
Improving Bone Formation by Guided Bone Regeneration Using a Collagen Membrane with rhBMP-2: A Novel Concept

 ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals and Materials
2.1.1. Experimental Animals
2.1.2. Collagen Membrane
2.1.3. Biphasic Calcium Phosphate
2.1.4. rhBMP-2
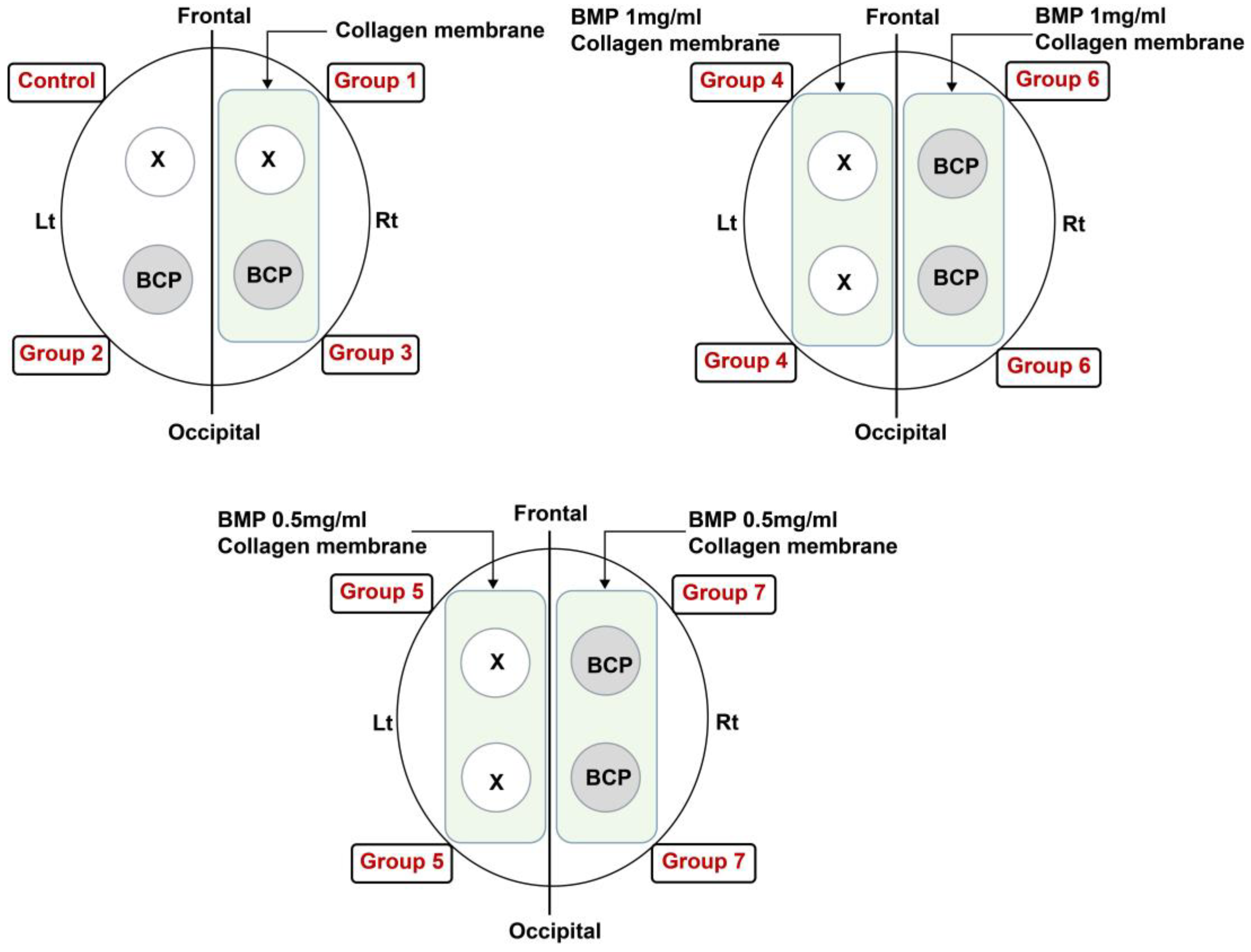
2.2. Study Design
2.2.1. Groups
2.2.2. Surgical Protocol
2.2.3. Sacrifice
2.2.4. Histological and Histomorphometric Analysis
2.2.5. Immunohistochemical Analysis
2.3. Statistical Analysis
3. Results
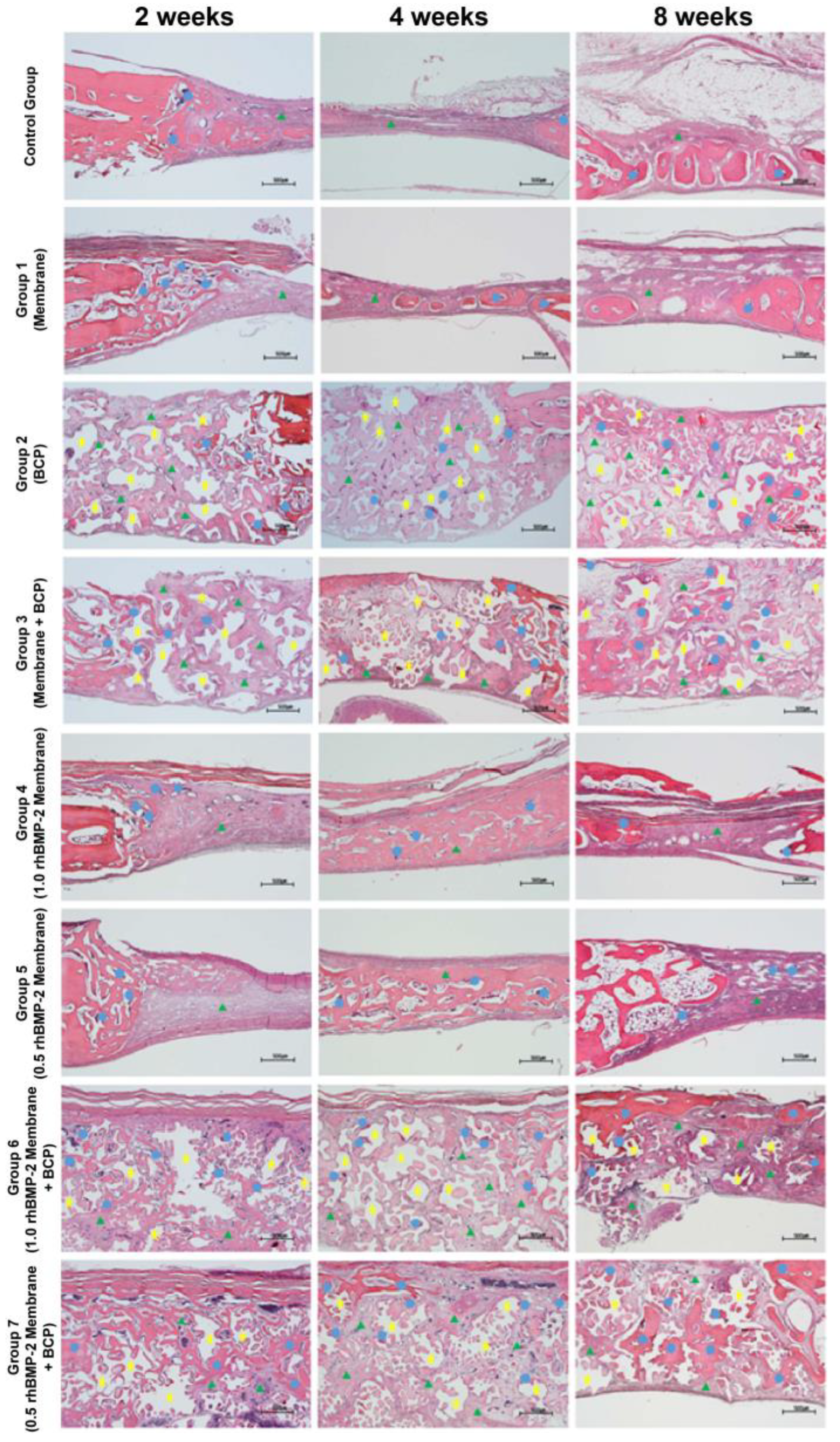
3.1. Histological Findings (H and E Staining)
3.2. Histomorphometric Findings
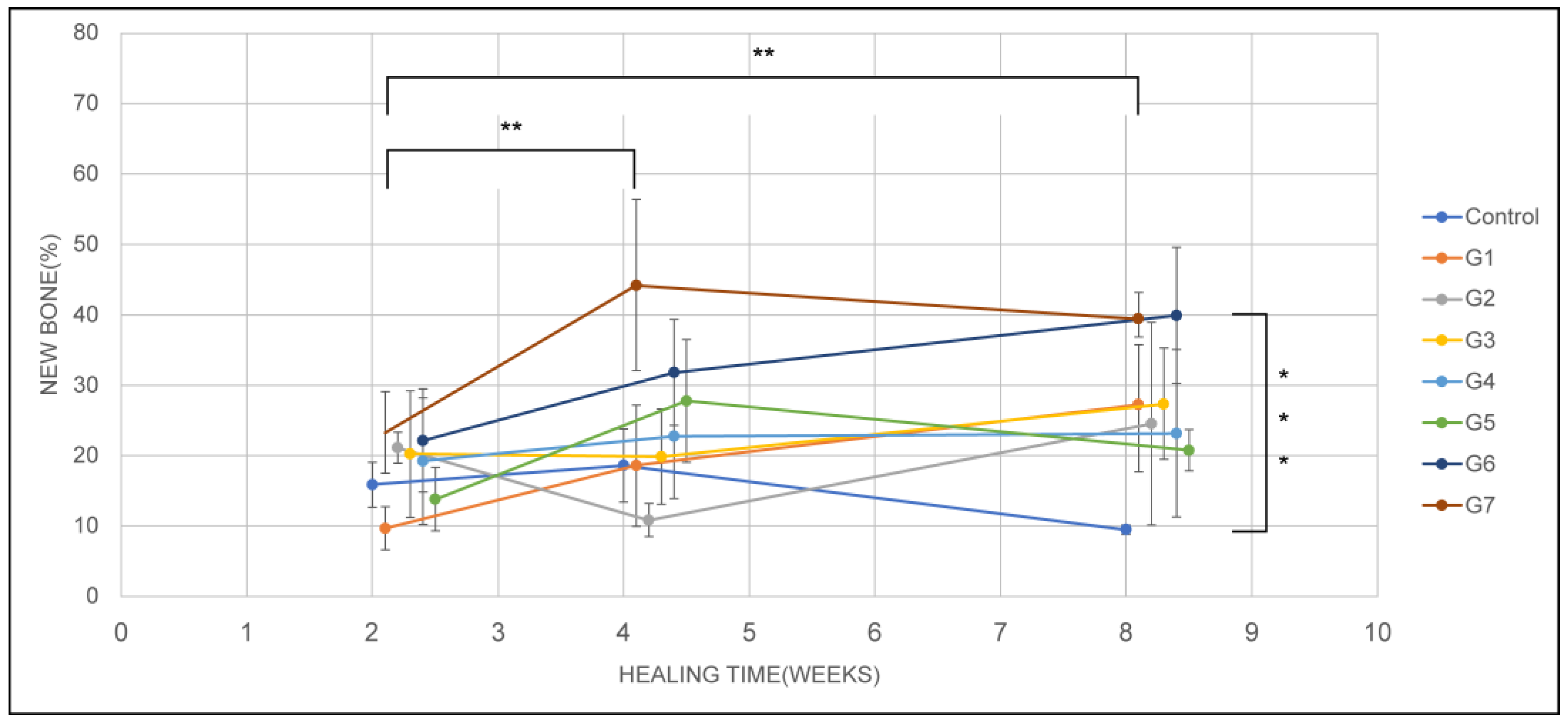
3.3. New Bone Formation
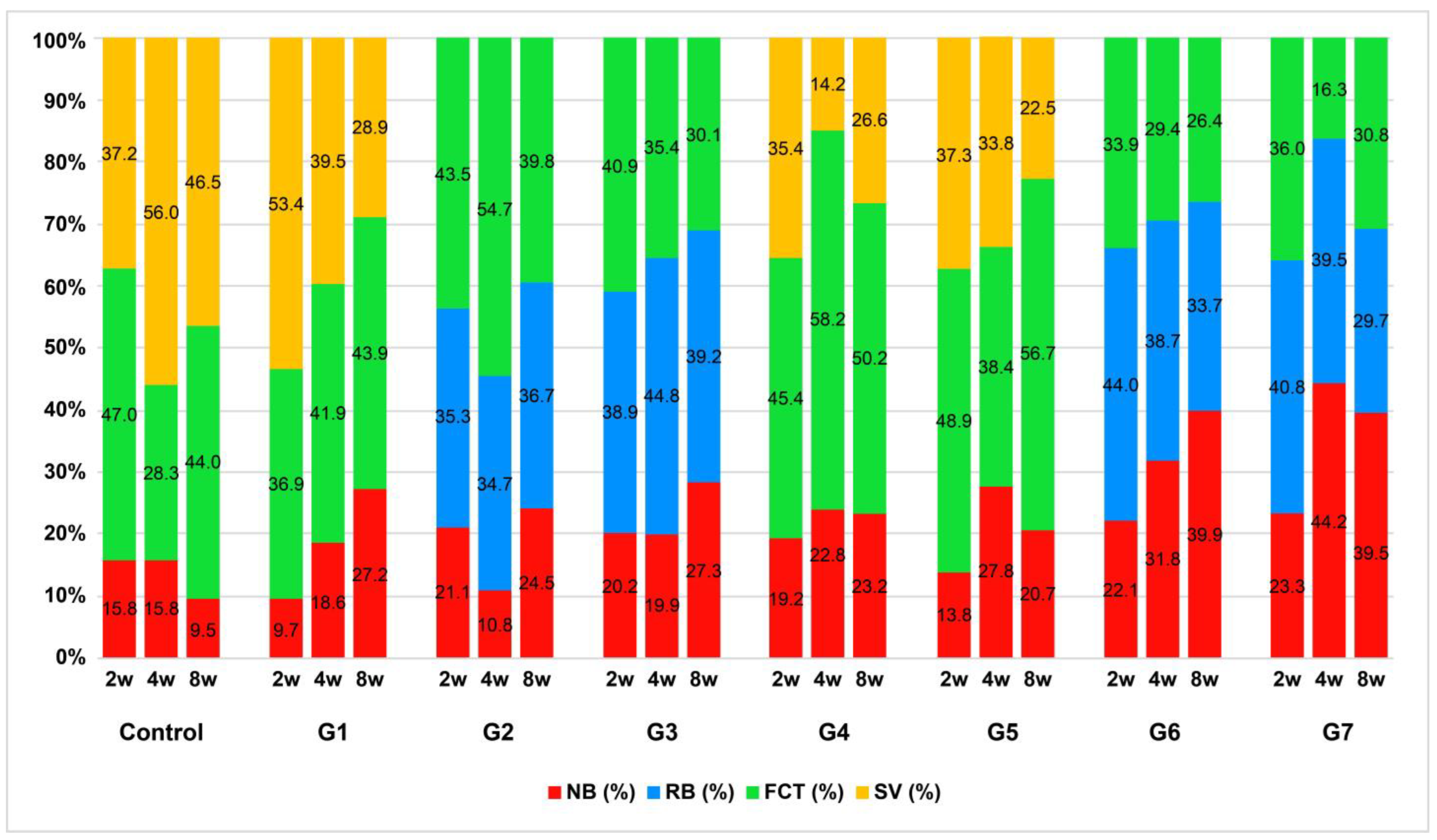
3.4. Histological Components
3.5. Histological Findings (Russell-Movat Pentachrome Staining)
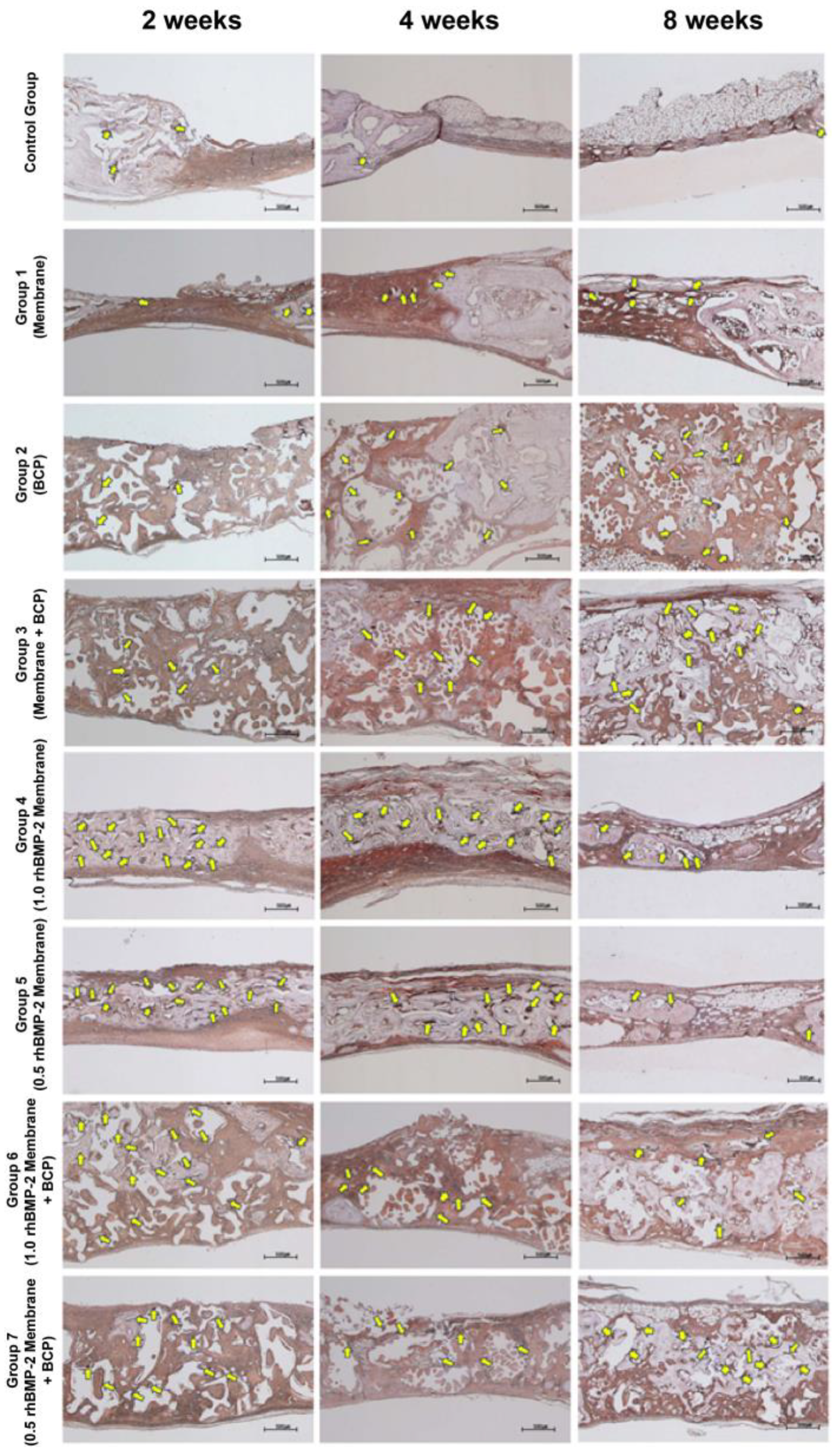
3.6. Immunohistochemical Findings (Anti-Osteocalcin Antibody Staining)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- El Bialy, I.; Jiskoot, W.; Nejadnik, M.R. Formulation, delivery and stability of bone morphogenetic proteins for effective bone regeneration. Pharm. Res. 2017, 34, 1152–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khojasteh, A.; Kheiri, L.; Motamedian, S.R.; Khoshkam, V. Guided bone regeneration for the reconstruction of alveolar bone defects. Ann. Maxillofac. Surg. 2017, 7, 263–277. [Google Scholar] [CrossRef] [PubMed]
- Retzepi, M.; Donos, N. Guided Bone Regeneration: Biological principle and therapeutic applications. Clin. Oral Implant. Res. 2010, 21, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Tolstunov, L.; Hamrick, J.F.E.; Broumand, V.; Shilo, D.; Rachmiel, A. Bone augmentation techniques for horizontal and vertical alveolar ridge deficiency in oral implantology. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 163–191. [Google Scholar] [CrossRef]
