
AI-Based Smart Sensing and AR for Gait Rehabilitation Assessment

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Related Work
2.1. Background
2.2. Technology and Physical Rehabilitation
2.3. Motivation Enhancement Systems for Physiotherapy
2.4. Smart Sensing in Healthcare
2.5. AI in Healthcare
- Activity recognition and monitoring: AI-powered activity recognition systems can automatically identify and analyze the activities of individuals in their living environment. These systems typically use sensors, cameras, or wearable devices to collect data and employ machine learning algorithms to recognize and interpret the patterns of daily living [44,45,46]. By monitoring the daily routines of individuals, AAL systems can detect unusual behaviors or changes in patterns, which may indicate health issues or potential risks, and alert caregivers or medical professionals accordingly.
- Fall detection and prevention: Falls are a significant concern for the elderly, as they can lead to severe injuries, loss of independence, and a decline in overall health. AI-based fall detection and prevention systems can analyze sensor data from wearable devices, cameras, or floor sensors to identify fall-related events and trigger alarms or notifications to caregivers or emergency services [47,48,49,49]. Furthermore, AI can also be employed to predict the risk of falling based on gait analysis, enabling the implementation of preventive measures to minimize the risk.
- Telemedicine and remote patient monitoring: AI can enhance telemedicine and remote patient monitoring by analyzing data collected from various sensors, wearable devices, and medical equipment in order to provide accurate and timely health assessments, personalized feedback, and recommendations for patients and healthcare professionals [53,54]. This enables the efficient and continuous monitoring of patients’ health, especially those with chronic conditions, reducing the need for frequent hospital visits.
2.5.1. Recurrent Neural Networks
2.5.2. Long Short-Term Networks
2.5.3. Gated Recurrent Unit Networks
2.5.4. Multilayer Perceptron Networks
