
Microscopic Inspection of the Adhesive Interface of Composite Onlays after Cementation on Low Loading: An In Vitro Study

 , ,
, , 

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
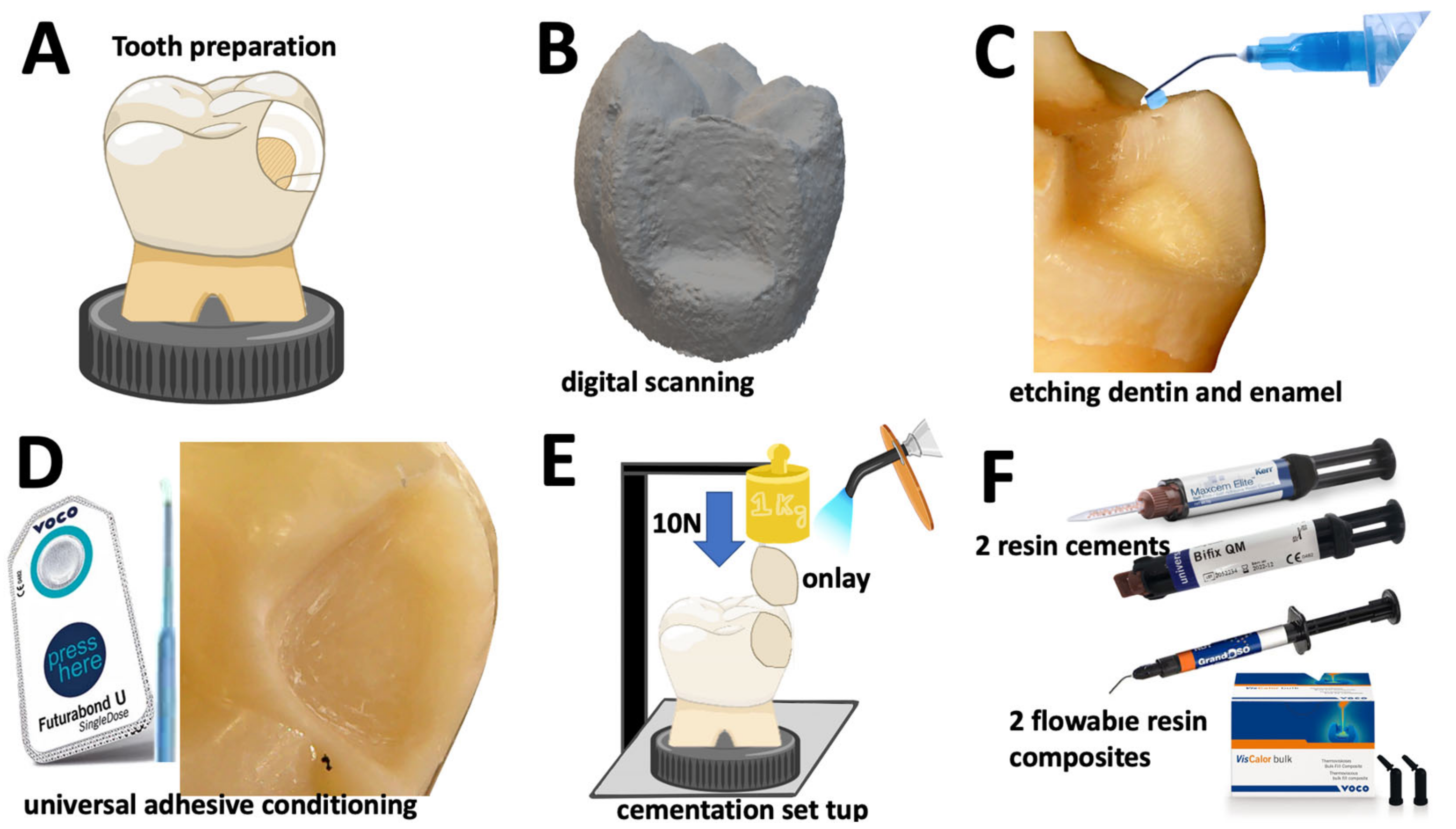
2.1. Preparation of Tooth Substrates
2.2. Preparation of Onlay Restorations
2.3. Cementation Procedure and Specimens
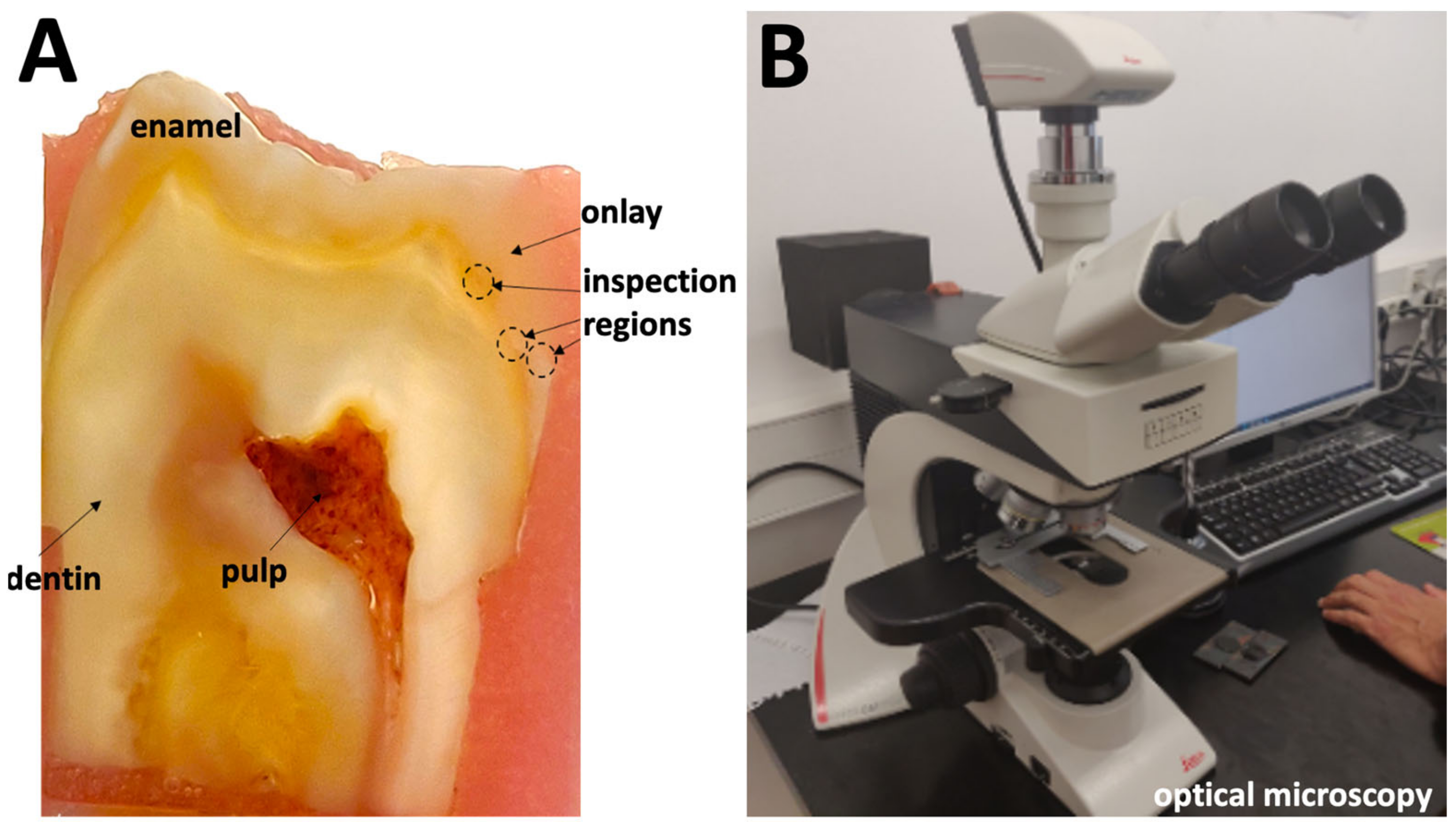
2.4. Microscopic Analyses
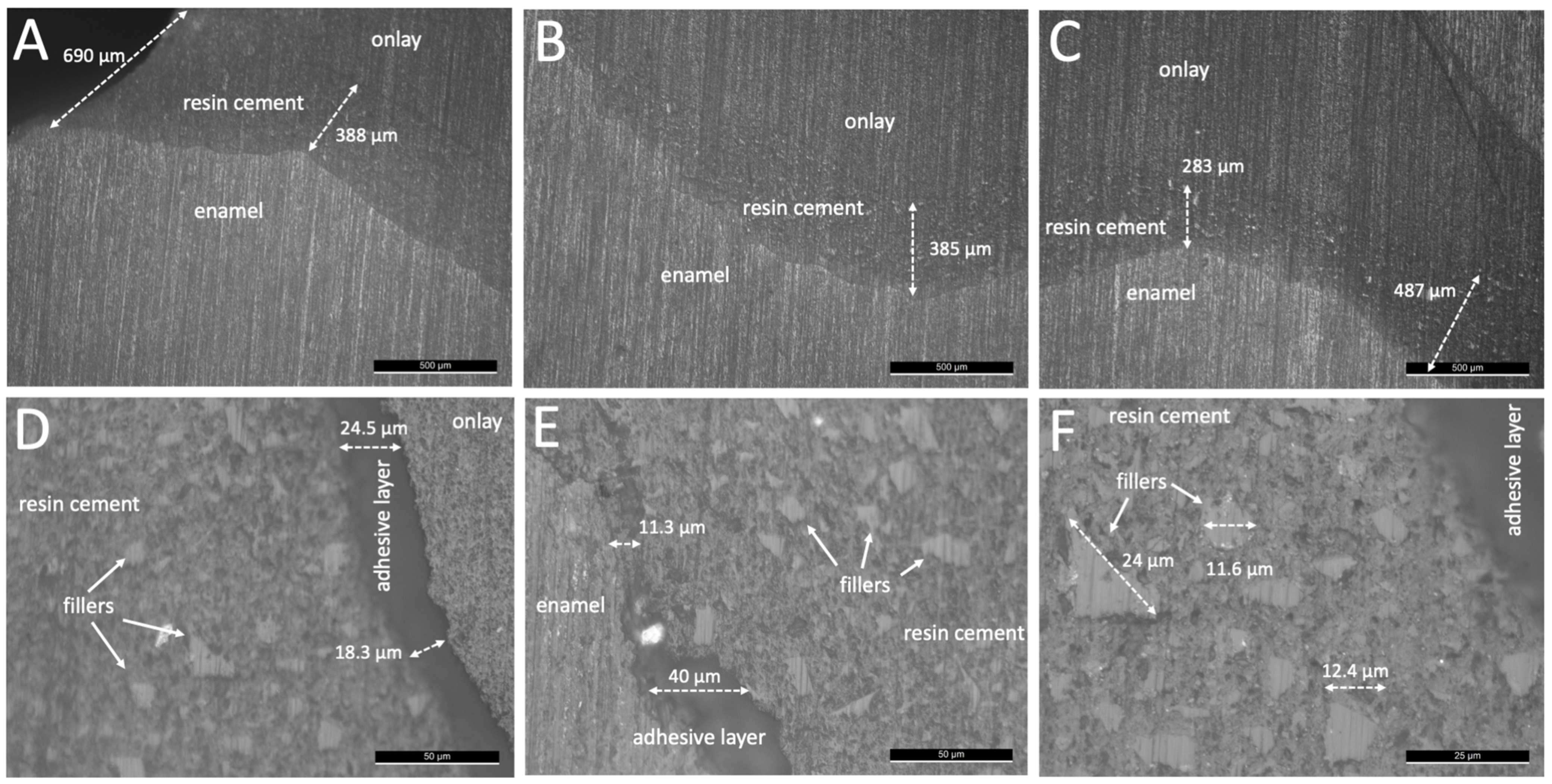
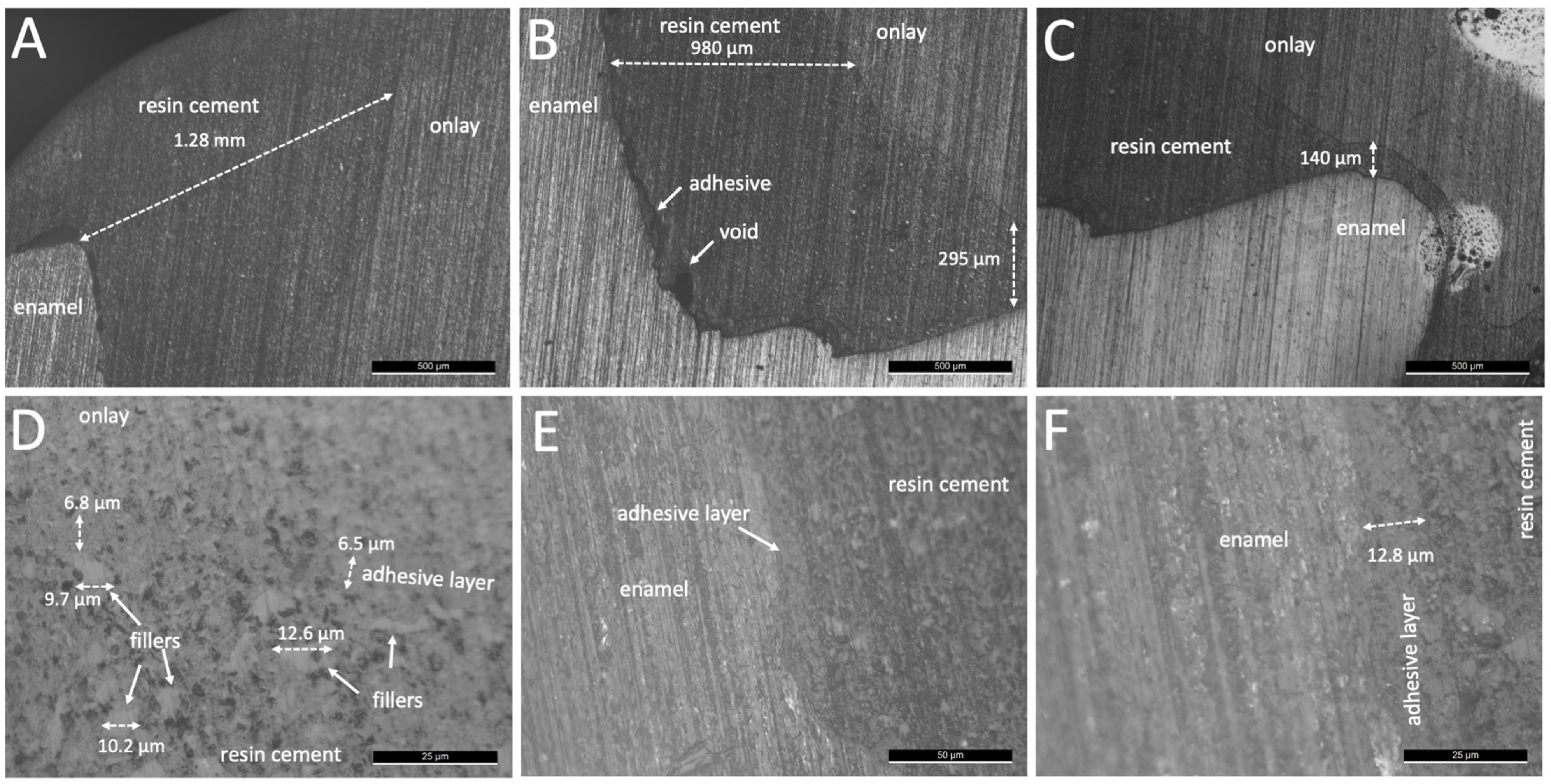
3. Results
4. Discussion
5. Conclusions
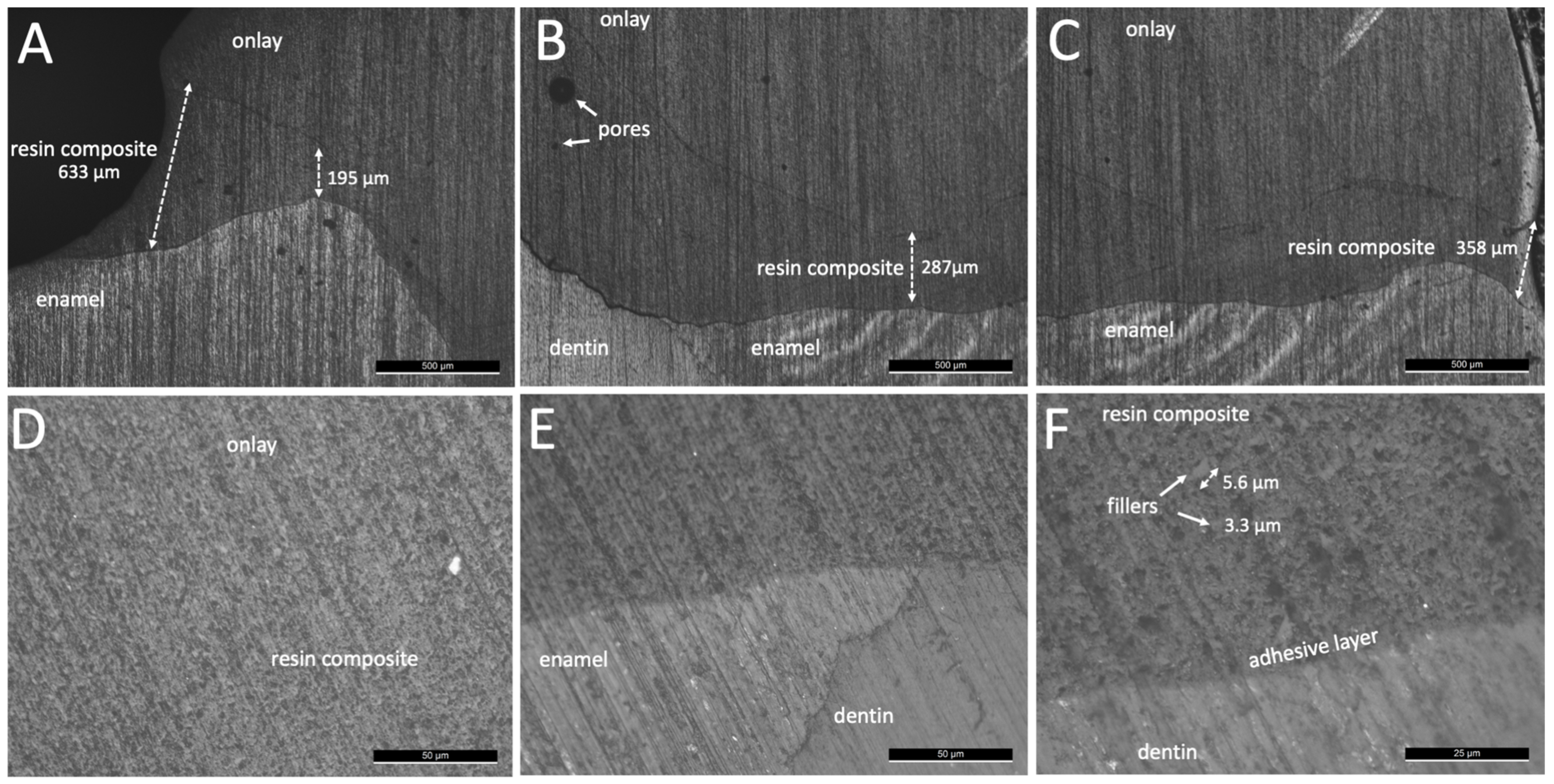
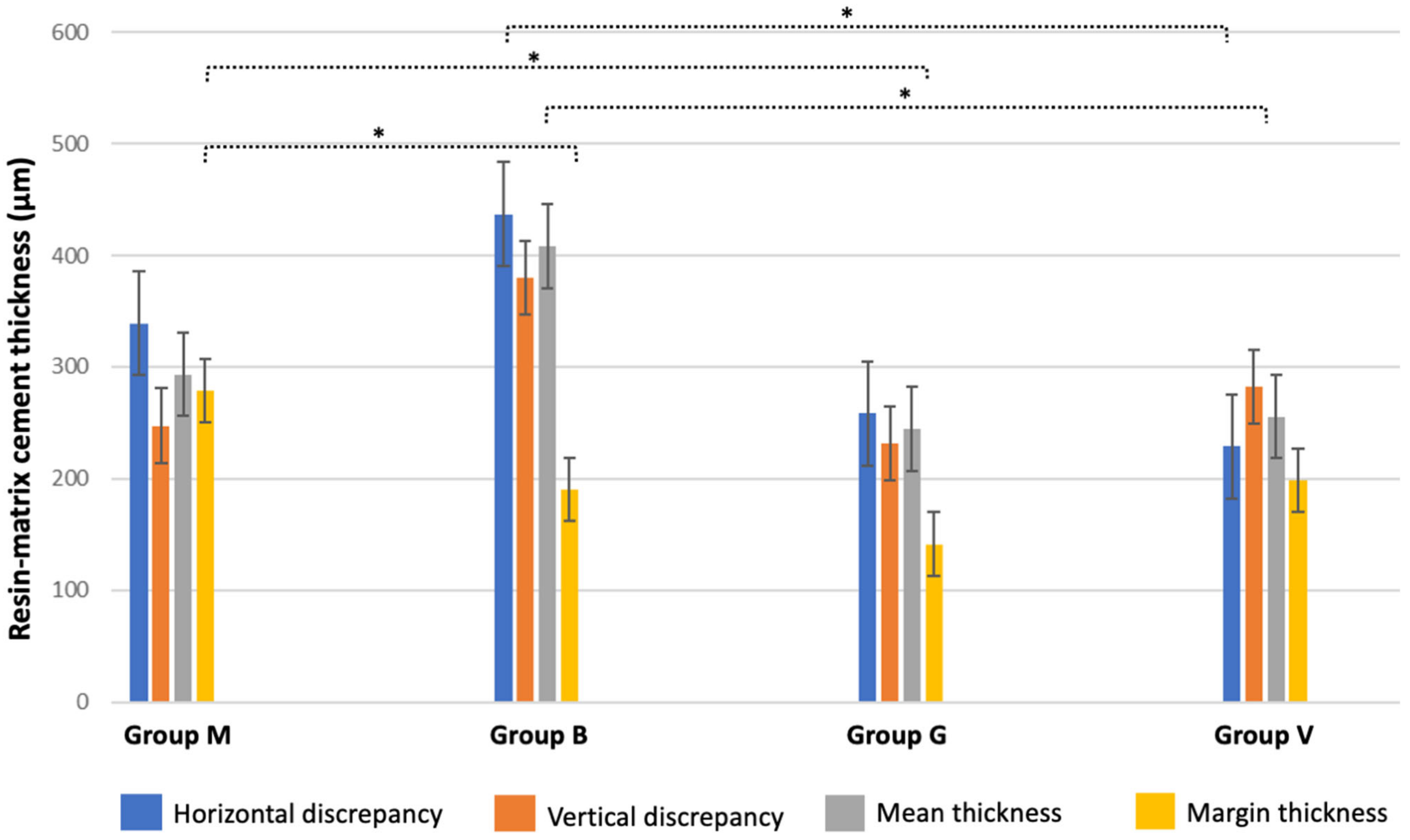
- A higher resin-matrix layer thickness was found for resin-matrix cements than that recorded for flowable resin-matrix composites after cementation at a low loading magnitude. The layer thickness of the resin-matrix cements and flowable composites varied along the onlay to dentin and enamel. An increased cementation layer thickness is more vulnerable to the formation of defects, such as macro- and micro-scale voids and pores.
- The adhesive layer also varied at the interfaces due to the lack of flowing of the resin-matrix cement and flowable composites on cementation at low loading magnitude. Additionally, an increased layer thickness of adhesive and resin-matrix cement or flowable composite can negatively affect the mechanical integrity of the interface since those materials reveal the lowest records of mechanical properties, such as strength, elastic modulus, and fracture toughness.
- Cementation procedures on low loading can occur in several clinical situations due to the operator technical sensitivity. An increase in the cementation loading magnitude by high handling pressure could promote a proper flowing of the adhesive system and the resin-matrix cements resulting in an adequate layer thickness at the onlay interface.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Approval
References
- Coelho, C.; Calamote, C.; Pinto, A.C.; Esteves, J.L.; Ramos, A.; Escuin, T.; Souza, J.C. Comparison of CAD-CAM and traditional chairside processing of 4-unit interim prostheses with and without cantilevers: Mechanics, fracture behavior, and finite element analysis. J. Prosthet. Dent. 2021, 125, 543.e1–543.e10. [Google Scholar] [CrossRef] [PubMed]
