump game. In this sense, patients would have to supply the water hose for a firefighter companion to prevent a fire.
- Shoulder Pulley T Type—simulating the flapping of a flying bird that is exploring the skies can be an interesting approach for this equipment. Moreover, for initial stages of recovery, where the range of possible movements is reduced, the expected task could be maintaining an hand glider stable while also exploring skies. To this end, the player would have to compensate possible wind flows.
4. Developing a Platform for Tele-Rehabilitation
4.1. Parameters Collected during the Playful Sessions
- Score: higher scores can be linked to higher correct responses to the demanding tasks.
- Final Level: higher game levels are certainly related to greater challenges, which require agile visuo-motor coordination and faster outcomes.
- Played Time: time plays an important role for any kind of physical exercise. Under therapeutic meanings, one can acknowledge that having longer sessions implies more repetitions of the recommended training.
- Distance Covered: measuring the distances covered by the affected limbs will in turn explain how much patients used their muscles, with the objective of strengthening them.
- Number of changes in Motion Direction: greater number of motion inversions may suggest inaccuracies in movements or that they were performed without objectives.
- Initial Amplitude of Movements: as a result of a calibration process, this metric can be considered to be an extremely important metric to understand patients’ evolution over time.
- Low scores and long played times will surely mean that patients were unable to complete the required tasks, which can lead to quick frustration and disapproval of the game.
- Long distance covered by the affected limb and short number of changes in motion direction means that individuals were most likely performing movements of wider range of amplitude, and thus being in a more advanced stage of recovery. In contrast, if short distances are