- Schlegel, A.; Möhler, H.; Busch, F.; Mehl, A. Preclinical and clinical studies of a collagen membrane (Bio-Gide). Biomaterials 1997, 18, 535–538. [Google Scholar] [CrossRef]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef] [Green Version]
- Sheikh, Z.; Qureshi, J.; Alshahrani, A.M.; Nassar, H.; Ikeda, Y.; Glogauer, M.; Ganss, B. Collagen based barrier membranes for periodontal guided bone regeneration applications. Odontology 2017, 105, 1–12. [Google Scholar] [CrossRef]
- Hong, I.; Khalid, A.W.; Pae, H.-C.; Cha, J.-K.; Lee, J.-S.; Paik, J.-W.; Jung, U.-W.; Choi, S.-H. Distinctive bone regeneration of calvarial defects using biphasic calcium phosphate supplemented ultraviolet-crosslinked collagen membrane. J. Periodontal Implant. Sci. 2020, 50, 14–27. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, K.; Lu, X.; Li, M.; Liu, H.; Xie, C.; Meng, F.; Jiang, O.; Li, C.; Zhi, W. BMP-2 encapsulated polysaccharide nanoparticle modified biphasic calcium phosphate scaffolds for bone tissue regeneration. J. Biomed. Mater. Res. Part A 2015, 103, 1520–1532. [Google Scholar] [CrossRef]
- Friedmann, A.; Dard, M.; Kleber, B.-M.; Bernimoulin, J.-P.; Bosshardt, D.D. Ridge augmentation and maxillary sinus grafting with a biphasic calcium phosphate: Histologic and histomorphometric observations. Clin. Oral Implant. Res. 2009, 20, 708–714. [Google Scholar] [CrossRef]
- Bignon, A.; Chouteau, J.; Chevalier, J.; Fantozzi, G.; Carret, J.-P.; Chavassieux, P.; Boivin, G.; Melin, M.; Hartmann, D. Effect of micro- and macroporosity of bone substitutes on their mechanical properties and cellular response. J. Mater. Sci. Mater. Med. 2003, 14, 1089–1097. [Google Scholar] [CrossRef]