- Vahey, B.R.; Sordi, M.B.; Stanley, K.; Magini, R.S.; de Oliveira, A.P.N.; Fredel, M.C.; Henriques, B.; Souza, J.C. Mechanical integrity of cement-and screw-retained zirconium-lithium silicate glass-ceramic crowns to Morse taper implants. J. Prosthet. Dent. 2018, 120, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Pacquet, W.; Tapie, L.; Mawussi, B.; Boitelle, P. Volumetric and dimensional accuracy assessment of CAD-CAM–manufactured dental prostheses from different materials. J. Prosthet. Dent. 2021, 129, 150–159. [Google Scholar] [CrossRef]
- Merrill, T.C.; Mackey, T.; Luc, R.; Lung, D.; Naseem, A.; Abduo, J. Effect of Chairside CAD/CAM Restoration Type on Marginal Fit Accuracy: A Comparison of Crown, Inlay and Onlay Restorations. Eur. J. Prosthodont. Restor. Dent. 2021, 29, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Tafur-Zelada, C.M.; Carvalho, O.; Silva, F.S.; Henriques, B.; Özcan, M.; Souza, J.C.M. The influence of zirconia veneer thickness on the degree of conversion of resin-matrix cements: An integrative review. Clin. Oral Investig. 2021, 25, 3395–3408. [Google Scholar] [CrossRef] [PubMed]
- Magne, P.; Razaghy, M.; Carvalho, M.A.; Soares, L.M. Luting of inlays, onlays, and overlays with preheated restorative composite resin does not prevent seating accuracy. Int. J. Esthet. Dent. 2018, 13, 318–332. [Google Scholar]
- Dursun, E.; Costa, A.M.-D.; Moussally, C. Chairside CAD/CAM Composite Onlays for the Restoration of Primary Molars. J. Clin. Pediatr. Dent. 2018, 42, 349–354. [Google Scholar] [CrossRef]
- Ozyoney, G.; Yanıkoğlu, F.; Tağtekin, D.; Hayran, O. Restoration of Morphologically Compromised and Endodontically Treated Molars. Int. J. Prosthodont. 2013, 26, 230–234. [Google Scholar] [CrossRef] [Green Version]
- Goujat, A.; Abouelleil, H.; Colon, P.; Jeannin, C.; Pradelle, N.; Seux, D.; Grosgogeat, B. Marginal and internal fit of CAD-CAM inlay/onlay restorations: A systematic review of in vitro studies. J. Prosthet. Dent. 2019, 121, 590–597.e3. [Google Scholar] [CrossRef]