covered with a high number of changes in motion direction, it means that either they are unable to perform wide gestures or they are inaccurate.
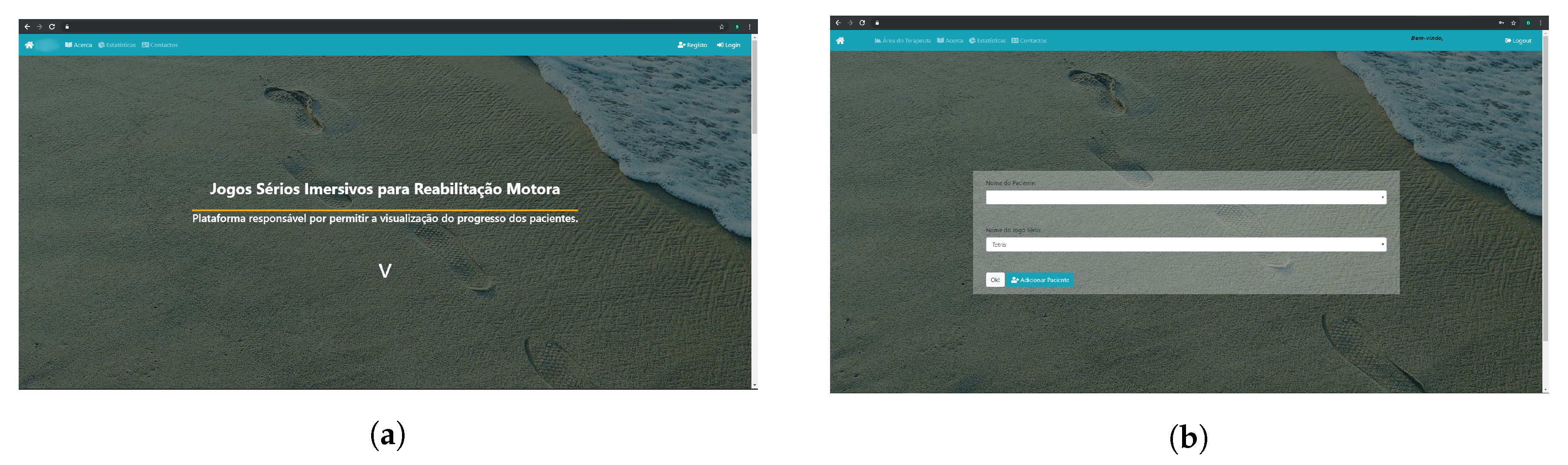
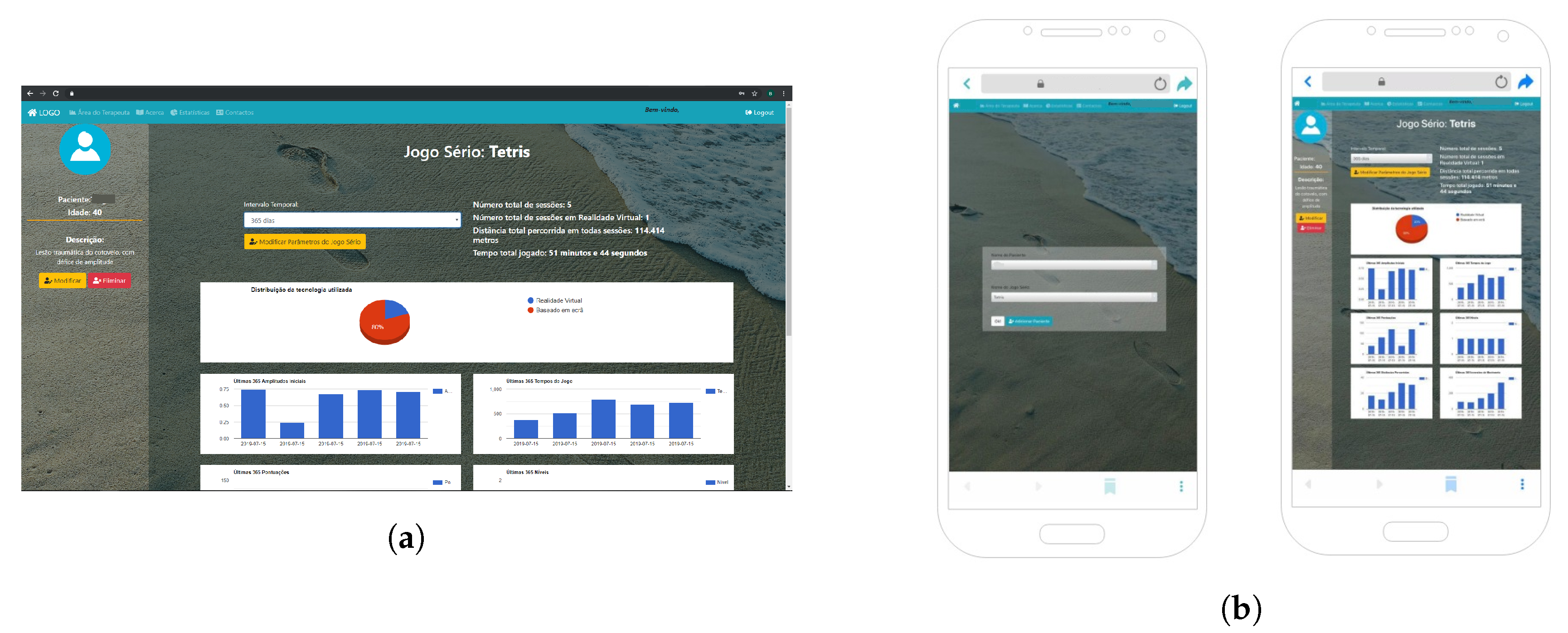
4.2. Patients’ Tracking Tool: A Back-Office for Therapists
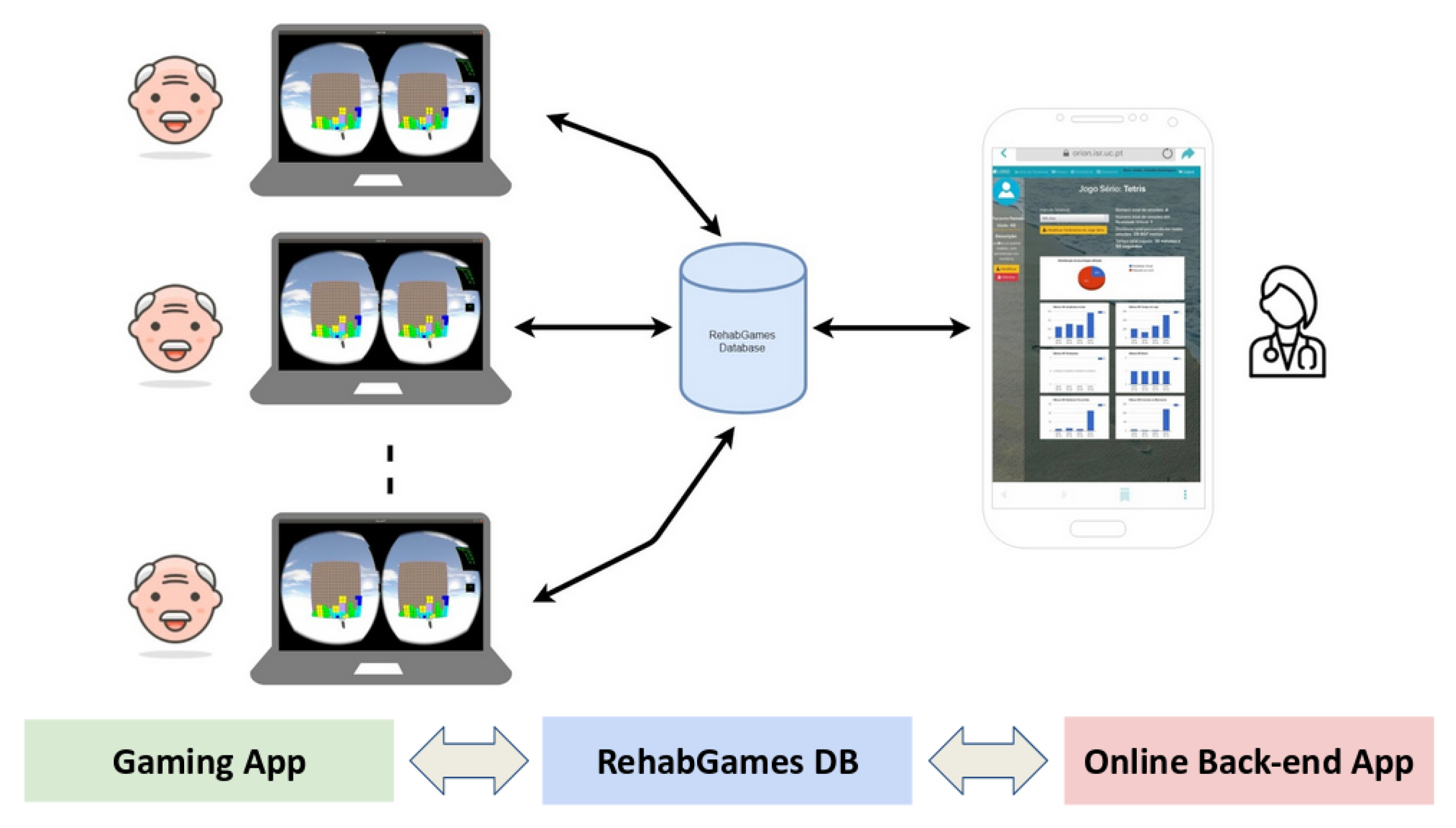
4.3. Platform Outline
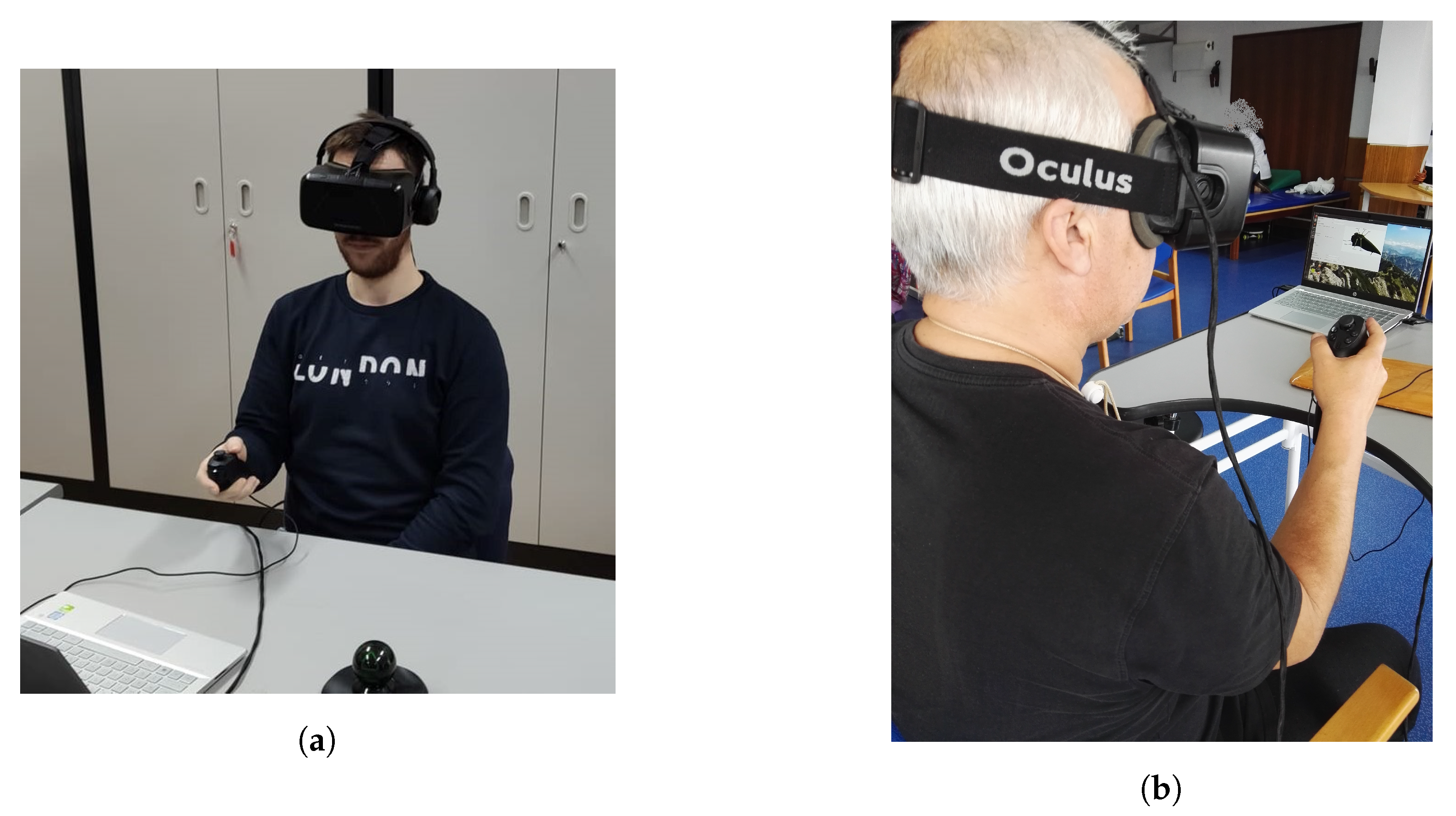
4.4. Play-Station: Set-Up Required and Currently Available Games
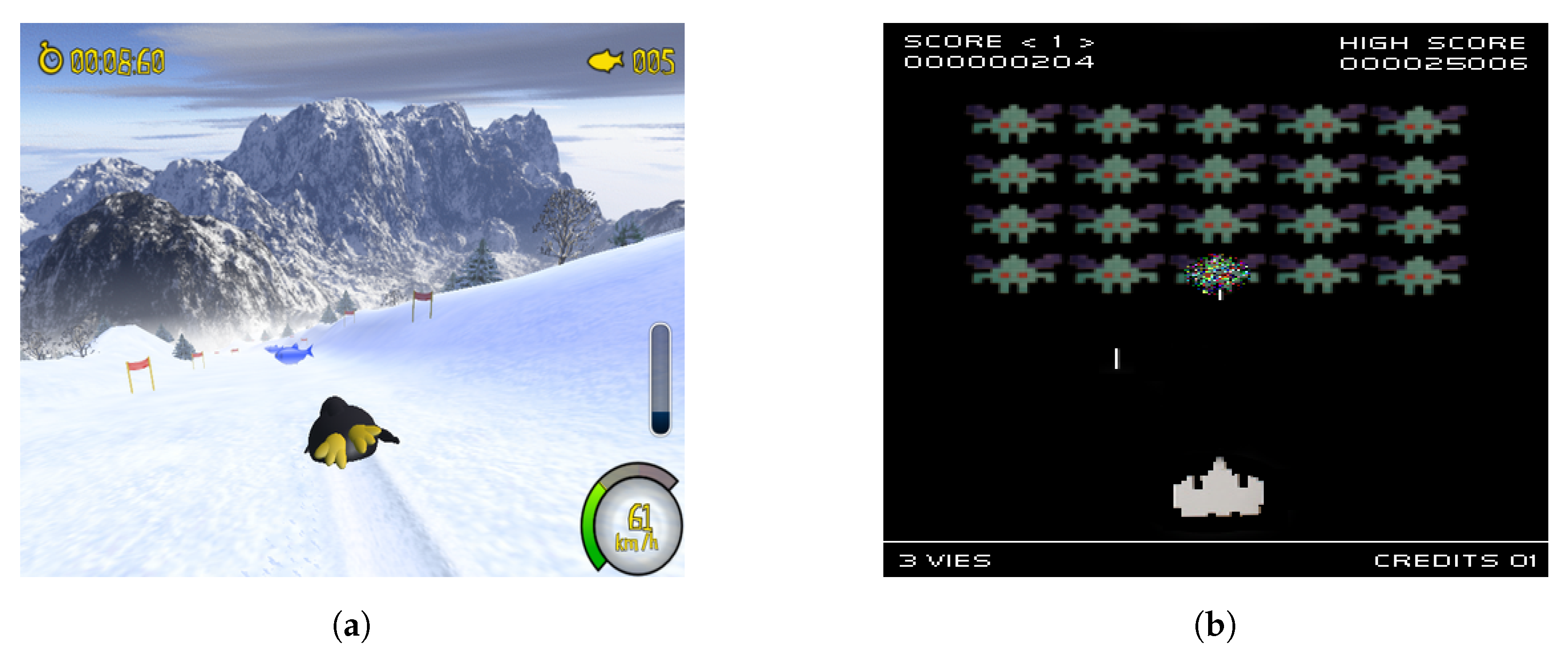
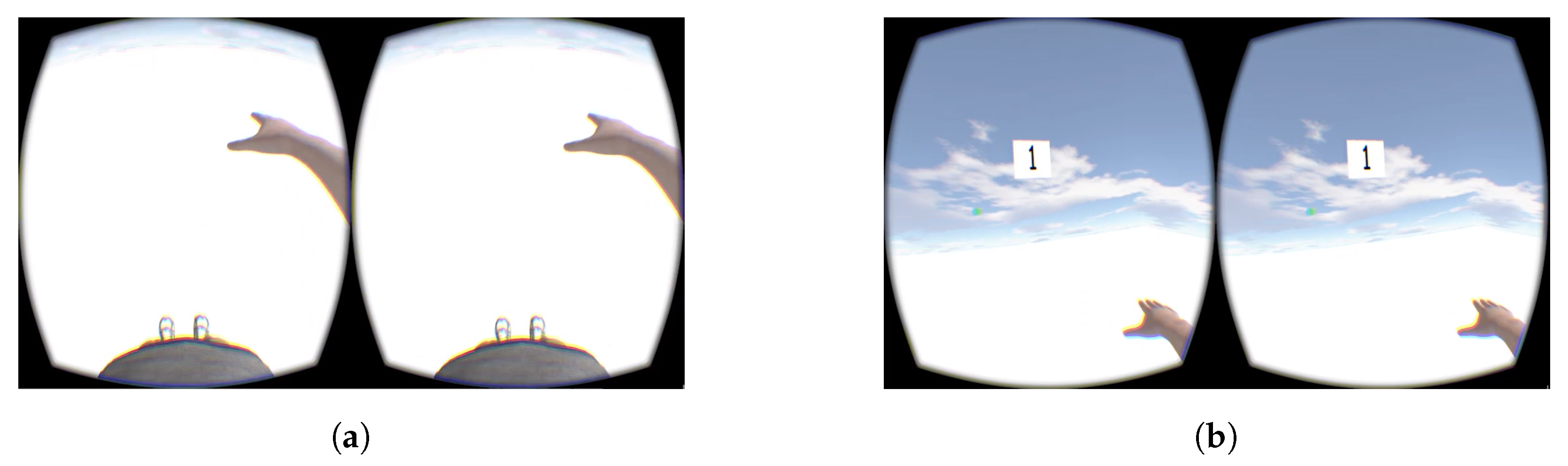
4.4.1. Game 1: Catch & Dodge
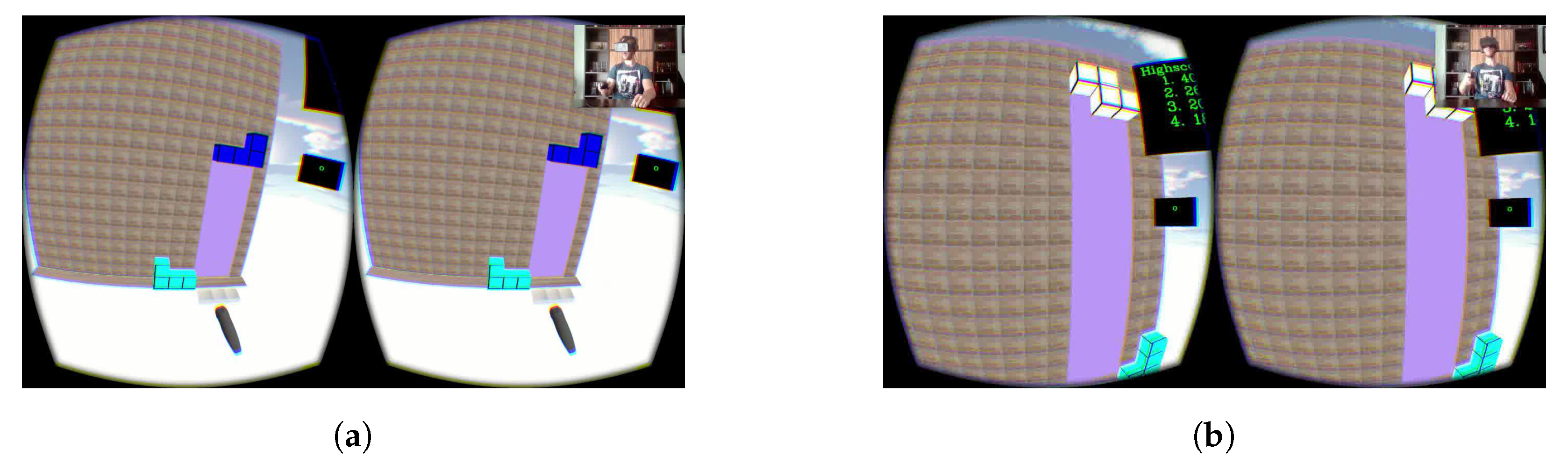
4.4.2. Game 2: Tetris4All
- Regular mode: players guide the falling tetrominoes by moving their paretic limb and rotating them if necessary. The rotation process can be achieved by either pressing a button or by rotating their wrist like they were rotating a door knob. As the score increases, the difficulty level also increases, which causes the tetrominoes to fall faster.
- Timed mode: a certain amount of time is given the player to decide the most advantageous position for the tetromino while moving/rotating it on top of the playing area, and when it runs out, the piece falls immediately. The amount of time is calculated for each patient, which means that it enables inexperienced users to have more time to decide where it should fall.