- Zhao, J.; Shinkai, M.; Takezawa, T.; Ohba, S.; Chung, U.-I.; Nagamune, T. Bone regeneration using collagen type I vitrigel with bone morphogenetic protein-2. J. Biosci. Bioeng. 2009, 107, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Caballé-Serrano, J.; Abdeslam-Mohamed, Y.; Munar-Frau, A.; Fujioka-Kobayashi, M.; Hernández-Alfaro, F.; Miron, R. Adsorption and release kinetics of growth factors on barrier membranes for guided tissue/bone regeneration: A systematic review. Arch. Oral Biol. 2019, 100, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Bessa, P.C.; Casal, M.; Reis, R.L. Bone morphogenetic proteins in tissue engineering: The road from laboratory to clinic, part II (BMP delivery). J. Tissue Eng. Regen. Med. 2008, 2, 81–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bessa, P.C.; Casal, M.; Reis, R.L. Bone morphogenetic proteins in tissue engineering: The road from the laboratory to the clinic, part I (basic concepts). J. Tissue Eng. Regen. Med. 2008, 2, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Gkiliopoulos, D.; Tsamesidis, I.; Theocharidou, A.; Pouroutzidou, G.K.; Christodoulou, E.; Stalika, E.; Xanthopoulos, K.; Bikiaris, D.; Triantafyllidis, K.; Kontonasaki, E. SBA-15 mesoporous silica as delivery vehicle for rhBMP-2 bone morphogenic protein for dental applications. Nanomaterials 2022, 12, 822. [Google Scholar] [CrossRef]
- Johnson, T.B.; Siderits, B.; Nye, S.; Jeong, Y.-H.; Han, S.-H.; Rhyu, I.-C.; Han, J.-S.; Deguchi, T.; Beck, F.M.; Kim, D.-G. Effect of guided bone regeneration on bone quality surrounding dental implants. J. Biomech. 2018, 80, 166–170. [Google Scholar] [CrossRef]
- Chung, S.-M.; Jung, I.K.; Yoon, B.-H.; Choi, B.R.; Kim, D.M.; Jang, J.S. Evaluation of different combinations of biphasic calcium phosphate and growth factors for bone formation in calvarial defects in a rabbit model. Int. J. Periodontics Restor. Dent. 2016, 36, s49–s59. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Yin, H.-M.; Luo, E.; Zhu, S.; Wang, P.; Zhang, Z.; Liao, G.-Q.; Xu, J.-Z.; Li, Z.-M.; Li, J.-H. Accelerating bone healing by decorating BMP-2 on porous composite scaffolds. ACS Appl. Bio Mater. 2019, 2, 5717–5726. [Google Scholar] [CrossRef]