- Davidowitz, G.; Kotick, P.G. The Use of CAD/CAM in Dentistry. Dent. Clin. North Am. 2011, 55, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Lebon, N.; Tapie, L.; Duret, F.; Attal, J.-P. Understanding dental CAD/CAM for restorations--dental milling machines from a mechanical engineering viewpoint. Part B: Labside milling machines. Int. J. Comput. Dent. 2016, 19, 115–134. [Google Scholar] [PubMed]
- Kelly, J.R.; Benetti, P. Ceramic materials in dentistry: Historical evolution and current practice. Aust. Dent. J. 2011, 56, 84–96. [Google Scholar] [CrossRef]
- Ruse, N.D.; Sadoun, M.J. Resin-composite blocks for dental CAD/CAM applications. J. Dent. Res. 2014, 93, 1232–1234. [Google Scholar] [CrossRef] [Green Version]
- Fabel, G.; Beuer, F. Establishing a suitable surface roughness for lithium disilicate implant abutments under laboratory conditions: A morphologic SEM and profilometric pilot study. Int. J. Comput. Dent. 2017, 20, 303–314. [Google Scholar]
- Souza, J.; Fuentes, M.V.; Baena, E.; Ceballos, L. One-year clinical performance of lithium disilicate versus resin composite CAD/CAM onlays. Odontology 2020, 109, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Bayrak, A.; Akat, B.; Ocak, M.; Kιlιçarslan, M.A.; Özcan, M. Micro-Computed Tomography Analysis of Fit of Ceramic Inlays Produced with Dif-ferent CAD Software Programs. Eur. J. Prosthodont. Restor. Dent. 2021, 29, 1–6. [Google Scholar] [CrossRef]
- Bosch, G.; Ender, A.; Mehl, A. A 3-dimensional accuracy analysis of chairside CAD/CAM milling processes. J. Prosthet. Dent. 2014, 112, 1425–1431. [Google Scholar] [CrossRef] [Green Version]
- Goujat, A.; Abouelleil, H.; Colon, P.; Jeannin, C.; Pradelle, N.; Seux, D.; Grosgogeat, B. Mechanical properties and internal fit of 4 CAD-CAM block materials. J. Prosthet. Dent. 2017, 119, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Ahlholm, P.; Lappalainen, R.; Lappalainen, J.; Tarvonen, P.-L.; Sipilä, K. Challenges of the Direct Filling Technique, Adoption of CAD/CAM Techniques, and Attitudes Toward 3D Printing for Restorative Treatments Among Finnish Dentists. Int. J. Prosthodont. 2019, 32, 402–410. [Google Scholar] [CrossRef]