3. Materials and Methods
3.1. System Architecture
3.2. Hardware Description
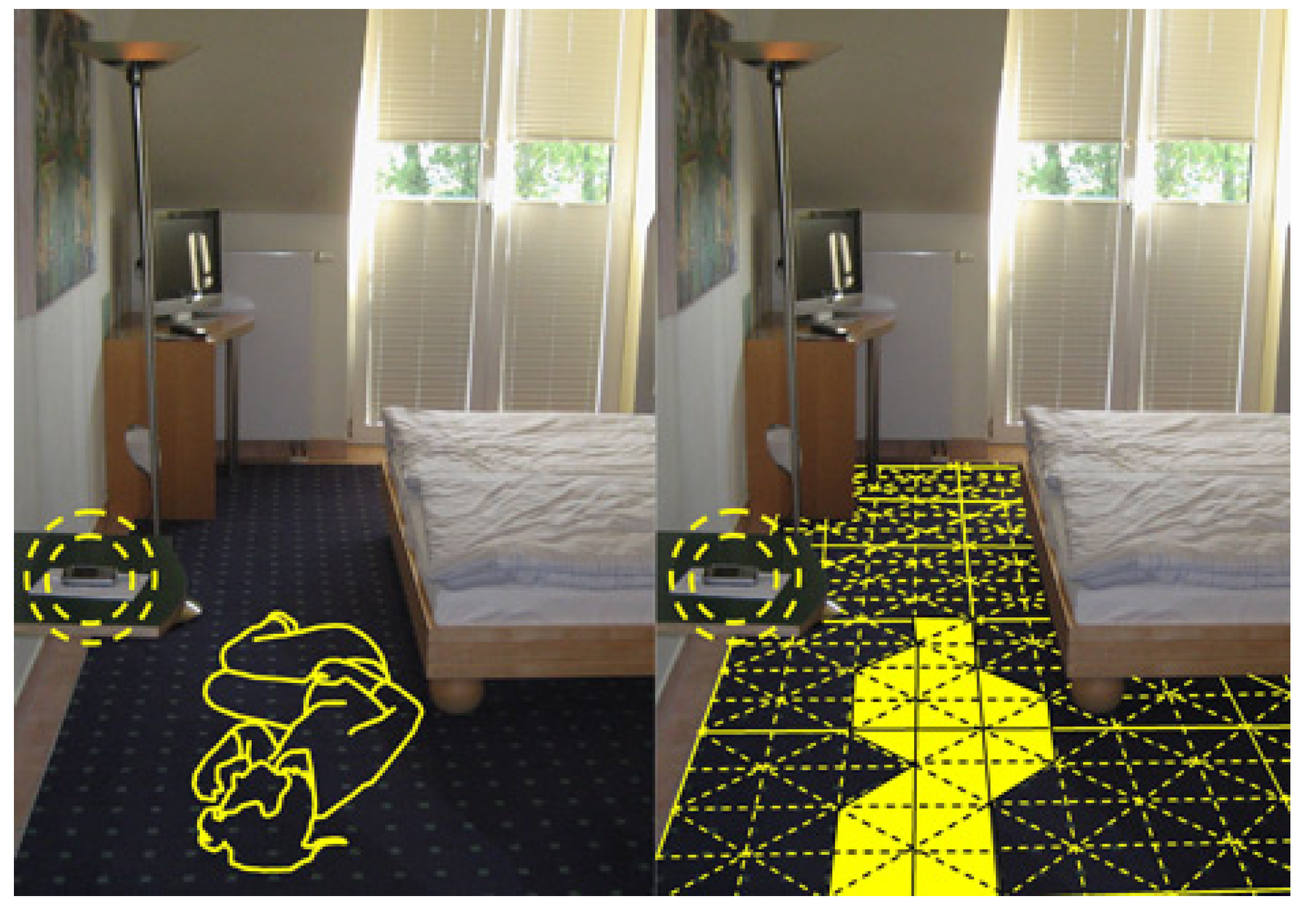
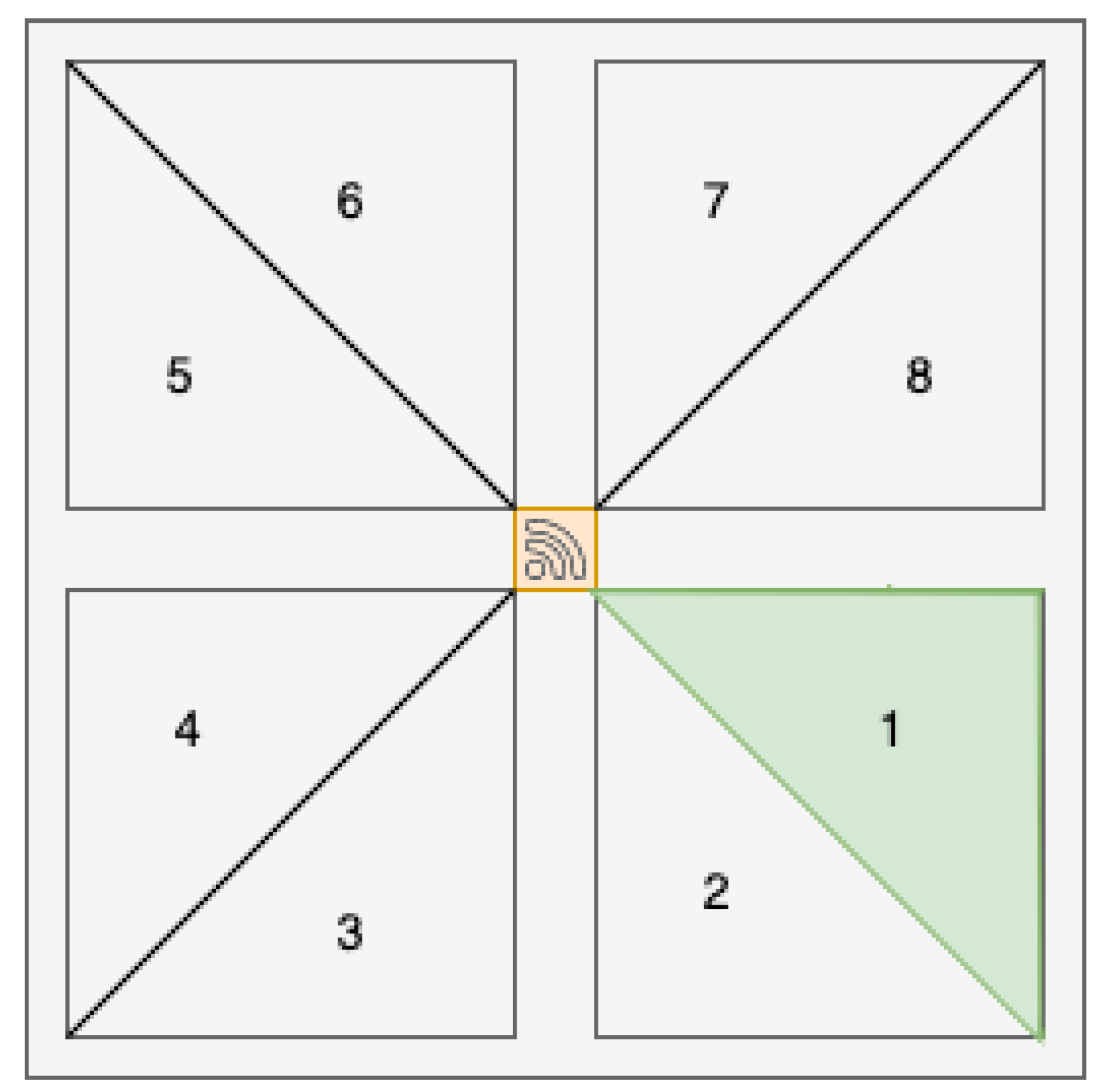
3.2.1. SensFloor®
- 1.
- Textile sensor layer: A grid of capacitive sensors is embedded within a thin, flexible textile in this layer. The sensor grid is made up of conductive fibers that have been woven into the fabric in a specific pattern to allow for precise foot position detection. The sensor grid’s size and resolution can be tailored to meet the needs of various applications.
- 2.
- SensFloor® Raspberry hat unit (Figure 8): This unit collects data from the textile sensor layer and communicates with external devices. The control unit contains analog-to-digital converters (ADCs) that convert capacitance signals into digital data. It also includes a microcontroller for data processing and a communication interface for sending processed data to external devices like the Raspberry Pi in our setup.
- 3.
- Raspberry Pi 3: The Raspberry Pi 3 is a credit card-sized single-board computer with a 1.2 GHz quad-core ARM Cortex-A53 CPU, 1GB LPDDR2 RAM, and a Broadcom VideoCore IV GPU. With a dual-band 802.11 n wireless LAN and Bluetooth 4.1 support, it has built-in wireless and Bluetooth connectivity. Four USB 2.0 ports, a full-size HDMI port, a 3.5 mm audio jack, a microSD card slot for storage, and a 40-pin GPIO header for connecting to other hardware are included on the board. The board is powered by a micro-USB port and is compatible with a variety of operating systems, including Linux distributions and Windows 10 IoT Core. In addition to camera and display interfaces, the Raspberry Pi 3 has a CSI camera port and a DSI display port for connecting to cameras and displays. Due to its small size, low cost, and extensive feature set, it is a popular choice for hobbyist projects, educational initiatives, and commercial applications.
- 4.
- Power supply: To ensure optimal performance, the SensFloor® system requires a stable power source. The power supply is typically connected to the control unit and supplies the voltage and current required to run the system.
- 5.