- Wadhwa, P.; Lee, J.H.; Zhao, B.C.; Cai, H.; Rim, J.-S.; Jang, H.-S.; Lee, E.-S. Microcomputed tomography and histological study of bone regeneration using tooth biomaterial with BMP-2 in rabbit calvarial defects. Scanning 2021, 2021, 6690221. [Google Scholar] [CrossRef]
- Hunt, D.R.; Jovanovic, S.A.; Wikesjö, U.M.; Wozney, J.M.; Bernard, G.W. Hyaluronan supports recombinant human bone morphogenetic protein-2 induced bone reconstruction of advanced alveolar ridge defects in dogs. A Pilot Study. J. Periodontol. 2001, 72, 651–658. [Google Scholar] [CrossRef]
- Sigurdsson, T.J.; Nygaard, L.; Tatakis, D.N.; Fu, E.; Turek, T.J.; Jin, L.; Wozney, J.M.; Wikesjö, U.M. Periodontal repair in dogs: Evaluation of rhBMP-2 carriers. Int. J. Periodontics Restor. Dent. 1996, 16, 524–537. [Google Scholar]
- Yamazaki, Y.; Oida, S.; Akimoto, Y.; Shioda, S. Response of the mouse femoral muscle to an implant of a composite of bone morphogenetic protein and plaster of paris. Clin. Orthop. Relat. Res. 1988, 234, 240–249. [Google Scholar] [CrossRef]
- James, A.W.; LaChaud, G.; Shen, J.; Asatrian, G.; Nguyen, V.; Zhang, X.; Ting, K.; Soo, C. A review of the clinical side effects of bone morphogenetic protein-2. Tissue Eng. Part B Rev. 2016, 22, 284–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-S.; Lee, S.-K.; Kim, B.-S.; Im, G.-I.; Cho, K.-S.; Kim, C.-S. Controlled release of BMP-2 using a heparin-conjugated carrier system reduces in vivo adipose tissue formation. J. Biomed. Mater. Res. Part A 2015, 103, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-S.; Kim, T.