- García-Cuesta, C.; Faus-Llácer, V.; Zubizarreta-Macho, Á.; Botello-Torres, R.; Faus-Matoses, V. A comparison of the marginal adaptation of composite overlays fabricated with silicone and an intraoral scanner. J. Clin. Exp. Dent. 2021, 13, e473–e478. [Google Scholar] [CrossRef]
- Blatz, M.B.; Vonderheide, M.; Conejo, J. The Effect of Resin Bonding on Long-Term Success of High-Strength Ceramics. J. Dent. Res. 2018, 97, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Tokita, C.; Maeno, M.; Nara, Y. The effect of space setting values and restorative block materials on the bonding of metal-free CAD/CAM onlay restorations. Dent. Mater. J. 2021, 40, 994–1006. [Google Scholar] [CrossRef]
- Ishii, N.; Maseki, T.; Nara, Y. Bonding state of metal-free CAD/CAM onlay restoration after cyclic loading with and without immediate dentin sealing. Dent. Mater. J. 2017, 36, 357–367. [Google Scholar] [CrossRef] [Green Version]
- Murata, T.; Maseki, T.; Nara, Y. Effect of immediate dentin sealing applications on bonding of CAD/CAM ceramic onlay restoration. Dent. Mater. J. 2018, 37, 928–939. [Google Scholar] [CrossRef] [Green Version]
- Koshida, S.; Maeno, M.; Nara, Y. Effect of differences in the type of restoration and adhesive resin cement system on the bonding of CAD/CAM ceramic restorations. Dent. Mater. J. 2020, 39, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, V.; Silva, A.S.; Carvalho, O.; Henriques, B.; Silva, F.S.; Özcan, M.; Souza, J.C.M. The resin-matrix cement layer thickness resultant from the intracanal fitting of teeth root canal posts: An integrative review. Clin. Oral Investig. 2021, 25, 5595–5612. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.Y.; Stoner, B.R.; Piascik, J.R.; Smith, R. Adhesion/cementation to zirconia and other non-silicate ceramics: Where are we now? Dent. Mater. 2011, 27, 71–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozcan, M.; Vallittu, P.K. Effect of surface conditioning methods on the bond strength of luting cement to ceramics. Dent. Mater. 2003, 19, 725–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fronza, B.; Ayres, A.; Pacheco, R.; Rueggeberg, F.; Dias, C.; Giannini, M. Characterization of Inorganic Filler Content, Mechanical Properties, and Light Transmission of Bulk-fill Resin Composites. Oper. Dent. 2017, 42, 445–455. [Google Scholar] [CrossRef] [Green Version]