4.5. Implementation Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ADL | Activities of the Daily Living |
| BCI | Brain–Computer Interfaces |
| CIMT | Constraint-induced Movement Therapy |
| HCI | Human Computer Interaction |
| HMD | Head-Mounted Display |
| SG | Serious Game |
| UBE | Upper Body Ergometer |
| VE | Virtual Environment |
| VR | Virtual Reality |
References
- Graber, M.; Baptiste, L.; Mohr, S.; Blanc-Labarre, C.; Dupont, G.; Giroud, M.; Béjot, Y. A review of psychosocial factors and stroke: A new public health problem. Revue Neurol. 2019, 175, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Stroke Association. State of the Nation: Stroke Statistics. 2018. Available online: https://www.stroke.org.uk/sites/default/files/state_of_the_nation_2018.pdf (accessed on 15 September 2019).
- English, C.; Bowen, A.; Hébert, D.; Bernhardt, J. Rehabilitation after stroke: Evidence, practice, and new directions. In Warlow’s Stroke: Practical Management; Hankey, G.J., Macleod, M., Gorelick, P.B., Chen, C., Caprio, F.Z., Mattle, H., Eds.; Wiley Online Library: Hoboken, NJ, USA, 2019; pp. 867–877. [Google Scholar]
- Lee, M.M.; Cho, H.; Song, C.H. The mirror therapy program enhances upper-limb motor recovery and motor function in acute stroke patients. Am. J. Phys. Med. Rehabil. 2012, 91, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Barker, R.N.; Brauer, S.G. Upper limb recovery after stroke: The stroke survivors’ perspective. Disabil. Rehabil. 2005, 27, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- Seidel, P.M.P.; Seidel, G.K. Stroke rehabilitation. In Extracranial Carotid and Vertebral Artery Disease: Contemporary Management; Hans, S.S., Ed.; Springer: Cham, Switzerland, 2018; pp. 279–292. [Google Scholar] [CrossRef]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Iosa, M.; Morone, G.; Fusco, A.; Bragoni, M.; Coiro, P.; Multari, M.; Venturiero, V.; De Angelis, D.; Pratesi, L.; Paolucci, S. Seven capital devices for the future of stroke rehabilitation. Stroke Res. Treat. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Reinkensmeyer, D.J.; Pang, C.T.; Nessler, J.A.; Painter, C.C. Web-based telerehabilitation for the upper extremity after stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 102–108. [Google Scholar] [CrossRef]
- Burke, J.W.; McNeill, M.; Charles, D.; Morrow, P.; Crosbie, J.; McDonough, S. Serious games for upper limb rehabilitation following stroke. In Proceedings of the 2009 Conference in Games and Virtual Worlds for Serious Applications, Coventry, UK, 23–24 March 2009; pp. 103–110. [Google Scholar]
- Ma, M.; Bechkoum, K. Serious games for movement therapy after stroke. In Proceedings of the 2008 IEEE International Conference on Systems, Man and Cybernetics, Singapore, 12–15 October 2008; pp. 1872–1877. [Google Scholar]
- Rizzo, A.S.; Kim, G.J. A SWOT analysis of the field of virtual reality rehabilitation and therapy. Presence Teleoper. Virtual Environ. 2005, 14, 119–146. [Google Scholar] [CrossRef]
- Johansson, T.; Wild, C. Telerehabilitation in stroke care–a systematic review. J. Telemed. Telecare 2011, 17, 1–6. [Google Scholar] [CrossRef]
- Bartnicka, J.; Herrera, C.; Michnik, R.; Pavan, E.E.; Vercesi, P.; Varela-Donoso, E.; Garrido, D. The role of virtual reality and biomechanical technologies in stroke rehabilitation. In Advances in Human Factors in Training, Education, and Learning Sciences; Nazir, S., Teperi, A.M., Polak-Sopińska, A., Eds.; Springer: Cham, Switzerland, 2018; pp. 351–361. [Google Scholar]
- Jacobs, A.; Timmermans, A.; Michielsen, M.; Plaetse, M.V.; Markopoulos, P. CONTRAST: Gamification of arm-hand training for stroke survivors. In Proceedings of the CHI’13 Extended Abstracts on Human Factors in Computing Systems, Paris, France, 27 April 2013; pp. 415–420. [Google Scholar]
- Sror, L.; Levy-Tzedek, S.; Levin, M.F.; Berman, S. Low-Cost Virtual Reality System with Passive Arm Support for Stroke Rehabilitation. Available online: https://www.idiap.ch/workshop/iros2018/files/04f-rehabsystem21sept2018_iros_final.pdf (accessed on 5 September 2019).