-W.; Park, S.; Kim, B.-S.; Im, G.-I.; Cho, K.-S.; Kim, C.-S. Reduction of adipose tissue formation by the controlled release of BMP-2 using a hydroxyapatite-coated collagen carrier system for sinus-augmentation/extraction-socket grafting. Materials 2015, 8, 7634–7649. [Google Scholar] [CrossRef] [Green Version]
- Aryal, R.; Chen, X.-P.; Fang, C.; Hu, Y.-C. Bone morphogenetic protein-2 and vascular endothelial growth factor in bone tissue regeneration: New insight and perspectives. Orthop. Surg. 2014, 6, 171–178. [Google Scholar] [CrossRef]
- Gittens, S.A.; Bagnall, K.; Matyas, J.R.; Löbenberg, R.; Uludaǧ, H. Imparting bone mineral affinity to osteogenic proteins through heparin–bisphosphonate conjugates. J. Control. Release 2004, 98, 255–268. [Google Scholar] [CrossRef]
- Al-Askar, M.; Javed, F.; Al-Hezaimi, K.; Al-Hamdan, K.S.; Ramalingam, S.; Aldahmash, A.; Nooh, N.; Al-Rasheed, A. Guided bone regeneration in standardized calvarial defects in rats using bio-oss and β-tricalcium phosphate with adjunct platelet-derived growth factor therapy: A real-time in vivo microcomputed tomographic, biomechanical, and histologic analysis. Int. J. Periodontics Restor. Dent. 2016, 36, s61–s73. [Google Scholar] [CrossRef] [Green Version]
- Al-Rasheed, A.; Al-Ahmari, F.; Ramalingam, S.; Nooh, N.; Wang, C.-Y.; Al-Hezaimi, K. Real-time assessment of guided bone regeneration in standardized calvarial defects using a combination of bone graft and platelet-derived growth factor with and without collagen membrane: An in vivo microcomputed tomographic and histologic experiment in rats. Int. J. Periodontics Restor. Dent. 2016, 36, s173–s186. [Google Scholar] [CrossRef] [Green Version]