- Prieto, L.T.; De Araújo, C.T.P.; Pierote, J.J.A.; De Oliveira, D.C.R.S.; Coppini, E.K.; Paulillo, L.A.M.S. Evaluation of degree of conversion and the effect of thermal aging on the color stability of resin cements and flowable composite. J. Conserv. Dent. 2018, 21, 47–51. [Google Scholar] [CrossRef]
- Melilli, D.; Cumbo, E.M.; Baldissara, P.; Wandscher, V.F.; Valandro, L.F.; Gallina, G.; Pizzo, G. Evaluation of marginal leakage after mechanical fatigue cycling of composite inlays luted with different cements. Gen. Dent. 2018, 66, 51–55. [Google Scholar] [PubMed]
- Souza, J.C.; Bentes, A.C.; Reis, K.; Gavinha, S.; Buciumeanu, M.; Henriques, B.; Silva, F.S.; Gomes, J.R. Abrasive and sliding wear of resin composites for dental restorations. Tribol. Int. 2016, 102, 154–160. [Google Scholar] [CrossRef]
- Rodrigues, D.S.; Buciumeanu, M.; Martinelli, A.E.; Nascimento, R.M.; Henriques, B.; Silva, F.S.; Souza, J.C.M. Mechanical Strength and Wear of Dental Glass-Ionomer and Resin Composites Affected by Porosity and Chemical Composition. J. Bio-Tribo-Corrosion 2015, 1, 14. [Google Scholar] [CrossRef] [Green Version]
- Lopes-Rocha, L.; Ribeiro-Gonçalves, L.; Henriques, B.; Özcan, M.; Tiritan, M.E.; Souza, J.C.M. An integrative review on the toxicity of Bisphenol A (BPA) released from resin composites used in dentistry. J. Biomed. Mater. Res. Part B Appl. Biomater. 2021, 109, 1942–1952. [Google Scholar] [CrossRef]
- Ferracane, J.L. Resin composite—State of the art. Dent. Mater. 2011, 27, 29–38. [Google Scholar] [CrossRef]
- Souza, J.C.M.; Fernandes, V.; Correia, A.; Miller, P.; Carvalho, O.; Silva, F.; Özcan, M.; Henriques, B. Surface modification of glass fiber-reinforced composite posts to enhance their bond strength to resin-matrix cements: An integrative review. Clin. Oral Investig. 2022, 26, 95–107. [Google Scholar] [CrossRef]
- Ahlholm, P. Accuracy of inlay and onlay restorations based on 3D printing or milling technique—A pilot study. Eur. J. Prosthodont. Restor. Dent. 2019, 27, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-H.; Yoo, Y.-J.; Shin, Y.-J.; Cho, B.-H.; Baek, S.-H. Marginal and internal fit of nano-composite CAD/CAM restorations. Restor. Dent. Endod. 2016, 41, 37–43. [Google Scholar] [CrossRef]
