

Assessing the Cleanliness of Dental Implants Using Scanning Electron Microscopy and Energy-Dispersive X-ray Spectroscopy Analysis—A SEM and EDS In Vitro Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.3. Unpacking the Implants
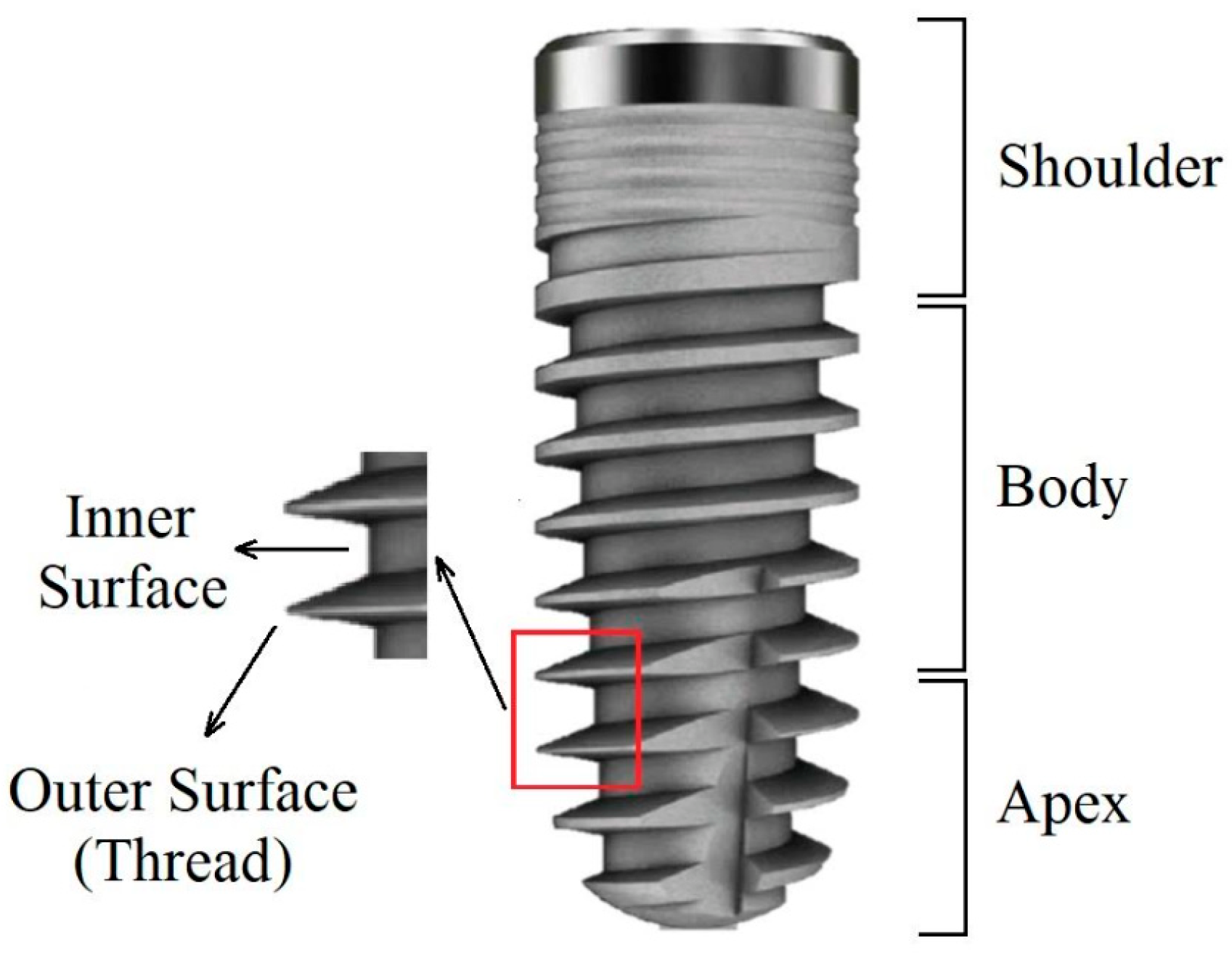
2.4. Image Mapping
2.5. Counting and Detection of Impurities
2.6. EDS Scanning Parameters
2.7. Statistical Analysis
3. Results
3.1. Cortex, Dental Implants Industries, LTD
3.2. Keystone Dental Inc, USA
3.3. Zimmer Biomet Holdings
3.4. Differences in Particle Counts among Companies
3.5. Differences in Particle Counts after Implants Were Exposed to Room Air
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- National Institutes of Health. National Institutes of Health consensus development conference statement: Dental implants. J. Am. Dent. Assoc. 1988, 117, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Brånemark, P.I.; Hansson, H.A.; Lindström, J. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brånemark, R.; Brånemark, P.I.; Rydevik, B.; Myers, R.R. Osseointegration in skeletal reconstruction and rehabilitation: A review. J. Rehabil. Res. Dev. 2001, 38, 175–181. [Google Scholar] [PubMed]
- Albrektsson, T.; Brunski, J.; Wennerberg, A. “A requiem for the periodontal ligament” revisited. Int. J. Prosthodont. 2009, 22, 120–122. [Google Scholar] [PubMed]
- Massaro, C.; Rotolo, P.; De Riccardis, F.; Milella, E.; Napoli, A.; Wieland, M.; Textor, M.; Spencer, N.D.; Brunette, D.M. Comparative investigation of the surface properties of commercial titanium dental implants. Part I: Chemical composition. J. Mater. Sci. Mater. Med. 2002, 13, 535–548. [Google Scholar] [CrossRef]
- Apostu, D.; Lucaciu, O.; Lucaciu, G.D.O.; Crisan, B.; Crisan, L.; Baciut, M.; Onisor, F.; Baciut, G.; Câmpian, R.S.; Bran, S. Systemic drugs that influence titanium implant osseointegration. Drug Metab. Rev. 2017, 49, 92–104. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 1—Review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int. J. Prosthodont. 2004, 17, 536–543. [Google Scholar]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. 4), 172–184. [Google Scholar] [CrossRef]
- Abuhussein, H.; Pagni, G.; Rebaudi, A.; Wang, H.-L. The effect of thread pattern upon implant osseointegration. Clin. Oral Implant. Res. 2010, 21, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Sakka, S.; Baroudi, K.; Nassani, M.Z. Factors associated with early and late failure of dental implants. J. Investig. Clin. Dent. 2012, 3, 258–261. [Google Scholar] [CrossRef]