- Chung, E.J.; Chien, K.B.; Aguado, B.A.; Shah, R.N. Osteogenic potential of BMP-2-releasing self-assembled membranes. Tissue Eng. Part A 2013, 19, 2664–2673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geiger, M.; Li, R.H.; Friess, W. Collagen sponges for bone regeneration with rhBMP-2. Adv. Drug Deliv. Rev. 2003, 55, 1613–1629. [Google Scholar] [CrossRef] [PubMed]
- Mumcuoglu, D.; Fahmy-Garcia, S.; Ridwan, Y.; Nicke, J.; Farrell, E.; Kluijtmans, S.G.; Van Osch, G.J. Injectable BMP-2 delivery system based on collagen-derived microspheres and alginate induced bone formation in a time- and dose-dependent manner. Eur. Cells Mater. 2018, 35, 242–254. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yang, S.; Zhou, W.; Fu, H.; Qian, L.; Miron, R.J. Addition of a synthetically fabricated osteoinductive biphasic calcium phosphate bone graft to BMP2 improves new bone formation. Clin. Implant. Dent. Relat. Res. 2016, 18, 1238–1247. [Google Scholar] [CrossRef]
- Detsch, R.; Mayr, H.; Ziegler, G. Formation of osteoclast-like cells on HA and TCP ceramics. Acta Biomater. 2008, 4, 139–148. [Google Scholar] [CrossRef]
- Taylor, J.C.; Cuff, S.E.; Leger, J.P.L.; Morra, A.; Anderson, G.I. In vitro osteoclast resorption of bone substitute biomaterials used for implant site augmentation: A pilot study. Int. J. Oral Maxillofac. Implant. 2002, 17, 321–330. [Google Scholar]
- Deeb, G.R.; Wilson, G.H.; Carrico, C.K.; Zafar, U.; Laskin, D.M.; Deeb, J.G. Is the tunnel technique more effective than open augmentation with a titanium-reinforced polytetrafluoroethylene membrane for horizontal ridge augmentation? J. Oral Maxillofac. Surg. 2016, 74, 1752–1756. [Google Scholar] [CrossRef] [Green Version]
- Dupoirieux, L.; Pourquier, D.; Picot, M.; Neves, M.A. Comparative study of three different membranes for guided bone regeneration of rat cranial defects. Int. J. Oral Maxillofac. Surg. 2001, 30, 58–62. [Google Scholar] [CrossRef]