- Gudugunta, L.; Mynampati, P.; Jeevan, M.B.; Kumar, S.M.; Akkaloori, A.; Tejavath, S.K. The marginal discrepancy of lithium disilicate onlays: Computer-aided design versus press. J. Conserv. Dent. 2019, 22, 336–339. [Google Scholar] [CrossRef]
- Tauböck, T.T.; Tarle, Z.; Marovic, D.; Attin, T. Pre-heating of high-viscosity bulk-fill resin composites: Effects on shrinkage force and monomer conversion. J. Dent. 2015, 43, 1358–1364. [Google Scholar] [CrossRef] [Green Version]
- Keshvad, A.; Hakimaneh, S.M.R. Microtensile Bond Strength of a Resin Cement to Silica-Based and Y-TZP Ceramics Using Different Surface Treatments. J. Prosthodont. 2018, 27, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Guo, Y.Y.; Chen, L.; Han, J.; Tong, H.; Zhang, B.; Zhang, Y. Effects of Different Surface Treatments on Bond Strength of Resin Cement to Machined Pure Titanium. J. Adhes. Dent. 2019, 21, 401–411. [Google Scholar] [CrossRef]
- Pitta, J.; Bijelic-Donova, J.; Burkhardt, F.; Fehmer, V.; Närhi, T.; Sailer, I. Temporary Implant-Supported Single Crowns Using Titanium Base Abutments: An In Vitro Study on Bonding Stability and Pull-out Forces. Int. J. Prosthodont. 2020, 33, 546–552. [Google Scholar] [CrossRef]
- Pitta, J.; Burkhardt, F.; Mekki, M.; Fehmer, V.; Mojon, P.; Sailer, I. Effect of airborne-particle abrasion of a titanium base abutment on the stability of the bonded interface and retention forces of crowns after artificial aging. J. Prosthet. Dent. 2021, 126, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Kaweewongprasert, P.; Phasuk, K.; Levon, J.A.; Eckert, G.J.; Feitosa, S.; Valandro, L.F.; Bottino, M.C.; Morton, D. Fatigue Failure Load of Lithium Disilicate Restorations Cemented on a Chairside Titanium-Base. J. Prosthodont. 2019, 28, 973–981. [Google Scholar] [CrossRef]