- Javed, F.; Ahmed, H.B.; Crespi, R.; Romanos, G.E. Role of primary stability for successful osseointegration of dental implants: Factors of influence and evaluation. Interv. Med. Appl. Sci. 2013, 5, 162–167. [Google Scholar] [CrossRef]
- Manzano, G.; Montero, J.; Martín-Vallejo, J.; Del Fabbro, M.; Bravo, M.; Testori, T. Risk Factors in Early Implant Failure: A Meta-Analysis. Implant Dent. 2016, 25, 272–280. [Google Scholar] [CrossRef] [Green Version]
- Kilpadi, D.V.; Lemons, J.E. Surface energy characterization of unalloyed titanium implants. J. Biomed. Mater. Res. 1994, 28, 1419–1425. [Google Scholar] [CrossRef]
- de Alcântara Pinto, C.M.S.; Goulart, D.R.; Asprino, L.; Olate, S.; de Moraes, M. Evaluation of Failed Implants by Metallographic and Energy Dispersive X-ray Analysis. Implant Dent. 2018, 27, 69–73. [Google Scholar] [CrossRef]
- Kasemo, B.; Gold, J. Implant surfaces and interface processes. Adv. Dent. Res. 1999, 13, 8–20. [Google Scholar] [CrossRef]
- Baier, R.E.; Meyer, A.E.; Natiella, J.R.; Natiella, R.R.; Carter, J.M. Surface properties determine bioadhesive outcomes: Methods and results. J. Biomed. Mater. Res. 1984, 18, 337–355. [Google Scholar] [CrossRef]
- Mouhyi, J.; Dohan Ehrenfest, D.M.; Albrektsson, T. The peri-implantitis: Implant surfaces, microstructure, and physicochemical aspects. Clin. Implant Dent. Relat. Res. 2012, 14, 170–183. [Google Scholar] [CrossRef]
- Rupp, F.; Scheideler, L.; Olshanska, N.; de Wild, M.; Wieland, M.; Geis-Gerstorfer, J. Enhancing surface free energy and hydrophilicity through chemical modification of microstructured titanium implant surfaces. J. Biomed. Mater. Res. A 2006, 76, 323–334. [Google Scholar] [CrossRef]
- Kang, B.-S.; Sul, Y.-T.; Oh, S.-J.; Lee, H.-J.; Albrektsson, T. XPS, AES and SEM analysis of recent dental implants. Acta Biomater. 2009, 5, 2222–2229. [Google Scholar] [CrossRef]
- Gudeppu, M.; Sawant, S.; Chockalingam, C.G.; Timiri Shanmugam, P.S. Medical device regulations. In Trends in Development of Medical Devices; Elsevier: Amsterdam, The Netherlands, 2020; pp. 135–152. ISBN 9780128209608. [Google Scholar]
- Park, J.H.; Olivares-Navarrete, R.; Baier, R.E.; Meyer, A.E.; Tannenbaum, R.; Boyan, B.D.; Schwartz, Z. Effect of cleaning and sterilization on titanium implant surface properties and cellular response. Acta Biomater. 2012, 8, 1966–1975. [Google Scholar] [CrossRef] [Green Version]