- Protective flooring: A high-density fiberboard (HDF) floor with AC5 resistance was used to guarantee durability and user safety. As demonstrated in Figure 9 the laminated floor was placed above the e-textile layer of SensFloor®. The laminated floor has an AC5 rating, indicating that the flooring is intended for heavy industrial use, with excellent durability and wear and tear resistance; while users engage with the system, this protective layer ensures that the SensFloor® textile sensor layer remains secure and functional. The 8mm HDF floor with AC5 resistance is an ideal protective surface for the SensFloor® system because it not only provides the required protection but also enables the capacitive sensors to detect foot positions and movements accurately and without hindrance. Due to the combination of these materials, the smart floor can effectively gather data for gait and posture analysis in a variety of settings, including residential and clinical settings.
3.2.2. Motion Sensing System
- 1.
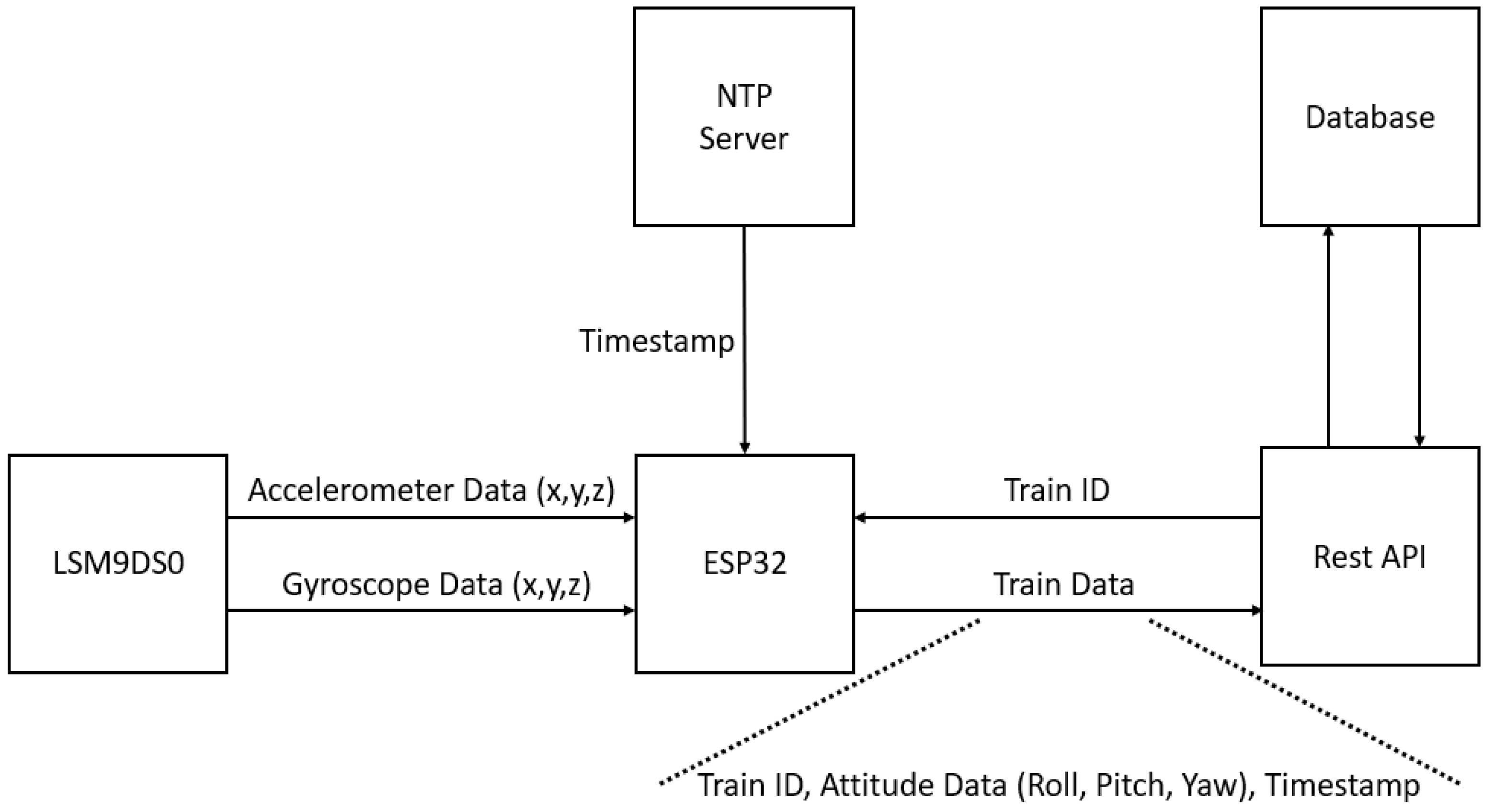
- LSM9DS0 IMU Sensor: The LSM9DS0 is a 9-axis motion sensor module that incorporates in a single package a 3-axis accelerometer, a 3-axis gyroscope, and a 3-axis magnetometer. Accelerometers measure linear acceleration, gyroscopes measure angular velocity, and magnetometers measure magnetic field strength. By combining these three kinds of measurements, the LSM9DS0 can provide precise information regarding an object’s orientation and movement in three-dimensional space. The LSM9DS0 communicates with an ESP32 microcontroller via an I2C interface, and each of its sensors has a programmable full-scale range.
- 2.
- ESP32 Microcontroller: The ESP32 microcontroller is a 32-bit, dual-core processor that operates at speeds up to 240 MHz. It has built-in Wi-Fi and Bluetooth connectivity as well as a variety of other peripherals, such as GPIOs, UARTs, I2C, SPI, ADC, and DAC. Also included on the ESP32’s onboard memory are 520 KB of SRAM and 4 MB of flash memory. For the purposes of this project, the ESP32 is responsible for processing the IMU data, inserting timestamps, and transmitting the data to the database via HTTP protocol.
- 3.
- Battery: The wearable module is powered by an 850 mAh Li-Po battery, providing approximately 3.5 h of continuous measurements.