- Aranha, R.V.; Araújo, L.V.; Monteiro, C.B.M.; Da Silva, T.D.; Nunes, F.L. Moveroffice: Virtual reality for upper limbs rehabilitation. In Proceedings of the 2016 XVIII Symposium on Virtual and Augmented Reality (SVR), Gramado, Brazil, 21–24 June 2016; pp. 160–169. [Google Scholar]
- Nordin, K.M.; Chellappan, K.; Sahathevan, R. Upper limb rehabilitation in post stroke patients: Clinical observation. In Proceedings of the 2014 IEEE Conference on Biomedical Engineering and Sciences (IECBES), Kuala Lumpur, Malaysia, 8–10 December 2014; pp. 700–704. [Google Scholar] [CrossRef]
- Adams, H.P. Principles of Cerebrovascular Disease, 1st ed.; McGraw Hill Professional: New York, NY, USA, 2007. [Google Scholar]
- Hepworth, L.R.; Rowe, F.J.; Walker, M.F.; Rockliffe, J.; Noonan, C.; Howard, C.; Currie, J. Post-stroke visual impairment: A systematic literature review of types and recovery of visual conditions. Ophthalmol. Res. Int. J. 2016, 11, 1–43. [Google Scholar] [CrossRef]
- Julkunen, L.; Tenovuo, O.; Jääskeläinen, S.; Hämäläinen, H. Rehabilitation of chronic post-stroke visual field defect with computer-assisted training. Restor. Neurol. Neurosci. 2003, 21, 19–28. [Google Scholar]
- Rose, F.D.; Brooks, B.M.; Rizzo, A.A. Virtual reality in brain damage rehabilitation. Cyberpsychol. Behav. 2005, 8, 241–262. [Google Scholar] [CrossRef]
- Zilli, A. Motor Re-Education of Hemiplegic Patients. Acta Clin. Belg. 1977, 32, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.M.; Johansen-Berg, H.; Ward, N.; Kennedy, N.C.; Chandler, E.; Weir, C.J.; Rothwell, J.; Wing, A.M.; Grey, M.J.; Barton, G.; et al. Functional strength training and movement performance therapy for upper limb recovery early poststroke—Efficacy, neural correlates, predictive markers, and cost-effectiveness: FAST-INdiCATE Trial. Front. Neurol. 2018, 8, 733. [Google Scholar] [CrossRef] [PubMed]
- Rego, P.; Moreira, P.M.; Reis, L.P. Serious games for rehabilitation: A survey and a classification towards a taxonomy. In Proceedings of the 5th Iberian Conference on Information Systems and Technologies, Santiago de Compostela, Spain, 16–19 June 2010; pp. 1–6. [Google Scholar]
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst. Rev. 2016, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oujamaa, L.; Relave, I.; Froger, J.; Mottet, D.; Pelissier, J.Y. Rehabilitation of arm function after stroke. Literature review. Ann. Phys. Rehabil. Med. 2009, 52, 269–293. [Google Scholar] [CrossRef] [PubMed]
- Sucar, L.E.; Orihuela-Espina, F.; Velazquez, R.L.; Reinkensmeyer, D.J.; Leder, R.; Hernández-Franco, J. Gesture therapy: An upper limb virtual reality-based motor rehabilitation platform. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 634–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, K.L.; Hepworth, L.R.; Rowe, F.J. The treatment methods for post-stroke visual impairment: A systematic review. Brain Behav. 2017, 7, e00682. [Google Scholar] [CrossRef] [Green Version]
- Young, M.F.; Slota, S.; Cutter, A.B.; Jalette, G.; Mullin, G.; Lai, B.; Simeoni, Z.; Tran, M.; Yukhymenko, M. Our princess is in another castle: A review of trends in serious gaming for education. Rev. Educ. Res. 2012, 82, 61–89. [Google Scholar] [CrossRef] [Green Version]
- Graafland, M.; Schraagen, J.M.; Schijven, M.P. Systematic review of serious games for medical education and surgical skills training. Br. J. Surg. 2012, 99, 1322–1330. [Google Scholar] [CrossRef]
- McCallum, S. Gamification and Serious Games for Personalized Health; pHealth: Quezon, Philippines, 2012; pp. 85–96. [Google Scholar]
- Kato, P.M. Video games in health care: Closing the gap. Rev. Gen. Psychol. 2010, 14, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Johnson, W.L.; Wang, N.; Wu, S. Experience with serious games for learning foreign languages and cultures. In Proceedings of the SimTecT 2007 Conference, Brisbane, Australia, 4–7 June 2007. [Google Scholar]
- Smith, R. The long history of gaming in military training. Simul. Gaming 2010, 41, 6–19. [Google Scholar] [CrossRef]
- Lafond, I.; Qiu, Q.; Adamovich, S.V. Design of a customized virtual reality simulation for retraining upper extremities after stroke. In Proceedings of the 2010 IEEE 36th Annual Northeast Bioengineering Conference (NEBEC), New York, NY, USA, 26–28 March 2010; pp. 1–2. [Google Scholar] [CrossRef]
- Bartolomé, N.A.; Zorrilla, A.M.; Zapirain, B.G. Can game-based therapies be trusted? Is game-based education effective? A systematic review of the Serious Games for health and education. In Proceedings of the 16th International Conference on Computer Games (CGAMES), Louisville, KY, USA, 27–30 July 2011; pp. 275–282. [Google Scholar]