- ASTM F86-13. Standard Practice for Surface Preparation and Marking of Metallic Surgical Implants. Available online: https://www.astm.org/Standards/F86.htm (accessed on 22 February 2020).
- Klein, M.; Tarnow, D.; Lehrfield, L. Marginal Bone Changes on Ultraclean, Micro-Threaded Platform-Switched Implants Following Restoration: 1- to 4-Year Data. Compend. Contin. Educ. Dent. 2020, 41, e7–e18. [Google Scholar] [PubMed]
- Duddeck, D.; Maghaireh, H.; Faber, F.J.; Neugebauer, J. SEM surface analyses of 120 sterile-packed implants. Clin. Implant. Dent. Relat. Res. 2014, 16, 817–826. Available online: https://alpha-bio.net/media/2529/edi-journal_2-2015_duddeck_implant-study_2015_part-2.pdf (accessed on 18 October 2022).
- Guler, B.; Uraz, A.; Çetiner, D. The chemical surface evaluation of black and white porous titanium granules and different commercial dental implants with energy-dispersive x-ray spectroscopy analysis. Clin. Implant Dent. Relat. Res. 2019, 21, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Duddeck, D.U.; Albrektsson, T.; Wennerberg, A.; Larsson, C.; Beuer, F. On the cleanliness of different oral implant systems: A pilot study. J. Clin. Med. 2019, 8, 1280. [Google Scholar] [CrossRef] [Green Version]
- Harloff, T.; Hönle, W.; Holzwarth, U.; Bader, R.; Thomas, P.; Schuh, A. Titanium allergy or not? “Impurity” of titanium implant materials. Health 2010, 2, 306–310. [Google Scholar] [CrossRef] [Green Version]
- Kasemo, B.; Lausmaa, J. Biomaterial and implant surfaces: On the role of cleanliness, contamination, and preparation procedures. J. Biomed. Mater. Res. 1988, 22, 145–158. [Google Scholar] [CrossRef]
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef] [Green Version]
- Shibli, J.A.; Marcantonio, E.; d’Avila, S.; Guastaldi, A.C.; Marcantonio, E. Analysis of failed commercially pure titanium dental implants: A scanning electron microscopy and energy-dispersive spectrometer x-ray study. J. Periodontol. 2005, 76, 1092–1099. [Google Scholar] [CrossRef] [Green Version]
- Albrektsson, T.; Canullo, L.; Cochran, D.; De Bruyn, H. “Peri-Implantitis”: A Complication of a Foreign Body or a Man-Made “Disease”. Facts and Fiction. Clin. Implant Dent. Relat. Res. 2016, 18, 840–849. [Google Scholar] [CrossRef]
- Olmedo, D.G.; Tasat, D.R.; Duffó, G.; Guglielmotti, M.B.; Cabrini, R.L. The issue of corrosion in dental implants: A review. Acta Odontol. Latinoam. 2009, 22, 3–9. [Google Scholar]