- 4.
- Charging Module: The adaptation of a powerbank module enables the battery to be charged and the operating voltage to be set to 5 V.
3.3. Software Description
- 1.
- The healthcare professional selects the level for the user.
- 2.
- The user receives a notification and visualizes the path and its position in real-time on a monitor or tv.
- 3.
- User finishes the session and can visualize is score on the application.
- 1.
- Mobile application uploads data to Firebase: The patient registers in the application, and their registration data is sent to Firebase’s cloud database (Cloud Firestore). The user is able to update their profile data and save it in the database. An optional profile picture can also be uploaded by the user, and will be stored in the Firebase storage. In addition, the patient can also register several personal physical measures, such as their weight, height, blood pressure and glucose level.
- 2.
- Mobile application retrieves data from Firebase: By sending their register and profile data to the cloud database, when the user accesses the application, it will automatically get the saved data (and optional profile picture from the Firebase Storage). If the user has any exams/medication prescribed by a healthcare professional, the files are loaded from the Firebase Storage and are shown in the mobile application; for this specific feature, a timeline-like interface was developed to ease the user’s point of view.
- 3.
- Web application uploads data to Firebase: Similarly to the mobile application, healthcare professionals can register in the web application, and their registration data is saved to Cloud Firestore. Then, it is possible for professionals to upload exam/medication files to patients; these files are then saved in the Firebase storage and are accessible in the patients’ application almost immediately. It is worth pointing out that when a healthcare professional prescribes any file, their profile information is aggregated to it, so that the patient knows who prescribed it and when.
- 4.
- Web application retrieves data from Firebase: After loading, the web application retrieves a list of all registered users from Firebase and offers the possibility to check what exams/medication each one has, keeping track of each patient’s medical history. Furthermore, the measurements users send to the cloud database are also automatically acquired.
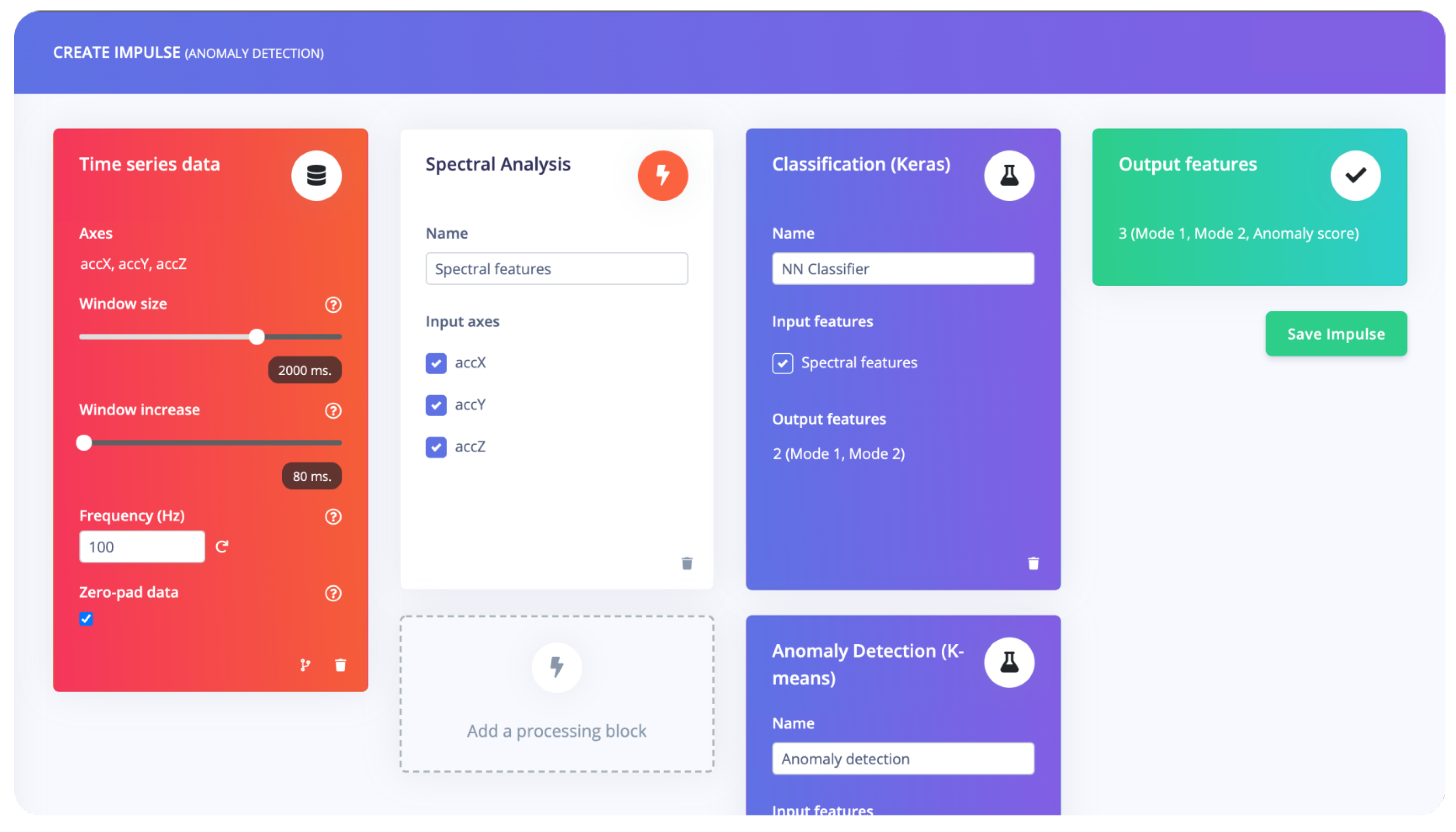
3.4. ML Description
3.4.1. Data Preprocessing
3.4.2. Feature Extraction
3.4.3. Model Selection and Training
- Class 1 is associated with an abnormal gait pattern, indicating a deviation from the expected or typical gait. This class represents instances where individuals exhibit significant deviations in their walking pattern, potentially indicating a gait impairment or dysfunction.