- Jung, R.E.; Lecloux, G.; Rompen, E.; Ramel, C.F.; Buser, D.; Hämmerle, C.H.F. A feasibility study evaluating anin situformed synthetic biodegradable membrane for guided bone regeneration in dogs. Clin. Oral Implant. Res. 2009, 20, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Lo, K.W.-H.; Ulery, B.D.; Ashe, K.M.; Laurencin, C.T. Studies of bone morphogenetic protein-based surgical repair. Adv. Drug Deliv. Rev. 2012, 64, 1277–1291. [Google Scholar] [CrossRef] [Green Version]
- Friess, W.; Uludag, H.; Foskett, S.; Biron, R. Bone regeneration with recombinant human bone morphogenetic protein-2 (rhBMP-2) using absorbable collagen sponges (ACS): Influence of processing on ACS characteristics and formulation. Pharm. Dev. Technol. 1999, 4, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, L.F.; Rinas, U. Optimized procedure for renaturation of recombinant human bone morphogenetic protein-2 at high protein concentration. Biotechnol. Bioeng. 2004, 85, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-Y.; Lee, J.-S.; Kim, M.-S.; Choi, S.-H.; Chai, J.-K.; Jung, U.-W. Comparison of collagen membrane and bone substitute as a carrier for rhBMP-2 in lateral onlay graft. Clin. Oral Implant. Res. 2015, 26, e13–e19. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Rothamel, D.; Herten, M.; Ferrari, D.; Sager, M.; Becker, J. Lateral ridge augmentation using particulated or block bone substitutes biocoated with rhGDF-5 and rhBMP-2: An immunohistochemical study in dogs. Clin. Oral Implant. Res. 2008, 19, 642–652. [Google Scholar] [CrossRef]
- Li, J.; Zhang, H.; Yang, C.; Li, Y.; Dai, Z. An overview of osteocalcin progress. J. Bone Miner. Metab. 2016, 34, 367–379. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | New Bone (%) | p-Value | Post hoc Analysis with LSD a Method |
|---|---|---|---|---|
| Group | <0.001 *** | Control, G1, G2, G3, G4, G5, <G6, G7 | ||