- Hori, N.; Att, W.; Ueno, T.; Sato, N.; Yamada, M.; Saruwatari, L.; Suzuki, T.; Ogawa, T. Age-dependent degradation of the protein adsorption capacity of titanium. J. Dent. Res. 2009, 88, 663–667. [Google Scholar] [CrossRef]
- Palani, N. ISO 19227: Implants for surgery—Cleanliness of orthopedic implants. In Medical Device Guidelines and Regulations Handbook; Timiri Shanmugam, P.S., Thangaraju, P., Palani, N., Sampath, T., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 57–73. ISBN 978-3-030-91854-5. [Google Scholar]
- Duddeck, D.; Albrektsson, T.; Wennerberg, A. CleanImplant Trusted Quality Mark 2017–2018—Guideline and Consensus Paper. Available online: https://www.cleanimplant.com/Awards/implants/ (accessed on 26 June 2019).
- Bauer, L.J.; Mustafa, H.A.; Zaslansky, P.; Mantouvalou, I. Chemical mapping of teeth in 2D and 3D: X-ray fluorescence reveals hidden details in dentine surrounding fillings. Acta Biomater. 2020, 109, 142–152. [Google Scholar] [CrossRef]
- Cierech, M.; Szerszeń, M.; Wojnarowicz, J.; Łojkowski, W.; Kostrzewa-Janicka, J.; Mierzwińska-Nastalska, E. Preparation and Characterisation of Poly(methyl metacrylate)-Titanium Dioxide Nanocomposites for Denture Bases. Polymers 2020, 12, 2655. [Google Scholar] [CrossRef]
- AlRefeai, M.H.; AlHamdan, E.M.; Al-Saleh, S.; Farooq, I.; Abrar, E.; Vohra, F.; Abduljabbar, T. Assessment of bond integrity, durability, and degree of conversion of a calcium fluoride reinforced dentin adhesive. Polymers 2021, 13, 2418. [Google Scholar] [CrossRef]
- Schappo, H.; Gindri, I.M.; Cubillos, P.O.; Maru, M.M.; Salmoria, G.V.; Roesler, C.R.M. Scanning Electron Microscopy and Energy-Dispersive X-Ray Spectroscopy as a Valuable Tool to Investigate the Ultra-High-Molecular-Weight Polyethylene Wear Mechanisms and Debris in Hip Implants. J. Arthroplast. 2018, 33, 258–262. [Google Scholar] [CrossRef]
- Ebnesajjad, S. Surface and material characterization techniques. In Surface Treatment of Materials for Adhesive Bonding; Elsevier: Amsterdam, The Netherlands, 2014; pp. 39–75. ISBN 9780323264358. [Google Scholar]
- Rizo-Gorrita, M.; Fernandez-Asian, I.; Garcia-de-Frenza, A.; Vazquez-Pachon, C.; Serrera-Figallo, M.-A.; Torres-Lagares, D.; Gutierrez-Perez, J.-L. Influence of three dental implant surfaces on cell viability and bone behavior. an in vitro and a histometric study in a rabbit model. Appl. Sci. 2020, 10, 4790. [Google Scholar] [CrossRef]
- Duddeck, D.U.; Albrektsson, T.; Wennerberg, A.; Larsson, C.; Mouhyi, J.; Beuer, F. Quality assessment of five randomly chosen ceramic oral implant systems: Cleanliness, surface topography, and clinical documentation. Int. J. Oral Maxillofac. Implant. 2021, 36, 863–874. [Google Scholar] [CrossRef]