- Class 2 is assigned to a less-abnormal gait pattern. It represents instances where individuals demonstrate some deviations from the optimal gait but to a lesser extent compared to Class 1. This class may include individuals with mild gait abnormalities or those in the early stages of recovery from a gait-related condition.
- Last, Class 3 represents the optimal gait pattern. It represents instances where individuals exhibit a normal, healthy gait without significant deviations or abnormalities. This class serves as a reference point to compare against the other classes and provides a benchmark for the ideal gait pattern.
3.4.4. Model Evaluation and Optimization
3.4.5. Deployment and Monitoring
4. Results and Discussion
4.1. Participant Selection
4.2. Experimental Protocol
4.3. Preliminary Assessment
4.4. ML Application
Performance Evaluation
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ADAM | Adaptive Moment Estimation |
| ALL | Ambient Assisted Living |
| ANN | Artificial Neural Network |
| AR | Augmented Reality |
| DL | Deep Learning |
| ECG | Electrocardiogram |
| FBG | Fiber Bragg Gratings |
| GRU | Gated Recurrent Unit Networks |
| HDF | High-density fiberboard |
| HRV | Heart Rate Variability |
| LSTM | Long-Short Term Memory |
| ML | Machine Learning |
| MR | Mixed Reality |
| PPG | Photoplethysmography |
| RMSE | Root Mean Square Error |
| RNN | Recurrent Neural Networks |
| MLP | Multi-Layer Perceptron |
| VR | Virtual Reality |
| IMU | Inertial Measurement Unit |
| IoT | Internet of Things |
References
- Elhoseny, M.; Ramírez-González, G.; Abu-Elnasr, O.M.; Shawkat, S.A.; Arunkumar, N.; Farouk, A. Secure Medical Data Transmission Model for IoT-Based Healthcare Systems. IEEE Access 2018, 6, 20596–20608. [Google Scholar] [CrossRef]
- Mimi, M.; Tang, S.K.; Wan, V.T.; Vong, S.K. The effectiveness of physical exercise training in pain, mobility, and psychological well-being of older persons living in nursing homes. Pain Manag. Nurs. 2014, 15, 778–788. [Google Scholar]
- Fan, Y.J.; Yin, Y.H.; Da Xu, L.; Zeng, Y.; Wu, F. IoT-based smart rehabilitation system. IEEE Trans. Ind. Inform. 2014, 10, 1568–1577. [Google Scholar]
- Shine, K.I. Technology and health. Technol. Soc. 2004, 26, 137–148. [Google Scholar] [CrossRef]
- Postolache, O.; Monge, J.; Alexandre, R.; Geman, O.; Jin, Y.; Postolache, G. Virtual Reality and Augmented Reality Technologies for Smart Physical Rehabilitation. In Smart Sensors, Measurement and Instrumentation; Springer: Berlin/Heidelberg, Germany, 2021; Volume 39, pp. 155–180. [Google Scholar] [CrossRef]
- Spencer, B.F.; Ruiz-Sandoval, M.E.; Kurata, N. Smart sensing technology: Opportunities and challenges. Struct. Control Health Monit. 2004, 11, 349–368. [Google Scholar] [CrossRef]
- Formica, D.; Schena, E. Smart Sensors for Healthcare and Medical Applications. Sensors 2021, 21, 543. [Google Scholar] [CrossRef]
- Eysenbach, G. What is e-health? J. Med Internet Res. 2001, 3, e20. [Google Scholar] [CrossRef]
- Hammen, C. Stress and Depression. Annu. Rev. Clin. Psychol. 2005, 1, 293–319. [Google Scholar] [CrossRef] [Green Version]
- Maclean, N.; Pound, P. Discussion. Soc. Sci. Med. 2000, 50, 495–506. [Google Scholar] [CrossRef]
- Jin, Y.; Monge, J.; Postolache, O.; Niu, W. Augmented Reality with Application in Physical Rehabilitation. In Proceedings of the 2019 International Conference on Sensing and Instrumentation in IoT Era (ISSI), Lisbon, Portugal, 29–30 August 2019; Volume 8, pp. 1–6. [Google Scholar] [CrossRef]
- Monge, J.; Postolache, O. Augmented Reality and Smart Sensors for Physical Rehabilitation. In Proceedings of the EPE 2018—10th International Conference and Expositions on Electrical Furthermore, Power Engineering, Iasi, Romania, 18–19 October 2018. [Google Scholar] [CrossRef]
- Hamet, P.; Tremblay, J. Artificial intelligence in medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef]
- Gunning, D.; Stefik, M.; Choi, J.; Miller, T.; Stumpf, S.; Yang, G.Z. XAI—Explainable artificial intelligence. Sci. Robot. 2019, 4, hleaay7120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohr, A.; Memarzadeh, K. The rise of artificial intelligence in healthcare applications. In Artificial Intelligence in Healthcare; Elsevier: Amsterdam, The Netherlands, 2020; pp. 25–60. [Google Scholar] [CrossRef]
- Gao, X.; Alimoradi, S.; Chen, J.; Hu, Y.; Tang, S. Assistance from the Ambient Intelligence: Cyber-physical system applications in smart buildings for cognitively declined occupants. Eng. Appl. Artif. Intell. 2023, 123, 106431. [Google Scholar] [CrossRef]
- Rintala, A.; Päivärinne, V.; Hakala, S.; Paltamaa, J.; Heinonen, A.; Karvanen, J.; Sjögren, T. Effectiveness of Technology-Based Distance Physical Rehabilitation Interventions for Improving Physical Functioning in Stroke: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2019, 100, 1339–1358. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.C.; Suryadevara, N.K.; Nag, A. Wearable sensors for healthcare: Fabrication to application. Sensors 2022, 22, 5137. [Google Scholar] [CrossRef] [PubMed]
- Lauterbach, C.; Steinhage, A.; Techmer, A. A large-area sensor system underneath the floor for ambient assisted living applications. In Pervasive and Mobile Sensing and Computing for Healthcare; Springer: Berlin/Heidelberg, Germany, 2013; pp. 69–87. [Google Scholar]