- Weyhrauch, M.; Igiel, C.; Scheller, H.; Weibrich, G.; Lehmann, K.M. Fracture Strength of Monolithic All-Ceramic Crowns on Titanium Implant Abutments. Int. J. Oral Maxillofac. Implant. 2016, 31, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Henriques, B.; Sampaio, M.; Buciumeanu, M.; Souza, J.C.; Gomes, J.R.; Silva, F.; Carvalho, O. Laser surface structuring of Ti6Al4V substrates for adhesion enhancement in Ti6Al4V-PEEK joints. Mater. Sci. Eng. C 2017, 79, 177–184. [Google Scholar] [CrossRef]
- Souza, J.C.M.; Tajiri, H.A.; Morsch, C.S.; Buciumeanu, M.; Mathew, M.T.; Silva, F.S.; Henriques, B. Tribocorrosion Behavior of Ti6Al4V Coated with a Bio-absorbable Polymer for Biomedical Applications. J. Bio-Tribo-Corrosion 2015, 1, 27. [Google Scholar] [CrossRef] [Green Version]
- Goracci, C.; Cury, A.H.; Cantoro, A.; Papacchini, F.; Tay, F.R.; Ferrari, M. Microtensile bond strength and interfacial properties of self-etching and self-adhesive resin cements used to lute composite onlays under different seating forces. J Adhes Dent 2006, 8, 327–335. [Google Scholar] [PubMed]
- Hironaka, N.G.; Ubaldini, A.L.; Sato, F.; Giannini, M.; Terada, R.S.; Pascotto, R.C. Influence of immediate dentin sealing and interim cementation on the adhesion of indirect restorations with dual-polymerizing resin cement. J. Prosthet. Dent. 2018, 119, 678.e1–678.e8. [Google Scholar] [CrossRef] [PubMed]
- Zortuk, M.; Bolpaca, P.; Kilic, K.; Ozdemir, E.; Aguloglu, S. Effects of Finger Pressure Applied by Dentists during Cementation of All-Ceramic Crowns. Eur. J. Dent. 2010, 04, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Uzgur, R.; Ercan, E.; Uzgur, Z.; Colak, H.; Yalçın, M.; Özcan, M. Cement Thickness of Inlay Restorations Made of Lithium Disilicate, Polymer-Infiltrated Ceramic and Nano-Ceramic CAD/CAM Materials Evaluated Using 3D X-Ray Micro-Computed Tomography. J. Prosthodont. 2018, 27, 456–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material Type (Brand, Manufacturer) | Organic Matrix | Fillers %(w/w) | Fillers % (v/v) | Filler Type | Elastic Modulus (GPa) |
|---|---|---|---|---|---|
| Dual-curing resin cement (Max Cem EliteTM, KERR Kloten, Switzerland) | Bis-GMA, HEMA, GPDM; UDMA; 1,1,3,3-tetramethylbutyl hydroperoxide TEGDMA, CHPO, MEHQ Bis-GMA, GPDM, co-monomers (33 wt%) | 67 | 46 | Barium alumina silica glass, fluoroalumina silicate glass borosilicate (30–60%) glass, Ytterbium fluoride (10–30%), amorphous silica (1–5%). (size~3.6 µm). | 4.5 |