- Szmukler-Moncler, S.; Bischof, M.; Nedir, R.; Ermrich, M. Titanium hydride and hydrogen concentration in acid-etched commercially pure titanium and titanium alloy implants: A comparative analysis of five implant systems. Clin. Oral Implant. Res. 2010, 21, 944–950. [Google Scholar] [CrossRef]
- Schupbach, P.; Glauser, R.; Bauer, S. Al2O3 Particles on Titanium Dental Implant Systems following Sandblasting and Acid-Etching Process. Int. J. Biomater. 2019, 2019, 6318429. [Google Scholar] [CrossRef] [Green Version]
- Dias, F.J.; Fuentes, R.; Navarro, P.; Weber, B.; Borie, E. Assessment of the Chemical Composition in Different Dental Implant Types: An Analysis through EDX System. Coatings 2020, 10, 882. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Vazquez, L.; Park, Y.-J.; Sammartino, G.; Bernard, J.-P. Identification card and codification of the chemical and morphological characteristics of 14 dental implant surfaces. J. Oral Implantol. 2011, 37, 525–542. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Lang, N.P. The role of bone debris in early healing adjacent to hydrophilic and hydrophobic implant surfaces in man. Clin. Oral Implant. Res. 2011, 22, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, I.; Berglundh, T.; Linder, E.; Lang, N.P.; Lindhe, J. Early bone formation adjacent to rough and turned endosseous implant surfaces. An experimental study in the dog. Clin. Oral Implant. Res. 2004, 15, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-J.; Song, Y.-H.; An, J.-H.; Song, H.-J.; Anusavice, K.J. Cytocompatibility of pure metals and experimental binary titanium alloys for implant materials. J. Dent. 2013, 41, 1251–1258. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cortex Dental Implant | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Magnification | 30× | 100× | 200× (Outer Surface) | 200× (Inner Surface) | ||||||||||
| Particle Size Area | L 1 | M 2 | S 3 | LM 4 | S | LM | S | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Shoulder | 1.64 | ±1.05 | 1.17 | ±0.91 | 2.40 | ±2.28 | 0.96 | ±1.17 | 3.32 | ±2.85 | 0.07 | ±0.25 | 2.92 | ±3.47 |
| Body | 1.66 | ±1.35 | 1.01 | ±0.69 | 2.32 | ±2.17 | 0.88 | ±0.9 | 2.50 | ±2.18 | 0.23 | ±0.47 | 1.46 | ±2.03 |
| Apex | 1.08 | ±0.94 | 0.74 | ±0.78 | 0.97 | ±1.64 | 0.16 | ±0.43 | 1.90 | ±2.5 | 0.07 | ±2.5 | 0.97 | ±2.4 |