- Kern, F.; Winter, C.; Gall, D.; Käthner, I.; Pauli, P.; Latoschik, M.E. Immersive virtual reality and gamification within procedurally generated environments to increase motivation during gait rehabilitation. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 500–509. [Google Scholar]
- Tamayo-Serrano, P.; Garbaya, S.; Bouakaz, S.; Blazevic, P. A game-based rehabilitation therapy for post-stroke patients: An approach for improving patient motivation and engagement. IEEE Syst. Man, Cybern. Mag. 2020, 6, 54–62. [Google Scholar] [CrossRef]
- Zhang, B.; Li, D.; Liu, Y.; Wang, J.; Xiao, Q. Virtual reality for limb motor function, balance, gait, cognition and daily function of stroke patients: A systematic review and meta-analysis. J. Adv. Nurs. 2021, 77, 3255–3273. [Google Scholar] [CrossRef]
- Jin, Y. Augmented Reality System with Application in Physical Rehabilitation. Ph.D. Thesis, Iscte—University Institute of Lisbon, Lisboa, Portugal, 2019. [Google Scholar]
- Postolache, O.; Teixeira, L.; Cordeiro, J.; Lima, L.; Arriaga, P.; Rodrigues, M.; Girão, P. Tailored virtual reality for smart physiotherapy. In Proceedings of the 2019 11th International Symposium on Advanced Topics in Electrical Engineering (ATEE), Bucharest, Romania, 28–30 March 2019; pp. 1–6. [Google Scholar]
- Alexandre, R.; Postolache, O.; Girão, P.S. Physical rehabilitation based on smart wearable and virtual reality serious game. In Proceedings of the 2019 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Auckland, New Zealand, 20–23 May 2019; pp. 1–6. [Google Scholar]
- Gumaa, M.; Rehan Youssef, A. Is Virtual Reality Effective in Orthopedic Rehabilitation? A Systematic Review and Meta-Analysis. Phys. Ther. 2019, 99, 1304–1325. [Google Scholar] [CrossRef] [Green Version]
- Madeira, R.N.; Costa, L.; Postolache, O. PhysioMate—Pervasive physical rehabilitation based on NUI and gamification. In Proceedings of the 2014 International Conference and Exposition on Electrical and Power Engineering (EPE), Iasi, Romania, 16–18 October 2014; Volume 10, pp. 612–616. [Google Scholar] [CrossRef]
- Ma, M.; Zheng, H. Virtual Reality and Serious Games in Healthcare. In Studies in Computational Intelligence; Springer: Berlin/Heidelberg, Germany, 2011; Volume 337, pp. 169–192. [Google Scholar] [CrossRef]
- Ferreira, D.; Oliveira, R.; Postolache, O. Physical rehabilitation based on kinect serious games. In Proceedings of the 2017 Eleventh International Conference on Sensing Technology (ICST), Sydney, Australia, 4–6 December 2017; Volume 12, pp. 1–6. [Google Scholar] [CrossRef] [Green Version]
- Paredes, T.V.; Postolache, O.; Monge, J.; Girao, P.S. Gait Rehabilitation System based on Mixed Reality. In Proceedings of the 2021 Telecoms Conference (ConfTELE), Leiria, Portugal, 11–12 February 2021; Volume 2, pp. 1–6. [Google Scholar] [CrossRef]
- Vinolo Gil, M.J.; Gonzalez-Medina, G.; Lucena-Anton, D.; Perez-Cabezas, V.; Ruiz-Molinero, M.D.C.; Martín-Valero, R. Augmented Reality in Physical Therapy: Systematic Review and Meta-analysis. JMIR Serious Games 2021, 9, e30985. [Google Scholar] [CrossRef]
- Fleury, A.; Sugar, M.; Chau, T. E-textiles in Clinical Rehabilitation: A Scoping Review. Electronics 2015, 4, 173–203. [Google Scholar] [CrossRef] [Green Version]
- Pantelopoulos, A.; Bourbakis, N. A Survey on Wearable Sensor-Based Systems for Health Monitoring and Prognosis. IEEE Trans. Syst. Man Cybern. Part C Appl. Rev. 2010, 40, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Xiao, X.; Zhao, X.; Tat, T.; Bick, M.; Chen, J. Electronic textiles for wearable point-of-care systems. Chem. Rev. 2021, 122, 3259–3291. [Google Scholar] [CrossRef] [PubMed]
- Ismar, E.; Kurşun Bahadir, S.; Kalaoglu, F.; Koncar, V. Futuristic clothes: Electronic textiles and wearable technologies. Glob. Challenges 2020, 4, 1900092. [Google Scholar] [CrossRef] [Green Version]
- Abdul Razak, A.H.; Zayegh, A.; Begg, R.K.; Wahab, Y. Foot Plantar Pressure Measurement System: A Review. Sensors 2012, 12, 9884–9912. [Google Scholar] [CrossRef] [Green Version]
- Monge, J.; Postolache, O.; Alexandre, R.; Fatima Domingues, M.d.; Antunes, P.; Viegas, V. Fiber Bragg Gratings Solution for Gait Assessement. In Proceedings of the 2020 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Dubrovnik, Croatia, 25–28 May 2020; Volume 5, pp. 1–6. [Google Scholar] [CrossRef]
- Garatva, P.; Terhorst, Y.; Messner, E.M.; Karlen, W.; Pryss, R.; Baumeister, H. Smart Sensors for Health Research and Improvement; Springer: Cham, Switzerland, 2023; pp. 395–411. [Google Scholar] [CrossRef]
- Duarte, N.; Postolache, O.; Scharcanski, J. KSGphysio-Kinect serious game for physiotherapy. In Proceedings of the 2014 International Conference and Exposition on Electrical and Power Engineering (EPE), Iasi, Romania, 16–18 October 2014; pp. 606–611. [Google Scholar]
- Oudah, M.; Al-Naji, A.; Chahl, J. Hand gestures for elderly care using a microsoft Kinect. Nano Biomed. Eng 2020, 12, 197–204. [Google Scholar] [CrossRef]
- Luca, C.; Fuior, R.; Corciovă, C.; Andriţoi, D. Development of an Interactive Post-stroke Rehabilitation Tool based on Microsoft Kinect. In Proceedings of the 2019 E-Health and Bioengineering Conference (EHB), Iasi, Romania, 21–23 November 2019; pp. 1–4. [Google Scholar]
- Tseng, C.M.; Lai, C.L.; Erdenetsogt, D.; Chen, Y.F. A Microsoft Kinect based virtual rehabilitation system. In Proceedings of the 2014 International Symposium on Computer, Consumer and Control, Taichung, Taiwan, 10–12 June; pp. 934–937.