| Control | 10 | 14.54 ± 4.86 | ||
| Membrane (G b 1) | 10 | 18.50 ± 10.88 | ||
| BCP c (G2) | 11 | 18.31 ± 10.17 | ||
| BCP + membrane (G3) | 12 | 22.47 ± 9.02 | ||
| Membrane + BMP-2 = 1 (G4) | 16 | 21.58 ± 10.65 | ||
| Membrane + BMP-2 = 0.5 (G5) | 15 | 20.30 ± 7.99 | ||
| Membrane + BMP-2 = 1 + BCP (G6) | 14 | 31.25 ± 11.62 | ||
| Membrane + BMP-2 = 0.5 + BCP (G7) | 12 | 32.56 ± 12.62 | ||
| Healing time | 0.008 ** | 2 weeks < 4 weeks, 8 weeks | ||
| 2 weeks | 37 | 18.71 ± 7.61 | ||
| 4 weeks | 31 | 23.29 ± 12.34 | ||
| 8 weeks | 32 | 27.03 ± 12.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, N.; Park, J.; Park, S.-H.; Oh, S.; Kim, S.; Cho, S.-W.; Kim, J.-E.; Moon, H.S.; Park, Y.-B. Improving Bone Formation by Guided Bone Regeneration Using a Collagen Membrane with rhBMP-2: A Novel Concept. J. Funct. Biomater. 2023, 14, 170. https://doi.org/10.3390/jfb14030170
Jung N, Park J, Park S-H, Oh S, Kim S, Cho S-W, Kim J-E, Moon HS, Park Y-B. Improving Bone Formation by Guided Bone Regeneration Using a Collagen Membrane with rhBMP-2: A Novel Concept. Journal of Functional Biomaterials. 2023; 14(3):170. https://doi.org/10.3390/jfb14030170
Chicago/Turabian StyleJung, Narae, Jaehan Park, Sang-Hyun Park, Seunghan Oh, Sungtae Kim, Sung-Won Cho, Jong-Eun Kim, Hong Seok Moon, and Young-Bum Park. 2023. "Improving Bone Formation by Guided Bone Regeneration Using a Collagen Membrane with rhBMP-2: A Novel Concept" Journal of Functional Biomaterials 14, no. 3: 170. https://doi.org/10.3390/jfb14030170
APA StyleJung, N., Park, J., Park, S. -H., Oh, S., Kim, S., Cho, S. -W., Kim, J. -E., Moon, H. S., & Park, Y. -B. (2023). Improving Bone Formation by Guided Bone Regeneration Using a Collagen Membrane with rhBMP-2: A Novel Concept. Journal of Functional Biomaterials, 14(3), 170. https://doi.org/10.3390/jfb14030170