| Implant mean | 4.38 | ±0.99 | 2.92 | ±0.64 | 5.68 | ±2.43 | 2 | ±1.32 | 7.73 | ±2.13 | 0.36 | ±0.28 | 5.35 | ±3.04 |
| p-value | 0.03 | 0.37 | 0.14 | 0.034 | 0.1 | 0.29 | 0.014 | |||||||
| Implants Company | Area | S 1 (In 3–Out 4) | LM 2 (In–Out) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Paired Differences | t-Test | p-Value | Paired Differences | t-Test | p-Value | ||||
| MEAN | SD± | MEAN | SD± | ||||||
| Cortex | SH 5 | −0.40 | 2.13 | −0.72 | 0.48 | −0.90 | 1.26 | −2.76 | <0.05 |
| B 6 | −1.05 | 1.62 | −2.49 | <0.05 | −0.65 | 1.16 | −2.17 | <0.05 | |
| A 7 | −0.93 | 1.53 | −2.37 | <0.05 | −0.09 | 0.53 | −0.69 | 0.50 | |
| Keystone | SH | −2.63 | 2.76 | −3.69 | <0.01 | −0.67 | 1.08 | −2.97 | <0.05 |
| B | −3.11 | 2.22 | −5.43 | <0.01 | −1.03 | 1.34 | −3.71 | 0.01 | |
| A | −3.20 | 2.73 | −4.54 | <0.01 | −0.82 | 0.86 | −6.30 | <0.01 | |
| Zimmer | SH | −3.27 | 2.01 | −6.30 | <0.01 | −1.09 | 1.49 | −2.84 | 0.013 |
| B | −5.80 | 2.04 | −11.01 | <0.01 | −0.79 | 1.32 | −2.24 | 0.043 | |
| A | −3.73 | 3.43 | −4.20 | <0.01 | −1.79 | 1.41 | −4.90 | <0.01 | |
| Cortex | |||
|---|---|---|---|
| Elements | Mean% | SD | (n) 1 |
| C | 57.3 | ±31.62 | 13 |
| N | 44.51 | ±25.75 | 13 |
| Al | 19.47 | ±14.3 | 14 |
| O | 27.27 | ±15.76 | 14 |
| Ti | 87.21 | ±3.91 | 5 |
| Si | 6.33 | ± 9.3 | 3 |
| S | 0.76 | - | 1 |
| Ca | 0.00 | - | 0 |
| Na | 0.95 | ±0.6 | 2 |
| Mg | 2.84 | - | 1 |
| Cu | 0.00 | - | 0 |
| F | 0.00 | - | 0 |
| Cl | 0.00 | - | 0 |
| Fe | 20.67 | - | 1 |
| P | 1.2 | ±0.45 | 4 |
| V | 66.61 | - | 1 |
| Keystone Dental Implant | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Magnification | 30× | 100× | 200× (Outer Surface) | 200× (Inner Surface) | ||||||||||
| Particle Size Area | L 1 | M 2 | S 3 | LM 4 | S | LM | S | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Shoulder | 1.63 | ±1.16 | 1.38 | ±1.08 | 3.72 | ±2.32 | 0.80 | ±0.81 | 3.30 | ±2.09 | 0.13 | ±0.51 | 0.67 | ±1.34 |
| Body | 2.24 | ±1.76 | 1.18 | ±1.1 | 3.53 | ±2.17 | 1.03 | ±1.33 | 4.19 | ±2 | 0.00 | - | 1.08 | ±1.68 |
| Apex | 1.53 | ±0.88 | 0.79 | ±0.83 | 2.75 | ±2.6 | 0.89 | ±0.93 | 3.97 | ±2.81 | 0.07 | ±0.25 | 0.77 | ±1.13 |
| Implant mean | 5.40 | ±1.14 | 3.35 | ±0.9 | 10 | ±1.56 | 2.72 | ±0.33 | 11.45 | ±1.38 | 0.2 | ±0.2 | 2.51 | ±0.63 |
| p-value | 0.06 | 0.18 | 0.35 | 0.83 | 0.36 | 0.57 | 0.35 | |||||||
| Keystone | |||
|---|---|---|---|
| Elements | Mean% | SD | (n) 1 |
| C | 42.94 | ±19.71 | 15 |
| N | 40.32 | ±13.03 | 13 |
| Al | 24.23 | ±14.77 | 13 |