- Cocconcelli, F.; Matrella, G.; Mora, N.; Casu, I.; Vargas Godoy, D.A.; Ciampolini, P. IoT Smart Flooring Supporting Active and Healthy Lifestyles. Sensors 2023, 23, 3162. [Google Scholar] [CrossRef]
- Ordóñez, F.; Roggen, D. Deep Convolutional and LSTM Recurrent Neural Networks for Multimodal Wearable Activity Recognition. Sensors 2016, 16, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demrozi, F.; Pravadelli, G.; Bihorac, A.; Rashidi, P. Human activity recognition using inertial, physiological and environmental sensors: A comprehensive survey. IEEE Access 2020, 8, 210816–210836. [Google Scholar] [CrossRef]
- Dang, L.M.; Min, K.; Wang, H.; Piran, M.J.; Lee, C.H.; Moon, H. Sensor-based and vision-based human activity recognition: A comprehensive survey. Pattern Recognit. 2020, 108, 107561. [Google Scholar] [CrossRef]
- Igual, R.; Medrano, C.; Plaza, I. Challenges, issues and trends in fall detection systems. BioMed. Eng. OnLine 2013, 12, 66. [Google Scholar] [CrossRef] [Green Version]
- Alam, E.; Sufian, A.; Dutta, P.; Leo, M. Vision-based human fall detection systems using deep learning: A review. Comput. Biol. Med. 2022, 146, 105626. [Google Scholar] [CrossRef]
- Şengül, G.; Karakaya, M.; Misra, S.; Abayomi-Alli, O.O.; Damaševičius, R. Deep learning based fall detection using smartwatches for healthcare applications. Biomed. Signal Process. Control 2022, 71, 103242. [Google Scholar] [CrossRef]
- Cavallo, F.; Aquilano, M.; Arvati, M. An Ambient Assisted Living Approach in Designing Domiciliary Services Combined With Innovative Technologies for Patients with Alzheimer’s Disease. Am. J. Alzheimer’s Dis. Other Dementias 2015, 30, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Sai, Y.P.; Kumari, L.R. Cognitive assistant DeepNet model for detection of cardiac arrhythmia. Biomed. Signal Process. Control 2022, 71, 103221. [Google Scholar]
- Xu, W.; Ouyang, F. A systematic review of AI role in the educational system based on a proposed conceptual framework. Educ. Inf. Technol. 2022, 27, 4195–4223. [Google Scholar] [CrossRef]
- Bashshur, R.L.; Howell, J.D.; Krupinski, E.A.; Harms, K.M.; Bashshur, N.; Doarn, C.R. The Empirical Foundations of Telemedicine Interventions in Primary Care. Telemed. E-Health 2016, 22, 342–375. [Google Scholar] [CrossRef] [Green Version]
- Shaik, T.; Tao, X.; Higgins, N.; Li, L.; Gururajan, R.; Zhou, X.; Acharya, U.R. Remote patient monitoring using artificial intelligence: Current state, applications, and challenges. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2023, 13, e1485. [Google Scholar] [CrossRef]
- Sherstinsky, A. Fundamentals of Recurrent Neural Network (RNN) and Long Short-Term Memory (LSTM) network. Phys. D Nonlinear Phenom. 2020, 404, 132306. [Google Scholar] [CrossRef] [Green Version]
- Grossberg, S. Recurrent neural networks. Scholarpedia 2013, 8, 1888. [Google Scholar] [CrossRef] [Green Version]
- Pearlmutter, B.A. Learning State Space Trajectories in Recurrent Neural Networks. Neural Comput. 1989, 1, 263–269. [Google Scholar] [CrossRef]
- Wikimedia Commons. File:Recurrent Neural Network Unfold.svg—Wikimedia Commons. 2017. Available online: https://commons.wikimedia.org/wiki/File:Recurrent_neural_network_unfold.svg (accessed on 4 May 2023).
- Linus Schilpp. Phoneme Classification and Alignment through Recognition on TIMIT. Ph.D. Thesis, Institute for Anthropomatics and Robotics Interactive Systems Lab, Karlsruhe, Germany, 2021. [Google Scholar]
- Wikimedia Commons. File:Long Short-Term Memory.svg—Wikimedia Commons. 2017. Available online: https://commons.wikimedia.org/wiki/File:Long_Short-Term_Memory.svg (accessed on 4 May 2023).