- Lee, M.M.; Lee, K.J.; Song, C.H. Game-based virtual reality canoe paddling training to improve postural balance and upper extremity function: A preliminary randomized controlled study of 30 patients with subacute stroke. Med. Sci. Monit. 2018, 24, 2590. [Google Scholar] [CrossRef] [PubMed]
- Bolognini, N.; Russo, C.; Edwards, D.J. The sensory side of post-stroke motor rehabilitation. Restor. Neurol. Neurosci. 2016, 34, 571–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turville, M.L.; Cahill, L.S.; Matyas, T.A.; Blennerhassett, J.M.; Carey, L.M. The effectiveness of somatosensory retraining for improving sensory function in the arm following stroke: A systematic review. Clin. Rehabil. 2019, 33, 834–846. [Google Scholar] [CrossRef]
- Dimyan, M.A.; Cohen, L.G. Neuroplasticity in the context of motor rehabilitation after stroke. Nat. Rev. Neurol. 2011, 7, 76. [Google Scholar] [CrossRef]
- Cramer, S.C.; Riley, J.D. Neuroplasticity and brain repair after stroke. Curr. Opin. Neurol. 2008, 21, 76–82. [Google Scholar] [CrossRef]
- Hordacre, B.; Moezzi, B.; Ridding, M.C. Neuroplasticity and network connectivity of the motor cortex following stroke: A transcranial direct current stimulation study. Hum. Brain Mapp. 2018, 39, 3326–3339. [Google Scholar] [CrossRef] [Green Version]
- Carey, L.; Walsh, A.; Adikari, A.; Goodin, P.; Alahakoon, D.; De Silva, D.; Ong, K.L.; Nilsson, M.; Boyd, L. Finding the Intersection of Neuroplasticity, Stroke Recovery, and Learning: Scope and Contributions to Stroke Rehabilitation. Neural Plast. 2019, 2019. [Google Scholar] [CrossRef]
- Margot Andrew, M.H.; Hedges, K. Your Guide to Exercise after a Stroke: A Guide for People with Stroke and Their Families. Available online: https://www.stroke.org.nz/exercise-after-stroke (accessed on 21 November 2019).
- Hung, Y.X.; Huang, P.C.; Chen, K.T.; Chu, W.C. What do stroke patients look for in game-based rehabilitation: A survey study. Medicine 2016, 95, e3032. [Google Scholar] [CrossRef]
- Khaleel, F.L.; Sahari, N.; Wook, T.S.M.T.; Ismail, A. Gamification elements for learning applications. Int. J. Adv. Sci. Eng. Inf. Technol. 2016, 6, 868–874. [Google Scholar] [CrossRef]
- Ferreira, B.; Lourenço, J.; Menezes, P. A Serious Game for Post-Stroke Motor Rehabilitation. In Proceedings of the 2019 5th Experiment International Conference (exp. at’19), Funchal, Portugal, 12–14 June 2019; pp. 383–387. [Google Scholar]
- Ferreira, B.; Menezes, P. Immersive Serious Games for Post-Stroke Motor Rehabilitation. In Proceedings of the 2019 5th Experiment International Conference (exp. at’19), Funchal, Portugal, 12–14 June 2019; pp. 237–238. [Google Scholar]
- Sims, V.K.; Mayer, R.E. Domain specificity of spatial expertise: The case of video game players. Appl. Cogn. Psychol. 2002, 16, 97–115. [Google Scholar] [CrossRef]
- Ferreira, B.; Menezes, P. An Adaptive Virtual Reality-Based Serious Game for Therapeutic Rehabilitation. Int. J. Online Biomed. Eng. 2019. Unpublished work. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Game Element | Description |
|---|---|
| Goals/Tasks | Something that players must achieve or work towards. |
| Rules | Express how the game is supposed to be played. |
| User Levels | Encodes patient’s proficiency. |
| Feedback | For every action performed there should be an immediate game’s response of success or failure. |
| Point System | Amount of points that should be added to the overall score for each successful action. |
| Score | Total points obtained so far. |
| Leaderboards | General representation of the highest scores obtained. Allows players to compare their performances to others. |
| Time Pressure | Reducing the amount of time available to complete a task. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, B.; Menezes, P. Gamifying Motor Rehabilitation Therapies: Challenges and Opportunities of Immersive Technologies. Information 2020, 11, 88. https://doi.org/10.3390/info11020088
Ferreira B, Menezes P. Gamifying Motor Rehabilitation Therapies: Challenges and Opportunities of Immersive Technologies. Information. 2020; 11(2):88. https://doi.org/10.3390/info11020088
Chicago/Turabian StyleFerreira, Bruno, and Paulo Menezes. 2020. "Gamifying Motor Rehabilitation Therapies: Challenges and Opportunities of Immersive Technologies" Information 11, no. 2: 88. https://doi.org/10.3390/info11020088
APA StyleFerreira, B., & Menezes, P. (2020). Gamifying Motor Rehabilitation Therapies: Challenges and Opportunities of Immersive Technologies. Information, 11(2), 88. https://doi.org/10.3390/info11020088