| O | 27.67 | ±12.53 | 15 |
| Ti | 9.09 | - | 1 |
| Si | 5.07 | ±4.5 | 5 |
| S | 0.89 | ±0.39 | 5 |
| Ca | 14.6 | - | 1 |
| Na | 1.33 | ±1.05 | 3 |
| Mg | 9.11 | ±11.06 | 2 |
| Cu | 2.5 | ±0.03 | 2 |
| F | 5.77 | - | 1 |
| Cl | 0.28 | - | 1 |
| Fe | 0.00 | - | 0 |
| P | 0.00 | - | 0 |
| V | 0.00 | - | 0 |
| Zimmer Dental Implant | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Magnification | 30× | 100× | 200× (Outer Surface) | 200× (Inner Surface) | ||||||||||
| Particle Size Area | L 1 | M 2 | S 3 | LM 4 | S | LM | S | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Shoulder | 2.73 | ±0.89 | 1.80 | ±0.97 | 6.95 | ±3.8 | 1.55 | ±1.47 | 7.78 | ±2 | 0.34 | ±0.58 | 4.5 | ±3.74 |
| Body | 3.99 | ±1.48 | 1.37 | ±0.69 | 3.85 | ±2.27 | 0.99 | ±1.1 | 4.19 | ±2 | 0.20 | ±0.5 | 1.22 | ±1.02 |
| Apex | 4.01 | ±1.67 | 1.38 | ±1.31 | 5.97 | ±4 | 2.12 | ±1.5 | 3.97 | ±2.81 | 0.27 | ±0.55 | 3.13 | ±2.52 |
| Implant mean | 10.73 | ±2.2 | 4.56 | ±0.74 | 16.77 | ±4.74 | 4.66 | ±1.68 | 21.65 | ±1.5 | 0.81 | ±0.2 | 8.85 | ±4.95 |
| p-value | <0.01 | 0.41 | 0.043 | 0.072 | 0.594 | 0.809 | <0.01 | |||||||
| Zimmer | |||
|---|---|---|---|
| Elements | Mean% | SD | (n) 1 |
| C | 37.52 | ±12.18 | 15 |
| N | 49 | ±13.76 | 15 |
| Al | 35.62 | ±42.85 | 3 |
| O | 21.15 | ±10.15 | 14 |
| Ti | 86.1 | ±3.13 | 2 |
| Si | 7.18 | ±11.5 | 5 |
| S | 0.64 | ±0.2 | 9 |
| Ca | 10.09 | ±5.37 | 8 |
| Na | 0.68 | ±0.27 | 6 |
| Mg | 8.89 | ±9.5 | 2 |
| Cu | 0.00 | - | 0 |
| F | 0.00 | - | 0 |
| Cl | 12.16 | - | 1 |
| Fe | 5.31 | - | 1 |
| P | 2.1 | - | 1 |
| V | 0.00 | - | 0 |
| Particle Implant Size Brand | L 1 | M 2 | S 3 | |||
|---|---|---|---|---|---|---|
| Mean% | SD | Mean% | SD | Mean% | SD | |
| Cortex | 1.46 | ±0.33 | 0.97 | ±0.21 | 1.89 | ±0.8 |
| Keystone | 1.80 | ±0.38 | 1.12 | ±0.3 | 3.33 | ±0.5 |
| Zimmer Biomet | 3.58 | ±0.73 | 1.52 | ±0.25 | 5.59 | ±1.6 |
| p-value | <0.01 | 0.052 | <0.01 | |||
| Magnification | Area | Dental Implants Brand | ||||||
|---|---|---|---|---|---|---|---|---|
| Cortex | Keystone | Zimmer | p-Value | |||||
| Mean% | SD | Mean% | SD | Mean% | SD | |||
| 30× | Sh 5 | 1.63 | ±1.05 | 1.64 | ±1.7 | 2.73 | ±0.89 | 0.01> |
| B 6 | 1.66 | ±1.35 | 2.24 | ±1.6 | 3.99 | ±1.48 | 0.01> | |
| A 7 | 1.08 | ±0.94 | 1.53 | ±0.88 | 4 | ±1.67 | 0.01> | |
| 100× M | Sh | 1.17 | ±0.91 | 1.38 | ±1.08 | 1.80 | ±0.97 | 0.22 |
| B | 1.01 | ±0.69 | 1.18 | ±1.1 | 1.37 | ±0.69 | 0.51 | |
| A | 0.74 | ±0.78 | 0.79 | ±0.83 | 1.38 | ±1.3 | 0.165 | |