- Conti, P.; Guo, M.; Manzoni, A.; Hesthaven, J.S. Multi-fidelity surrogate modeling using long short-term memory networks. Comput. Methods Appl. Mech. Eng. 2022, 404, 115811. [Google Scholar] [CrossRef]
- Van Houdt, G.; Mosquera, C.; Nápoles, G. A review on the long short-term memory model. Artif. Intell. Rev. 2020, 53, 5929–5955. [Google Scholar] [CrossRef]
- Cho, K.; van Merrienboer, B.; Gulcehre, C.; Bahdanau, D.; Bougares, F.; Schwenk, H.; Bengio, Y. Learning Phrase Representations using RNN Encoder–Decoder for Statistical Machine Translation. In Proceedings of the 2014 Conference on Empirical Methods in Natural Language Processing (EMNLP), Stroudsburg, PA, USA, 25–29 October 2014; Volume 6, pp. 1724–1734. [Google Scholar] [CrossRef]
- Wikimedia Commons. File:Gated Recurrent Unit.svg—Wikimedia Commons. 2017. Available online: https://commons.wikimedia.org/wiki/File:Gated_Recurrent_Unit.svg (accessed on 4 May 2023).
- Shewalkar, A.; Nyavanandi, D.; Ludwig, S.A. Performance Evaluation of Deep Neural Networks Applied to Speech Recognition: RNN, LSTM and GRU. J. Artif. Intell. Soft Comput. Res. 2019, 9, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Rumelhart, D.E.; Hinton, G.E.; Williams, R.J. Learning representations by back-propagating errors. Nature 1986, 323, 533–536. [Google Scholar] [CrossRef]
- SensFloor®: A Smart Floor to Detect Falls. 2015. Available online: https://www.silvereco.org/en/sensfloor-a-smart-floor-to-detect-falls/ (accessed on 1 June 2023).
- New Flooring Technology Helps Improve Outcomes at Senior Care Community. Available online: https://www.iands.design/interior-design/technology/article/10180655/new-flooring-technology-helps-improve-outcomes-at-senior-care-community (accessed on 1 June 2023).
- Lauterbach, C.; Steinhage, A.; Techmer, A. Large-area wireless sensor system based on smart textiles. In Proceedings of the International Multi-Conference on Systems, Sygnals & Devices, Chemnitz, Germany, 20–23 March 2012; Volume 3, pp. 1–2. [Google Scholar] [CrossRef]
- Santos, J.; Postolache, O.; Mendes, D. Ambient Assisted Living using Non-intrusive Smart Sensing and IoT for Gait Rehabilitation. In Proceedings of the 2022 IEEE International Conference on Metrology for Extended Reality, Artificial Intelligence and Neural Engineering (MetroXRAINE), Milano, Italy, 25–27 October 2022; pp. 489–494. [Google Scholar] [CrossRef]
- Handelman, G.S.; Kok, H.K.; Chandra, R.V.; Razavi, A.H.; Huang, S.; Brooks, M.; Lee, M.J.; Asadi, H. Peering into the black box of artificial intelligence: Evaluation metrics of machine learning methods. Am. J. Roentgenol. 2019, 212, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Keprate, A. Predicting Remaining Fatigue Life of Topside Piping Using Deep Learning. In Proceedings of the International Conference on Applied Artificial Intelligence (ICAPAI 2021), Halden, Norway, 19–21 May 2021. [Google Scholar] [CrossRef]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensing Unit | Features Extracted |
|---|---|
| LSM9DS0 | yaw, pitch, roll, |
| average, minimum, maximum, | |
| root-mean square and standard deviation | |
| SensFloor® | x, y |
| Male | Female | Total | |
|---|---|---|---|
| Participants | 7 | 9 | 15 |
| Age Range | 21–32 | 18–28 | 18–32 |
| Average Range | 26 | 23 | 25 |
| Standard Deviation of Ages | 3.34 | 3.5 | 3.77 |
| Hyperparameter | Value |
|---|---|
| Epochs | 100 |
| Optimizer | ADAM |
| Loss | Sparse Categorical Cross Entropy |
| Initial LR | 0.0001 |
| Batch size | 512 |
| Batch Normalization | Yes |
| Activation Function | ReLU & Softmax |
| Class 1 | Class 2 | Class 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Model | P | R | F1 | P | R | F1 | P | R | F1 | Acc |
| MLP | 0.84 | 0.67 | 0.75 | 0.56 | 0.71 | 0.62 | 0.58 | 0.72 | 0.64 | 0.69 |
| LSTM | 0.80 | 0.83 | 0.81 | 0.69 | 0.6 | 0.64 | 0.68 | 0.70 | 0.69 | 0.751 |
| GRU | 0.78 | 0.86 | 0.82 | 0.69 | 0.62 | 0.65 | 0.75 | 0.63 | 0.68 | 0.757 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monge, J.; Ribeiro, G.; Raimundo, A.; Postolache, O.; Santos, J. AI-Based Smart Sensing and AR for Gait Rehabilitation Assessment. Information 2023, 14, 355. https://doi.org/10.3390/info14070355
Monge J, Ribeiro G, Raimundo A, Postolache O, Santos J. AI-Based Smart Sensing and AR for Gait Rehabilitation Assessment. Information. 2023; 14(7):355. https://doi.org/10.3390/info14070355
Chicago/Turabian StyleMonge, João, Gonçalo Ribeiro, António Raimundo, Octavian Postolache, and Joel Santos. 2023. "AI-Based Smart Sensing and AR for Gait Rehabilitation Assessment" Information 14, no. 7: 355. https://doi.org/10.3390/info14070355
APA StyleMonge, J., Ribeiro, G., Raimundo, A., Postolache, O., & Santos, J. (2023). AI-Based Smart Sensing and AR for Gait Rehabilitation Assessment. Information, 14(7), 355. https://doi.org/10.3390/info14070355