| Dual-curing, resin cement (Bifix QMTM, VOCO GmbH, Cluxhaven, Germany) | Bi-functional methacrylate, acid methacrylate, Bis-GMA, benzoyl peroxide, amines and BHT, Gly-DMA, UDMA, phosphate monomers (30 wt%) | 70 | 61 | Glass fillers, amorphous silica; (size~2.9 µm) | 6–7.5 |
| Flowable resin composite (GrandioSO Heavy FlowTM, VOCO GmbH, Cluxhaven, Germany) | BisGMA, BisEMA, TEGDMA, HDDMA, CQ, amine and BHT (17 wt%) | 83 | 68 | nanoparticles of SiO2 (size~20–40 nm); glass-ceramic; (size~1 µm) | 11.5 |
| Thermally induced flowable resin composite (VisCalor bulk- fill TM, VOCO GmbH, Cluxhaven, Germany) | Bis-GMA, aliphatic dimethacrylate (17 wt%) | 83 | 68 | nanoparticles of SiO2 (size~20–40 nm); glass-ceramic (size~1 µm) | 12.3–17.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magalhães, T.; Fidalgo-Pereira, R.; Torres, O.; Carvalho, Ó.; Silva, F.S.; Henriques, B.; Özcan, M.; Souza, J.C.M. Microscopic Inspection of the Adhesive Interface of Composite Onlays after Cementation on Low Loading: An In Vitro Study. J. Funct. Biomater. 2023, 14, 148. https://doi.org/10.3390/jfb14030148
Magalhães T, Fidalgo-Pereira R, Torres O, Carvalho Ó, Silva FS, Henriques B, Özcan M, Souza JCM. Microscopic Inspection of the Adhesive Interface of Composite Onlays after Cementation on Low Loading: An In Vitro Study. Journal of Functional Biomaterials. 2023; 14(3):148. https://doi.org/10.3390/jfb14030148
Chicago/Turabian StyleMagalhães, Tiago, Rita Fidalgo-Pereira, Orlanda Torres, Óscar Carvalho, Filipe S. Silva, Bruno Henriques, Mutlu Özcan, and Júlio C. M. Souza. 2023. "Microscopic Inspection of the Adhesive Interface of Composite Onlays after Cementation on Low Loading: An In Vitro Study" Journal of Functional Biomaterials 14, no. 3: 148. https://doi.org/10.3390/jfb14030148
APA StyleMagalhães, T., Fidalgo-Pereira, R., Torres, O., Carvalho, Ó., Silva, F. S., Henriques, B., Özcan, M., & Souza, J. C. M. (2023). Microscopic Inspection of the Adhesive Interface of Composite Onlays after Cementation on Low Loading: An In Vitro Study. Journal of Functional Biomaterials, 14(3), 148. https://doi.org/10.3390/jfb14030148