| 100× S | Sh | 2.39 | ±2.28 | 3.72 | ±2.32 | 6.95 | ±3.8 | 0.01> |
| B | 2.32 | ±2.17 | 3.41 | ±2 | 3.85 | ±2.27 | 0.15 | |
| A | 0.97 | ±1.65 | 2.56 | ±2.6 | 5.9 | ±4.04 | 0.01> | |
| 200× Out S 1 | Sh | 3.3 | ±2.85 | 3.3 | ±2.1 | 7.78 | ±2.67 | 0.01> |
| B | 2.50 | ±2.2 | 4.19 | ±2 | 7.01 | ±2.5 | 0.01> | |
| A | 1.9 | ±2.5 | 3.97 | ±2.8 | 6.86 | ±3.3 | 0.01> | |
| 200× Out ML 2 | Sh | 0.97 | ±1.2 | 0.8 | ±0.8 | 1.75 | ±1.6 | 0.097 |
| B | 0.88 | ±0.9 | 1 | ±1.33 | 0.92 | ±1.1 | 0.93 | |
| A | 0.16 | ±0.43 | 0.89 | ±0.93 | 2.11 | ±1.45 | 0.01> | |
| 200× In S 3 | Sh | 2.9 | ±3.5 | 0.7 | ±1.3 | 4.51 | ±3.7 | 0.01> |
| B | 1.5 | ±2 | 1.1 | ±1.7 | 1.2 | ±1 | 0.80 | |
| A | 1 | ±2.5 | 0.76 | ±1.1 | 3.1 | ±2.5 | 0.01> | |
| 200× In ML 4 | Sh | 0.07 | ±0.26 | 0.13 | ±0.52 | 0.66 | ±1.36 | 0.13 |
| B | 0.23 | ±0.48 | 0 | - | 0.2 | ±0.52 | 0.26 | |
| A | 0.07 | ±0.26 | 0.07 | ±0.26 | 0.32 | ±0.56 | 0.13 | |
| Implant Company | Cortex | Keystone | Zimmer | |||
|---|---|---|---|---|---|---|
| (n 1 = 15) | (n = 15) | (n = 15) | ||||
| Mean | SD | Mean | SD | Mean | SD | |
| Before | 2.73 | ±1.703 | 3.363 | ±1.97 | 6.37 | ±2.12 |
| After | 2.74 | ±1.715 | 3.376 | ±2 | 6.39 | ±2.14 |
| t-test | t (14) = −1 | t (14) = −1 | t (14) = −1.72 | |||
| p-value | 0.334 | 0.334 | 0.1 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mtanis, T.; Biadsee, A.; Ormianer, Z. Assessing the Cleanliness of Dental Implants Using Scanning Electron Microscopy and Energy-Dispersive X-ray Spectroscopy Analysis—A SEM and EDS In Vitro Study. J. Funct. Biomater. 2023, 14, 172. https://doi.org/10.3390/jfb14030172
Mtanis T, Biadsee A, Ormianer Z. Assessing the Cleanliness of Dental Implants Using Scanning Electron Microscopy and Energy-Dispersive X-ray Spectroscopy Analysis—A SEM and EDS In Vitro Study. Journal of Functional Biomaterials. 2023; 14(3):172. https://doi.org/10.3390/jfb14030172
Chicago/Turabian StyleMtanis, Tarek, Ameer Biadsee, and Zeev Ormianer. 2023. "Assessing the Cleanliness of Dental Implants Using Scanning Electron Microscopy and Energy-Dispersive X-ray Spectroscopy Analysis—A SEM and EDS In Vitro Study" Journal of Functional Biomaterials 14, no. 3: 172. https://doi.org/10.3390/jfb14030172
APA StyleMtanis, T., Biadsee, A., & Ormianer, Z. (2023). Assessing the Cleanliness of Dental Implants Using Scanning Electron Microscopy and Energy-Dispersive X-ray Spectroscopy Analysis—A SEM and EDS In Vitro Study. Journal of Functional Biomaterials, 14(3), 172. https://doi.org/10.3390/jfb14030172